
Immediate Effects of Whole-Body Vibration Associated with Squatting Exercises on Hemodynamic Parameters in Sarcopenic Older People: A Randomized Controlled Trial

 , , , , , , ,
, , , , , , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
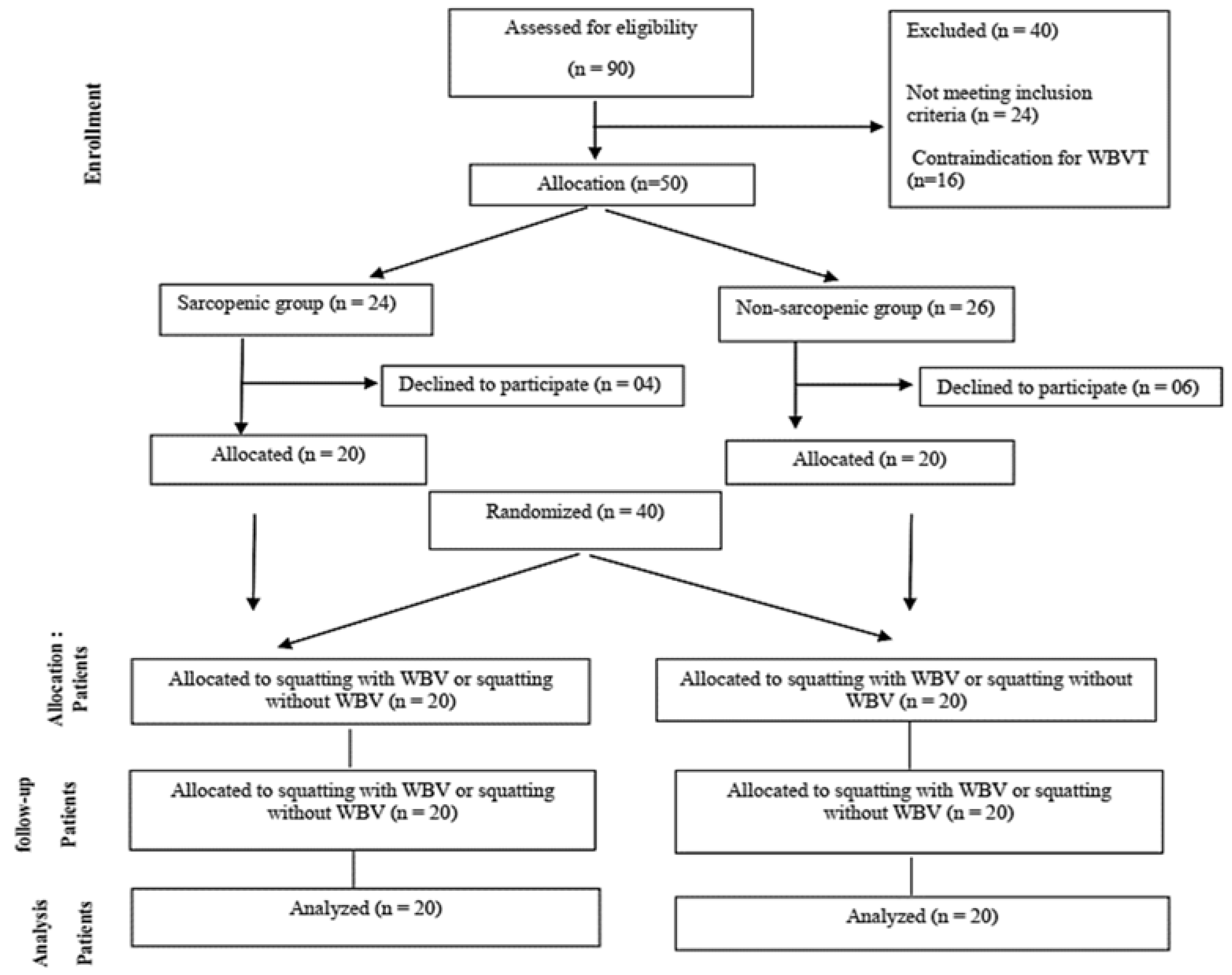
2.1. Participants and Sample Size Estimation
2.2. Diagnostic Criteria to Sarcopenia
2.3. Procedures
2.3.1. Body Mass Index (BMI)
2.3.2. Body Composition Assessment
2.3.3. Functionality Assessment
2.4. Interventions
2.4.1. Exercise Intervention with WBV
2.4.2. Exercise Intervention without WBV
2.5. Data Collection
2.5.1. Hemodynamic Measurements
2.5.2. Subjective Perception of Effort (SPE)
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
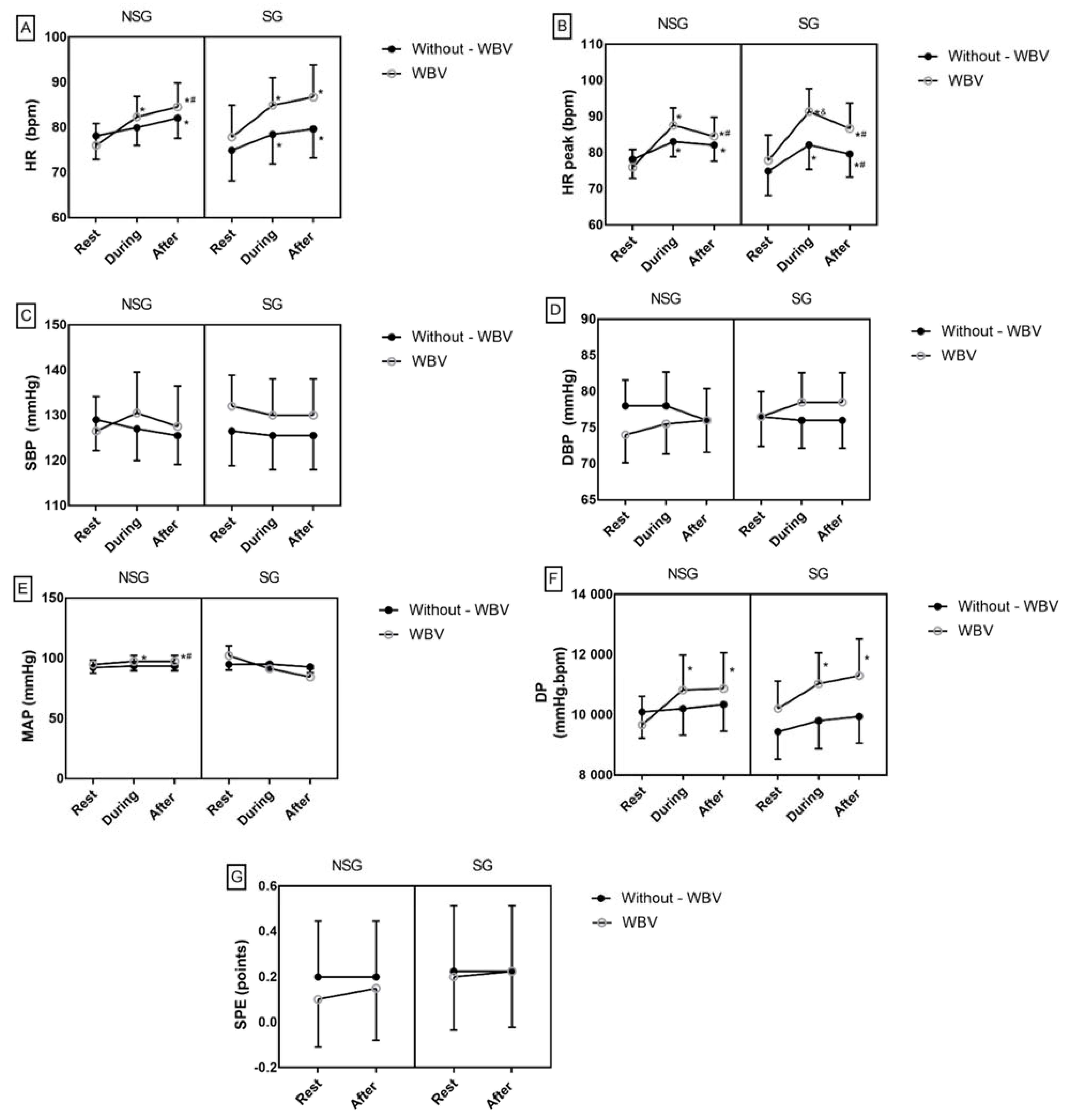
3.2. Hemodynamic Responses in the Situations with and without WBV in NSG and SG
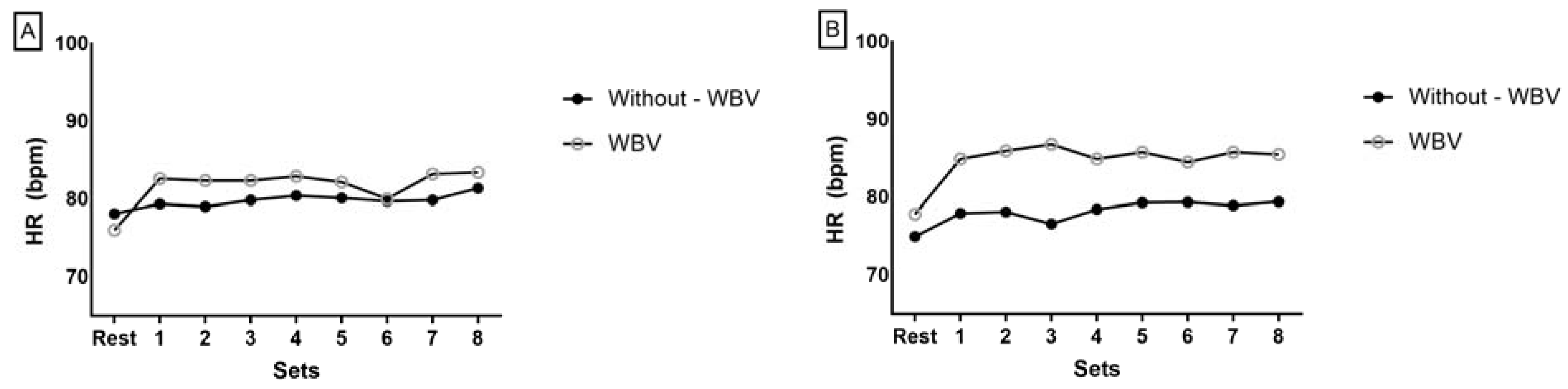
3.3. Heart Rate (HR) Behavior after Each Set of Exercises in Interventions with and without WBV in NSG and SG
3.4. Comparison of Hemodynamic Parameters between the Interventions in the NSG and the SG
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, K.; Otten, L. Financial impact of sarcopenia or low muscle mass—A short review. Clin. Nutr. 2019, 38, 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Churilov, I.; Churilov, L.; MacIsaac, R.J.; Ekinci, E.I. Systematic review and meta-analysis of prevalence of sarcopenia in post acute inpatient rehabilitation. Osteoporos. Int. 2018, 29, 805–812. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 48–759. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.Y.; Bruyère, O. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.; Kang, G.; Yoon, J.; Kim, W.; Kim, H. Relationship between within-visit blood pressure variability and skeletal muscle mass. J. Nutr. Health Aging 2019, 23, 79–83. [Google Scholar] [CrossRef]
- Investigations, O. Diastolic Blood Pressure, Subclinical Myocardial Damage, and Cardiac Events. J. Am. Coll. Cardiol. 2016, 68, 1713–1722. [Google Scholar] [CrossRef]
- Muller, M.D.; Gao, Z.; Mast, J.L.; Blaha, C.A.; Drew, R.C.; Leuenberger, U.A.; Sinoway, L.I. Aging attenuates the coronary blood flow response to cold air breathing and isometric handgrip in healthy humans. Am. J. Physiol.-Heart Circ. Physiol. 2012, 302, H1737–H1746. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.; Jaime, S.J.; Grubbs, B.; Panton, L.B.; Fischer, S.M. Attenuated aortic blood pressure responses to metaboreflex activation in older adults with dynapenia. Exp. Gerontol. 2020, 138, 110984. [Google Scholar] [CrossRef]
- Curcio, F.; Testa, G.; Liguori, I.; Papillo, M.; Flocco, V.; Panicara, V.; Galizia, G.; Della-Morte, D.; Gargiulo, G.; Cacciatore, F.; et al. Sarcopenia and heart failure. Nutrients 2020, 12, 211. [Google Scholar] [CrossRef] [Green Version]
- Calvani, R.; Marini, F.; Cesari, M.; Tosato, M.; Anker, S.D.; Von Haehling, S.; Miller, R.R.; Bernabei, R.; Landi, F.; Marzetti, E. Biomarkers for physical frailty and sarcopenia: State of the science and future developments. J. Cachexia. Sarcopenia Muscle 2015, 6, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Wesley, G.; Rodrigues, M.; De Souza, F.R.; Jose, M.; Costa, A.; Von Haehling, S.; Takayama, L.; Pereira, R.M.R.; Negrão, C.E.; Anker, S.D.; et al. Original Article Sympatho-Vagal Imbalance is Associated with Sarcopenia in Male Patients with Heart Failure. Arq. Bras. Cardiol. 2018, 112, 739–746. [Google Scholar] [CrossRef]
- Yanaga, M.C. Sarcopenia em Idosos: Um estudo de revisão. Int. J. Nutrol. 2020, 13, 089–094. [Google Scholar] [CrossRef]
- Rolland, Y.; Czerwinski, S.; Van Kan, G.A.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [Green Version]
- Visvanathan, R.; Chapman, I. Preventing sarcopaenia in older people. Maturitas 2010, 66, 383–388. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E. Pharmacologic Options for the Treatment of Sarcopenia. Calcif. Tissue Int. 2016, 98, 319–333. [Google Scholar] [CrossRef]
- Valenzuela, P.L.; Castillo-García, A.; Morales, J.S.; Izquierdo, M.; Serra-Rexach, J.A.; Santos-Lozano, A.; Lucia, A. Physical exercise in the oldest old. Compr. Physiol. 2019, 9, 1281–1304. [Google Scholar] [CrossRef]
- Rittweger, J. Vibration as an exercise modality: How it may work, and what its potential might be. Eur. J. Appl. Physiol. 2010, 108, 877–904. [Google Scholar] [CrossRef] [Green Version]
- Freitas, E.D.S.; Frederiksen, C.; Miller, R.M.; Heishman, A.; Anderson, M.; Pardo, G.; Fjeldstad, C.; Bemben, D.A.; Bemben, M.G. Acute and Chronic Effects of Whole-Body Vibration on Balance, Postural Stability, and Mobility in Women With Multiple Sclerosis. Dose-Response 2018, 16, 1559325818816577. [Google Scholar] [CrossRef]
- Lam, F.M.H.; Liao, L.R.; Kwok, T.C.Y.; Pang, M.Y.C. The effect of vertical whole-body vibration on lower limb muscle activation in elderly adults: Influence of vibration frequency, amplitude and exercise. Maturitas 2016, 88, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Von Stengel, S. Alternative Exercise Technologies to Fight against Sarcopenia at Old Age: A Series of Studies and Review. J. Aging Res. 2012, 2012, 109013. [Google Scholar] [CrossRef]
- Thompson, W.R.; Yen, S.S.; Rubin, J. Vibration therapy: Clinical applications in bone. Curr. Opin. Endocrinol. Diabetes Obes. 2014, 21, 447–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Y.Q.; Peng, N.; Zhou, M.; Liu, P.P.; Qi, X.L.; Wang, N.; Wang, G.; Wu, Z.P. Tai Chi and whole-body vibrating therapy in sarcopenic men in advanced old age: A clinical randomized controlled trial. Eur. J. Ageing 2019, 16, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Avelar, N.C.P.; Simão, A.P.; Tossige-Gomes, R.; Neves, C.D.C.; Mezencio, B.; Szmuchrowski, L.; Coimbra, C.C.; Lacerda, A.C.R. Oxygen consumption and heart rate during repeated squatting exercises with or without whole-body vibration in the elderly. J. Strength Cond. Res. 2011, 25, 3495–3500. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, D.J.; North, P.; Zealand, N.; Drive, T.; Zealand, N. Vibration Exercise: The Potential Benefits. Int. J. Sports Med. 2011, 32, 75–99. [Google Scholar] [CrossRef] [Green Version]
- Cochrane, D.J.; Sartor, F.; Winwood, K.; Stannard, S.R.; Narici, M.V.; Rittweger, J. A Comparison of the Physiologic Effects of Acute Whole-Body Vibration Exercise in Young and Older People. Arch. Phys. Med. Rehabil. 2008, 89, 815–821. [Google Scholar] [CrossRef]
- Lage, V.K.S.; Lacerda, A.C.R.; Neves, C.D.C.; Chaves, M.G.A.; Soares, A.A.; Lima, L.P.; Matos, M.A.; Leite, H.R.; Fernandes, J.S.C.; Oliveira, V.C.; et al. Cardiorespiratory responses in different types of squats and frequencies of whole body vibration in patients with chronic obstructive pulmonary disease. J. Appl. Physiol. 2019, 126, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Sá-Caputo, D.C.; Paineiras-Domingos, L.L.; Oliveira, R.; Neves, M.F.T.; Brandão, A.; Marin, P.J.; Sañudo, B.; Furness, T.; Taiar, R.; Bernardo-Filho, M. Acute Effects of Whole-Body Vibration on the Pain Level, Flexibility, and Cardiovascular Responses in Individuals With Metabolic Syndrome. Dose-Response 2018, 16, 1559325818802139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bautmans, I.; Van Hees, E.; Lemper, J.C.; Mets, T. The feasibility of whole body vibration in institutionalised elderly persons and its influence on muscle performance, balance and mobility: A randomised controlled trial [ISRCTN62535013]. BMC Geriatr. 2005, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, V.G.C.; Mendonça, V.A.; Souza, A.L.C.; Fonseca, S.F.; Camargos, A.C.R.; Lage, V.K.S.; Neves, C.D.C.; Santos, J.M.; Teixeira, L.A.C.; Vieira, E.L.M.; et al. Inflammatory biomarkers responses after acute whole body vibration in fibromyalgia. Braz. J. Med. Biol. Res. 2018, 51, 1–9. [Google Scholar] [CrossRef]
- Gould, H.; Brennan, S.L.; Kotowicz, M.A.; Nicholson, G.C.; Pasco, J.A. Total and appendicular lean mass reference ranges for Australian men and women: The Geelong osteoporosis study. Calcif. Tissue Int. 2014, 94, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Cervi, A.; Franceschini, S.D.C.C.; Priore, S.E. Análise crítica do uso do índice de massa corporal para idosos. Rev. Nutr. 2005, 18, 765–775. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, 85–94. [Google Scholar] [CrossRef]
- Avelar, N.C.P.; Ribeiro, V.G.C.; Mezêncio, B.; Fonseca, S.F.; Tossige-Gomes, R.; da Costa, S.J.; Szmuchrowski, L.; Gripp, F.; Coimbra, C.C.; Lacerda, A.C.R. Influence of the knee flexion on muscle activation and transmissibility during whole body vibration. J. Electromyogr. Kinesiol. 2013, 23, 844–850. [Google Scholar] [CrossRef]
- Brum, P.C.; de M Forjaz, C.L.; Tinucci, T.; Negrão, C.E. Adaptações agudas e crônicas do exercício físico no sistema cardiovascular. Rev. Paul. Educ. Fís. 2004, 18, 21–31. [Google Scholar]
- Miranda, H.; Simão, R.; Lemos, A.; Dantas, B.H.A.; Baptista, L.A.; Novaes, J. Análise de freqüência cardíaca, pressão arterial e duplo-produto em diferentes posições corporais nos exercícios resistidos. Rev. Bras. Med. Esporte 2005, 11, 295–298. [Google Scholar] [CrossRef]
- Tibana, R.; Balsamo, S.; Prestes, J. Association between muscle strength and at-rest blood pressure among sedentary women. Int. J. Cardiovasc. Sci. 2011, 24, 163–168. [Google Scholar]
- Robergs, R. JEP Online Journal of Exercise Physiology Online. 2014. Available online: https://d1wqtxts1xzle7.cloudfront.net/33678326/ENERGY_COST_AND_PHYSIOLOGICAL_EFFICIENCY_IN_MALE_YOGA_PRACTITIONERS.pdf?1399878894=&response-content-disposition=inline%3B+filename%3DENERGY_COST_AND_PHYSIOLOGICAL_EFFICIENCY.pdf&Expires=1636340622&Signature=Felqh2JJJUuoFQr7AYwYyggMpBmLG~QQCJymo474e6aOoMK4cEZUGioYuDJfwqhU137ofFD8xmsfb6TPc-vfZKmkb~x8L85uANDulEKA012lk9cIXYgmR611LBhfuGgnAosw8A9XUUB~u176LjOBs1qg4hcaOh6ticjKH~dLbfbq5m~BZZHGK0yRYANoF1ZmtYdJuHfulhRWyKmqUz8qXLq-awRChScmrFZPn~E~JXN5eYmOqNy967C8BQp2VhkpjTnAlAyjrPvhvoGuICIG4rGLE7lZmG0stLpA~zDoPOM5QukTsPlCC7Lx2EZjcVOuHX0bKWJf050An-jK0xcqqA__&Key-Pair-Id=APKAJLOHF5GGSLRBV4ZA (accessed on 24 August 2021).
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Liu, C.K.; Leng, X.; Hsu, F.C.; Kritchevsky, S.B.; Ding, J.; Earnest, C.P.; Ferrucci, L.; Goodpaster, B.H.; Guralnik, J.M.; Lenchik, L.; et al. The impact of sarcopenia on a physical activity intervention: The lifestyle interventions and independence for elders pilot study (LIFE-P). J. Nutr. Health Aging 2014, 18, 59–64. [Google Scholar] [CrossRef]
- Verlaan, S.; Aspray, T.J.; Bauer, J.M.; Cederholm, T.; Hemsworth, J.; Hill, T.R.; McPhee, J.S.; Piasecki, M.; Seal, C.; Sieber, C.C.; et al. Nutritional status, body composition, and quality of life in community-dwelling sarcopenic and non-sarcopenic older adults: A case-control study. Clin. Nutr. 2017, 36, 267–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, M.; Nishiguchi, S.; Fukutani, N.; Tanigawa, T.; Yukutake, T.; Kayama, H.; Aoyama, T.; Arai, H. Prevalence of sarcopenia in community-dwelling Japanese older adults. J. Am. Med. Dir. Assoc. 2013, 14, 911–915. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Khanal, P.; Morse, C.I.; Williams, A.; Thomis, M. Differentially methylated gene patterns between age-matched sarcopenic and non-sarcopenic women. J. Cachexia Sarcopenia Muscle 2019, 10, 1295–1306. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.M.; Heishman, A.D.; Freitas, E.D.S.; Bemben, M.G. Comparing the acute effects of intermittent and continuous whole-body vibration exposure on neuromuscular and functional measures in sarcopenia and nonsarcopenic elderly women. Dose-Response 2018, 16, 1559325818797009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, N.; Pang, M.Y.C.; Ng, S.S.M.; Ng, G.Y.F. Optimal frequency/time combination of whole body vibration training for developing physical performance of people with sarcopenia: A randomized controlled trial. Clin. Rehabil. 2017, 31, 1313–1321. [Google Scholar] [CrossRef]
- David, S.; Filho, S.; Bernardo, R.M.; Santos, F.A.; Meyer, P.F.; Ronzio, O.A.; Speranza, S.; Guedes, V.; Gass, R.; Cardoso, D.M.; et al. Exercícios de vibração de corpo inteiro em plataformas vibratórias: Interesse Científico. Saúde 2015, 41, 19–26. [Google Scholar]
- Rittweger, J.; Beller, G.; Felsenberg, D. Acute physiological effects of exhaustive whole-body vibration exercise in man. Clin. Physiol. 2000, 20, 134–142. [Google Scholar] [CrossRef]
- Hazell, T.J.; Thomas, G.W.R.; DeGuire, J.R.; Lemon, P.W.R. Vertical whole-body vibration does not increase cardiovascular stress to static semi-squat exercise. Eur. J. Appl. Physiol. 2008, 104, 903–908. [Google Scholar] [CrossRef]
- Polito, M.D.; Farinatti, P.T.V. Respostas de frequência cardíaca, pressão arterial e duplo-produto ao exercício contra-resistência: Uma revisão da literatura. Rev. Port. Ciências Desporto 2003, 2003, 79–91. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- American Heart Association. Diretrizes de RCP e ACE.; American Heart Association: Chicago, IL, USA, 2020; Volume 32. [Google Scholar]
- Dias, T.; Polito, M. Acute Cardiovascular Response during Resistance Exercise with Whole-body Vibration in Sedentary Subjects: A Randomized Cross-over Trial. Res. Sport. Med. 2015, 23, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Bastos, G.; Fagundes, A.D.A.; Angela, E.; Schiavo, L. Journal of Bodywork & Movement Therapies Acute effects of whole body vibration on heart rate variability in elderly people. J. Bodyw. Mov. Ther. 2018, 22, 618–621. [Google Scholar] [CrossRef]
- Pinheiro, F.A.; Viana, B.; Pires, F.O. Ratings of perceived exertion as an indicator of the tolerable exercise duration. Motricidade 2014, 10, 100–106. [Google Scholar] [CrossRef]
- Monteiro, W.; Simão, R.; Farinatti, P. Manipulação na ordem dos exercícios e sua influência sobre número de repetições e percepção subjetiva de esforço em mulheres treinadas. Rev. Bras. Med. Esporte 2005, 11, 146–150. [Google Scholar] [CrossRef] [Green Version]
- Fornitano, L.D.; De Godoy, M.F. Increased rate-pressure product as predictor for the absence of significant obstructive coronary artery disease in patients with positive exercise test. Arq. Bras. Cardiol. 2006, 86, 138–144. [Google Scholar] [CrossRef]
- Aoyama, A.; Yamaoka-Tojo, M.; Obara, S.; Shimizu, E.; Fujiyoshi, K.; Noda, C.; Matsunaga, A.; Ako, J. Acute effects of whole-body vibration training on endothelial function and cardiovascular response in elderly patients with cardiovascular disease: A single-arm pilot study. Int. Heart J. 2019, 60, 854–861. [Google Scholar] [CrossRef] [Green Version]
- Vlachopoulos, C.; Aznaouridis, K.; Rourke, M.F.O.; Safar, M.E.; Baou, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: A systematic review and metaanalysis. Eur. Heart J. 2010, 31, 1865–1871. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, M.; Bosco, C. The use of vibration as an exercise intervention. Exerc. Sport Sci. Rev. 2003, 31, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Lythgo, N.; Eser, P.; De Groot, P.; Galea, M. Whole-body vibration dosage alters leg blood flow. Clin. Physiol. Funct. Imaging 2009, 29, 53–59. [Google Scholar] [CrossRef]
- Kerschan-Schindl, K.; Grampp, S.; Henk, C.; Resch, H.; Preisinger, E.; Fialka-Moser, V.; Imhof, H. Whole-body vibration exercise leads to alterations in muscle blood volume. Clin. Physiol. 2001, 21, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Maloney-Hinds, C.; Petrofsky, J.S.; Zimmerman, G.; Hessinger, D.A. The Role of Nitric Oxide in Skin Blood Flow Increases Due to Vibration in Healthy Adults and Adults with Type 2 Diabetes. Diabetes Technol. Ther. 2009, 11, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Ng, G.; Yuen, K. Acute effects of whole-body vibration on trunk muscle functioning in young healthy adults. J. Strength Cond. Res. 2014, 28, 2872–2879. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | NSG (n = 20) | SG (n = 20) | p-Value |
|---|---|---|---|
| Demographic and body composition | |||
| Age (years) | 72.4 (69.1–75.8) | 71.6 (67.7–75.5) | 0.73 |
| Sex (Men/Women) | 11/9 | 11/9 | |
| BMI (kg/m2) | 24.9 (23.7–26.2) | 21.2 (20.2–22.2) | 0.01 |
| BF (%) | 32.8 (29.8–35.8) | 31.7 (27.8–35.7) | 0.65 |
| Lean mass (kg) | 39.4.1 (35.9–42.8) | 33.4 (30.1 -36.6) | 0.01 |
| Fat mass (kg) | 19.1 (17.2–20.9) | 15.5 (13.4–17.7) | 0.01 |
| RSMI Men | 8.0 (7.5–8.6) | 6.5 (6.1–6.9) | 0.01 |
| RSMI Women | 6.4 (5.9–6.7) | 5.2 (5.0–5.4) | 0.01 |
| Strength and functional tests | |||
| SPPB (points) | 10.7 (10.3–11.2) | 10.1 (9.5–10.8) | 0.21 |
| 5STS (s) | 9.1 (8.3–9.8) | 10.9 (9.8–12.1) | 0.01 |
| Walking speed (m/s) | 1.9 (1.7–2.0) | 1.7 (1.5–1.8) | 0.06 |
| Handgrip strength (kgf) | 34.8 (30.7–39.0) | 31.8 (27.0–36.5) | 0.31 |
| Men Handgrip strength (kgf) | 41.2 (34.5–47.9) | 41.2 (38.9–43.4) | 0.98 |
| Women Handgrip strength (kgf) | 29.6 (26.4–32.8) | 24.1 (19.6–28.6) | 0.05 |
| Medicines | |||
| Antihypertensives | 9 (45%) | 9 (45%) | |
| Statins | 1 (5%) | 3 (15%) | |
| Oral antidiabetics | 0 (0%) | 1 (5%) | |
| Anticoagulant | 1 (5%) | 0 (0%) | |
| Antirheumatics | 0 (0%) | 1 (5%) | |
| Antidepressants | 1 (5%) | 0 (0%) | |
| None | 10 (50%) | 11 (55%) |
| Outcomes | Intervention | NSG | SG |
|---|---|---|---|
| Δ HR, bpm | Without WBV | 1.80 (−0.82–4.43) | 3.50 (0.90–6.2) |
| WBV | 6.30 (3.68–8.92) | 7.10 (4.44–9.70) | |
| Mean Difference | 4.50 (0.78–8.20) * | 3.50 (−0.177–7.24) | |
| Δ peak HR, bpm | Without WBV | 4.90 (2.20–7.60) | 7.20 (4.46–9.94) |
| WBV | 11.60 (8.86–14.34) | 13.55 (10.81–16.30) | |
| Mean Difference | 6.70 (2.83–10.57) * | 6.35 (2.47–10.22) * | |
| Δ SBP, mmHg | Without WBV | −2.00 (−6.54–2.54) | −1.00 (−5.54–3.54) |
| WBV | 4.00 (−0.54–8.54) | −2.00 (−6.54–2.54) | |
| Mean Difference | 6.00 (−0.42–12.42) | 1.00 (−5.42–7.42) | |
| Δ DBP, mmHg | Without WBV | 0.00 (−3.50–3.50) | −0.50 (−3.40–2.99) |
| WBV | 1.50 (−1.99–4.99) | 2.00 (−1.50–5.50) | |
| Mean Difference | 1.50 (−3.44–6.44) | 2.50 (−2.44–7.44) | |
| Δ MAP, mmHg | Without WBV | 0.17 (−4.80–5.13) | 1.17 (−3.80–6.13) |
| WBV | −10.67 (−15.63–−5.70) | 2.66 (−2.30–7.63) | |
| Mean Difference | −10.83 (−17.85–−3.81) * | −1.50 (−8.52–−5.52) | |
| Δ DP, mmHg, bpm | Without WBV | 110.60 (−370.36 −591.56) | 365.90 (−115.06–846.86) |
| WBV | 1160.75 (679.73–1641.70) | 822.85 (341.90–1303.80) | |
| Mean Difference | 1050.15 (369.97–1730.33) * | 456.95 (−223.23–1137.13) | |
| Without WBV | 0.00 (−0.05–0.05) | 0.00 (−0.056–0.056) | |
| Δ SPE, points | WBV | 0.05 (−0.006–0.106) | 0.02 (−0.03–0.08) |
| Mean Difference | −0.05 (-0.13–0.03) | −0.02 (−0.10–0.05) |
| Outcomes | Between Groups (NSG vs. SG) | Within Groups (Without-WBV vs. WBV) | Interaction | |||
|---|---|---|---|---|---|---|
| p | F | p | F | p | F | |
| Δ HR, bpm | 0.35 | 0.89 | 0.003 | 9.3 | 0.72 | 0.13 |
| Δ peak HR, bpm | 0.12 | 2.38 | 0.000 | 22.51 | 0.89 | 0.02 |
| Δ SBP, mmHg | 0.28 | 1.20 | 0.28 | 1.20 | 0.13 | 2.36 |
| Δ DBP, mmHg | 1.00 | 0.00 | 0.26 | 1.30 | 0.78 | 0.08 |
| Δ MAP, mmHg | 0.005 | 8.27 | 0.06 | 3.50 | 0.02 | 6.12 |
| Δ DP, mmHg, bpm | 0.86 | 0.03 | 0.003 | 9.74 | 0.22 | 1.50 |
| Δ SPE, points | 0.65 | 0.20 | 0.18 | 1.80 | 0.65 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Paula, F.A.; Mendonça, V.A.; Lage, V.K.d.S.; da Silva, G.P.; de Almeida, H.C.; Lima, L.P.; Santos, J.N.V.; de Castro, D.P.; da Paixão, C.F.; Rodrigues, A.L.d.S.N.T.; et al. Immediate Effects of Whole-Body Vibration Associated with Squatting Exercises on Hemodynamic Parameters in Sarcopenic Older People: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 11852. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211852
de Paula FA, Mendonça VA, Lage VKdS, da Silva GP, de Almeida HC, Lima LP, Santos JNV, de Castro DP, da Paixão CF, Rodrigues ALdSNT, et al. Immediate Effects of Whole-Body Vibration Associated with Squatting Exercises on Hemodynamic Parameters in Sarcopenic Older People: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(22):11852. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211852
Chicago/Turabian Stylede Paula, Fabiana Angélica, Vanessa Amaral Mendonça, Vanessa Kelly da Silva Lage, Guilherme Pinto da Silva, Hellen Cristina de Almeida, Liliana Pereira Lima, Joyce Noelly Vítor Santos, Daniela Pereira de Castro, Camila Franciele da Paixão, Ana Luiza da Silva Nunes Teixeira Rodrigues, and et al. 2021. "Immediate Effects of Whole-Body Vibration Associated with Squatting Exercises on Hemodynamic Parameters in Sarcopenic Older People: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 22: 11852. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211852