
Vocational Interventions to Improve Employment Participation of People with Psychosocial Disability, Autism and/or Intellectual Disability: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources, Search Strategy and Selection Process
2.3. Data Extraction and Data Items
2.4. Risk of Bias Assessment
2.5. Synthesis
3. Results
3.1. Study Characteristics
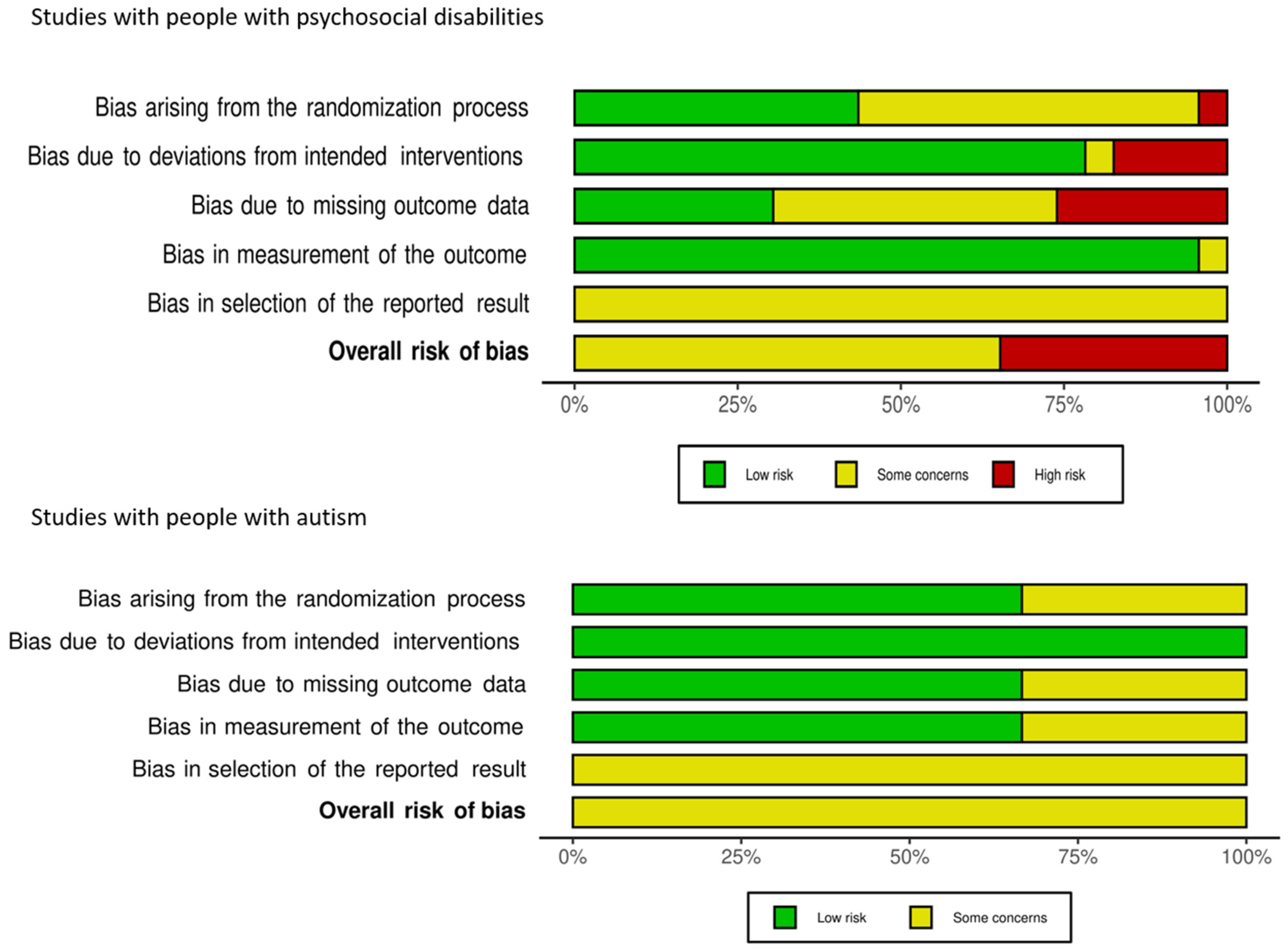
3.2. Risk of Bias Assessment
3.3. Psychosocial Disability
3.3.1. Primary Outcomes: Studies with Moderate Risk of Bias
3.3.2. Primary Outcomes: Studies with High Risk of Bias
3.3.3. Secondary Outcomes: Moderate Risk of Bias
3.3.4. Secondary Outcomes: High Risk of Bias
3.4. Autism
Primary Outcomes: Moderate Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Modini, M.; Joyce, S.; Mykletun, A.; Christensen, H.; Bryant, R.A.; Mitchell, P.B.; Harvey, S.B. The mental health benefits of employment: Results of a systematic meta-review. Australas. Psychiatry 2016, 24, 331–336. [Google Scholar] [CrossRef]
- Krasovitsky, M.; Zaballa, A.; Purcell, D. Willing to Work: National Inquiry into Employment Discrimination against Older Australians and Australians with Disability; Australian Human Rights Commission: Sydney, Australia, 2016. Available online: http://dea.conferenceworks.com.au (accessed on 16 July 2021).
- Frederick, D.E.; VanderWeele, T.J. Supported employment: Meta-analysis and review of randomized controlled trials of individual placement and support. PLoS ONE 2019, 14, e0212208. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; LaMontagne, A.D.; Aitken, Z.; Bentley, R.; Kavanagh, A.M. Employment status and mental health among persons with and without a disability: Evidence from an Australian cohort study. J. Epidemiol. Community Health 2014, 68, 1064–1071. [Google Scholar] [CrossRef]
- Aitken, Z.; Simpson, J.A.; Bentley, R.; Milner, A.; LaMontagne, A.D.; Kavanagh, A.M. Does the effect of disability acquisition on mental health differ by employment characteristics? A longitudinal fixed-effects analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 1031–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milner, A.; King, T.L.; LaMontagne, A.D.; Aitken, Z.; Petrie, D.; Kavanagh, A.M. Underemployment and its impacts on mental health among those with disabilities: Evidence from the HILDA cohort. J. Epidemiol. Community Health 2017, 71, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Mithen, J.; Aitken, Z.; Ziersch, A.; Kavanagh, A.M. Inequalities in social capital and health between people with and without disabilities. Soc. Sci. Med. 2015, 126, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Aitken, Z.; Simpson, J.A.; Bentley, R.; Kavanagh, A.M. Disability acquisition and mental health: Effect modification by demographic and socioeconomic characteristics using data from an Australian longitudinal study. BMJ Open 2017, 7, e016953. [Google Scholar] [CrossRef] [Green Version]
- Kavanagh, A.M.; Aitken, Z.; Baker, E.; LaMontagne, A.D.; Milner, A.; Bentley, R. Housing tenure and affordability and mental health following disability acquisition in adulthood. Soc. Sci. Med. 2016, 151, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Deloitte Access Economics. The Economic Benefits of Increasing Employment for People with Disability; Commissioned by the Australian Network on Disability; Deloitte Access Economics: Sydney, Australia, 2011. [Google Scholar]
- Organisation for Economic Cooperation and Development. Sickness, Disability and Work: Keeping on Track in the Economic Downturn. In Proceedings of the High-Level Forum, Stockholm, Sweden, 14–15 May 2009; pp. 14–15. [Google Scholar]
- Mizunoya, S.; Mitra, S. Is there a disability gap in employment rates in developing countries? World Dev. 2013, 42, 28–43. [Google Scholar] [CrossRef] [Green Version]
- US Bureau of Labour Statistics. Persons with a Disability: Labor Force Characteristics Summary. Available online: https://www.bls.gov/news.release/disabl.nr0.htm# (accessed on 7 June 2021).
- Powell, A. Disabled People in Employment; House of Commons: London, UK, 2021.
- Australian Bureau of Statistics. Disability, Ageing and Carers, Australia: Summary of Findings, 2018. Cat. 4430.0. Available online: https://www.abs.gov.au/ausstats/[email protected]/mf/4430.0 (accessed on 10 July 2021).
- Australian Bureau of Statistics. Disability and the Labour Force. 2018. Available online: https://www.abs.gov.au/articles/disability-and-labour-force#key-statistics (accessed on 30 May 2021).
- Office of National Statistics. Outcomes for Disabled People in the UK. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/disability/articles/outcomesfordisabledpeopleintheuk/2020 (accessed on 7 June 2021).
- Australian Bureau of Statistics. Psychosocial Disability. Available online: https://www.abs.gov.au/articles/psychosocial-disability#employment (accessed on 10 July 2021).
- Australian Bureau of Statistics. Autism in Australia. Available online: https://www.abs.gov.au/statistics/health/disability/disability-ageing-and-carers-australia-summary-findings/2018#autism-in-australia (accessed on 7 June 2021).
- Suijkerbuijk, Y.B.; Schaafsma, F.G.; van Mechelen, J.C.; Ojajärvi, A.; Corbiere, M.; Anema, J.R. Interventions for obtaining and maintaining employment in adults with severe mental illness, a network meta-analysis. Cochrane Database Syst. Rev. 2017, 9, CD011867. [Google Scholar] [CrossRef] [PubMed]
- Waghorn, G.; Killackey, E.; Dickson, P.; Brock, L.; Skate, C. Evidence-based supported employment for people with psychiatric disabilities in Australia: Progress in the past 15 years. Psychiatr. Rehabil. J. 2020, 43, 32. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, J.; Pilkington, P. Supported employment for persons with mental illness: Systematic review of the effectiveness of individual placement and support in the UK. J. Ment. Health 2011, 20, 368–380. [Google Scholar] [CrossRef]
- Noel, V.A.; Bond, G.R.; Drake, R.E.; Becker, D.R.; McHugo, G.J.; Swanson, S.J.; Luciano, A.E.; Greene, M.A. Barriers and facilitators to sustainment of an evidence-based supported employment program. Adm. Policy Ment. Health Ment. Health Serv. Res. 2017, 44, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Modini, M.; Tan, L.; Brinchmann, B.; Wang, M.-J.; Killackey, E.; Glozier, N.; Mykletun, A.; Harvey, S.B. Supported employment for people with severe mental illness: Systematic review and meta-analysis of the international evidence. Br. J. Psychiatry 2016, 209, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Bond, G.R.; Drake, R.E.; Pogue, J.A. Expanding individual placement and support to populations with conditions and disorders other than serious mental illness. Psychiatr. Serv. 2019, 70, 488–498. [Google Scholar] [CrossRef]
- McLaren, J.; Lichtenstein, J.D.; Lynch, D.; Becker, D.; Drake, R. Individual placement and support for people with autism spectrum disorders: A pilot program. Adm. Policy Ment. Health Ment. Health Serv. Res. 2017, 44, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Bond, G.R.; Kim, S.J.; Becker, D.R.; Swanson, S.J.; Drake, R.E.; Krzos, I.M.; Fraser, V.V.; O’Neill, S.; Frounfelker, R.L. A controlled trial of supported employment for people with severe mental illness and justice involvement. Psychiatr. Serv. 2015, 66, 1027–1034. [Google Scholar] [CrossRef]
- Davis, L.L.; Leon, A.C.; Toscano, R.; Drebing, C.E.; Ward, L.C.; Parker, P.E.; Kashner, T.M.; Drake, R.E. A randomized controlled trial of supported employment among veterans with posttraumatic stress disorder. Psychiatr. Serv. 2012, 63, 464–470. [Google Scholar] [CrossRef]
- Davis, M.; Sheidow, A.J.; McCart, M.R.; Perrault, R.T. Vocational coaches for justice-involved emerging adults. Psychiatr. Rehabil. J. 2018, 41, 266. [Google Scholar] [CrossRef]
- Riesen, T.; Morgan, R.L.; Griffin, C. Customized employment: A review of the literature. J. Vocat. Rehabil. 2015, 43, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Wehman, P.; Brooke, V.; Brooke, A.M.; Ham, W.; Schall, C.; McDonough, J.; Lau, S.; Seward, H.; Avellone, L. Employment for adults with autism spectrum disorders: A retrospective review of a customized employment approach. Res. Dev. Disabil. 2016, 53, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Elinson, L.; Frey, W.D.; Li, T.; Palan, M.A.; Horne, R.L. Evaluation of customized employment in building the capacity of the workforce development system. J. Vocat. Rehabil. 2008, 28, 141–158. [Google Scholar]
- Scott, M.; Milbourn, B.; Falkmer, M.; Black, M.; Bölte, S.; Halladay, A.; Lerner, M.; Taylor, J.L.; Girdler, S. Factors impacting employment for people with autism spectrum disorder: A scoping review. Autism 2019, 23, 869–901. [Google Scholar] [CrossRef] [PubMed]
- Galletly, C.; Castle, D.; Dark, F.; Humberstone, V.; Jablensky, A.; Killackey, E.; Tran, N. Royal Australian New Zealand College of Psychiatrists. The economic cost of serious mental illness and comorbidities in Australia and New Zealand. Aust. N. Z. J. Psychiatry 2016, 50, 410–472. [Google Scholar] [CrossRef] [Green Version]
- Crowther, R.; Marshall, M.; Bond, G.R.; Huxley, P. Vocational Rehabilitation for People with Severe Mental Illness. Cochrane Database Syst. Rev. 2001, 2001, CD003080. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003080/full (accessed on 1 October 2020). [CrossRef] [PubMed] [Green Version]
- Kinoshita, Y.; Furukawa, T.A.; Kinoshita, K.; Honyashiki, M.; Omori, I.M.; Marshall, M.; Kingdon, D. Supported Employment for Adults with Severe Mental Illness. Cochrane Database Syst. Rev. 2013, 9, CD008297. [Google Scholar] [CrossRef] [Green Version]
- National Disability Insurance Agency. NDIS Participant Employment Strategy 2019–2022; Palgrave Macmillan: Singapore, 2019; pp. 285–304.
- World Bank. High Income Data. Available online: https://data.worldbank.org/country/XD (accessed on 5 October 2020).
- Hedley, D.; Uljarević, M.; Cameron, L.; Halder, S.; Richdale, A.; Dissanayake, C. Employment Programmes and Interventions Targeting Adults with Autism Spectrum Disorder: A Systematic Review of the Literature. Autism 2017, 21, 929–941. [Google Scholar] [CrossRef]
- Cheng, C.; Oakman, J.; Bigby, C.; Fossey, E.; Cavanagh, J.; Meacham, H.; Bartram, T. What Constitutes Effective Support in Obtaining and Maintaining Employment for Individuals with Intellectual Disability? A Scoping Review. J. Intellect. Dev. Disabil. 2018, 43, 317–327. [Google Scholar] [CrossRef]
- Veritas Health Innovation. Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2014.
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Heslin, M.; Howard, L.; Leese, M.; McCrone, P.; Rice, C.; Jarrett, M.; Spokes, T.; Huxley, P.; Thornicroft, G. Randomized controlled trial of supported employment in England: 2 year follow-up of the Supported Work and Needs (SWAN) study. World Psychiatry 2011, 10, 132. [Google Scholar] [CrossRef]
- Hoffmann, H.; Jäckel, D.; Glauser, S.; Mueser, K.T.; Kupper, Z. Long-term effectiveness of supported employment: 5-year follow-up of a randomized controlled trial. Am. J. Psychiatry 2014, 171, 1183–1190. [Google Scholar] [CrossRef]
- Wehman, P.H.; Schall, C.M.; McDonough, J.; Kregel, J.; Brooke, V.; Molinelli, A.; Ham, W.; Graham, C.W.; Riehle, J.E.; Collins, H.T. Competitive employment for youth with autism spectrum disorders: Early results from a randomized clinical trial. J. Autism Dev. Disord. 2014, 44, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Bejerholm, U.; Areberg, C.; Hofgren, C.; Sandlund, M.; Rinaldi, M. Individual placement and support in Sweden—A randomized controlled trial. Nord. J. Psychiatry 2015, 69, 57–66. [Google Scholar] [CrossRef]
- Hoffmann, H.; Jäckel, D.; Glauser, S.; Kupper, Z. A randomised controlled trial of the efficacy of supported employment. Acta Psychiatr. Scand. 2012, 125, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Lecomte, T.; Corbière, M.; Giguère, C.-E.; Titone, D.; Lysaker, P. Group cognitive behaviour therapy for supported employment–results of a randomized controlled cohort trial. Schizophr. Res. 2020, 215, 126–133. [Google Scholar] [CrossRef]
- McGurk, S.R.; Mueser, K.T.; Xie, H.; Welsh, J.; Kaiser, S.; Drake, R.E.; Becker, D.R.; Bailey, E.; Fraser, G.; Wolfe, R. Cognitive enhancement treatment for people with mental illness who do not respond to supported employment: A randomized controlled trial. Am. J. Psychiatry 2015, 172, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Michon, H.; van Busschbach, J.T.; Stant, A.D.; van Vugt, M.D.; van Weeghel, J.; Kroon, H. Effectiveness of individual placement and support for people with severe mental illness in the Netherlands: A 30-month randomized controlled trial. Psychiatr. Rehabil. J. 2014, 37, 129. [Google Scholar] [CrossRef] [Green Version]
- Oshima, I.; Sono, T.; Bond, G.R.; Nishio, M.; Ito, J. A randomized controlled trial of individual placement and support in Japan. Psychiatr. Rehabil. J. 2014, 37, 137. [Google Scholar] [CrossRef]
- Poremski, D.; Rabouin, D.; Latimer, E. A randomised controlled trial of evidence based supported employment for people who have recently been homeless and have a mental illness. Adm. Policy Ment. Health Ment. Health Serv. Res. 2017, 44, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Russinova, Z.; Gidugu, V.; Bloch, P.; Restrepo-Toro, M.; Rogers, E.S. Empowering individuals with psychiatric disabilities to work: Results of a randomized trial. Psychiatr. Rehabil. J. 2018, 41, 196. [Google Scholar] [CrossRef]
- Schneider, J.; Akhtar, A.; Boycott, N.; Guo, B.; Latimer, E.; Cao, Z.; McMurran, M. Individual placement and support versus individual placement and support enhanced with work-focused cognitive behaviour therapy: Feasibility study for a randomised controlled trial. Br. J. Occup. Ther. 2016, 79, 257–269. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.J.; Fleming, M.F.; Wright, M.A.; Jordan, N.; Humm, L.B.; Olsen, D.; Bell, M.D. Job offers to individuals with severe mental illness after participation in virtual reality job interview training. Psychiatr. Serv. 2015, 66, 1173–1179. [Google Scholar] [CrossRef]
- Tsang, H.W.; Fung, K.M.; Leung, A.Y.; Li, S.M.; Cheung, W. Three year follow-up study of an integrated supported employment for individuals with severe mental illness. Aust. N. Z. J. Psychiatry 2010, 44, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Waghorn, G.; Dias, S.; Gladman, B.; Harris, M.; Saha, S. A multi-site randomised controlled trial of evidence-based supported employment for adults with severe and persistent mental illness. Aust. Occup. Ther. J. 2014, 61, 424–436. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Sato, S.; Horio, N.; Yoshida, K.; Shimodaira, M.; Taneda, A.; Ikebuchi, E.; Nishio, M.; Ito, J. Cost-effectiveness of cognitive remediation and supported employment for people with mental illness: A randomized controlled trial. Psychol. Med. 2017, 47, 53. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.J.; Fleming, M.F.; Wright, M.A.; Roberts, A.G.; Humm, L.B.; Olsen, D.; Bell, M.D. Virtual reality job interview training and 6-month employment outcomes for individuals with schizophrenia seeking employment. Schizophr. Res. 2015, 166, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Nuechterlein, K.H.; Subotnik, K.L.; Ventura, J.; Turner, L.R.; Gitlin, M.J.; Gretchen-Doorly, D.; Becker, D.R.; Drake, R.E.; Wallace, C.J.; Liberman, R.P. Enhancing return to work or school after a first episode of schizophrenia: The UCLA RCT of Individual Placement and Support and Workplace Fundamentals Module training. Psychol. Med. 2020, 50, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Twamley, E.W.; Vella, L.; Burton, C.Z.; Becker, D.R.; Bell, M.D.; Jeste, D.V. The efficacy of supported employment for middle-aged and older people with schizophrenia. Schizophr. Res. 2012, 135, 100–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killackey, E.; Allott, K.; Jackson, H.J.; Scutella, R.; Tseng, Y.-P.; Borland, J.; Proffitt, T.-M.; Hunt, S.; Kay-Lambkin, F.; Chinnery, G. Individual placement and support for vocational recovery in first-episode psychosis: Randomised controlled trial. Br. J. Psychiatry 2019, 214, 76–82. [Google Scholar] [CrossRef]
- Craig, T.; Shepherd, G.; Rinaldi, M.; Smith, J.; Carr, S.; Preston, F.; Singh, S. Vocational rehabilitation in early psychosis: Cluster randomised trial. Br. J. Psychiatry 2014, 205, 145–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erickson, D.H.; Roes, M.M.; DiGiacomo, A.; Burns, A. “Individual Placement and Support” boosts employment for early psychosis clients, even when baseline rates are high. Early Interv. Psychiatry 2020, 15, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Wehman, P.; Schall, C.; McDonough, J.; Sima, A.; Brooke, A.; Ham, W.; Whittenburg, H.; Brooke, V.; Avellone, L.; Riehle, E. Competitive employment for transition-aged youth with significant impact from autism: A multi-site randomized clinical trial. J. Autism Dev. Disord. 2020, 50, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Whittenburg, H.N.; Schall, C.M.; Wehman, P.; McDonough, J.; DuBois, T. Helping high school-aged military dependents with autism gain employment through project SEARCH+ ASD supports. Mil. Med. 2020, 185, 663–668. [Google Scholar] [CrossRef] [Green Version]
- Howard, L.M.; Heslin, M.; Leese, M.; McCrone, P.; Rice, C.; Jarrett, M.; Spokes, T.; Huxley, P.; Thornicroft, G. Supported employment: Randomised controlled trial. Br. J. Psychiatry 2010, 196, 404–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wehman, P.; Schall, C.M.; McDonough, J.; Graham, C.; Brooke, V.; Riehle, J.E.; Brooke, A.; Ham, W.; Lau, S.; Allen, J. Effects of an employer-based intervention on employment outcomes for youth with significant support needs due to autism. Autism 2017, 21, 276–290. [Google Scholar] [CrossRef] [PubMed]
- Knapp, M.; Patel, A.; Curran, C.; Latimer, E.; Catty, J.; Becker, T.; Drake, R.E.; Fioritti, A.; Kilian, R.; Lauber, C. Supported employment: Cost-effectiveness across six European sites. World Psychiatry 2013, 12, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evensen, S.; Wisløff, T.; Lystad, J.U.; Bull, H.; Martinsen, E.W.; Ueland, T.; Falkum, E. Exploring the potential cost-effectiveness of a vocational rehabilitation program for individuals with schizophrenia in a high-income welfare society. BMC Psychiatry 2019, 19, 140. [Google Scholar] [CrossRef] [Green Version]
- Dixon, L.; Hoch, J.S.; Clark, R.; Bebout, R.; Drake, R.; McHugo, G.; Becker, D. Cost-effectiveness of two vocational rehabilitation programs for persons with severe mental illness. Psychiatr. Serv. 2002, 53, 1118–1124. [Google Scholar] [CrossRef] [Green Version]
- Christensen, T.N.; Kruse, M.; Hellström, L.; Eplov, L.F. Cost-utility and cost-effectiveness of individual placement support and cognitive remediation in people with severe mental illness: Results from a randomized clinical trial. Psychol. Med. 2017, 47, 53–65. [Google Scholar] [CrossRef] [PubMed]
- LaMontagne, A.; Krnjacki, L.; Milner, A.; Butterworth, P.; Kavanagh, A. Psychosocial job quality in a national sample of working Australians: A comparison of persons working with versus without disability. Soc. Sci. Med. Popul. Health 2016, 2, 175–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Labour Organization. The ILOs Decent Work Agenda. Available online: https://www.ilo.org/global/topics/decent-work/lang--en/index.htm (accessed on 2 July 2021).
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 2015. [Google Scholar]
- Richter, D.; Hoffmann, H. Effectiveness of supported employment in non-trial routine implementation: Systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 525–531. [Google Scholar] [CrossRef]
- Smith, D.L.; Atmatzidis, K.; Capogreco, M.; Lloyd-Randolfi, D.; Seman, V. Evidence-Based Interventions for Increasing Work Participation for Persons with Various Disabilities: A Systematic Review. OTJR Occup. Particip. Health 2017, 37, 3S–13S. [Google Scholar] [CrossRef]
- Greig, R.; Chapman, P.; Eley, A.; Watts, R.; Love, B.; Bourlet, G. The Cost Effectiveness of Employment Support for People with Disabilities; Final Detailed Research Report. Available online: https://www.basw.co.uk/system/files/resources/basw_115259-5_0.pdf (accessed on 1 October 2020).
- Tune, D. Dedifferentiation and people with intellectual disabilities in the Australian National Disability Insurance Scheme: Bringing research, politics and policy together. J. Intellect. Dev. Disabil. 2020, 45, 309–319. [Google Scholar]
- Johnson, S.; Kuhlmann, R.; Group, E. The European service mapping schedule (ESMS): Development of an instrumentfor the description and classificationof mental health services. Acta Psychiatr. Scand. 2000, 102, 14–23. [Google Scholar] [CrossRef]
- Xu, T.; Stancliffe, R.J. An evaluation of employment outcomes achieved by transition to work service providers in Sydney, Australia. J. Intellect. Dev. Disabil. 2019, 44, 51–63. [Google Scholar] [CrossRef]
- ARTD Consultants. Ticket to Work Outcomes Evaluation—Customised Employment Report. A Report for National Disability Services. Available online: https://tickettowork.org.au/media/research_submissions_files/Customised-Employment-Outcomes-final.pdf (accessed on 20 August 2021).
- Langi, F.F.G.; Oberoi, A.; Balcazar, F.E.; Awsumb, J. Vocational rehabilitation of transition-age youth with disabilities: A propensity-score matched study. J. Occup. Rehabil. 2017, 27, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Kaya, C.; Chan, F.; Rumrill, P.; Hartman, E.; Wehman, P.; Iwanaga, K.; Pai, C.-H.; Avellone, L. Vocational rehabilitation services and competitive employment for transition-age youth with autism spectrum disorders. J. Vocat. Rehabil. 2016, 45, 73–83. [Google Scholar] [CrossRef]
- Devine, A.; Vaughan, C.; Kavanagh, A. If I had stable housing I would be a bit more receptive to having a job. Factors influencing the effectiveness of Disability Employment Services reform. Work 2020, 65, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Mellifont, D. DESperately Seeking Service: A narrative review informing a disability employment services reform framework for Australians with mental illness. Work 2017, 58, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, J.D.; Drake, R.E.; Bond, G.R. Economic, labor, and regulatory moderators of the effect of individual placement and support among people with severe mental illness: A systematic review and meta-analysis. Schizophr. Bull. 2018, 44, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Cooperation and Development. OECD Employment Outlook 2020: Worker Security and the COVID-19 Crisis; Organization for Economic Co-Operation and Development: Paris, France, 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Studies with People with Psychosocial Disabilities | ||||||
|---|---|---|---|---|---|---|
| Study, Country | N Total (Control/Intervention) | Male Participants (%) | Age Range | Mean Age (SD) Total, Control, Intervention | Description of Psychosocial Disabilities (%) | Employment Status at Baseline |
| Bejerholm 2015, Sweden [46] | 120 (60/60) | 55.8 | 18–63 | Total: Not reported (NR) C: 38 (8) I: 38 (8) (only provided whole digits) | 64.2% schizophrenia and other psychosis (ICD-10 F20–29), 7.5% bipolar (ICD-10 F31), 27.5% other diagnoses (ICD-10 F32 F40 F60) | Had not worked in the preceding year |
| Bond 2015, USA [27] | 90 (45/45) n = 3 dropped post-randomization and sample reduced to 87 (1 control, 2 intervention) | 79.3 | 18 or older | Total: NR C: 44.6 (11.6) I: 42.9 (11.5) | 53% schizophrenia, 18% depressive disorder, 25% bipolar disorder, 3% other (information not available) | No competitive employment in past three months |
| Craig 2014, UK [63] | 159 (78/81) | 73.0 | 18–35 | Total: NR C: Midlands 2: 24 (3.7); London 2: 24 (4.7) I: Midlands 1: 23 (4.2); London 1: 25 (4.2) (only provided whole digits) | 100% early psychosis | Unemployed |
| Davis 2012, USA [28] | 85 (43/42) | 88.2 | 19 to 60 | Total: NR C: 40.5 (12.5) I: 39.9 (11.9) | 100% post-traumatic stress disorder, 89% major depressive disorder, 20% dysthymia, 54% agoraphobia, 59% panic disorder, 28% social phobia, 42% alcohol dependence, 21% alcohol abuse, 37% drug dependence, and 18% drug abuse | Unemployed |
| Davis 2018, USA [29] | 32 (16/16) | 78.1 | 17–20 | Total: 17.8 (NR) C: 17.9 (NR) I: 17.6 (NR) | 50% major depressive disorder, 25% anxiety disorder, 16% bipolar disorder, 9% state MH Authority Services | Employed or unemployed |
| Erickson 2020, Canada [64] | 109 (53/56) | 82.6 | 18–30 | Total: NR C: 22.7 (3.3) I: 23.4 (3.5) | 4.6% schizophreniform, 37.6% schizophrenia, 8.3% schizo-affective disorder, 18.4% bipolar, 9.2% major depression, 15.6% Psychosis NOS, 4.6% substance-induced psychosis, 0.9% delusional disorder, 0.9% Aspergers | Unemployed or employed and seeking better jobs |
| Hoffmann 2012, Switzerland [47] | 100 (54/46) | 65.0 | 18–64 | Total: NR C: 34.1 (9.2) I: 33.5 (9.8) | 38% schizophrenia spectrum, 41% affective disorder, 21% other, 12% concomitant substance abuse | Out of competitive employment |
| Howard 2010, UK [67] | 219 (110/109) | 67.1 | 18–65 | Total: NR C: 38.3 (9.3) I: 38.4 (9.5) | 72.5% psychotic disorder; 27.5% mood disorder | Unemployed for at least 3 months |
| Killackey 2019, UK [62] | 146 (73/73) | 69.2 | 15–25 | Total: 20.4 (2.4) C: 20.5 (2.1) I: 20.4 (2.7) | 100% psychotic disorder including 43.8% schizophreniform/schizophrenia, 13.0% schizoaffective disorder, 11.6% major depressive disorder with psychotic features, 13.7% bipolar disorder, 11.6% psychosis not otherwise specified, 6.2% other | Unemployed or employed |
| Lecomte 2020, Canada [48] | 164 (85/79) Data recorded as treated, not as intention to treat. | 60.7% | NR | Total: 36.6 (11.3) C: 37.0 (11.6) I: 36.1 (11.0) | Severe mental illness (schizophrenia, bipolar, or major depression). Primary diagnoses: 18.5% Dx mood disorder, 7.4% Dx anxiety disorder, 0.6% Dx organic disorder, 58.6% Dx psychotic disorder, 1.2% Dx substance-related, 6.2% Dx personality disorder, 1.9% Dx developmental disorder, 5.6% Dx other. | Currently not working and seeking work, or working less than 5 h a week and wishing for another job with more hours |
| McGurk 2015, USA [49] | 107 (50/57) | 75.4 | NR | Total: 44.1 (11.0) C: 42.9 (10.7) I: 45.1 (11.3) | 23.4% schizophrenia, 22.4% schizoaffective disorder, 23.4% bipolar disorder, 16.8% major depression, 14.0% other | Not worked in past 3 months, or exited competitive job that lasted <3 months |
| Michon 2014, Netherlands [50] | 151 (80/71) | 74.2 | 18–65 | Total: NR C: 35.6 (11.0) I: 34.1 (9.9) | Clients of long-term mental health care and at baseline 93% of participants were diagnosed with one or more specific mental disorders. 50.6% psychotic disorder. Remaining participants had various diagnoses, such as enduring major depression, personality disorders, developmental disorders. At baseline 7% was assessed by mental health care professionals as ‘diagnosis postponed’ or ‘no diagnosis available’ | No paid work |
| Nuechterlein 2020, USA [60] | 69 (23/46) | 66.7 | 18–45 | Total: 24.5 C: 25.1 (3.8) I: 24.2 (4.2) | 84% schizophrenia, 14% schizoaffective disorder, depressed type, mainly schizophrenic, 2% with schizoaffective disorder, manic type, mainly schizophrenic | Employed or unemployed |
| Oshima 2014, Japan [51] | 37 (19/18) | 75.7 | 18–59 | Total: NR C: 41.1 (9.4) I: 40.1 (8.5) | Primary diagnosis of either schizophrenia, mood disorder, or neurotic disorder | Not competitively employed |
| Poremski 2017, Canada [52] | 90 (45/45) | 63.3 | 18 or older | Total: NR C: 47.1 (10.6) I: 45.2 (9.4) | 64% major depressive disorder, 22% psychotic disorder, 6% panic disorder, 4% mania-hypomania, 3% post-traumatic stress disorder | Not working |
| Russinova 2018, USA [53] | 55 (29/26 N = 4 (C:2, I:2) excluded from analysis as already in receipt of employment services) | 39.2 | 18 or older | Total: NR C: 45.3 (14.2) I: 47.0 (10.9) | 31.4% schizophrenia/schizoaffective, 31.4% bipolar, 33.3% bipolar, 2.0% post-traumatic stress disorder and anxiety/panic disorder, 2.0% personality disorder, 2.0% post-traumatic stress disorder, anxiety/panic disorder and personality disorder | Not working |
| Schneider 2016, UK [54] | 74 (37/37) | 70.3 | 18–60 | Total: NR C: 29.5 (NR) I: 30.5 (NR) | 43.2% psychosis, 23.0% schizophrenia, 14.9% bipolar disorder, 13.5% depression, 4.1% other | Not currently in work |
| Smith 2015a, USA [55] | 25 (8/17) N = 32 with participants from previous RCTs included in analysis (11 control, 21 intervention) | 53.1 | 18–55 | Total: NR C: 39.1 (10.6) I: 40.8 (12.2) | 100% schizophrenia or schizoaffective disorder | Unemployed or underemployed |
| Smith 2015b, USA [59] | 70 (22/48) | NR (68.6 at 6 months) | 18–65 | Total: NR C: 49.1 (10.9) I: 47 (12.4) | 45.1% posttraumatic stress disorder, 47.1% major depressive disorder, 33.3% bipolar disorder, 15.7% schizophrenia or schizoaffective disorder | Unemployed or underemployed |
| Tsang 2010, Hong Kong [56] | 189 (IPS 65, Integrated Supported Employment 58, TVR 66) | 49.2 | NR | Total: NR C: 36.5 (7.6) I: 34.1 (9.0) | 76.7% schizophrenia, 23.3% other | Unemployed |
| Twamley 2012, USA [61] | 58 (28/30) | 63.8 | 45 or older | Total: 51 (SD NR) C: 51.8 (5.1) I: 50.3 (3.5) | 40% schizophrenia, 60% schizoaffective disorder | Unemployed |
| Waghorn 2014, Australia [57] | 208 (102/106) | 69.2 | 18–59 | Total: NR C: 32.8 (8.9) I: 32.0 (8.9) | 80.8% psychotic disorder, 8.2% bipolar affective disorder, 6.3% major depression or anxiety disorder | Not employed within the previous three months |
| Yamaguchi 2017, Japan [58] | 111 (54/57) | 62.0 | 20–45 | Total: 35 (SD NR) C: 34.5 (6.8) I: 34.8 (7.1) | 87.0% schizophrenia, 7.6% major depression or 5.4% bipolar disorder | Unemployed |
| Studies with People with Autism | ||||||
| Study, Country | N Total (Control/Intervention) | Male Participants (%) | Age Range | Mean Age (SD) Total, Control, Intervention | Type of Disability (%) | Employment Status at Baseline |
| Wehman 2014, USA [45] | 44 (20/24) 4 assigned to control group dropped out prior to study, so C = 16. | 72.5 | 18–21 | Total: NR C: 19.1 (1.1) I: 20.0 (1.1) | Autism (ASD diagnosis and/or educational eligibility of Autism) | Unemployed |
| Wehman 2020, USA [65] | 156 (75/81) | 76.0 | 18–21 | Total: NR C: 19.5 (1.2) I: 19.8 (1.1) | Autism | Unemployed |
| Whittenburg 2020, USA [66] | 14 (8/6) | 78.6 | 18–21 | Total: NR C: NR I: NR | Autism. Participants with comorbid intellectual disability and/or mental health disorders were included | Unemployed |
| Studies with People with Psychosocial Disabilities | ||||||||
|---|---|---|---|---|---|---|---|---|
| Study | Interventions | Intervention Categories | Duration of Intervention, Months | Follow-Up, Months after Randomisation (Unless Otherwise Stated) | Definition of Primary Outcome and Measurement (Timepoint/Period in Months) | Primary Outcomes | Secondary Outcomes | Results |
| Bejerholm 2015, Sweden [46] | IPS vs. Traditional vocational rehabilitation | SE vs. Skills development | 18 | 18 | Open employment defined as worked for at least 1 week in employment that paid at least minimum wage, available to any citizen and located in mainstream settings (0–18) | More IPS participants worked than participants in the TVR group (19/41, 46.3% versus 5/46, 10.9%, respectively; Difference (95% CI): 36 (18–54); p < 0.001) | Favors IPS | |
| Bond 2015, USA [27] | IPS vs. Work Choice | SE vs. Career guidance | No fixed duration | 12 | Open employment (Worked at least one day in the community for which an individual is paid at least minimum wage during 0–12) Supported employment, agency-run job (worked at least one day, an agency-run, for profit business that sells products or goods to the public and provides supported employment to disabled individuals during 0–12) or sheltered work (at least one day, transitional and/or long-term employment in a controlled and protected working environment for those who are unable either to compete or to function in the open job market due to their disabilities during 0–12 months postintervention) | More participants in the IPS condition worked in open employment than those in the control condition (13/42, 31.0% versus 3/43, 7.0%; N = 85, χ2 = 7.99, df = 1, p < 0.01) More participants in the control than IPS condition were in sheltered employment (1/43, 2.3% versus 0/42, 0% respectively) | Favors IPS for open employment, no effect for sheltered employment | |
| Craig 2014, UK [63] | IPS and motivational interviewing vs. IPS only | SE and career guidance vs. SE | 12 | 12 | Open employment (12, 0–12 months) | More participants in the IPS and motivational interviewing condition were in open employment from baseline to 12 months than participants in the IPS only condition (29/68, 43% vs. 12/66, 18% respectively; OR = 3.5, 95% CI 1.5–8.1). and on the day of interview at 12 months (26/68, 38.2% vs. 10/66, 15.2%, respectively; χ2 = 8.79, df = 1, p = 0.003) | Favor IPS and MI over IPS only | |
| Davis 2012, USA [28] | IPS (fair fidelity) vs. Veteran Affairs Vocational Rehabilitation Program | SE vs. Career guidance and work experience | 12 | 12 | Open employment (job for regular wages in a setting that was not set aside, sheltered, or enclaved. Day labor (that is, pick-up cash-based day jobs for yard work, babysitting, manual labor, and so forth) and military drill were not counted as competitive employment, at least one day (any number of hours) of actual work during (0–12 months) | More participants assigned to IPS obtained open employment compared to the TVR participants (76.2% vs. 27.9%, number needed to treat = 2.07, 95% CI = 1.96–2.19; χ2 = 19.84, df = 1, p < 0.001) | IPS participants worked higher mean number of weeks in a competitive job compared to control group (21.6 (17.7) vs. 6.8 (13.8), p < 0.001 (Mann-Whitney z), Cohen’s d = 0.93, 95% CI = 0.50–1.36) | Favors IPS |
| Davis 2018, USA [29] | Standard Coaches vs. Vocational Coaches | Skills development vs. Skill development | 6–16 (depending on client needs) | 1 month post-intervention, 4 months post-intervention | Paid employment in the 30-day period from the end of intervention to 1-month post-intervention | There was no difference in paid employment between participants with vocational coaches compared with standard coaches (6/14, 42.9% versus 4/14, 28.6%, p = 0.430) | No effect | |
| Erickson 2020, Canada [64] | IPS vs. No constraints on the use of other employment support services | SE vs. Passive control condition | 12 | 6, 12 | Open employment, at least 1 day of work (0–6, 6–12) | No effect from baseline to 6 months follow-up between the IPS and control conditions (30/50, 60% vs. 30/52, 57.7%, respectively; no effect from 6 months to end of intervention at 12 months follow-up (34/48, 72.3% versus 25/51, 50.0%) (please note that the n and % don’t add up, and authors did not clarify) | No effect | |
| Hoffmann 2012, 2014, Switzerland [44,47] | Job Coach vs. Traditional train-place vocational rehabilitation programs | SE vs. Work experience and skills development | 60 | 24, 60 | In open employment for at least 2 weeks over the 5-year study (60, 0–60) Supported employment (24) | Participants in the Job Coach condition were more likely to work in open employment than TVR participants over the 5-year study period (30/46, 65.2% vs. 18/54, 33.3%) (p = 0.002); and on the day of interview at 5 years follow-up (20/46, 43.5% vs. 9/54, 16.7%; p = 0.002). Participants in the control condition were more likely to be in sheltered employment than those in the supported employment condition (control 19/54, 35% vs. SE 12/46, 26%; Sign. < 0.001) | Intervention participants were more often employed at least 50% (130 weeks) in a competitive job (SE 20/46, 43.5% vs. control 6/54, 11.1%, respectively; p < 0.001). There were no significant differences in vocational program or mental health service costs between the groups. However, participants in the Job Coach condition had significantly higher income than controls | Favors Job Coach for open employment, but not sheltered employment |
| Howard 2010, UK [67] Heslin 2011, UK [43] | IPS vs. Local traditional vocational services | Supported employment (SE) vs. skills development and career guidance | 24 | 24 | Open employment defined as a job paying at least the minimum wage, located in a mainstream socially integrated setting not set aside for persons with disabilities, held independently (i.e., was not agency owned) and the participant was in continuous employment for at least 30 days (with parttime employment rated pro-rata) (0–12, 0–24) | More participants in the IPS condition were in open employment from baseline to 24 months, compared to participants in the TVR condition (IPS 22.1% vs. TVR 11.6%, risk ratio 1.91; 95% CI 0.98 to 3.74; p = 0.053; adjusted analysis p = 0.041) | There were no differences in self-esteem as measured with the Rosenberg Self Esteem questionnaire at 12 months (p = 0.90) or 24 months p = 0.47) There was no difference in job satisfaction at the 12 month follow-up using the Indiana Job Satisfaction Scale between employed participants in the two groups (p = 0.29) Cost-effectiveness showed no substantial differences. | Favors IPS |
| Killackey 2019, UK [62] | IPS (Good fidelity) vs. Referral to external government-contracted employment agencies | IPS vs. TVR | 6 | 6 | Open employment defined as working in a job in the open labor marker that paid the legislated minimum wage for a minimum of 1 day in the previous 6-month period (0–6). | IPS participants were more likely to work compared to control participants (47/66, 71.2% versus 29/60, 48.0% respectively; OR = 3.40, 95% CI 1.17–9.91, z = 2.25, p = 0.025) | Favors IPS | |
| Lecomte 2020, Canada [48] | Cognitive behaviour therapy group intervention adapted for supported employment programs (CBT-SE) plus supported employment program vs. supported employment program only. | SE and skills development vs. SE | 1 month | 12 | Open employment (0–12). A minimum of one week. | Participants in the CBT-SE intervention were more likely to work than those in the SE only condition (57/76, 75.0% versus 37/64, 57.8% respectively; p < 0.05; OR 2.2, 95% CI: 1.0, 4.8). please note, this was not an intention-to-treat analysis, but rather -as treated. | Favors CBT-SE | |
| McGurk 2015, USA [49] | Enhanced supported employment plus the Thinking Skills for Work Program vs. Enhanced supported employment only. | 6 | 24 | Open employment (0–24 months) Any paid employment (0–24). | More intervention participants than control participants were in open employment from 0 to 24 months from baseline (34 out of 57, 60% vs. 18 out of 50, 36%) p = 0.02; More IPS participants than control participants were in paid employment from 0 to 24 months from baseline (37 out of 57, 65% vs. 22 out of 50, 44%) from 0 to 24 months from baseline (p = 0.03) | Favors Thinking Skills for Work Program | ||
| Michon 2014, Netherlands [50] | IPS (moderate to good) vs. Traditional vocational rehabilitation | Skills development and work experience | No limit (although a limit of 36 months is often prescribed by financing systems in the Netherlands) | 30 (last follow-up timepoint) | Open employment (worked in a competitive job for one day or more) (competitive employment was defined as having a paid job in a company or organization in the regular labor market, against prevailing wages, not set aside for persons with a disability, that is, in an integrated work setting). (0–30 months) | More IPS participants worked compared to TVR participants, (31/71, 43.7% versus 20/79, 25.3%, p < 0.05.) | The Rosenberg Self Esteem questionnaire showed no significant difference between IPS and traditional vocational rehabilitation at 30-month follow-up | Favors IPS |
| Nuechterlein 2020, USA [60] | IPS plus Workplace Fundamentals Module vs. Conventional Brokered Vocational Rehabilitation plus social skills training intervention | 18 | 6, 18 | Open employment defined as paid work in a job that was open to applications from the general public (competitive employment), no minimum number of days of employment, but typically participants were employed at least several weeks.” (1–6, 7–18 months) | There was no difference in open employment between participants in the intervention condition compared to control condition in the initial 6-month period (7/22, 32% versus 12/41, 29%, respectively), From 7 months to end of intervention at 18 months more intervention participants worked compared to controls (69% vs. 33%, respectively, (Adjusted analysis, p = 0.02) | No effect for initial 6 months, Favors IPS + WFM –for the following 1-year period | ||
| Oshima 2014, Japan [51] | Good IPS vs. Conventional vocational rehabilitation | Skills development and work experience | NR | 6 | Open employment defined as a job paying at least minimum wage (as established in Japanese law), with five and more work hours per week, for which anyone can apply, and not controlled by a service agency. (0–6) Supported employment (0–6) | Participants in the IPS condition were more likely to obtain open employment than those in the control group (44.4% versus 10.5% respectively; p = 0.022) There was no difference in supported employment rates between IPS participants and TVR participants (2/18, 11.1% versus 0/19, 0%, respectively; p = 0.128) | Favors IPS for open employment, no effect for supported employment | |
| Poremski 2017, Canada [52] | IPS vs. free to seek employment by any means of their choice | Entire intervention: 27 Good fidelity: 8 | 27 | Open employment (20–27, during the 8 months of good fidelity IPS) | More participants in the IPS condition obtained employment than those in control condition (34% vs. 22%, respectively; p = 0.16; adjusted analysis showed that participants in the IPS group had a 2.4 (p = 0.02) greater chance of obtaining employment | Favors IPS | ||
| Russinova 2018, USA [53] | Vocational Empowerment Photovoice (high fidelity) vs. Wait-list control | Approx. 4.5 months | 4.5 (postintervention), 7.5 (3 months post-intervention) | Open employment: having at least one day on the job (point prevalence of competitive employment at postintervention and 3 months postintervention) | There was no difference in open employment between participants in intervention condition and waitlist controls at postintervention (14% vs. 4% respectively; Cohen’s d = 0.75) | Participants in the intervention condition had a s greater increase in overall empowerment compared to waitlist controls, including self-efficacy (overall empowerment: Group effects: F = 6.65, p = 0.01e, Effect size (Cohen’s d) = 0.39) (self-efficacy subscale: Group effects: F = 6.08, p = 0.02, Cohen’s d= 0.30) | No effect | |
| Schneider 2016, UK [54] | IPS plus work-focused counselling intervention vs. IPS only. | 12 | 12 | Open employment (0–12) | There was no difference in employment between groups (intervention 41% vs. control 29%; χ2 = 0.73, p = 0.39) | No difference in the Rosenberg Self Esteem questionnaire at 12-month follow-up. There was no strong evidence for cost-effectiveness | No effect | |
| Smith 2015a, USA [55] | Virtual reality job interview training (VR-JIT) vs. TAU waitlist control | Skills development | 5–10 business days | 6 months postintervention | Open employment (accepted job offers during 0–6 months postintervention) | More participants in the virtual reality group accepted job offers compared to control participants. (38.5% vs. 25.0%, no statistical analysis) | None | Potentially favors VR-JIT (no statistical analysis) |
| Smith 2015b, USA [59] | Virtual reality job interview training vs. Waitlist control | 2 weeks | 6 months postintervention | Open employment (accepted job offers during 0–6 months postintervention) | More participants in the virtual reality job interview training group accepted job offers compared with control participants. (39.1% vs. 14.3%, no statistical analysis) | None | Potentially favors VR-JIT (no statistical analysis) | |
| Tsang 2010, Hong Kong, [56] | Integrated Supported Employment (ISE): IPS and work-related social skills training vs. IPS vs. Traditional vocational rehabilitation (TVR) (good fidelity) | SE and skills development vs. SE vs. career guidance and skills development/work experience | TVR: 15 ISE, IPS: 39 | 15, 39 | Open employment (competitive employment, continuously worked in the job for > = 2 months for at least 20 h per week) (0–15, 0–39) | There were significant differences between the three groups at 15 month follow up (end of TVR) (TVR 4/66 6.1% vs. IPS 29/65 44.6% vs. Integrated Supported Employment 43/58 74.1%, p < 0.001, More participants in the ISE condition worked compared to the IPS condition at 39 months (ISE 48/58 82.8% vs. IPS 40/65 61.5%, p = 0.009) | Favors ISE over IPS at both timepoints and IPS and ISE over TVR at the first timepoint | |
| Twamley 2012, USA [61] | IPS (Fair to good fidelity) vs. Conventional vocational rehabilitation | SE vs. career guidance and skills development | 12 | 12 | Open employment defined as employment paying at least minimum wage and not reserved for the disabled. “We only considered someone employed if they worked for any part of a day.” (0–12 months); Any paid employment (0–12) | More IPS participants were in open employment than those in TVR during the 12-month study (56.7% versus 28.6% respectively; p = 0.031)More IPS participants obtained paid employment than TVR participants (70.0% versus 35.7%, respectively; p = 0.009) | Favors IPS | |
| Waghorn 2014, Australia [57] | IPS vs. Non-integrated forms of supported employment | 12 | 12 | Open employment (0–12) | More participants in the IPS condition obtained open employment than control participants (42.5% versus 23.5% respectively; OR (95% CI) = 2.40 (1.32, 4.36), p < 0.01). | Favors IPS | ||
| Yamaguchi 2017, Japan [58] | Cognitive remediation and supported employment vs. traditional vocational services | Skills development + SE vs. TVR | NR, waiting for author’s response | 12 | Open employment: number of people who worked at least 1 day in competitive work at 12 months follow-up | More participants in the cognitive remediation and supported employment condition were in work compared to those in the traditional vocational services condition (62.2% versus 19.1% respectively), p < 0.001; adj OR = 11.06 (95% CI 3.53–34.62) | There was no difference in mean total costs between the groups, however, the mean cost for medical services in the intervention group was lower. Further, the intervention showed high probability for cost-effectiveness in terms of vocational outcomes. | Favors CR + SE |
| Studies with People with Autism | ||||||||
| Study | Interventions | Intervention Categories | Duration of Intervention, Months | Follow-Up, Months after Randomisation | Definition of Outcome and Measurement (Timepoint/Period in Months) | Primary Outcomes | Secondary Outcomes | Results |
| Wehman 2014, 2017, USA [45,68] | Project SEARCH plus ASD Supports vs. High school special education services as usual | Collaborative, employer-based employment training and placement program | 9 | 9 (post-intervention) | Open employment (9) | Intervention participants were more likely to be in competitive employment than control participants at graduation (74.2%, 23/31 versus 5.6%, 1/18, respectively; p < 0.0001) | Favors SE + ASD | |
| Wehman 2020, USA [65] | Project SEARCH plus ASD Supports vs. High school special education services as usual | Collaborative, employer-based employment training and placement program | 9 | 9 | Open employment (9) | Intervention participants were more likely to be in employment than control participants, (31.6% vs. 4.8% p < 0.001; adj RR 5.84, 95% CI 1.50, 13.3, p = 0.014) | Favors SE + ASD | |
| Whittenburg 2020, USA [66] | Project SEARCH plus ASD Supports vs. High school special education services as usual | Collaborative, employer-based employment training and placement program | NR | 12 | Accepted job offers for open employment (0–12) Sheltered work (12) | More intervention participants accepted job offers compared to control group participants (83.3% vs. 12.5%, no statistical analyses, very small group). At the 12-month follow-up, one of the control participants and none of the PS + ASD participants was in sheltered work | Probably favors SE + ASD for open employment (no statistical analysis performed), no effect for sheltered employment. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weld-Blundell, I.; Shields, M.; Devine, A.; Dickinson, H.; Kavanagh, A.; Marck, C. Vocational Interventions to Improve Employment Participation of People with Psychosocial Disability, Autism and/or Intellectual Disability: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212083
Weld-Blundell I, Shields M, Devine A, Dickinson H, Kavanagh A, Marck C. Vocational Interventions to Improve Employment Participation of People with Psychosocial Disability, Autism and/or Intellectual Disability: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(22):12083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212083
Chicago/Turabian StyleWeld-Blundell, Isabelle, Marissa Shields, Alexandra Devine, Helen Dickinson, Anne Kavanagh, and Claudia Marck. 2021. "Vocational Interventions to Improve Employment Participation of People with Psychosocial Disability, Autism and/or Intellectual Disability: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 22: 12083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212083