
Resistance Training with Blood Flow Restriction Compared to Traditional Resistance Training on Strength and Muscle Mass in Non-Active Older Adults: A Systematic Review and Meta-Analysis


 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Information Sources and Search
2.3. Eligibility Criteria and Study Selection
2.4. Data Collection Process
2.5. Risk of Bias of Individual Studies
2.6. Summary Measures
2.7. Additional Analysis
2.8. Certainty of the Evidence: GRADE Approach
3. Results
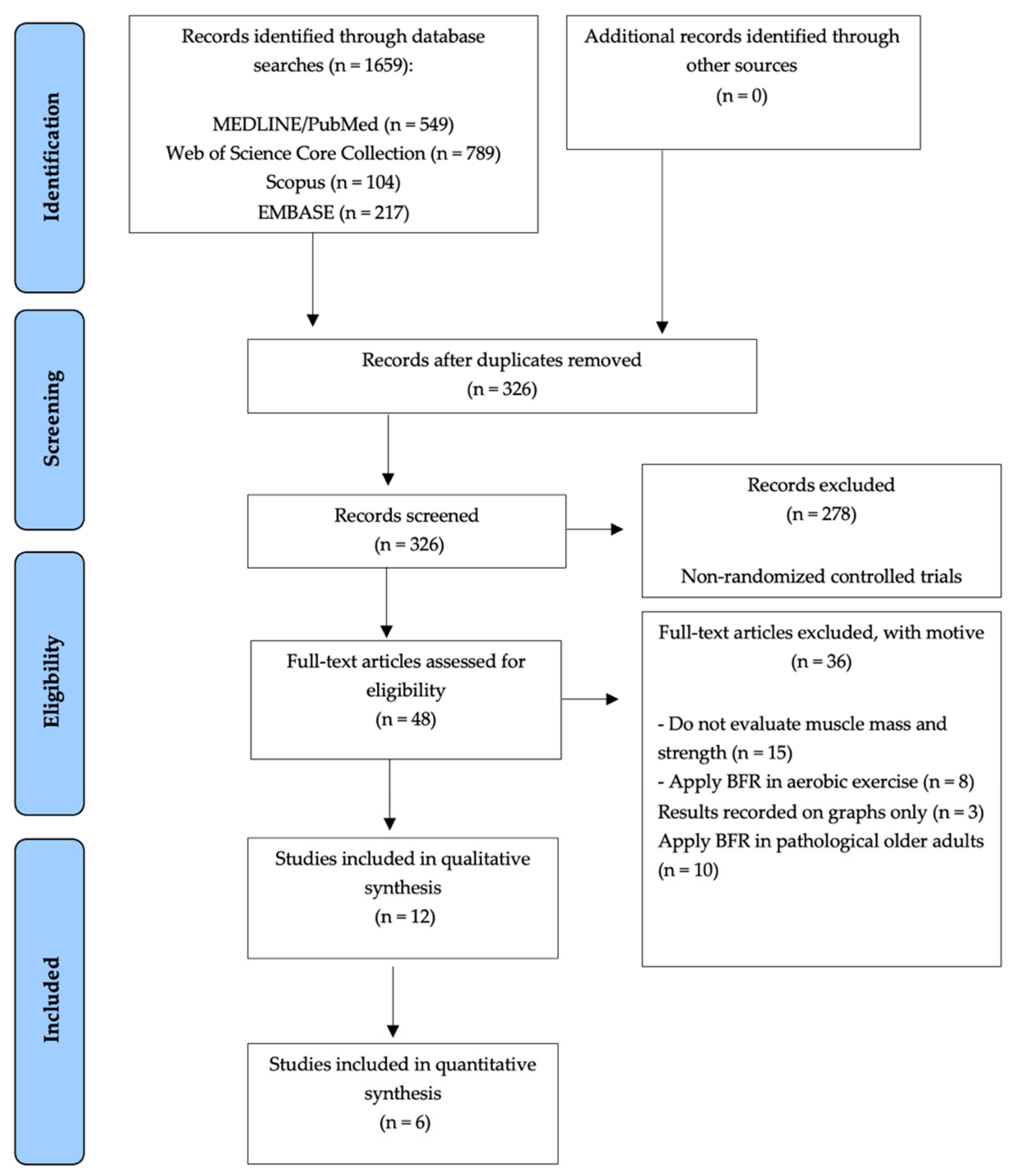
3.1. Literature Search and Article Selection
3.2. Risk of Bias Individual Studies
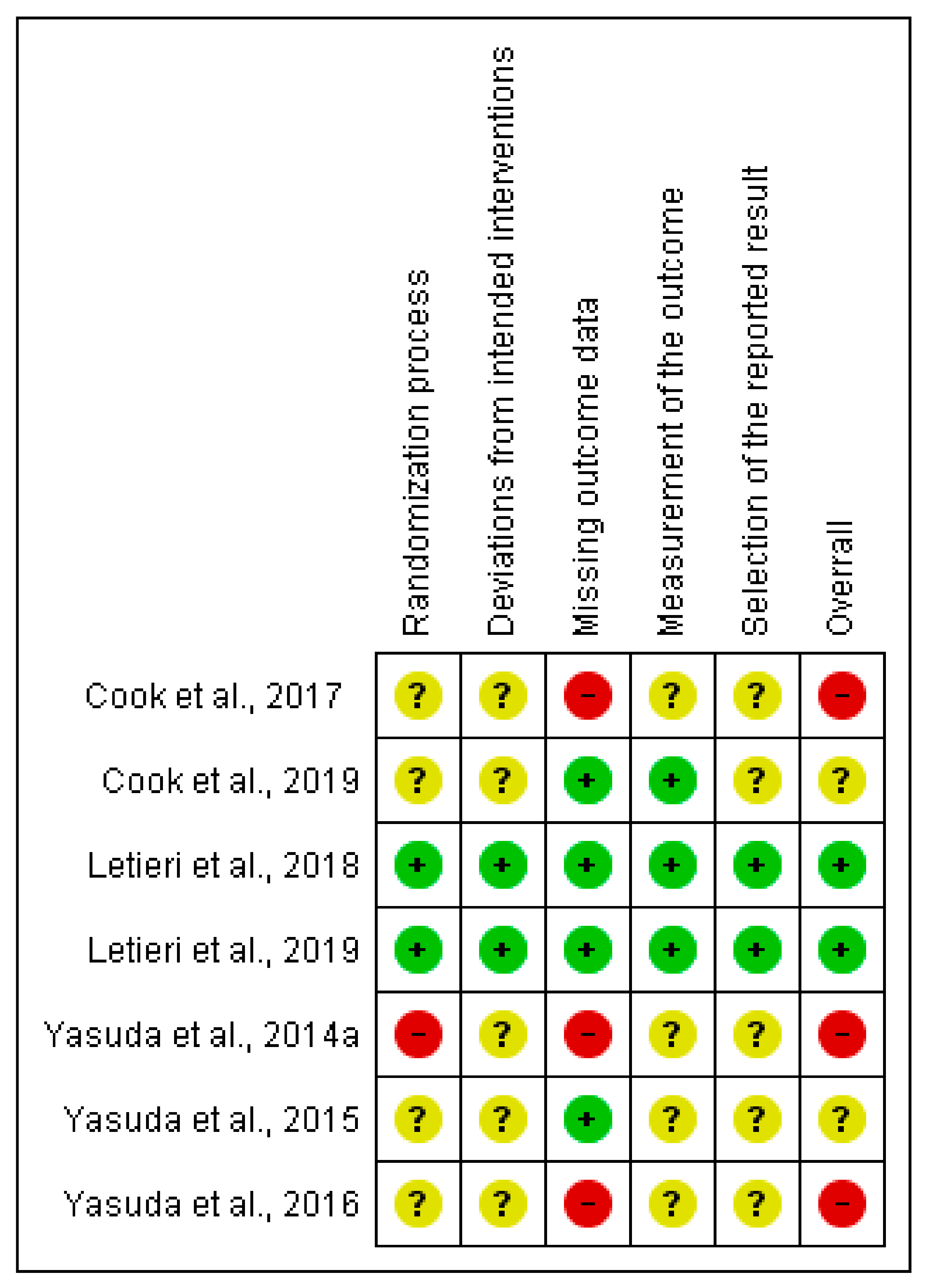
3.2.1. Muscular Strength Outcome (RM Test)
3.2.2. Muscular Strength Outcome (MVC Test)
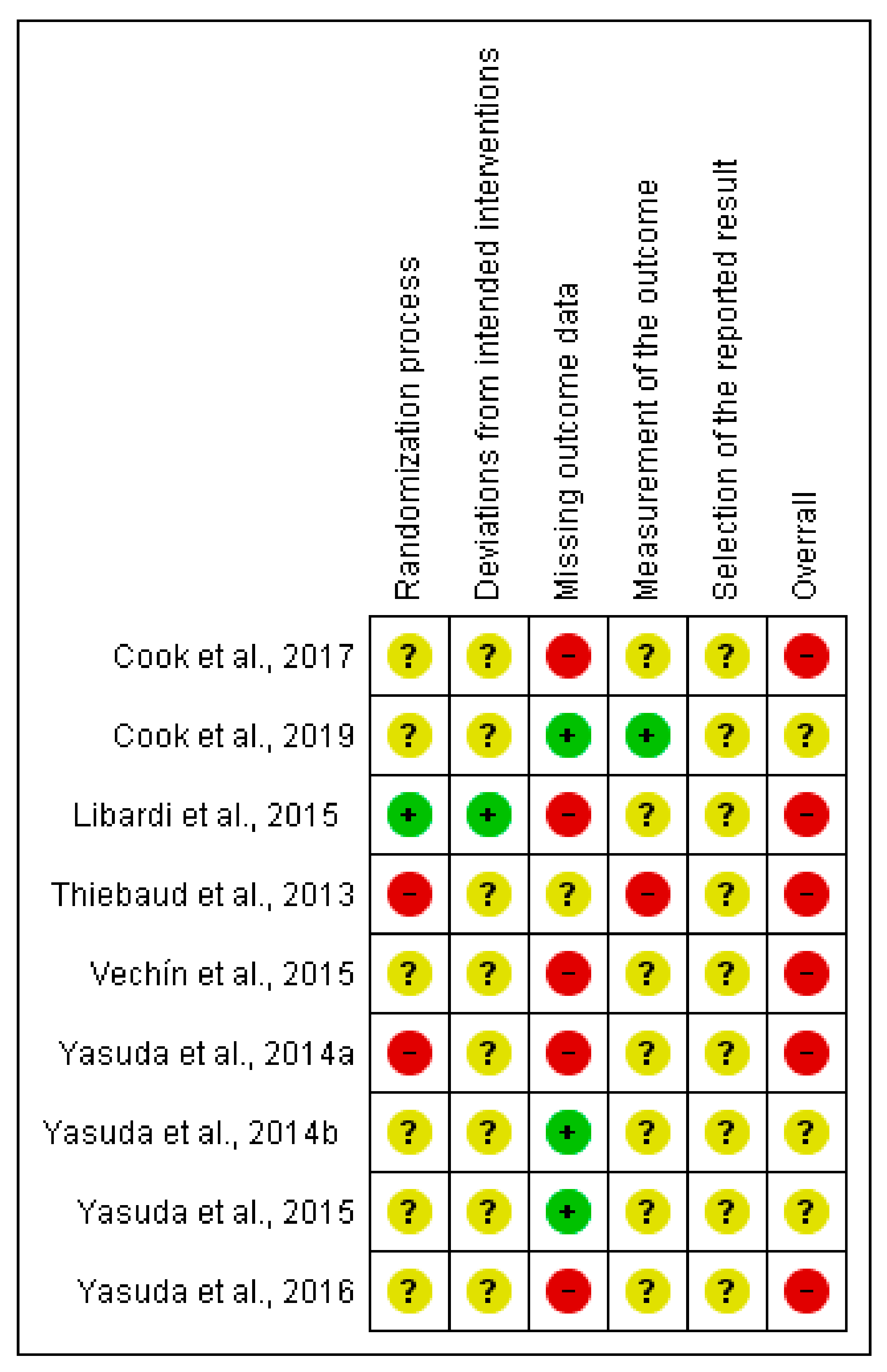
3.2.3. Muscle Mass Outcome (cm2)
3.3. Main Findings
3.3.1. Narrative Synthesis
3.3.2. Quantitative Synthesis
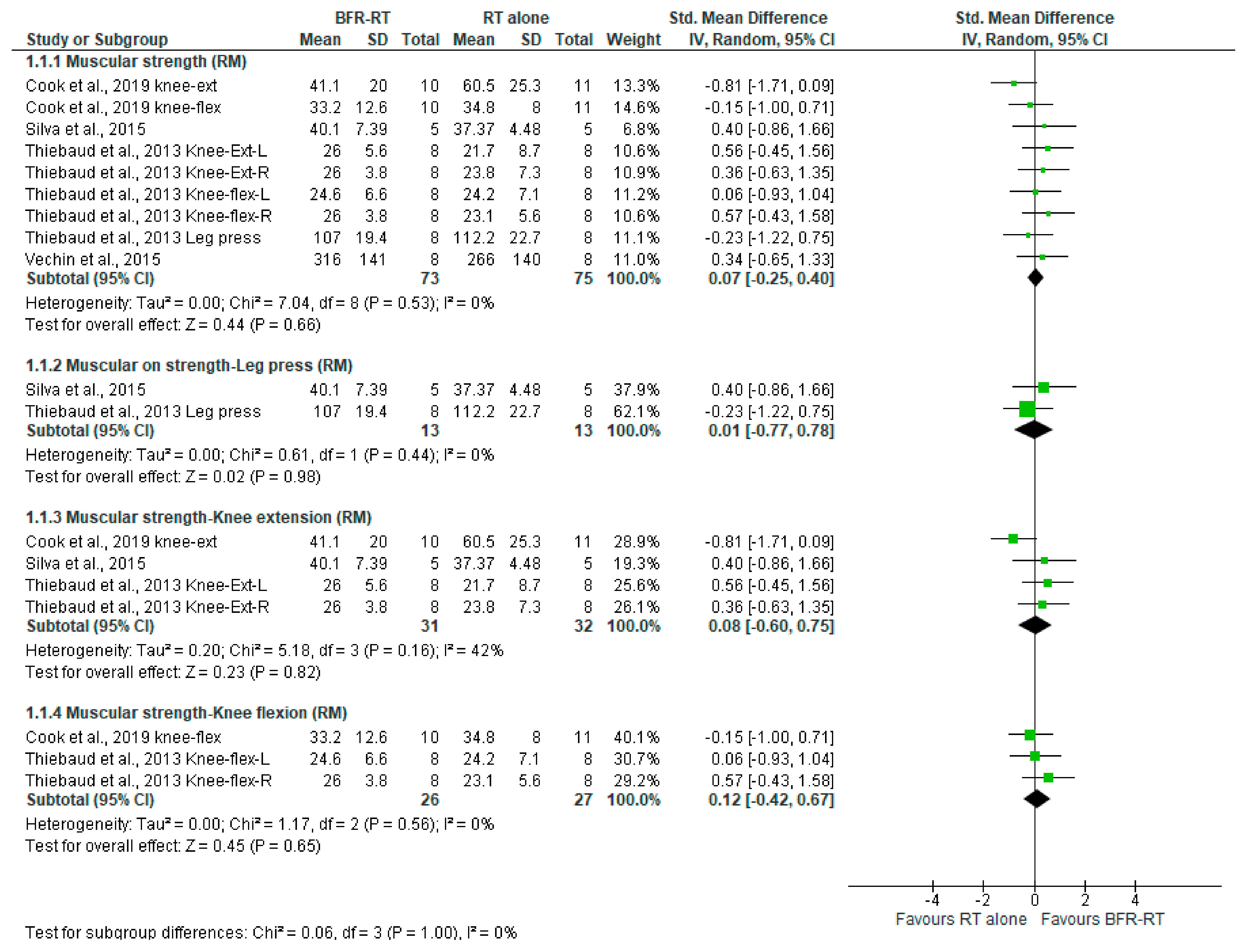
LI-BFR vs. RT Alone on Muscular Strength via RM Test
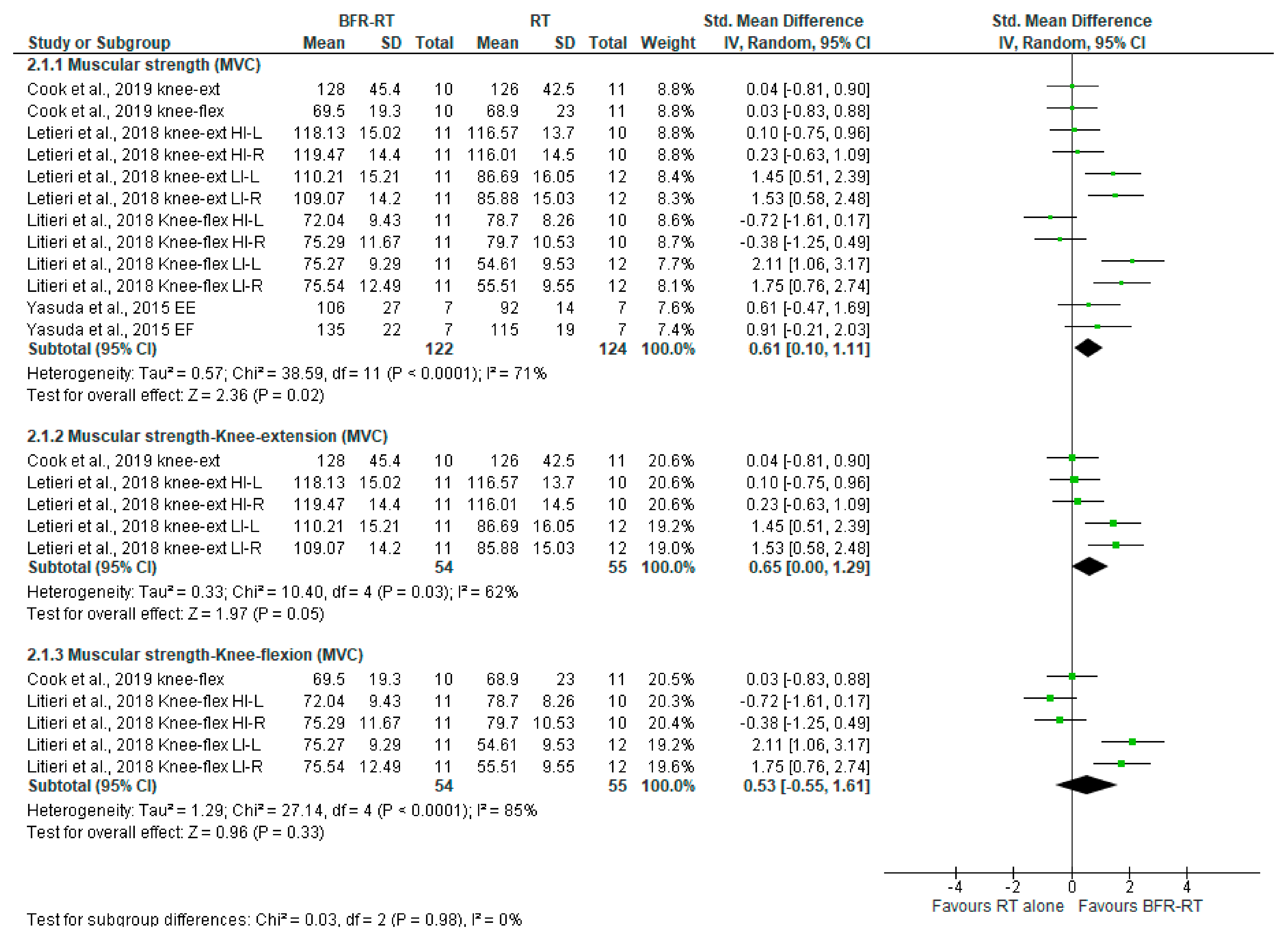
LI-BFR vs. RT Alone on Muscular Strength via the MVC Testing
LI-BFR vs. RT Alone on Muscle Mass (cm2)
4. Discussion
4.1. Summary of Main Results
4.2. Certain of Evidence
4.3. Potential Biases in the Review Process
4.4. Agreements and Disagreements with Other Studies or Reviews
4.5. Implications for Practice and Further Research
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Ageing and Health. World Health Organization. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.+Geneva%2C+World+Health+Organization%2C+2018&btnG= (accessed on 25 June 2021).
- Olshansky, S.J. From Lifespan to Healthspan. JAMA 2018, 320, 1323–1324. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, N.; Lord, J.M.; Harridge, S.D.R. The Relationships and Interactions between Age, Exercise and Physiological Function. J. Physiol. 2019, 597, 1299–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. Frailty and Sarcopenia in Elderly. Wien. Klin. Wochenschr. 2016, 128, 439–445. [Google Scholar] [CrossRef]
- Mora, J.C.; Valencia, W.M. Exercise and Older Adults. Clin. Geriatr. Med. 2018, 34, 145–162. [Google Scholar] [CrossRef]
- Shaw, S.; Dennison, E.M.; Cooper, C. Epidemiology of Sarcopenia: Determinants throughout the Lifecourse. Calcif. Tissue Int. 2017, 101, 229–247. [Google Scholar] [CrossRef] [Green Version]
- Fragala, M.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement from the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical Activity and Exercise: Strategies to Manage Frailty. Redox Biol. 2020, 35, 101513. [Google Scholar] [CrossRef]
- Clark, B.; Manini, T.M. Functional Consequences of Sarcopenia and Dynapenia in the Elderly. Clin. Nutr. Metab. 2010, 13, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Manini, T.M.; Clark, B.C. Dynapenia and Aging: An Update. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 28–40. [Google Scholar] [CrossRef] [Green Version]
- McGrath, R.P.; Kraemer, W.J.; Vincent, B.M.; Hall, O.T.; Peterson, M.D. Muscle Strength Is Protective against Osteoporosis in an Ethnically Diverse Sample of Adults. J. Strength Cond. Res. 2017, 31, 2586–2589. [Google Scholar] [CrossRef]
- Peterson, M.D.; Zhang, P.; Choksi, P.; Markides, K.S.; Al Snih, S. Muscle Weakness Thresholds for Prediction of Diabetes in Adults. Sports Med. 2016, 46, 619–628. [Google Scholar] [CrossRef] [Green Version]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Association of Muscle Strength with the Risk of Alzheimer Disease and the Rate of Cognitive Decline in Community-Dwelling Older Persons. Arch. Neurol. 2009, 66, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Blood Flow Restricted Exercise for Athletes: A Review of Available Evidence. J. Sci. Med. Sport 2016, 19, 360–367. [Google Scholar] [CrossRef]
- Wortman, R.J.; Brown, S.M.; Savage-Elliott, I.; Finley, Z.J.; Mulcahey, M.K. Blood Flow Restriction Training for Athletes: A Systematic Review. Am. J. Sports Med. 2021, 49, 1938–1944. [Google Scholar] [CrossRef]
- Grønfeldt, B.M.; Lindberg Nielsen, J.; Mieritz, R.M.; Lund, H.; Aagaard, P. Effect of Blood-Flow Restricted vs Heavy-Load Strength Training on Muscle Strength: Systematic Review and Meta-Analysis. Scand. J. Med. Sci. Sports 2020, 30, 837–848. [Google Scholar] [CrossRef]
- Lixandrão, M.E.; Ugrinowitsch, C.; Berton, R.; Vechin, F.C.; Conceição, M.S.; Damas, F.; Libardi, C.A.; Roschel, H. Magnitude of Muscle Strength and Mass Adaptations Between High-Load Resistance Training Versus Low-Load Resistance Training Associated with Blood-Flow Restriction: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 361–378. [Google Scholar] [CrossRef]
- Centner, C.; Wiegel, P.; Gollhofer, A.; König, D. Effects of Blood Flow Restriction Training on Muscular Strength and Hypertrophy in Older Individuals: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 95–108. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Littlewood, A.; Marshall, C.; Metzendorf, M.I.; Noel-Storr, A.; Rader, T.; Shokraneh, F.; Thomas, J.; et al. Searching for and Selecting Studies. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Oxford, UK, 2019; pp. 67–107. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Aminian, S.; et al. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Rivière, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6, 288. [Google Scholar] [CrossRef]
- Sato, Y. The History and Future of KAATSU Training. Int. J. KAATSU Train. Res. 2005, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- American College of Sports Medicine Position Stand. Progression Models in Resistance Training for Healthy Adults. Med. Sci. Sports Exer. 2009, 41, 687–708. [Google Scholar]
- Cook, S.B.; LaRoche, D.P.; Villa, M.R.; Barile, H.; Manini, T.M. Blood Flow Restricted Resistance Training in Older Adults at Risk of Mobility Limitations. Exp. Gerontol. 2017, 99, 138–145. [Google Scholar] [CrossRef]
- Cook, S.B.; Cleary, C.J. Progression of Blood Flow Restricted Resistance Training in Older Adults at Risk of Mobility Limitations. Front. Physiol. 2019, 10, 738. [Google Scholar] [CrossRef]
- Letieri, R.V.; Teixeira, A.M.; Furtado, G.E.; Lamboglia, C.G.; Rees, J.L.; Gomes, B.B. Effect of 16 Weeks of Resistance Exercise and Detraining Comparing Two Methods of Blood Flow Restriction in Muscle Strength of Healthy Older Women: A randomized controlled trial. Exp. Gerontol. 2018, 114, 78–86. [Google Scholar] [CrossRef]
- Letieri, R.V.; Furtado, G.E.; Barros, P.M.N.; Farias, M.J.A.; Antunez, B.F.; Gomes, B.; Teixeira, A.M. Effect of 16-Week Blood Flow Restriction Exercise on Functional Fitness in Sarcopenic Women: A Randomized Controlled Trial. Int. J. Morphol. 2019, 37, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Libardi, C.A.; Chacon-Mikahil, M.P.T.; Cavaglieri, C.R.; Tricoli, V.; Roschel, H.; Vechin, F.C.; Conceição, M.S.; Ugrinowitsch, C. Effect of Concurrent Training with Blood Flow Restriction in the Elderly. Int. J. Sports Med. 2015, 36, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, J.; Neto, G.R.; Freitas, E.; Pereira Neto, E.; Batista, G.; Torres, M.; Sousa, M. Chronic Effect of Strength Training with Blood Flow Restriction on Muscular Strength among Women with Osteoporosis. J. Exerc. Physiol. 2015, 18, 33–41. [Google Scholar]
- Thiebaud, R.S.; Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Kim, D.; Abe, T.; Anderson, M.A.; Young, K.C.; Bemben, D.A.; Bemben, M.G. The Effects of Elastic Band Resistance Training Combined with Blood Flow Restriction on Strength, Total Bone-free Lean Body Mass and Muscle Thickness in Postmenopausal Women. Clin. Physiol. Funct. Imaging. 2013, 33, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Vechin, F.C.; Libardi, C.A.; Conceição, M.S.; Damas, F.R.; Lixandrão, M.E.; Berton, R.P.; Tricoli, V.A.; Roschel, H.A.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.; et al. Comparision between Low-Intensity Resistance Training with Blood Flow Restriction and High-Intensity Resistance Training on Quadriceps Muscle Mass and Strength in Elderly. J. Strength Cond. Res. 2015, 29, 1071–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuda, T.; Fukumura, K.; Uchida, Y.; Koshi, H.; Iida, H.; Masamune, K.; Yamasoba, T.; Sato, Y.; Nakajima, T. Effects of Low-Load, Elastic Band Resistance Training Combined with Blood Flow Restriction on Muscle Size and Arterial Stiffness in Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 950–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuda, T.; Fukumura, K.; Sato, Y.; Yamasoba, T.; Nakajima, T. Effects of Detraining after Blood Flow-Restricted Low-Intensity Training on Muscle Size and Strength in Older Adults. Aging Clin. Exp. Res. 2014, 26, 561–564. [Google Scholar] [CrossRef]
- Yasuda, T.; Fukumura, K.; Iida, H.; Nakajima, T. Effects of Detraining after Blood Flow-Restricted Low-Load Elastic Band Training on Muscle Size and Arterial Stiffness in Older Women. SpringerPlus 2015, 4, 348. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, T.; Fukumura, K.; Tomaru, T.; Nakajima, T. Thigh Muscle Size and Vascular Function after Blood Flow-Restricted Elastic Band Training in Older Women. Oncotarget 2016, 7, 33595–33607. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psych. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Moodie, E.M.; Forget, M.F.; Desmarais, P.; Keezer, M.R.; Wolfson, C. Health Heterogeneity in Older Adults: Exploration in the Canadian Longitudinal Study on Aging. J. Am. Geriatr. Soc. 2021, 69, 678–687. [Google Scholar] [CrossRef]
- Chmelo, E.A.; Crotts, C.I.; Newman, J.C.; Brinkley, T.E.; Lyles, M.F.; Leng, X.; Marsh, A.P.; Nicklas, B.J. Heterogeneity of Physical Function Responses to Exercise Training in Older Adults. J. Am. Geriatr. Soc. 2015, 63, 462–469. [Google Scholar] [CrossRef]
- Patterson, S.D.; Hughes, L.; Warmington, S.; Burr, J.; Scott, B.R.; Owens, J.; Abe, T.; Nielsen, J.L.; Libardi, C.A.; Laurentino, G.; et al. Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Front. Physiol. 2019, 10, 533. [Google Scholar] [CrossRef]
- Baker, B.S.; Stannard, M.S.; Duren, D.L.; Cook, J.L.; Stannard, J.P. Does Blood Flow Restriction Therapy in Patients Older Than Age 50 Result in Muscle Hypertrophy, Increased Strength, or Greater Physical Function? A Systematic Review. Clin. Orthop. Relat. Res. 2020, 478, 593–606. [Google Scholar] [CrossRef]
- Centner, C.; Zdzieblik, D.; Roberts, L.; Gollhofer, A.; König, D. Effects of Blood Flow Restriction Training with Protein Supplementation on Muscle Mass and Strength in Older Men. J. Sports Sci. Med. 2019, 18, 471. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | N | Age (yrs) | Functional Status | % 1RM | Cuff (cm) | Pressure (mmHg) | Frequency (d/wk) | Duration (wk) | Protocol (st × rp) | Measurements |
|---|---|---|---|---|---|---|---|---|---|---|
| Cook et al., 2017 [27] | 36 | 69–82 | Non active and risk of functional limitation | RT: 70% LI-BFR: 30% (LE and LC) and 50% (LP) | 6 | 184 ± 25 | 2 | 12 | RT: 3 × 10 LI-BFR: 3 × 10 | CSA-MRI; MVC |
| Cook et al., 2019 [28] | 21 | 67–85 | Non active and risk of functional limitation | RT: 70% LI-BFR: 30% (LE and LC) and 50% (LP) | 6 | 184 ± 25 | 2 | 12 | RT: 3 × 10 LI-BFR: 3 × 10 | CSA-MRI; MVC; 10RM Test |
| Letieri et al., 2018 [29] | 56 | 68.8 ± 5.09 | Non active | RT: 80% BFR: 30% | Not stated | BFRH: 185 ± 5 BFRL: 105 ± 6 | 3 | 16 | RT: 3 × 6–8 LI- BFR: 1 × 30 + 3 × 15 | MVC |
| Letieri et al., 2019 [30] | 23 | 69.4 ± 5.73 | Non active | RT: 80% BFR: 30% | 13 | 80% | 3 | 16 | RT: 3 × 6–8 LI-BFR: 1 × 30 + 3 × 16 | AMM; MVC |
| Libardi et al., 2015 [31] | 25 | 64.7 ± 4.1 | Non active | RT: 80% BFR: 20% | 18 | 50% | 3 | 12 | RT: 4 × 10 LI-BFR: 1 × 30 + 3 × 15 | CSA-MRI; RM Test |
| Silva et al., 2015 [32] | 15 | 61.8 ± 6.01 | Non active | RT: 80% BFR: 30% | 18 | 80% | 2 | 12 | RT: 4 × Fail LI-BFR: 4 × Fail | RM Test |
| Thiebaud et al., 2013 [33] | 14 | 60.5 ± 3.5 | Non active | RT: 80% BFR: 30% | 18 | 80-120 | 3 | 8 | RT: 3 × 10 LI-BFR: 1 × 30 + 2 × 15 | CSA-MRI; RM Test |
| Vechin et al., 2015 [34] | 23 | 59–71 | Non active | RT: 80% BFR: 30% | 18 | 50% | 2 | 12 | RT: 4 × 10 LI-BFR: 1 × 30 + 3 × 15 | CSA-MRI; RM Test |
| Yasuda et al., 2014 (a) [35] | 17 | 61–85 | Non active | Not stated | 3 | 196 ± 18 | 2 | 12 | RT: 4 × 10 LI-BFR: 1 × 30 + 3 × 16 | CSA-MRI; MVC |
| Yasuda et al., 2014 (b) [36] | 16 | 61–78 | Non active | Not stated | Not stated | 120–270 | 2 | 12 | RT: 4 × 10 LI-BFR: 1 × 30 + 3 × 17 | CSA-MRI; 10RM Test |
| Yasuda et al., 2015 [37] | 14 | 61–85 | Non active | Not stated | Not stated | 202 ± 8 | 2 | 12 | RT: 4 × 10 LI-BFR: 1 × 30 + 3 × 18 | CSA-MRI; MVC |
| Yasuda et al., 2016 [38] | 30 | 61–86 | Non active | Not stated | 5 | 160–200 | 2 | 12 | RT: 3 × 12 LI-BFR: 1 × 30 + 3 × 15 | CSA-MRI; MVC |
| Study ID | Population | Intervention | Comparison | Outcome | ||
|---|---|---|---|---|---|---|
| LI-BFR (Mean/PI ± SD) | RT (Mean/PI ± SD) | CON (Mean/PI ± SD) | ||||
| Cook et al. (2017) - United States | 36 elderly males and females non-active and risk of functional limitation with ages between 69 and 82 years | LI-BFR (n = 12) | RT and stretching (CON): RT (n = 12) CON (n = 12) | LE (RM-kg): 9.1, 95% CI [5, 13.2] p < 0.01 LC (RM-kg): 5.4, 95% CI [0.5, 10.2] p < 0.01 LP (RM-kg): 18.7, 95% CI [9.0, 28.4] p < 0.01 MVC (Nm): 11.2, 95% CI [-2.7, 25] p = 0.14 CSA (cm2): 3.23, 95% CI [1.29, 5.16] p < 0.01 | LE (RM-kg): 21.2, 95% CI [13, 29.5] p < 0.01 LC (RM-kg): 8.2, 95% CI [5.4, 11.1] p < 0.01 LP (RM-kg): 31.7, 95% CI [13.6, 50] p < 0.01 MVC (Nm): 19.3, 95% CI [8.3, 30.3] p = 0.14 CSA (cm2): 2.86, 95% CI [1.87, 3.86] p < 0.01 | LE (RM-kg): 0.6, 95% CI [−4.2, 5.3] p < 0.01 LC (RM-kg): 0.4, 95% CI [−1, 1.8] p < 0.01 LP (RM-kg): −0.2, 95% CI [−10.4, 10.1] p < 0.01 MVC (Nm): 3.5, 95% CI [−7.3, 14.3] p = 0.14 CSA (cm2): 0.07, 95% CI [−0.67, 0.82] p < 0.01 |
| Letieri et al. (2019) - Brazil | 56 elderly females non-active with ages between 63 and 74 years | LI-BFR (n = 11) | RT (n = 12) | HG (kg): 23.02 ± 3.2, p = 0.432 | HG (kg): 23.04 ± 5.97, p = 0.432 | No control group |
| Libardi et al. (2015) - Brazil | 25 elderly males and females non-active with ages between 60 and 69 years | LI-BFR (n = 10) | RT and other unspecified (CON): RT (n = 8) CON (n = 7) | Percent increase (PI) Strength (RM-kg): 35.4%, p = 0.001 CSA (cm2): 7.6%, p < 0.0001 | Percent increase (PI) Strength (RM-kg): 38.1%, p < 0.001 CSA (cm2): 7.3%, p < 0.0001 | Percent increase (PI) Strength (RM-kg): −4.3%, p > 0.05 CSA (cm2): −2.2%, p > 0.05 |
| Yasuda et al. (2014) (a) - Japan | 17 elderly males and females non-active with ages between 61 and 85 years | LI-BFR (n = 9) | RT (n = 8) | Percent increase (PI) EF (MVC-Nm): 7.8%, p = 0.0082 EE (MVC-Nm): 16.1%, p = 0.0131 EF (CSA-cm2): 17.6%, p < 0.0001 EE (CSA-cm2): 17.4%, p = 0.0131 | Percent increase (PI) EF (MVC-Nm): No changes EE (MVC-Nm): No changes EF (CSA-cm2): No changes EE (CSA-cm2): No changes | No control group |
| Yasuda et al. (2014) (b) - Japan | 16 elderly males and females non- active with ages between 61 and 78 years | LI-BFR (n = 8) | RT (n = 8) | LE (RM-kg): 66 ± 27, p < 0.01 LP (RM-kg): 191 ± 60, p < 0.01 QD (CSA-cm2): 49.1 ± 9.6, p < 0.01 AD (CSA-cm2): 24.2 ± 8.4, p > 0.05 HM (CSA-cm2): 22.1 ± 4.8, p > 0.05 GM (CSA-cm2): 40.8 ± 7, p = 0.07 | LE (RM-kg): 63 ± 24, p > 0.05 LP (RM-kg): 158 ± 44, p > 0.05 QD (CSA-cm2): 44.7 ± 8.9, p > 0.05 AD (CSA-cm2): 20.8 ± 3.6, p > 0.05 HM (CSA-cm2): 20.8 ± 3.6, p > 0.05 GM (CSA-cm2): 36.5 ± 7.7, p > 0.05 | No control group |
| Yasuda et al. (2016) - Japan | 30 elderly females non- active with ages between 61 and 86 years | LI-BFR (n = 10) | RT and other unspecified (CON): RT (n = 10) CON (n = 10) | Percent increase (PI) Strength (RM-kg): 16.4%, p < 0.001 Strength (MVC-Nm): 13.7%, p = 0.028 CSA (cm2): 6.9%, p < 0.001 | Percent increase (PI) Strength (RM-kg): 17.6%, p < 0.001 Strength (MVC-Nm): No changes, p = 0.196 CSA (cm2): 1.5%, p = 0.871 | Percent increase (PI) Strength (RM-kg): No changes p = 0.912 Strength (MVC-Nm): No changes, p = 0.810 CSA (cm2): −2.2%, p = 0.395 |
| Resistance Training with Blood Blow Restriction Versus Resistance Training Alone | |||||
|---|---|---|---|---|---|
| Population: Non-Active older adults Intervention: resistance training with blood flow restriction Comparison: resistance training Setting: laboratory | |||||
| Outcomes | Relative Effect (95% CI) | Anticipated Absolute Effect * (95% CI) | N° of Participants (Studies) | Certainty of the Evidence (Grade) | |
| Assumed Risk with Control | Assumed Risk with Intervention | ||||
| Muscular strength (RM Test) Up to 12 weeks | SMD 0.07 * (−0.25 to 0.40) | 21.7 to 266 | Mean strength in intervention was 0.07 higher (0.25 lower to 0.40 higher) | 148 (4 RCTs) | ⨁◯◯◯ VERY LOW 1,2 |
| Muscular strength-Leg press (RM Test) Up to 12 weeks | SMD 0.01 * (−0.77 to 0.78) | 37.37 to 112.2 | Mean strength in intervention was 0.01 higher (0.77 lower to 0.78 higher) | 26 (2 RCTs) | ⨁◯◯◯ VERY LOW 1,2 |
| Muscular strength-Knee extension (RM Test) Up to 12 weeks | SMD 0.08 * (−0.60 to 0.75) | 21.7 to 60.5 | Mean strength in intervention was 0.08 higher (0.60 lower to 0.75 higher) | 63 (3 RCT) | ⨁◯◯◯ VERY LOW 1,2 |
| Muscular strength-Knee flexion (RM Test) Up to 12 weeks | SMD 0.12 * (−0.42 to 0.67) | 23.1 to 34.8 | Mean strength in intervention was 0.12 higher (0.42 lower to 0.67 higher) | 53 (2 RCTs) | ⨁◯◯◯ VERY LOW 2,3 |
| Resistance Training with Blood Blow Restriction Versus Resistance Training | |||||
|---|---|---|---|---|---|
| Population: Non-active older adults Intervention: resistance training with blood flow restriction Comparison: resistance training Setting: laboratory | |||||
| Outcomes | Relative Effect (95% CI) | Anticipated Absolute Effect * (95% CI) | N° of Participants (Studies) | Certainty of the Evidence (Grade) | |
| Assumed Risk with Control | Assumed Risk with Intervention | ||||
| Muscular strength (MVC test) Up to 16 weeks | SMD 0.61 * (0.10 to 1.11) | 54.61 to 126 | Mean strength in intervention was 0.61 higher (0.10 lower to 1.11 higher) | 246 (3 RCTs) | ⨁◯◯◯ VERY LOW 1,2 |
| Muscular strength-Knee extension (MVC test) Up to 16 weeks | SMD 0.65 * (0.00 to 1.29) | 85.88 to 126 | Mean strength in intervention was 0.65 higher (0.00 lower to 1.29 higher) | 109 (2 RCTs) | ⨁◯◯◯ VERY LOW 1,2 |
| Muscular strength-Knee flexion (MVC test) Up to 16 weeks | SMD 0.53 * (−0.55 to 1.61) | 85.88 to 126 | Mean strength in intervention was 0.53 higher (0.55 lower to 1.61 higher) | 109 (2 RCTs) | ⨁◯◯◯ VERY LOW 1,2 |
| Resistance Training with Blood Blow Restriction Versus Resistance Training | |||||
|---|---|---|---|---|---|
| Population: Non-active older adults Intervention: resistance training with blood flow restriction Comparison: resistance training Setting: laboratory | |||||
| Outcomes | Relative Effect (95% CI) | Anticipated Absolute Effect * (95% CI) | N° of Participants (Studies) | Certainty of the Evidence (Grade) | |
| Assumed Risk with Control | Assumed Risk with Intervention | ||||
| Muscle mass (cm2) Up to 12 weeks | SMD 0.62 * (−0.09 to 1.34) | 10.7 to 61.7 | Mean strength in intervention was 0.62 higher (0.09 lower to 1.34 higher) | 86 (3 RCTs) | ⨁◯◯◯ VERY LOW 1,2,3 |
| Muscle mass knee extensors (cm2) Up to 12 weeks | SMD 0.26 * (−0.39 to 0.91) | 47.7 to 61.7 | Mean strength in intervention was 0.26 higher (0.39 lower to 0.91 higher) | 37 (2 RCTs) | ⨁◯◯◯ VERY LOW 1,3 |
| Muscle mass knee flexors (cm2) Up to 12 weeks | SMD −0.20 * (−1.06 to 0.66) | 23.5 | Mean strength in intervention was −0.20 higher (−1.06 lower to 0.66 higher) | 21 (1 RCTs) | ⨁◯◯◯ VERY LOW 1,3 |
| Muscle mass elbow flexors and extensors (cm2) Up to 12 weeks | SMD 1.65 * (0.75 to 2.54) | 10.7 to 12 | Mean strength in intervention was 1.65 higher (0.75 lower to 2.54 higher) | 28 (1 RCTs) | ⨁◯◯◯ VERY LOW 1,3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigo-Mallorca, D.; Loaiza-Betancur, A.F.; Monteagudo, P.; Blasco-Lafarga, C.; Chulvi-Medrano, I. Resistance Training with Blood Flow Restriction Compared to Traditional Resistance Training on Strength and Muscle Mass in Non-Active Older Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11441. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111441
Rodrigo-Mallorca D, Loaiza-Betancur AF, Monteagudo P, Blasco-Lafarga C, Chulvi-Medrano I. Resistance Training with Blood Flow Restriction Compared to Traditional Resistance Training on Strength and Muscle Mass in Non-Active Older Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(21):11441. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111441
Chicago/Turabian StyleRodrigo-Mallorca, Darío, Andrés Felipe Loaiza-Betancur, Pablo Monteagudo, Cristina Blasco-Lafarga, and Iván Chulvi-Medrano. 2021. "Resistance Training with Blood Flow Restriction Compared to Traditional Resistance Training on Strength and Muscle Mass in Non-Active Older Adults: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 21: 11441. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111441