
The Patient Centered Assessment Method (PCAM) for Action-Based Biopsychosocial Evaluation of Patient Needs: Validation and Perceived Value of the Dutch Translation

 ,
,  ,
,
Abstract
:1. Introduction
1.1. PCAM: Theoretical Foundation
1.2. TARGET Program for Integrated, Person-Centered Care
2. Materials and Methods
2.1. Translation and Contextualization
2.2. Psychometric Properties
2.2.1. Population
2.2.2. Analysis
2.3. Perceived Value, Feasibility and Face Validity
3. Results
3.1. Dutch Version of PCAM
3.2. Study Participants
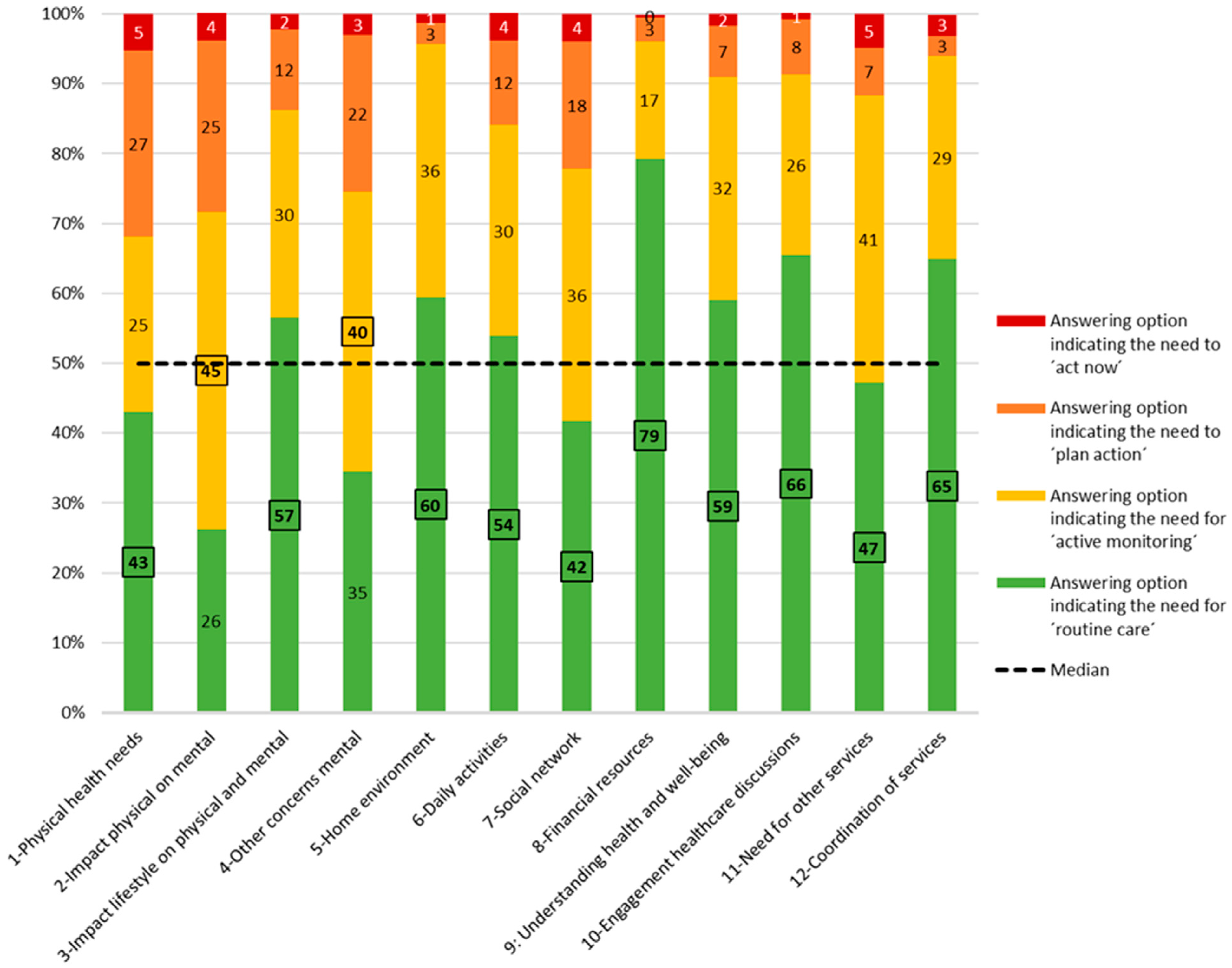
3.3. PCAM General Properties
3.4. Psychometric Properties
3.5. Perceived Value, Feasibility and Face Validity
3.5.1. PCAM as Measurement Tool
“We have got more measurement tools, for instance for people with COPD. It could have some value [to use the PCAM as measurement tool], but on the other hand I think: we have got so many measurement tools. With the conversation [the needs assessment] you mainly focus on: Who is in front of you? What can you do for someone?”(Primary care professional 2)
“Such a conversation [the needs assessment] is about things that are very important for the patient. […] So it happens that topics are not addressed which I, as a caregiver, wanted to address but the patients did not want to. And when you then fill in the PCAM, you sometimes miss information. So it is a matter of translating the thoughts of the patient to how the professional interprets it.”(Primary care professional 3)
3.5.2. PCAM as Action Planning Tool
“It is helpful to have a sort of evaluation moment at the end of such a conversation [the needs assessment]. […] I like to wrap it up like: What types of challenges does the patient encounter? And what is already going well? The PCAM is suited for this, in my opinion.”(Primary care professional 9)
3.5.3. PCAM as Conversation Tool
3.5.4. Feasibility
3.5.5. Face Validity
“A red score on ‘financial problems’ does not have to indicate that there is a problem. We’ve got one patient who scores definitely ‘red’ in terms of the financial situation, but she still manages it with some help. So it is not really a problem, but I still have to score it as a problem. […] It should be a green score, but that is not possible because green says there are no financial problems.”(Primary care professional 8)
4. Discussion
4.1. Practical Implications, Future Research and Policy
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Additional Information about the Dutch Primary Care System
Appendix B. Final Dutch Version of the PCAM

| Gezondheid en Welbevinden | ||||
| 1. | Als u nadenkt over de fysieke gezondheid van uw patiënt, zijn er dan enige symptomen of problemen (risico indicatoren) waar u over twijfelt, die verder onderzoek behoeven? | |||
| Geen twijfels of problemen worden al onderzocht | Milde vage fysieke symptomen of problemen; maar die hebben géén impact op het dagelijks leven of leiden niet tot ongerustheid bij de patiënt | Matige tot ernstige symptomen of problemen die impact hebben op het dagelijks leven | Ernstige symptomen of problemen die een significante impact veroorzaken op het dagelijks leven | |
| 2. | Hebben de fysieke gezondheidsproblemen van de patiënt impact op zijn/haar mentaal welbevinden? | |||
| Geen redenen tot ongerustheid | Milde impact op het mentaal welbevinden, bijvoorbeeld “verminderd genieten” | Matige tot ernstige impact op het mentaal welbevinden en verhinderen het genieten van dagelijkse activiteiten | Ernstige impact op het mentaal welbevinden en verhinderen het uitvoeren van dagelijkse activiteiten | |
| 3. | Zijn er problemen met het leefstijlgedrag (alcohol, drugs, dieet, lichaamsbeweging) van uw patiënt, die impact hebben op het fysiek of mentaal welbevinden? | |||
| Geen redenen tot ongerustheid | Enige milde ongerustheid over potentieel negatieve impact op het welbevinden | Matige tot ernstige impact op het welbevinden van de patiënt, verhinderen het genieten van dagelijkse activiteiten | Ernstige impact op het welbevinden van de patiënt en mogelijke invloed op de omgeving | |
| 4. | Heeft u enige andere redenen tot zorgen over het mentaal welbevinden van uw patiënt? Hoe zou u de ernst en impact daarvan op uw patiënt beoordelen? | |||
| Geen redenen tot ongerustheid | Milde problemen- beperken het functioneren niet | Matige tot ernstige problemen die het functioneren beperken | Ernstige problemen die de meeste dagelijkse functies aantasten | |
| Sociale Omgeving | ||||
| 1. | Hoe zou u hun thuisomgeving beoordelen in termen van veiligheid en stabiliteit (waaronder relatieproblemen, onzekere thuissituatie, burenoverlast)? | |||
| Constant veilig, ondersteunend, stabiel, geen problemen geïdentificeerd | Over het algemeen veilig, stabiel, maar met enige uitzonderingen | Veiligheid/stabiliteit twijfelachtig | Onveilig en onstabiel | |
| 2. | Hoe hebben dagelijkse activiteiten impact op het welbevinden van de patiënt? (waaronder huidige of verwachte werkloosheid, werk, (mantel) zorgtaken, mogelijkheid tot vervoer of anderszins) | |||
| Geen problemen geïdentificeerd of positieve voordelen waargenomen | Enige algemene ontevredenheid, maar geen ongerustheid | Draagt bij aan een sombere stemming of stress op sommige momenten | Ernstige impact op slecht mentaal welbevinden | |
| 3. | Hoe zou u hun sociale netwerk beoordelen (familie, werk, vrienden en verenigingsleven)? | |||
| Goede participatie in sociale netwerken | Voldoende participatie in sociale netwerken | Beperkte participatie, met enige mate van sociale isolatie | Weinig participatie, eenzaam en sociaal geïsoleerd | |
| 4. | Hoe zou u hun financiële middelen beoordelen (waaronder mogelijkheid om in de basisbehoeften te voorzien en alle benodigde medische zorg te betalen)? | |||
| Financieel zeker, voldoende middelen, geen problemen geïdentificeerd | Financieel zeker, enkele uitdagingen om rond te komen | Financieel onzeker, enkele uitdagingen om rond te komen | Financieel onzeker, heel weinig middelen, acute uitdagingen om rond te komen | |
| Gezondheidsvaardigheden en Communicatie | ||||
| 1. | Hoe goed begrijpt de patiënt nu zijn/haar gezondheid en welbevinden (symptomen, signalen of risicofactoren) en wat hij of/zij moet doen om regie te voeren over zijn/haar gezondheid? | |||
| Redelijk tot goed begrip en voert al regie over zijn/haar gezondheid of is bereid om betere regie te voeren | Redelijk tot goed begrip, maar voelt zich op dit moment niet in staat om met adviezen bezig te zijn | Weinig begrip, wat impact heeft op hun vermogen om betere regie te voeren | Slecht begrip met significante impact op het vermogen regie te voeren over gezondheid | |
| 2. | Hoe goed denkt u dat uw patiënt mee kan doen in zorggesprekken? (beperkingen zijn bijvoorbeeld taal, doofheid, afasie, alcohol- of drugsproblematiek, leerproblemen, concentratie) | |||
| Duidelijke en open communicatie, geen beperkingen geïdentificeerd | Voldoende communicatie, met of zonder minieme beperkingen | Enkele moeilijkheden in communicatie, met of zonder redelijke beperkingen | Serieuze moeilijkheden in communicatie, met ernstige beperkingen | |
| Zorgcoördinatie | ||||
| 1. | Moeten andere disciplines betrokken worden om deze patiënt te helpen? | |||
| Andere zorg/disciplines niet nodig op dit moment | Andere zorg/disciplines betrokken en voldoende | Andere zorg/disciplines betrokken, maar niet toereikend | Andere zorg/disciplines niet betrokken, wel nodig | |
| 2. | Zijn de disciplines, die op dit moment bij de patiënt betrokken zijn, goed op elkaar afgestemd? (houdt rekening met andere disciplines die u nu aanbeveelt) | |||
| Alle benodigde zorg/disciplines betrokken en goed op elkaar afgestemd | Benodigde zorg/disciplines betrokken en voldoende op elkaar afgestemd | Benodigde zorg/disciplines betrokken met enkele belemmeringen voor het afstemmen van zorg | Benodigde zorg/disciplines ontbreken en/of werken niet goed samen | |
| Reguliere zorg | Actief monitoren | Plan Actie | Handel Nu | |
| Welke Actie Is Nodig? | Wie Moet Betrokken Worden? | Belemmeringen Voor Actie? | Welke Actie Wordt Ondernomen? |
| Notities: | |||
| |||
References
- Maxwell, M.; Hibberd, C.; Pratt, R.; Cameron, I.; Mercer, S. Development and Initial Validation of the Minnesota Edinburgh Complexity Assessment Method (MECAM) for Use within the Keep Well Health Check; NHS Health Scotland: Edinburgh, Scotland, 2011. [Google Scholar]
- Pratt, R.; Hibberd, C.; Cameron, I.M.; Maxwell, M. The Patient Centered Assessment Method (PCAM): Integrating the social dimensions of health into primary care. J. Comorb. 2015, 5, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Hewner, S.; Casucci, S.; Sullivan, S.; Mistretta, F.; Xue, Y.; Johnson, B.; Pratt, R.; Lin, L.; Fox, C. Integrating social determinants of health into primary care clinical and informational workflow during care transitions. EGEMS 2017, 5, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Hewner, S.; Sullivan, S.S.; Yu, G. Reducing emergency room visits and in-hospitalizations by implementing best practice for transitional care using innovative technology and big data. Worldviews Evid. Based Nurs. 2018, 15, 170–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, S.; Matsushima, M.; Wakabayashi, H.; Mutai, R.; Murayama, S.; Hayashi, T.; Ichikawa, H.; Nakano, Y.; Watanabe, T.; Fujinuma, Y. Validity and reliability of the Patient Centred Assessment Method for patient complexity and relationship with hospital length of stay: A prospective cohort study. BMJ Open 2017, 7, e016175. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Matsushima, M.; Wakabayashi, H.; Mutai, R.; Sugiyama, Y.; Yodoshi, T.; Horiguchi, R.; Watanabe, T.; Fujinuma, Y. Correlation of patient complexity with the burden for health-related professions, and differences in the burden between the professions at a Japanese regional hospital: A prospective cohort study. BMJ Open 2019, 9, e025176. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, M.; Hibberd, C.; Aitchison, P.; Calveley, E.; Pratt, R.; Dougall, N.; Hoy, C.; Mercer, S.; Cameron, I. The Patient Centred Assessment Method for improving nurse-led biopsychosocial assessment of patients with long-term conditions: A feasibility RCT. Health Serv. Deliv. Res. 2018, 6, 1–119. [Google Scholar] [CrossRef] [Green Version]
- Kuipers, S.J.; Nieboer, A.P.; Cramm, J.M. Easier said than done: Healthcare professionals’ barriers to the provision of patient-centered primary care to patients with multimorbidity. Int. J. Environ. Res. Public Health 2021, 18, 6057. [Google Scholar] [CrossRef]
- Smeets, R.G.M.; Kroese, M.E.A.L.; Ruwaard, D.; Hameleers, N.; Elissen, A.M.J. Person-centred and efficient care delivery for high-need, high-cost patients: Primary care professionals’ experiences. BMC Fam. Pract. 2020, 21, 106. [Google Scholar] [CrossRef]
- de Jonge, P.; Huyse, F.J.; Stiefel, F.C.; Slaets, J.P.J.; Gans, R.O.B. INTERMED—A clinical instrument for biopsychosocial assessment. Psychosomatics 2001, 42, 106–109. [Google Scholar] [CrossRef]
- de Jonge, P.; Latour, C.; Huyse, F.J. Interrater reliability of the INTERMED in a heterogeneous somatic population. J. Psychosom. Res. 2002, 52, 25–27. [Google Scholar] [CrossRef]
- Huyse, F.J.; Lyons, J.S.; Stiefel, F.C.; Slaets, J.P.J.; de Jonge, P.; Fink, P.; Gans, R.O.B.; Guex, P.; Herzog, T.; Lobo, A.; et al. “INTERMED”: A method to assess health service needs: I. Development and reliability. Gen. Hosp. Psychiatry 1999, 21, 39–48. [Google Scholar] [CrossRef]
- Stiefel, F.C.; de Jonge, P.; Huyse, F.J.; Guex, P.; Slaets, J.P.J.; Lyons, J.S.; Spagnoli, J.; Vannotti, M. “INTERMED”: A method to assess health service needs: II. Results on its validity and clinical use. Gen. Hosp. Psychiatry 1999, 21, 49–56. [Google Scholar] [CrossRef]
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Eklund, J.H.; Holmström, I.K.; Kumlin, T.; Kaminsky, E.; Skoglund, K.; Höglander, J.; Sundler, A.J.; Condén, E.; Meranius, M.S. “Same same or different?” A review of reviews of person-centered and patient-centered care. Patient Educ. Couns. 2019, 102, 3–11. [Google Scholar] [CrossRef] [PubMed]
- The American Geriatrics Society Expert Panel on Person-Centered Care. Person-centered care: A definition and essential elements. J. Am. Geriatr. Soc. 2016, 64, 15–18. [Google Scholar] [CrossRef] [Green Version]
- Olsson, L.-E.; Ung, E.J.; Swedberg, K.; Ekman, I. Efficacy of person-centred care as an intervention in controlled trials—A systematic review. J. Clin. Nurs. 2013, 22, 456–465. [Google Scholar] [CrossRef]
- Tierney, S.; Wong, G.; Roberts, N.; Boylan, A.-M.; Park, S.; Abrams, R.; Reeve, J.; Williams, V.; Mahtani, K.R. Supporting social prescribing in primary care by linking people to local assets: A realist review. BMC Med. 2020, 18, 49. [Google Scholar] [CrossRef] [Green Version]
- Wolf, A.; Moore, L.; Lydahl, D.; Naldemirci, Ö.; Elam, M.; Britten, N. The realities of partnership in person-centred care: A qualitative interview study with patients and professionals. BMJ Open 2017, 7, e016491. [Google Scholar] [CrossRef] [Green Version]
- Smeets, R.G.M.; Hertroijs, D.F.L.; Mukumbang, F.C.; Kroese, M.E.A.L.; Ruwaard, D.; Elissen, A.M.J. First things first: How to elicit the initial program theory for a realist evaluation of complex integrated care programs. Milbank Q. 2021. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Sinsky, C. From Triple to Quadruple Aim: Care of the patient requires care of the provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef] [Green Version]
- Hameleers, N.; Elissen, A.; Kroese, M.; Ruwaard, D. Op Weg Naar een Integraal Programma Chronische Zorg: Resultaten Deelonderzoek in de Zorggroep Huisartsenzorg Drenthe; Maastricht University: Maastricht, The Netherlands, 2017. [Google Scholar]
- Huber, M.; Knottnerus, J.A.; Green, L.; Horst, H.v.d.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; van der Meer, J.W.M.; et al. How should we define health? BMJ 2011, 343, d4163. [Google Scholar] [CrossRef] [Green Version]
- Huber, M.; van Vliet, M.; Giezenberg, M.; Winkens, B.; Heerkens, Y.; Dagnelie, P.C.; Knottnerus, J.A. Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: A mixed methods study. BMJ Open 2016, 5, e010091. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Process of Translation and Adaptation of Instruments. Available online: https://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 6 October 2020).
- University of Minnesota, Department of Family Medicine and Community Health. Patient Centered Assessment Method. Available online: https://med.umn.edu/familymedicine/research/faculty-research/pcam (accessed on 6 October 2021).
- DiStefano, C.; Hess, B. Using confirmatory factor analysis for construct validation: An empirical review. J. Psychoeduc. Assess. 2005, 23, 225–241. [Google Scholar] [CrossRef]
- Moshagen, M.; Musch, J. Sample size requirements of the robust weighted least squares estimator. Methodol. Eur. J. Res. Methods Behav. Soc. Sci. 2014, 10, 60–70. [Google Scholar] [CrossRef]
- Yang-Wallentin, F.; Jöreskog, K.G.; Luo, H. Confirmatory factor analysis of ordinal variables with misspecified models. Struct. Equ. Modeling 2010, 17, 392–423. [Google Scholar] [CrossRef]
- Ware, J.E.; Gandek, B. Methods for testing data quality, scaling assumptions, and reliability: The IQOLA project approach. J. Clin. Epidemiol. 1998, 51, 945–952. [Google Scholar] [CrossRef]
- Yong, A.G.; Pearce, S. A beginner’s guide to factor analysis: Focusing on exploratory factor analysis. Tutor Quant Methods Psychol. 2013, 9, 79–94. [Google Scholar] [CrossRef]
- Costello, A.B.; Osborne, J. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2005, 10, 7. [Google Scholar] [CrossRef]
- Feenstra, M.; Smidt, N.; van Munster, B.C.; Glynn, N.W.; de Rooij, S.E. Translation and validation of the Dutch Pittsburgh Fatigability Scale for older adults. BMC Geriatr. 2020, 20, 234. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.L.; Gillaspy Jr, J.A.; Purc-Stephenson, R. Reporting practices in confirmatory factor analysis: An overview and some recommendations. Psychol. Methods 2009, 14, 6. [Google Scholar] [CrossRef]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. In Methodological Issues and Strategies in Clinical Research; Kazdin, A.E., Ed.; American Psychological Association: Washington, WA, USA, 2016. [Google Scholar]
- de Souza, A.C.; Alexandre, N.M.C.; Guirardello, E.B. Psychometric properties in instruments evaluation of reliability and validity. Epidemiol. Serv. Saúde 2017, 26, 649–659. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Striving to meet the trustworthiness criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Sociaal en Cultureel Planbureau (SCP). Waar Wonen de Armen in Nederland? Available online: https://digitaal.scp.nl/armoedeinkaart2019/waar-wonen-de-armen-in-nederland/ (accessed on 28 September 2021).
- Fitzpatrick, T.; Rosella, L.C.; Calzavara, A.; Petch, J.; Pinto, A.D.; Manson, H.; Goel, V.; Wodchis, W.P. Looking beyond income and education: Socioeconomic status gradients among future high-cost users of health care. Am. J. Prev. Med. 2015, 49, 161–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luppa, M.; Giersdorf, J.; Riedel-Heller, S.; Prütz, F.; Rommel, A. Frequent attenders in the German healthcare system: Determinants of high utilization of primary care services. Results from the cross-sectional German health interview and examination survey for adults (DEGS). BMC Fam. Pract. 2020, 21, 10. [Google Scholar] [CrossRef]
- Smeets, R.G.M.; Elissen, A.M.J.; Kroese, M.E.A.L.; Hameleers, N.; Ruwaard, D. Identifying subgroups of high-need, high-cost, chronically ill patients in primary care: A latent class analysis. PLoS ONE 2020, 15, e0228103. [Google Scholar] [CrossRef] [PubMed]
- Sterling, S.; Chi, F.; Weisner, C.; Grant, R.; Pruzansky, A.; Bui, S.; Madvig, P.; Pearl, R. Association of behavioral health factors and social determinants of health with high and persistently high healthcare costs. Prev. Med. Rep. 2018, 11, 154–159. [Google Scholar] [CrossRef]
- Barry, C.A.; Bradley, C.P.; Britten, N.; Stevenson, F.A.; Barber, N. Patients’ unvoiced agendas in general practice consultations: Qualitative study. BMJ 2000, 320, 1246–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloch, G.; Rozmovits, L.; Giambrone, B. Barriers to primary care responsiveness to poverty as a risk factor for health. BMC Fam. Pract. 2011, 12, 62. [Google Scholar] [CrossRef] [Green Version]
- Pinto, A.D.; Bloch, G. Framework for building primary care capacity to address the social determinants of health. Can. Fam. Physician 2017, 63, e476–e482. [Google Scholar]
- Mutai, R.; Sugiyama, Y.; Yoshida, S.; Horiguchi, R.; Watanabe, T.; Kaneko, M.; Tominaga, T.; Hayashi, D.; Matsushima, M. Development and validation of a Japanese version of the Patient Centred Assessment Method and its user guide: A cross-sectional study. BMJ Open 2020, 10, e037282. [Google Scholar] [CrossRef]
- Thomas, H.; Mitchell, G.; Rich, J.; Best, M. Definition of whole person care in general practice in the English language literature: A systematic review. BMJ Open 2018, 8, e023758. [Google Scholar] [CrossRef] [PubMed]
- Lines, L.M.; Lepore, M.; Wiener, J.M. Patient-centered, person-centered, and person-directed care: They are not the same. Med. Care 2015, 53, 561–563. [Google Scholar] [CrossRef] [PubMed]
- van Vliet, M.; Doornenbal, B.M.; Boerema, S.; van den Akker-van Marle, E.M. Development and psychometric evaluation of a Positive Health measurement scale: A factor analysis study based on a Dutch population. BMJ Open 2021, 11, e040816. [Google Scholar] [CrossRef] [PubMed]
- Long, P.; Abrams, M.; Milstein, A.; Anderson, G.; Apton, K.; Dahlberg, M.; Whicher, D. Effective Care for High-Need Patients; National Academy of Medicine: Washington, DC, USA, 2017. [Google Scholar]
- Pestka, D.L.; Paterson, N.L.; Benedict, K.A.; Williams, D.D.; Shellenbarger, B.A.; McVay-Steer, A.J.; Cheng, T.; Pangburn, J.; Warner, D.; Bryant, L. Delivering care to high-cost high-need patients: Lessons learned in the development of a complex care primary care team. J. Prim. Care Community Health 2021, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Vaida, B. For super-utilizers, integrated care offers a new path. Health Aff. 2017, 36, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A.; Checkland, K.; Sidhu, M.; Hammond, J.; Parkinson, S. Primary care networks: Are they fit for the future? Br. J. Gen. Pract. 2021, 71, 106. [Google Scholar] [CrossRef]
- Peek, C.J.; Baird, M.A.; Coleman, E. Primary care for patient complexity, not only disease. Fam. Syst. Health 2009, 27, 287–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroneman, M.; Boerma, W.; van den Berg, M.; Groenewegen, P.; de Jong, J.; van Ginneken, E. Netherlands: Health system review. Health Syst. Transit. 2016, 18, 1–239. [Google Scholar]
- van Weel, C.; Schers, H.; Timmermans, A. Health care in the Netherlands. J. Am. Board Fam. Med. 2012, 25, S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hassel, D.; Batenburg, R.; van der Velden, L. Praktijkondersteuners (POH’s) in Beeld: Aantallen, Kenmerken en Geografische Spreiding in Nederland; NIVEL: Utrecht, The Netherlands, 2016. [Google Scholar]
- de Bakker, D.H.; Struijs, J.N.; Baan, C.A.; Raams, J.; de Wildt, J.-E.; Vrijhoef, H.J.M.; Schut, F.T. Early results from adoption of bundled payment for diabetes care in the Netherlands show improvement in care coordination. Health Aff. 2012, 31, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Out, K.E.; de Jong, J.D. Het Perspectief van Zorggroepen en Gezondheidscentra op Onderhandelingen en Contracten Met Zorgverzekeraars; NIVEL: Utrecht, The Netherlands, 2017. [Google Scholar]



{kind=link}
{kind=link}
| N (SD/Percentage) | |
|---|---|
| Age in years a, mean (SD) | 72.5 (±14.1) |
| Age in years a, number (percentage) | |
| <65 years | 55 (23.7%) |
| ≥65 and <80 years | 85 (36.6%) |
| ≥80 years | 92 (39.7%) |
| Sex, number (percentage) | |
| Male | 64 (29.1%) |
| Female | 156 (70.9%) |
| Weighted care utilization, mean (SD) b | 46.9 (±20.4) |
| Number of chronic conditions c, number (percentage) | |
| One | 41 (18.2%) |
| Two | 78 (34.7%) |
| Three of more | 106 (47.1%) |
| Type of chronic condition(s) c, number (percentage) | |
| Only physical | 159 (70.7%) |
| Only mental | 4 (1.8%) |
| Combination of physical and mental | 62 (27.6%) |
| Chronic conditions c, number (percentage) | |
| Diabetes mellitus | 124 (55.1%) |
| Asthma | 50 (22.2%) |
| Cancer | 49 (21.8%) |
| Chronic obstructive pulmonary disease (COPD) | 45 (20.0%) |
| Coronary heart diseases | 37 (16.4%) |
| Chronic back or neck disorder | 35 (15.6%) |
| Heart failure | 33 (14.7%) |
| Mood disorders | 32 (14.2%) |
| Heart arrhythmia | 31 (13.8%) |
| Osteoarthritis | 31 (13.8%) |
| Visual disorders | 23 (10.2%) |
| Stroke (including TIA) | 21 (9.3%) |
| Anxiety disorders | 19 (8.4%) |
| Burnout | 12 (5.3%) |
| Osteoporosis | 10 (4.4%) |
| Rheumatoid arthritis | 8 (3.6%) |
| Dementia including Alzheimer’s | 7 (3.1%) |
| Hearing disorders | 7 (3.1%) |
| Endocardial conditions, valvular conditions | 5 (2.2%) |
| Chronic alcohol abuse | 4 (1.8%) |
| Mental retardation | 3 (1.3%) |
| Migraine | 3 (1.3%) |
| Epilepsy | 1 (0.4%) |
| Parkinson’s disease | 1 (0.4%) |
| Personality disorders | 1 (0.4%) |
| Schizophrenia | 1 (0.4%) |
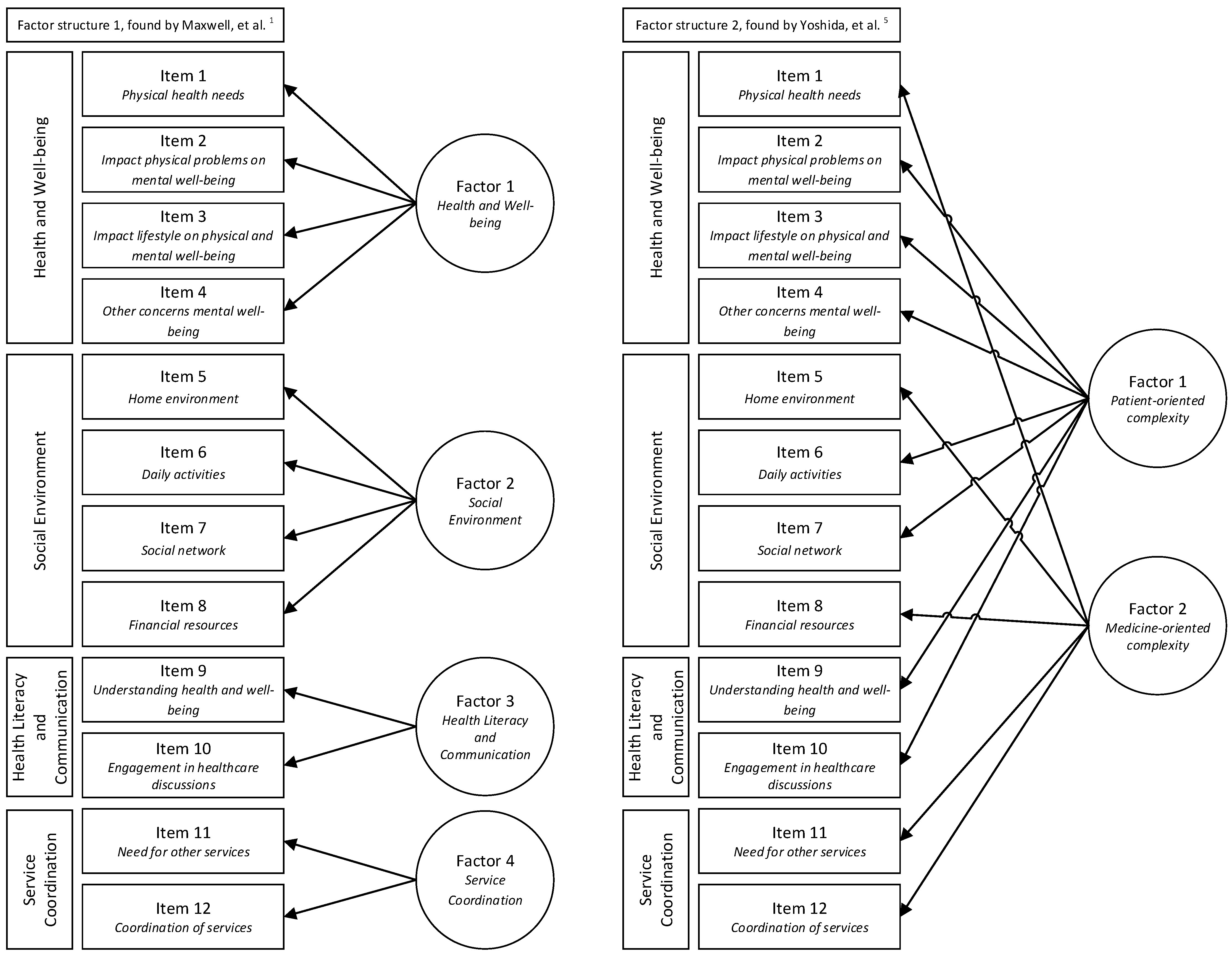
| Factor Structure 1, by Maxwell et al. [1] | Factor Structure 2, by Yoshida et al. [5] | ||
|---|---|---|---|
| Factors | Factor Loadings | Factors | Factor Loadings |
| Factor 1: health and well-being | Item 1: 0.432 Item 2: 0.692 Item 3: 0.630 Item 4: 0.897 | Factor 1: patient-oriented complexity | Item 2: 0.654 Item 3: 0.596 Item 4: 0.832 Item 6: 0.684 Item 7: 0.713 Item 9: 0.701 Item 10: 0.701 |
| Factor 2: social environment | Item 5: 0.681 Item 6: 0.748 Item 7: 0.783 Item 8: 0.409 | Factor 2: medicine-oriented complexity | Item 1: 0.426 Item 5: 0.664 Item 8: 0.382 Item 11: 0.773 Item 12: 0.842 |
| Factor 3: health literacy and communication | Item 9: 0.860 Item 10: 0.853 | ||
| Factor 4: service coordination | Item 11: 0.827 Item 12: 0.917 | ||
| Factor Structure 1, Found by Maxwell et al. [1] | Factor Structure 2, Found by Yoshida et al. [5] | |
|---|---|---|
| SRMR a | 0.061 * | 0.098 |
| TLI b | 0.968 * | 0.885 |
| RMSEA c | 0.057 * | 0.109 |
| Cronbach’s alpha | Factor 1: 0.69 Factor 2: 0.66 Factor 3: 0.75 * Factor 4: 0.75 * | Factor 1: 0.8 * Factor 2: 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smeets, R.G.M.; Hertroijs, D.F.L.; Kroese, M.E.A.L.; Hameleers, N.; Ruwaard, D.; Elissen, A.M.J. The Patient Centered Assessment Method (PCAM) for Action-Based Biopsychosocial Evaluation of Patient Needs: Validation and Perceived Value of the Dutch Translation. Int. J. Environ. Res. Public Health 2021, 18, 11785. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211785
Smeets RGM, Hertroijs DFL, Kroese MEAL, Hameleers N, Ruwaard D, Elissen AMJ. The Patient Centered Assessment Method (PCAM) for Action-Based Biopsychosocial Evaluation of Patient Needs: Validation and Perceived Value of the Dutch Translation. International Journal of Environmental Research and Public Health. 2021; 18(22):11785. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211785
Chicago/Turabian StyleSmeets, Rowan G. M., Dorijn F. L. Hertroijs, Mariëlle E. A. L. Kroese, Niels Hameleers, Dirk Ruwaard, and Arianne M. J. Elissen. 2021. "The Patient Centered Assessment Method (PCAM) for Action-Based Biopsychosocial Evaluation of Patient Needs: Validation and Perceived Value of the Dutch Translation" International Journal of Environmental Research and Public Health 18, no. 22: 11785. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211785