
Smoking Cessation Apps: A Systematic Review of Format, Outcomes, and Features

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection Criteria
2.2.1. Study Characteristics
2.2.2. Participants
2.2.3. Type of Intervention
2.2.4. Exclusion Criteria
2.3. Outcomes
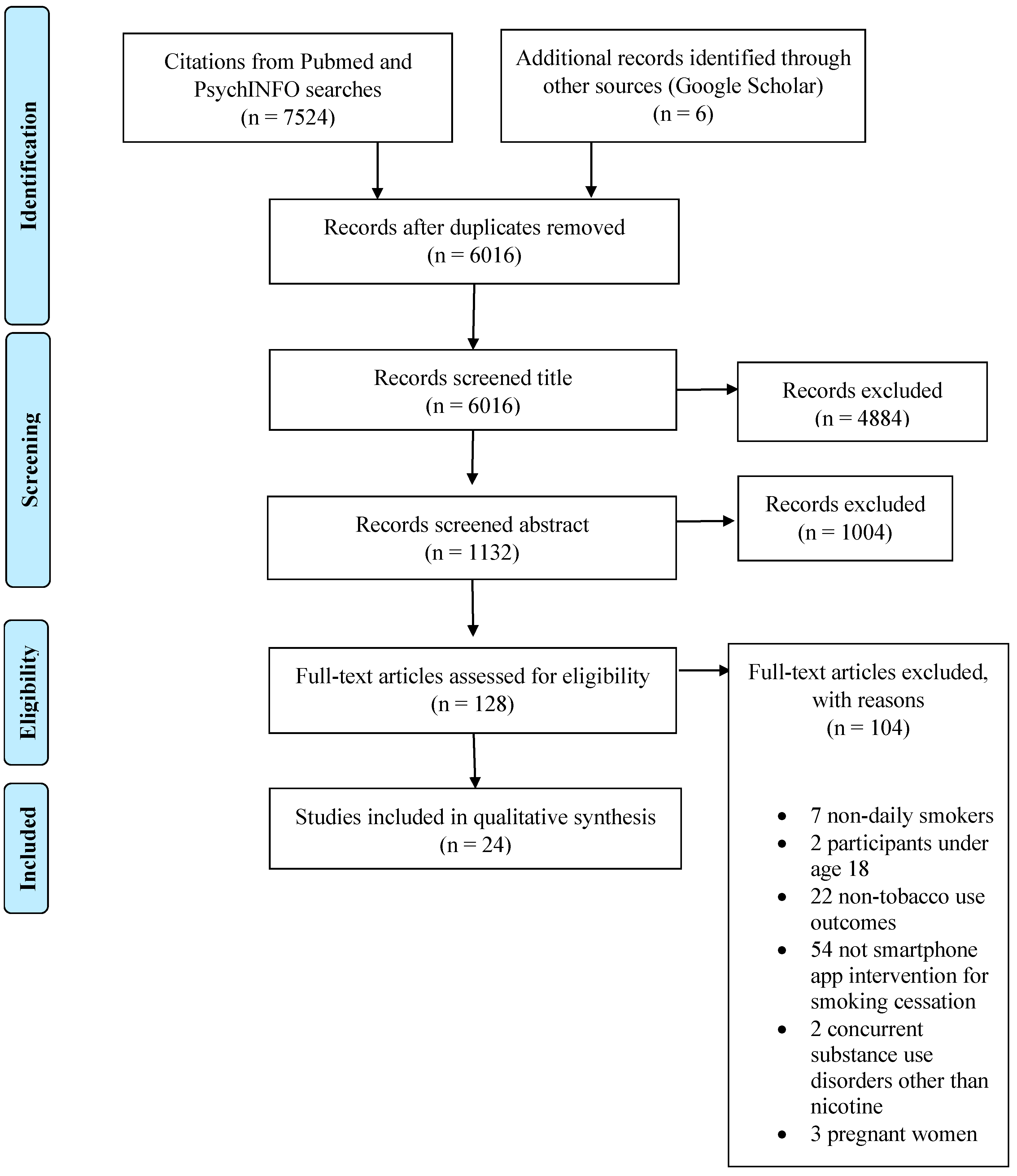
2.4. Study Selection
2.5. Data Extraction and Analysis
2.6. Assessment of Risk of Bias
3. Results
3.1. Study Characteristics
3.2. Methodological Quality Assessment

{kind=link}
{kind=link}
{kind=link}
| Selection Bias | Study Design | Confounders | Blinding | Data Collection | Withdrawals | Global Rating | |
|---|---|---|---|---|---|---|---|
| Baskerville et al. (2018) [55] | Strong | Strong | Strong | Strong | Strong | Weak | Moderate |
| BinDhim et al. (2018) [32] | Strong | Strong | Strong | Strong | Strong | Strong | Strong |
| Bricker et al. (2014) [33] | Strong | Strong | Strong | Strong | Strong | Strong | Strong |
| Bricker et al. (2017) [38] | Moderate | Moderate | Weak | Moderate | Strong | Strong | Moderate |
| Buller et al. (2014) [44] | Moderate | Strong | Strong | Strong | Strong | Moderate | Strong |
| Businelle et al. (2016) [39] | Moderate | Moderate | Weak | Moderate | Strong | Moderate | Moderate |
| Carpenter et al. (2015) [40] | Weak | Moderate | Weak | Moderate | Strong | Moderate | Weak |
| Dan et al. (2016) [54] | Moderate | Moderate | Weak | Moderate | Strong | Moderate | Moderate |
| Dar (2017) [34] | Moderate | Moderate | Weak | Moderate | Strong | Strong | Moderate |
| Garrison et al. (2020) [47] | Weak | Strong | Weak | Strong | Strong | Weak | Weak |
| Hébert et al. (2020) [41] | Strong | Strong | Strong | Moderate | Strong | Moderate | Strong |
| Hertzberg et al. (2013) [35] | Weak | Strong | Strong | Moderate | Strong | Strong | Moderate |
| Hicks et al. (2017) [36] | Weak | Strong | Weak | Moderate | Strong | Weak | Weak |
| Iacoviello et al. (2017) [43] | Strong | Moderate | Weak | Moderate | Strong | Strong | Moderate |
| Janes et al. (2019) [49] | Weak | Strong | Strong | Strong | Strong | Strong | Moderate |
| Krishnan et al. (2019) [37] | Strong | Strong | Weak | Moderate | Strong | Moderate | Moderate |
| Marler et al. (2019) [42] | Weak | Moderate | Weak | Moderate | Strong | Strong | Weak |
| Masaki et al. (2019) [50] | Strong | Moderate | Weak | Moderate | Strong | Strong | Moderate |
| Masaki et al. (2020) [46] | Moderate | Strong | Strong | Moderate | Strong | Strong | Strong |
| McClure et al. (2018) [51] | Moderate | Moderate | Weak | Moderate | Strong | Strong | Moderate |
| Minami et al. (2018) [52] | Strong | Moderate | Weak | Moderate | Strong | Strong | Moderate |
| O’Connor et al. (2020) [45] | Strong | Strong | Strong | Moderate | Strong | Strong | Strong |
| Raiff et al. (2017) [48] | Weak | Moderate | Weak | Moderate | Strong | Weak | Weak |
| Wilson et al. (2019) [53] | Moderate | Moderate | Weak | Moderate | Strong | Moderate | Moderate |
3.3. Effects of Smartphone Apps on Abstinence, Tobacco Use, and Relapse Rates
3.3.1. General Apps for Smoking Cessation (GSC-Apps)
3.3.2. Combine Apps with Face-to-Face Contact (FFSC-Apps)
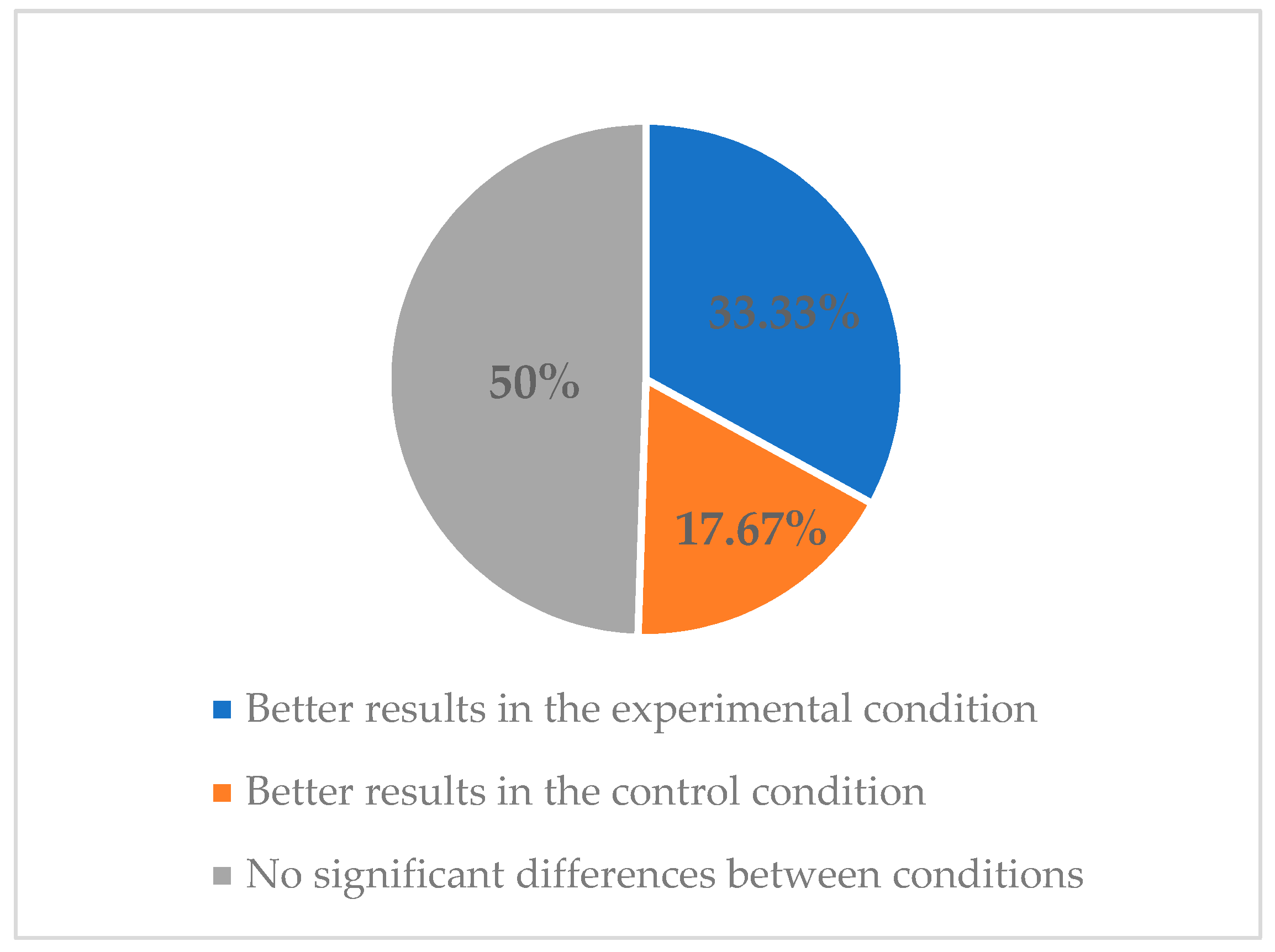
3.4. Effects of Smartphone Apps on Abstinence, Tobacco Use, and Relapse Rates Regarding the Methodological Quality of the Studies
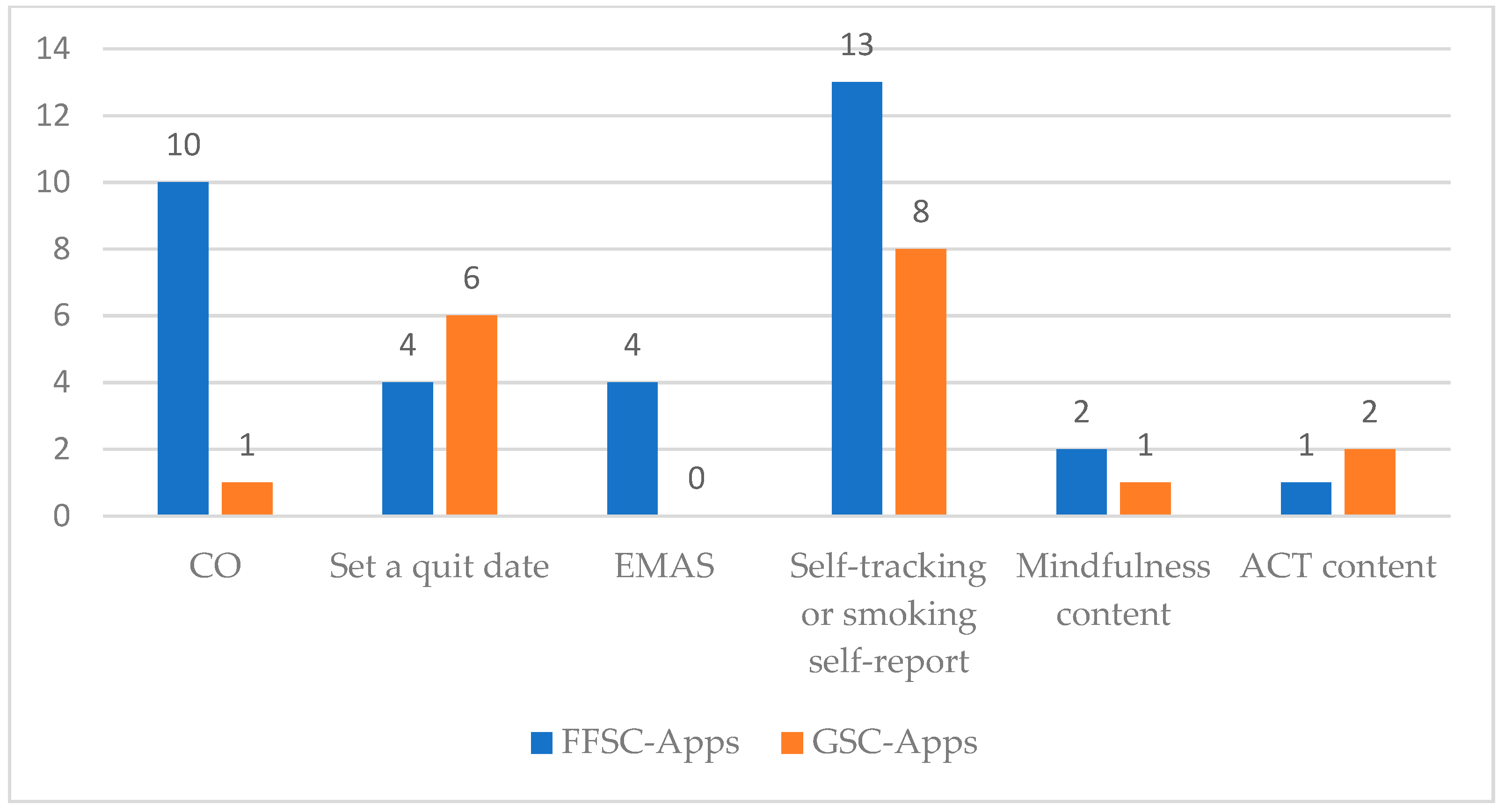
3.5. Features of Smartphone Apps for Smoking Cessation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). Current Cigarette Smoking Among Adults in the United States. 2021. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm (accessed on 1 March 2021).
- Talhout, R.; Schulz, T.; Florek, E.; Van Benthem, J.; Wester, P.; Opperhuizen, A. Hazardous Compounds in tobacco smoke. Int. J. Environ. Res. Public. Health 2011, 8, 613–628. [Google Scholar] [CrossRef] [PubMed]
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2014.
- World Health Organization (WHO). WHO Report on the Global Tobacco Epidemic, 2019: Offer Help to Quit Tobacco Use. 2020. Available online: https://apps.who.int/iris/handle/10665/326043 (accessed on 1 March 2021).
- Goldenberg, M.; Danovitch, I.; IsHak, W.W. Quality of life and smoking. Am. J. Addict. 2014, 23, 540–562. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Das, S.; Young-Wolff, K.C. Smoking, Mental Illness, and Public Health. Annu. Rev. Public Health 2017, 38, 165–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fluharty, M.; Taylor, A.E.; Grabski, M.; Munafò, M.R. The Association of Cigarette Smoking With Depression and Anxiety: A Systematic Review. Nicotine Tob. Res. 2017, 19, 3–13. [Google Scholar] [CrossRef]
- Siu, A.L. Behavioral and Pharmacotherapy Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Women: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2015, 163, 622–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, R.; Stapleton, J. Clinical and public health significance of treatments to aid smoking cessation. Eur. Respir. Rev. 2008, 17, 199–204. [Google Scholar] [CrossRef] [Green Version]
- García, M.C.; Bastian, B.; Rossen, L.M.; Anderson, R.; Miniño, A.; Yoon, P.W.; Faul, M.; Massetti, G.; Thomas, C.C.; Hong, Y.; et al. Potentially Preventable Deaths Among the Five Leading Causes of Death—United States, 2010 and 2014. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 1245–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiore, M.C.; Jaén, C.R.; Baker, T.B.; Bailey, W.C.; Benowitz, N.L.; Curry, S.J.; Dorfman, S.F.; Froelicher, E.S.; Goldstein, M.G.; Healton, C.G.; et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. 2008. Available online: https://www.ahrq.gov/prevention/guidelines/tobacco/index.html (accessed on 1 March 2021).
- World Health Organization (WHO). Global Diffusion of EHealth: Making Universal Health Coverage Achievable. Report of the Third Global Survey on EHealth. 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/252529/9789241511780-eng.pdf;jsessionid=0FDF0200A88173BE06F79C193B8E60DA?sequence=1 (accessed on 1 March 2021).
- Whittaker, R.; McRobbie, H.; Bullen, C.; Rodgers, A.; Gu, Y.; Dobson, R. Mobile phone text messaging and app-based interventions for smoking cessation. Cochrane Database Syst. Rev. 2019, 10, CD006611. [Google Scholar] [CrossRef]
- Keoleian, V.; Polcin, D.; Galloway, G.P. Text messaging for addiction: A review. J. Psychoact. Drugs 2015, 47, 158–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spohr, S.A.; Nandy, R.; Gandhiraj, D.; Vemulapalli, A.; Anne, S.; Walters, S.T. Efficacy of SMS Text Message Interventions for Smoking Cessation: A Meta-Analysis. J. Subst. Abuse Treat. 2015, 56, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Vilardaga, R.; Casellas-Pujol, E.; McClernon, J.F.; Garrison, K.A. Mobile Applications for the Treatment of Tobacco Use and Dependence. Curr. Addict. Rep. 2019, 6, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, R.; McRobbie, H.; Bullen, C.; Rodgers, A.; Gu, Y. Mobile phone-based interventions for smoking cessation. Cochrane Database Syst. Rev. 2016, 4, CD006611. [Google Scholar] [CrossRef]
- Lancaster, T.; Stead, L.F. Individual behavioural counselling for smoking cessation. Cochrane Database Syst. Rev. 2017, 3, CD001292. [Google Scholar] [CrossRef] [PubMed]
- Nohlert, E.; Tegelberg, Å.; Tillgren, P.; Johansson, P.; Rosenblad, A.; Helgason, Á.R. Comparison of a high and a low intensity smoking cessation intervention in a dentistry setting in Sweden—A randomized trial. BMC Public Health 2009, 9, 121e. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statista. Number of Smartphone Users Worldwide from 2016 to 2023. 2021. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/330695/number-of-smartphone-users-worldwide/ (accessed on 1 March 2021).
- Ditrendia. Informe Mobile en España y en el Mundo 2020. 2021. Available online: https://mktefa.ditrendia.es/informe-mobile-2020 (accessed on 1 March 2021).
- Bennett, M.E.; Toffey, K.; Dickerson, F.; Himelhoch, S.; Katsafanas, E.; Savage, C.L.G. A review of android apps for smoking cessation. J. Smok. Cessat. 2015, 10, 106–115. [Google Scholar] [CrossRef]
- Cheng, F.; Xu, J.; Su, C.; Fu, X.; Bricker, J. Content Analysis of Smartphone Apps for Smoking Cessation in China: Empirical Study. JMIR MHealth UHealth 2017, 5, e93. [Google Scholar] [CrossRef] [Green Version]
- Formagini, T.D.B.; Ervilha, R.R.; Machado, N.M.; Andrade, B.A.B.B.D.; Gomide, H.P.; Ronzani, T.M. A review of smartphone apps for smoking cessation available in Portuguese. Cad. Saúde Pública 2017, 33, e00178215. [Google Scholar] [CrossRef] [Green Version]
- Thornton, L.; Quinn, C.; Birrell, L.; Guillaumier, A.; Shaw, B.; Forbes, E.; Deady, M.; Kay-Lambkin, F. Free smoking cessation mobile apps available in Australia: A quality review and content analysis. Aust. N. Z. J. Public Health 2017, 41, 625–630. [Google Scholar] [CrossRef]
- Haskins, B.L.; Lesperance, D.; Gibbons, P.; Boudreaux, E.D. A systematic review of smartphone applications for smoking cessation. Transl. Behav. Med. 2017, 7, 292–299. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, A.H.; Funk, A.P.; Goodwin, R.D. A review of epidemiologic research on smoking behavior among persons with alcohol and illicit substance use disorders. Prev. Med. 2016, 92, 148–159. [Google Scholar] [CrossRef] [Green Version]
- Herbec, A.; Beard, E.; Brown, J.; Gardner, B.; Tombor, I.; West, R. The needs and preferences of pregnant smokers regarding tailored Internet-based smoking cessation interventions: A qualitative interview study. BMC Public Health 2014, 14, 1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, J.; Dinnes, J.; D’Amico, R.; Sowden, A.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, 1517–1518. [Google Scholar] [CrossRef] [Green Version]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- BinDhim, N.F.; McGeechan, K.; Trevena, L. Smartphone Smoking Cessation Application (SSC App) trial: A multicountry double-blind automated randomised controlled trial of a smoking cessation decision-aid “app”. BMJ Open 2018, 8, e017105. [Google Scholar] [CrossRef]
- Bricker, J.B.; Mull, K.E.; Kientz, J.A.; Vilardaga, R.; Mercer, L.D.; Akioka, K.J.; Heffner, J.L. Randomized, controlled pilot trial of a smartphone app for smoking cessation using acceptance and commitment therapy. Drug Alcohol Depend. 2014, 143, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Dar, R. Effect of Real-Time Monitoring and Notification of Smoking Episodes on Smoking Reduction: A Pilot Study of a Novel Smoking Cessation App. Nicotine Tob. Res. 2018, 20, 1515–1518. [Google Scholar] [CrossRef] [PubMed]
- Hertzberg, J.S.; Carpenter, V.L.; Kirby, A.C.; Calhoun, P.S.; Moore, S.D.; Dennis, M.F.; Dennis, P.A.; Dedert, E.A.; Beckham, J.C. Mobile contingency management as an adjunctive smoking cessation treatment for smokers with posttraumatic stress disorder. Nicotine Tob. Res. 2013, 15, 1934–1938. [Google Scholar] [CrossRef] [Green Version]
- Hicks, T.A.; Thomas, S.P.; Wilson, S.M.; Calhoun, P.S.; Kuhn, E.R.; Beckham, J.C. A preliminary investigation of a relapse prevention mobile application to maintain smoking abstinence among individuals with posttraumatic stress disorder. J. Dual Diagn. 2017, 13, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, N.; Elf, J.L.; Chon, S.; Golub, J.E. COach2Quit: A Pilot Randomized Controlled Trial of a Personal Carbon Monoxide Monitor for Smoking Cessation. Nicotine Tob. Res. 2019, 21, 1573–1577. [Google Scholar] [CrossRef]
- Bricker, J.B.; Copeland, W.; Mull, K.E.; Zeng, E.Y.; Watson, N.L.; Akioka, K.J.; Heffner, J.L. Single-arm trial of the second version of an acceptance & commitment therapy smartphone application for smoking cessation. Drug Alcohol Depend. 2017, 170, 37–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Businelle, M.S.; Ma, P.; Kendzor, D.E.; Frank, S.G.; Vidrine, D.J.; Wetter, D.W. An Ecological Momentary Intervention for Smoking Cessation: Evaluation of Feasibility and Effectiveness. J. Med. Internet Res. 2016, 18, e321. [Google Scholar] [CrossRef]
- Carpenter, V.L.; Hertzberg, J.S.; Kirby, A.C.; Calhoun, P.S.; Moore, S.D.; Dennis, M.F.; Dennis, P.A.; Dedert, E.A.; Hair, L.P.; Beckham, J.C. Multicomponent smoking cessation treatment including mobile contingency management in homeless veterans. J. Clin. Psychiatry 2015, 76, 959–964. [Google Scholar] [CrossRef]
- Hébert, E.T.; Ra, C.K.; Alexander, A.C.; Helt, A.; Moisiuc, R.; Kendzor, D.E.; Vidrine, D.J.; Funk-Lawler, R.K.; Businelle, M.S. A Mobile Just-in-Time Adaptive Intervention for Smoking Cessation: Pilot Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e16907. [Google Scholar] [CrossRef] [PubMed]
- Marler, J.D.; Fujii, C.A.; Utley, D.S.; Tesfamariam, L.J.; Galanko, J.A.; Patrick, H. Initial Assessment of a Comprehensive Digital Smoking Cessation Program that Incorporates a Mobile App, Breath Sensor, and Coaching: Cohort Study. JMIR MHealth UHealth 2019, 7, e12609. [Google Scholar] [CrossRef]
- Iacoviello, B.M.; Steinerman, J.R.; Klein, D.B.; Silver, T.L.; Berger, A.G.; Luo, S.X.; Schork, N.J. Clickotine, A Personalized Smartphone App for Smoking Cessation: Initial Evaluation. JMIR MHealth UHealth 2017, 5, e56. [Google Scholar] [CrossRef]
- Buller, D.B.; Borland, R.; Bettinghaus, E.P.; Shane, J.H.; Zimmerman, D.E. Randomized trial of a smartphone mobile application compared to text messaging to support smoking cessation. Telemed. e-Health 2014, 20, 206–214. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, M.; Whelan, R.; Bricker, J.; McHugh, L. Randomized Controlled Trial of a Smartphone Application as an Adjunct to Acceptance and Commitment Therapy for Smoking Cessation. Behav. Ther. 2020, 51, 162–177. [Google Scholar] [CrossRef] [PubMed]
- Masaki, K.; Tateno, H.; Nomura, A.; Muto, T.; Suzuki, S.; Satake, K.; Hida, E.; Fukunaga, K. A Randomized Controlled Trial of a Smoking Cessation Smartphone Application with a Carbon Monoxide Checker. Npj Digit. Med. 2020, 3, 35. [Google Scholar] [CrossRef]
- Garrison, K.A.; Pal, P.; O’Malley, S.S.; Pittman, B.P.; Gueorguieva, R.; Rojiani, R.; Scheinost, D.; Dallery, J.; Brewer, J.A. Craving to Quit: A Randomized Controlled Trial of Smartphone App-Based Mindfulness Training for Smoking Cessation. Nicotine Tob. Res. 2020, 22, 324–331. [Google Scholar] [CrossRef]
- Raiff, B.R.; Arena, A.; Meredith, S.E.; Grabinksi, M.J. Feasibility of a mobile group financial-incentives intervention among pairs of smokers with a prior social relationship. Psychol. Rec. 2017, 67, 231–239. [Google Scholar] [CrossRef]
- Janes, A.C.; Datko, M.; Roy, A.; Barton, B.; Druker, S.; Neal, C.; Ohashi, K.; Benoit, H.; van Lutterveld, R.; Brewer, J.A. Quitting starts in the brain: A randomized controlled trial of app-based mindfulness shows decreases in neural responses to smoking cues that predict reductions in smoking. Neuropsychopharmacology 2019, 44, 1631–1638. [Google Scholar] [CrossRef]
- Masaki, K.; Tateno, H.; Kameyama, N.; Morino, E.; Watanabe, R.; Sekine, K.; Ono, T.; Satake, K.; Suzuki, S.; Nomura, A.; et al. Impact of a Novel Smartphone App (CureApp Smoking Cessation) on Nicotine Dependence: Prospective Single-Arm Interventional Pilot Study. JMIR MHealth UHealth 2019, 7, e12694. [Google Scholar] [CrossRef]
- McClure, E.A.; Tomko, R.L.; Carpenter, M.J.; Treiber, F.A.; Gray, K.M. Acceptability and compliance with a remote monitoring system to track smoking and abstinence among young smokers. Am. J. Drug Alcohol Abuse 2018, 44, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Minami, H.; Brinkman, H.R.; Nahvi, S.; Arnsten, J.H.; Rivera-Mindt, M.; Wetter, D.W.; Bloom, E.L.; Price, L.H.; Vieira, C.; Donnelly, R.; et al. Rationale, design and pilot feasibility results of a smartphone-assisted, mindfulness-based intervention for smokers with mood disorders: Project mSMART MIND. Contemp. Clin. Trials 2018, 66, 36–44. [Google Scholar] [CrossRef]
- Wilson, S.M.; Thompson, A.C.; Currence, E.D.; Thomas, S.P.; Dedert, E.A.; Kirby, A.C.; Elbogen, E.B.; Moore, S.D.; Calhoun, P.S.; Beckham, J.C. Patient-informed treatment development of behavioral smoking cessation for people with schizophrenia. Behav. Ther. 2019, 50, 395–409. [Google Scholar] [CrossRef] [PubMed]
- Dan, M.; Grabinski, M.J.; Raiff, B.R. Smartphone-based contingency management for smoking cessation with smokers diagnosed with attention-deficit/hyperactivity disorder. Transl. Issues Psychol. Sci. 2016, 2, 116–127. [Google Scholar] [CrossRef] [Green Version]
- Baskerville, N.B.; Struik, L.L.; Guindon, G.E.; Norman, C.D.; Whittaker, R.; Burns, C.; Hammond, D.; Dash, D.; Brown, K.S. Effect of a Mobile Phone Intervention on Quitting Smoking in a Young Adult Population of Smokers: Randomized Controlled Trial. JMIR MHealth UHealth 2018, 6, e10893. [Google Scholar] [CrossRef]
- Patnode, C.D.; Henderson, J.T.; Melnikow, J.; Coppola, E.L.; Durbin, S.; Thomas, R. Interventions for Tobacco Cessation in Adults, Including Pregnant Women: An Evidence Update for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2021; pp. 1–266. [Google Scholar]
- Burgess, E.S.; Brown, R.A.; Kahler, C.W.; Niaura, R.; Abrams, D.B.; Goldstein, M.G.; Miller, I.W. Patterns of change in depressive symptoms during smoking cessation: Who’s at risk for relapse? J. Consult. Clin. Psychol. 2002, 70, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Kearns, N.T.; Carl, E.; Stein, A.T.; Vujanovic, A.A.; Zvolensky, M.J.; Smits, J.A.J.; Powers, M.B. Posttraumatic stress disorder and cigarette smoking: A systematic review. Depress. Anxiety 2018, 35, 1056–1072. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.H.; Mazure, C.M.; McKee, S.A. Smoking and mental illness in the US population. Tob. Control 2014, 23, e147–e153. [Google Scholar] [CrossRef]
- Tsai, J.; Rosenheck, R.A. Smoking Among Chronically Homeless Adults: Prevalence and Correlates. Psychiatr. Serv. 2012, 63, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Reid, J.L.; Hammond, D.; Boudreau, C.; Fong, G.T.; Siahpush, M.; ITC Collaboration. Socioeconomic disparities in quit intentions, quit attempts, and smoking abstinence among smokers in four western countries: Findings from the International Tobacco Control Four Country Survey. Nicotine Tob. Res. 2010, 12, S20–S33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donny, E.C.; Griffin, K.M.; Shiffman, S.; Sayette, M.A. The relationship between cigarette use, nicotine dependence, and craving in laboratory volunteers. Nicotine Tob. Res. 2008, 10, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Snell, M.; Harless, D.; Shin, S.; Cunningham, P.; Barnes, A. A longitudinal assessment of nicotine dependence, mental health, and attempts to quit smoking: Evidence from waves 1–4 of the Population Assessment of Tobacco and Health (PATH) study. Addict. Behav. 2021, 115, 106787. [Google Scholar] [CrossRef] [PubMed]
- Vangeli, E.; Stapleton, J.; Smit, E.S.; Borland, R.; West, R. Predictors of attempts to stop smoking and their success in adult general population samples: A systematic review. Addiction 2011, 106, 2110–2121. [Google Scholar] [CrossRef] [PubMed]
- Falomir-Pichastor, J.M.; Blondé, J.; Desrichard, O.; Felder, M.; Riedo, G.; Folly, L. Tobacco dependence and smoking cessation: The mediating role of smoker and ex-smoker self-concepts. Addict. Behav. 2020, 102, 106200. [Google Scholar] [CrossRef] [PubMed]
- Chu, K.H.; Matheny, S.J.; Escobar-Viera, C.G.; Wessel, C.; Notier, A.E.; Davis, E.M. Smartphone health apps for tobacco Cessation: A systematic review. Addict. Behav. 2021, 112, 106616. [Google Scholar] [CrossRef]
- Dorner, T.E.; Tröstl, A.; Womastek, I.; Groman, E. Predictors of Short-Term Success in Smoking Cessation in Relation to Attendance at a Smoking Cessation Program. Nicotine Tob. Res. 2011, 13, 1068–1075. [Google Scholar] [CrossRef]
- Garey, L.; Rogers, A.H.; Manning, K.; Smit, T.; Derrick, J.L.; Viana, A.G.; Schmidt, N.B.; Zvolensky, M.J. Effects of smoking cessation treatment attendance on abstinence: The moderating role of psychologically based behavioral health conditions. J. Subst. Abuse Treat. 2020, 109, 1–7. [Google Scholar] [CrossRef]
- The IQVIA Institute. The Growing Value of Digital Health. Evidence and Impact on Human Health and the Healthcare System. 2017. Available online: https://www.iqvia.com/insights/the-iqvia-institute/reports/the-growing-value-of-digital-health (accessed on 2 March 2021).
- Cobos-Campos, R.; Mar, J.; Apiñaniz, A.; de Lafuente, A.S.; Parraza, N.; Aizpuru, F.; Orive, G. Cost-effectiveness analysis of text messaging to support health advice for smoking cessation. Cost. Eff. Resour. Alloc. 2021, 19, 9. [Google Scholar] [CrossRef] [PubMed]
- Guerriero, C.; Cairns, J.; Roberts, I.; Rodgers, A.; Whittaker, R.; Free, C. The cost-effectiveness of smoking cessation support delivered by mobile phone text messaging: Txt2stop. Eur. J. Health Econ. 2013, 14, 789–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatzipavlou, I.A.; Christoforidou, S.A.; Vlachopoulou, M. A recommended guideline for the development of mHealth Apps. mHealth 2016, 2, 21. [Google Scholar] [CrossRef] [Green Version]
- Llorens-Vernet, P.; Miró, J. Standards for Mobile Health–Related Apps: Systematic Review and Development of a Guide. JMIR MHealth UHealth 2020, 8, e13057. [Google Scholar] [CrossRef] [PubMed]



| General Smartphone Apps | |||
|---|---|---|---|
| Author | Abstinence | Tobacco Use | Relapse Rates |
| Baskerville et al. (2018) [55] | Significant differences between conditions at 6 months point-assessment in favor of the control group (22.3% vs. 18.3%). | Nonsignificant differences in CPD at 6-month point-assessment between conditions. | Not reported. |
| BinDhim et al. (2018) [32] | Significant differences between conditions in continuous abstinence rates at 10-days (32.2% vs. 20.8%), 1- (28.5% vs. 16.9%), 3- (23.8% vs. 10.2), and 6-month point-assessments (10.2% vs. 4.8%) in favor of the experimental group. | Not reported. | Not reported. |
| Bricker et al. (2014) [33] | Nonsignificant differences between conditions at 2-month post-enrollment point-assessment (13% experimental vs. 8% control). | Not reported. | Not reported. |
| Bricker et al. (2017) [38] | 21% for 7-day PPA and 11% for 30-day PPA at 2-month-post-enrollment point-assessment. | 75% reduction rate of CPD at 2-month point-assessment. | Not reported. |
| Buller et al. (2014) [44] | Significant differences between conditions at 6-week point-assessment in favor of the control group (58% vs. 30%). | Not reported. | Not reported. |
| Dar (2017) [34] | Not reported. | Significant differences in CPD reduction between conditions in favor of the experimental group at the end of the study. | Not reported. |
| Garrison et al. (2020) [47] | Nonsignificant differences between conditions at 6-month point-assessment (9.8% experimental vs. 12.1% control). | Nonsignificant differences between conditions in CPD reduction. Significant reductions in CPD from baseline to the 6-month point-assessment. | Not reported. |
| Iacoviello et al. (2017) [43] | 45.2% for 7-day PPA and 26.2% for 30-day PPA at the end of the study. | Not reported. | Not reported. |
| Marler et al. (2019) [42] | 32.0% for 7-day PPA and 27.6% for 30-day PPA at the end of the study. | Nonabstinent participants reduced 29.1% in CPD at the end of the study. | Not reported. |
| Combine apps with face-to-face contact | |||
| Author | Abstinence | Tobacco use | Relapse rates |
| Businelle et al. (2016) [39] | 41% at quit date, 17% at 1-week, 31% at 2-week, 27% at 3-week, 22% at 4-week, and 20% at 12-week point-assessment. | Not reported. | Not reported. |
| Carpenter et al. (2015) [40] | 50% at 4 weeks. Of these, 65% at 3-months and 60% at 6-months point-assessment remained abstinent. | Not reported. | Not reported. |
| Dan et al. (2016) [54] | 3% at baseline, 42% at tapering, 55% at treatment, and 42% at thinning. 0% at 1-week follow-up were abstinent. | Not reported. | Not reported. |
| Hébert et al. (2020) [41] | Nonsignificant differences between conditions. 22% Smart-T2, 26% QuitGuide, 30% usual care at 4 weeks point-assessment. 22% Smart-T2, 15% QuitGuide, 15% usual care at 12-weeks point-assessment. | Not reported. | Not reported. |
| Hertzberg et al. (2013) [35] | Nonsignificant differences between conditions at 4-week point-assessment (82% experimental vs. 45% control). | Not reported. | Not reported. |
| Hicks et al. (2017) [36] | Nonsignificant differences between conditions at post-treatment (60% experimental vs. 100% control) and at 2-week point-assessment (60% experimental vs. 67% control). | Not reported. | Not reported. |
| Janes et al. (2019) [49] | Not reported. | Nonsignificant differences between conditions in CPD reduction. Significant reductions in CPD from baseline to 1-month follow-up under both conditions. | Not reported. |
| Krishnan et al. (2019) [37] | Nonsignificant differences between conditions at 30-day point-assessment (3% experimental vs. 2% control). | Nonsignificant differences in CPD between baseline and 30-day point-assessment. | Not reported. |
| Masaki et al. (2019) [50] | 64% from weeks 9 to 24, 76% from weeks 9 to 12, and 58% from 9 to 52 weeks in continuous abstinence rate. | Not reported. | Not reported. |
| Masaki et al. (2020) [46] | Significant differences between conditions in continuous abstinence rates from weeks 9 to 12 (75.4% vs. 66.2%), 9 to 24 (63.9% vs. 50.5%), and 9 to 52 (52.3% vs. 41.5%) in favor of the experimental group. | Not reported. | Significant differences between conditions in time to the first lapse after the quit date in favor of the experimental group. |
| McClure et al. (2018) [51] | 25% at the quit date and 0% at the 5-day follow-up. | Not reported. | Not reported. |
| Minami et al. (2018) [52] | 12.5% at 2-week, 4-week, and 3-months point-assessment. | All participants reported reductions in CPD from baseline to 2-week, 4-week, and 3-month point-assessments. | Not reported. |
| O’Connor et al. (2020) [45] | Nonsignificant differences between conditions at post-treatment (36% combined group, 20% ACT, and 24% behavioral support). Nonsignificant differences between conditions at 6-month follow-up (24% combined group, 24% ACT, and 20% behavioral support). | Significant differences in CPD reduction in favor of the combined condition. | Not reported. |
| Raiff et al. (2017) [48] | 1.25% at baseline, 13.8% at tapering, 35.5% at abstinence induction, and 0% at 1-month follow-up. | Not reported. | Not reported. |
| Wilson et al. (2019) [53] | Cohort 1: 40% at post-treatment and 20% at 3-months follow-up. Cohort 2: 38% at post-treatment and 15% at 3-months follow-up. | Cohort 1: 20% reduced CPD at post-treatment. Cohort 2: 38% reduced CPD at post-treatment | Not reported. |
| Feature | Definition |
|---|---|
| CO | Taking a CO breath sample |
| Set a quit date | Creating a tailored quit plan or set a quit date |
| EMAS | Ecological momentary assessment, whose definition appears in each study |
| Self-tracking or smoking self-report | Providing information about self-progress through the smoking cessation process or logging cigarettes in the app. |
| Mindfulness content | Any information, material, or activity based on mindfulness |
| ACT content | Any information, material, or activity based on acceptance and commitment therapy |
| Smartphone App | CO | Set a Quit Date | EMAS | Self-Tracking or Smoking Self-Report | Mindfulness Content | ACT Content |
|---|---|---|---|---|---|---|
| CTC app [55] | X | X | ||||
| Intervention app [32] | X | X | ||||
| SmartQuit [33,45] | X | X | X | |||
| SQ2.0 app [38] | X | X | X | |||
| REQ-Mobile [44] | X | |||||
| SmokeBeat app [34] | X | |||||
| Craving to Quit [47] | X | X | ||||
| Clickotine app [43] | X | X | ||||
| Pivot mobile app [42] | X | X | ||||
| Smart-T app [39] | X | |||||
| mCM app [35,36,40,53] | X | X | ||||
| Motiv8 app [48,54] | X | X | ||||
| Smart-T2 app [41] | X | X | ||||
| Stay Quit Coach app [36,53] | X | |||||
| App-based MT program [49] | X | X | X | |||
| Coach2Quit app [37] | X | X | X | |||
| CASC smartphone app [50] | X | |||||
| CASC smartphone app [46] | X | X | ||||
| M3 app [51] | X | X | X | |||
| Smartphone app [52] | X | X | X | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barroso-Hurtado, M.; Suárez-Castro, D.; Martínez-Vispo, C.; Becoña, E.; López-Durán, A. Smoking Cessation Apps: A Systematic Review of Format, Outcomes, and Features. Int. J. Environ. Res. Public Health 2021, 18, 11664. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111664
Barroso-Hurtado M, Suárez-Castro D, Martínez-Vispo C, Becoña E, López-Durán A. Smoking Cessation Apps: A Systematic Review of Format, Outcomes, and Features. International Journal of Environmental Research and Public Health. 2021; 18(21):11664. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111664
Chicago/Turabian StyleBarroso-Hurtado, María, Daniel Suárez-Castro, Carmela Martínez-Vispo, Elisardo Becoña, and Ana López-Durán. 2021. "Smoking Cessation Apps: A Systematic Review of Format, Outcomes, and Features" International Journal of Environmental Research and Public Health 18, no. 21: 11664. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111664