
The Nutritional Content of Rescued Food Conveyed by a Food Aid Organization


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Commission. Eurostat Income Poverty Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Income_poverty_statistics (accessed on 31 July 2020).
- European Commission. Food Waste. Available online: https://ec.europa.eu/food/safety/food_waste_en (accessed on 28 October 2020).
- Vittuari, M.; Azzurro, P.; Gaiani, S.; Gheoldus, M.; Burgos, S.; Aramyan, L.; Valeeva, N.; Rogers, D.; Östergren, K.; Timmermans, T. Recommendations and Guidelines for a Common European Food Waste Policy Framework; FUSIONS: Bologna, Italy, 2016; ISBN 978-94-6257-959-0. Available online: https://www.eu-fusions.org/phocadownload/Publications/D3.5%20recommendations%20and%20guidelines%20food%20waste%20policy%20FINAL.pdf (accessed on 22 October 2020).
- United Nations. Identifying Social Inclusion and Exclusion. Available online: https://www.un.org/esa/socdev/rwss/2016/chapter1.pdf (accessed on 22 October 2020).
- Leung, C.W.; Epel, E.S.; Ritchie, L.D.; Crawford, P.B.; Laraia, B.A. Food Insecurity Is Inversely Associated with Diet Quality of Lower-Income Adults. J. Acad. Nutr. Diet. 2014, 114, 1943–1953.e2. [Google Scholar] [CrossRef] [PubMed]
- FAO. Declaration of the World Summit on Food Security World Summit on Food Security; FAO: Rome, Italy, 2009. [Google Scholar]
- FAO. Policy Brief Changing Policy Concepts of Food Security; FAO: Rome, Italy, 2006; Available online: https://www.fao.org/fileadmin/templates/faoitaly/documents/pdf/pdf_Food_Security_Cocept_Note.pdf (accessed on 22 October 2020).
- Smith, M.D.; Rabbitt, M.P.; Coleman- Jensen, A. Who Are the World’s Food Insecure? New Evidence from the Food and Agriculture Organization’s Food Insecurity Experience Scale. World Dev. 2017, 93, 402–412. [Google Scholar] [CrossRef] [Green Version]
- Tarasuk, V.; Mitchell, A. Household Food Insecurity in Canada; Research to Identify Policy Options to Reduce Food Insecurity (PROOF): Toronto, ON, Canada, 2020; Available online: https://proof.utoronto.ca/ (accessed on 22 October 2020).
- Grimaccia, E.; Naccarato, A. Food Insecurity in Europe: A Gender Perspective. Soc. Indic. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia Estatística—IBGE; Ministério do Desenvolvimento Social e Combate à Fome; Ministério do Planejamento Orçamento e Gestão. Pesquisa Nacional por Amostra de Domicílios (PNAD): Segurança Alimentar; Instituto Brasileiro de Estatística: Rio de Janeiro, Brazil, 2004. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv91984.pdf (accessed on 22 October 2020).
- Gregório, M.J.; Graça, P.; Santos, A.C.; Gomes, S.; Portugal, A.C.; Nogueira, P.J. Relatório InfoFamília 2011–2014—Quatro Anos de Monitorização da Segurança Alimentar e Outras Questões de Saúde Relacionadas com Condições Socioeconómicas, em Agregados Familiares Portugueses Utentes dos Cuidados de Saúde Primários do Serviço Nacional de Saúde 2011–2014; Direção-Geral da Saúde: Lisboa, Portugal, 2017. [Google Scholar]
- Principato, L. Food Waste at Consumer Level: A Comprehensive Literature Review; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Arriola, N.B. Food Insecurity and Hunger Experiences and Their Impact on Food Pantry Clients in the Tampa Bay. Master’s Dissertation, University of South Florida, Tampa, FL, USA, 2015. Available online: https://scholarcommons.usf.edu/etd/5446 (accessed on 22 October 2020).
- Fan, S.; Brzeska, J. Sustainable Food Security and Nutrition: Demystifying Conventional Beliefs. Glob. Food Sec. 2016, 11, 11–16. [Google Scholar] [CrossRef]
- Brennan, A.; Browne, S. Food Waste and Nutrition Quality in the Context of Public Health: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 5379. [Google Scholar] [CrossRef]
- Pettes, T.; Dachner, N.; Gaetz, S.; Tarasuk, V. An Examination of Charitable Meal Programs in Five Canadian Cities. J. Health Care Poor Underserved 2016, 27, 1303–1315. [Google Scholar] [CrossRef]
- Lindberg, R.; Lawrence, M.; Gold, L.; Friel, S. Food Rescue—An Australian Example. Br. Food J. 2014, 116, 1478–1489. [Google Scholar] [CrossRef]
- Garrone, P.; Melacini, M.; Perego, A. Surplus Food Recovery and Donation in Italy: The Upstream Process. Br. Food J. 2014, 116, 1460–1477. [Google Scholar] [CrossRef]
- Reynolds, C.J.; Piantadosi, J.; Boland, J. Rescuing Food from the Organics Waste Stream to Feed the Food Insecure: An Economic and Environmental Assessment of Australian Food Rescue Operations Using Environmentally Extended Waste Input-Output Analysis. Sustainability 2015, 7, 4707–4726. [Google Scholar] [CrossRef] [Green Version]
- Nair, D.J.; Rashidi, T.H.; Dixit, V.V. Estimating Surplus Food Supply for Food Rescue and Delivery Operations. Socioecon. Plann. Sci. 2017, 57, 73–83. [Google Scholar] [CrossRef]
- Burston, T.; Breton, M. The Eating Patterns and Problems of Homeless Women. Women Health 1990, 16, 43–62. [Google Scholar] [CrossRef]
- Irwin, J.D.; Ng, V.K.; Rush, T.J.; Nguyen, C.; He, M. Can Food Banks Sustain Nutrient Requirements? Can. J. Public Health 2007, 98, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Tse, C.; Tarasuk, V. Nutritional Assessment of Charitable Meal Programmes Serving Homeless People in Toronto. Public Health Nutr. 2008, 11, 1296–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, A.; Dachner, N.; Tarasuk, V. Food Intake Patterns of Homeless Youth in Toronto. Can. J. Public Health 2009, 100, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Tarasuk, V.; Dachner, N. The Proliferation of Charitable Meal Programs in Toronto. Can. Public Policy 2009, 35, 433–450. [Google Scholar] [CrossRef]
- Darmon, N.; Coupel, J.; Deheeger, M.; Briend, A. Dietary Inadequacies Observed in Homeless Men Visiting an Emergency Night Shelter in Paris. Public Health Nutr. 2001, 4, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Langnäse, K.; Müller, M.J. Nutrition and Health in an Adult Urban Homeless Population in Germany. Public Health Nutr. 2001, 4, 805–811. [Google Scholar] [CrossRef] [Green Version]
- Maioli, C.; Colosio, C.; Muzio, F.; Cioni, F. Aspetti Nutrizionali Dei Pasti Di Una Mensa per i Poveri: L’ Esperienza Dell’ Opera Di San Francesco Di Milano, Italy. Progr. Nutr. 2016, 18, 396–402. [Google Scholar]
- Neter, J.E.; Dijkstra, S.C.; Visser, M.; Brouwer, I.A.; Dekkers, A.L.M.; Ocké, M.C. Dutch Food Bank Recipients Have Poorer Dietary Intakes than the General and Low-Socioeconomic Status Dutch Adult Population. Eur. J. Nutr. 2018, 57, 2747–2758. [Google Scholar] [CrossRef] [Green Version]
- Sprake, E.F.; Russell, J.M.; Barker, M.E. Food Choice and Nutrient Intake amongst Homeless People. J. Hum. Nutr. Diet. 2014, 27, 242–250. [Google Scholar] [CrossRef]
- Pelham-Burn, S.E.; Frost, C.J.; Russell, J.M.; Barker, M.E. Improving the Nutritional Quality of Charitable Meals for Homeless and Vulnerable Adults. A Case Study of Food Provision by a Food Aid Organisation in the UK. Appetite 2014, 82, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Fallaize, R.; Newlove, J.; White, A.; Lovegrove, J.A. Nutritional Adequacy and Content of Food Bank Parcels in Oxfordshire, UK: A Comparative Analysis of Independent and Organisational Provision. J. Hum. Nutr. Diet. 2020, 33, 477–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, A.; Krummel, D.A.; Lee, S.Y. Availability of Food Options and Nutrition Education in Local Food Pantries. J. Nutr. Educ. Behav. 2020, 52, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Buttorff, C.; Trujillo, A.J.; Diez-Canseco, F.; Bernabe-Ortiz, A.; Miranda, J.J. Evaluating Consumer Preferences for Healthy Eating from Community Kitchens in Low-Income Urban Areas: A Discrete Choice Experiment of Comedores Populares in Peru. Soc. Sci. Med. 2015, 140, 1–8. [Google Scholar] [CrossRef]
- Hoisington, A.; Manore, M.M.; Raab, C. Nutritional Quality of Emergency Foods. J. Am. Diet. Assoc. 2011, 111, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.W.; Ding, E.L.; Catalano, P.J.; Villamor, E.; Rimm, E.B.; Willett, W.C. Dietary Intake and Dietary Quality of Low-Income Adults in the Supplemental Nutrition Assistance Program. Am. J. Clin. Nutr. 2012, 96, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.W.; Musicus, A.A.; Willett, W.C.; Rimm, E.B. Improving the Nutritional Impact of the Supplemental Nutrition Assistance Program: Perspectives From the Participants. Am. J. Prev. Med. 2017, 52, S193–S198. [Google Scholar] [CrossRef] [Green Version]
- Lyles, C.R.; Drago-Ferguson, S.; Lopez, A.; Seligman, H.K. Nutritional Assessment of Free Meal Programs in San Francisco. Prev. Chronic Dis. 2013, 10, E90. [Google Scholar] [CrossRef] [Green Version]
- Mousa, T.Y.; Freeland-Graves, J.H. Organizations of Food Redistribution and Rescue. Public Health 2017, 152, 117–122. [Google Scholar] [CrossRef]
- Mousa, T.Y.; Freeland-Graves, J.H. Impact of Food Pantry Donations on Diet of a Low-Income Population. Int. J. Food Sci. Nutr. 2019, 70, 78–87. [Google Scholar] [CrossRef]
- Simmet, A.; Depa, J.; Tinnemann, P.; Stroebele-Benschop, N. The Nutritional Quality of Food Provided from Food Pantries: A Systematic Review of Existing Literature. J. Acad. Nutr. Diet. 2017, 117, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Greger, J.L.; Maly, A.; Jensen, N.; Kuhn, J.; Monsun, K.; Stocks, A. Food Pantries Can Provide Nutritionally Adequate Food Packets but Need Help to Become Effective Referral Units for Public Assistance Programs. J. Am. Diet. Assoc. 2002, 102, 1126–1128. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Y.; Yen, S.T. Does Supplemental Nutrition Assistance Program Reduce Food Insecurity among Households with Children? Evidence from the Current Population Survey. Int. J. Environ. Res. Public Health 2021, 18, 3178. [Google Scholar] [CrossRef] [PubMed]
- Hegde, S.; Lodge, J.S.; Trabold, T.A. Characteristics of Food Processing Wastes and Their Use in Sustainable Alcohol Production. Renew. Sustain. Energy Rev. 2018, 81, 510–523. [Google Scholar] [CrossRef]
- Dombroski, K.; Diprose, G.; Sharp, E.; Graham, R.; Lee, L.; Scobie, M.; Richardson, S.; Watkins, A.; Martin-Neuninger, R. Food for People in Place: Reimagining Resilient Food Systems for Economic Recovery. Sustainability 2020, 12, 9369. [Google Scholar] [CrossRef]
- Healy, S.; Chitranshi, B.; Diprose, G.; Eskelinen, T.; Madden, A.; Santala, I.; Williams, M. Planetary Food Commons and Postcapitalist Post-COVID Food Futures. Development 2020, 63, 277–284. [Google Scholar] [CrossRef]
- Jablonski, B.B.R.; Casnovsky, J.; Clark, J.K.; Cleary, R.; Feingold, B.; Freedman, D.; Gray, S.; Romeiko, X.; Olabisi, L.S.; Torres, M.; et al. Emergency Food Provision for Children and Families during the COVID-19 Pandemic: Examples from Five U.S. Cities. Appl. Econ. Perspect. Policy 2020, 43, 169–184. [Google Scholar] [CrossRef]
- Fleetwood, J. Social Justice, Food Loss, and the Sustainable Development Goals in the Era of COVID-19. Sustainability 2020, 12, 5027. [Google Scholar] [CrossRef]
- UN. The Sustainable Development Goals Report 2020; United Nations: New York, NY, USA, 2020; Available online: https://unstats.un.org/sdgs/report/2020/The-Sustainable-Development-Goals-Report-2020.pdf (accessed on 22 October 2020).
- European Commission. The 2030 Agenda for Sustainable Development. Available online: https://ec.europa.eu/info/strategy/international-strategies/sustainable-development-goals/eu-and-united-nations-common-goals-sustainable-future_en (accessed on 4 September 2021).
- Refood. O movimento Refood. Available online: http://www.re-food.org/pt (accessed on 1 August 2020).
- ESHA Reasearch. ESHA’s History ESHA’s History. Available online: https://esha.com/blog/history-of-the-nutrition-facts-label-celebrating-30-years-of-genesis-rd/ (accessed on 14 April 2021).
- Stage, L.; Vitamin, A.; Vitamin, K. Dietary Reference Intakes ( DRIs ): Recommended Dietary Allowances and Adequate Intakes, Vitamins Food and Nutrition Board, Institute of Medicine. Natl. Acad. 2011, 3, 165–182. [Google Scholar] [CrossRef]
- WHO. Population Nutrient Intake Goals for Preventing Diet-Related Chronic Diseases. In Diet, Nutrition and the Prevention of Chronic Diseases; WHO Technical Report Series, No. 797; World Health Organization: Geneva, Switzerland, 2003; Chapter 5; pp. 54–60. [Google Scholar]
- Van Horn, L. Fiber, Lipids, and Coronary Heart Disease. Circulation 1997, 95, 2701–2704. [Google Scholar] [CrossRef]
- Nogueira, A.; Alves, F.; Vaz-Fernandes, P. The Contribution of Up-Cycled Food Waste to a Balanced Diet of Low-Income Households. Sustainability 2021, 13, 4779. [Google Scholar] [CrossRef]
- USDA. Measurement. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/measurement.aspx#measurement (accessed on 7 April 2021).
- Bickel, G.; Nord, M.; Price, C.; Hamilton, W.; Cook, J. Guide to Measuring Household Food Security; Food and Nutrition Service, USDA: Alexandria, VA, USA, 2000. Available online: https://naldc.nal.usda.gov/download/38369/PDF (accessed on 22 October 2020).
- Radimer, K.L.; Radimer, K.L. Measurement of Household Food Security in the USA and Other Industrialised Countries. Public Health Nutr. 2002, 5, 859–864. [Google Scholar] [CrossRef] [PubMed]
- Neter, J.E.; Dijkstra, S.C.; Visser, M.; Brouwer, I.A. Food Insecurity among Dutch Food Bank Recipients: A Cross-Sectional Study. BMJ Open 2014, 4, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Cafiero, C.; Viviani, S.; Nord, M. Food Security Measurement in a Global Context: The Food Insecurity Experience Scale. Meas. J. Int. Meas. Confed. 2018, 116, 146–152. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. BMI Calculator for Children and Teen. Available online: https://www.cdc.gov/healthyweight/bmi/calculator.html (accessed on 14 April 2021).
- Rodrigues, S.S.P.; Franchini, B.; Graça, P.; de Almeida, M.D.V. A New Food Guide for the Portuguese Population: Development and Technical Considerations. J. Nutr. Educ. Behav. 2006, 38, 189–195. [Google Scholar] [CrossRef] [PubMed]
- WHO. Adolescent health in the South-East Asia Region. Available online: https://www.who.int/southeastasia/health-topics/adolescent-health (accessed on 21 February 2021).
- Koletzko, B. Basic Concepts in Nutrition: Nutritional Needs of Children and Adolescents. e-SPEN 2008, 3, e179–e184. [Google Scholar] [CrossRef] [Green Version]
- Mayo Clinic. Nutrition for Kids: Guidelines for a Healthy Diet. Available online: https://www.mayoclinic.org/healthy-lifestyle/childrens-health/in-depth/nutrition-for-kids/art-20049335 (accessed on 16 December 2019).
- Akobundu, U.O.; Cohen, N.L.; Laus, M.J.; Schulte, M.J.; Soussloff, M.N. Vitamins a and C, Calcium, Fruit, and Dairy Products Are Limited in Food Pantries. J. Am. Diet. Assoc. 2004, 104, 811–813. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; De Benoist, B.; Darnton-Hill, I.; Delange, F. Iodine Deficiency in Europe: A Continuing Public Health Problem; WHO: Geneva, Switzerland, 2007; ISBN 978 92 4 159396 0. Available online: http://ernaehrungsdenkwerkstatt.de/fileadmin/user_upload/EDWText/TextElemente/Ernaehrungswissenschaft/Naehrstoffe/Jodmangel_in_Eruope_2007_WHO.pdf (accessed on 22 October 2020).
- Bogh, M.K.B.; Schmedes, A.V.; Philipsen, P.A.; Thieden, E.; Wulf, H.C. Vitamin D Production after UVB Exposure Depends on Baseline Vitamin D and Total Cholesterol but Not on Skin Pigmentation. J. Invest. Dermatol. 2010, 130, 546–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F.; Chen, T.C.; Lu, Z.; Sauter, E. Vitamin D and Skin Physiology: A D-Lightful Story. J. Bone Miner. Res. 2007, 22 (Suppl. 2), 28–33. [Google Scholar] [CrossRef]


{kind=link}
| Sociodemographic Sample Characteristics | ||
|---|---|---|
| n | % | |
| Families | 27 | |
| Households | ||
| 1 2 3 4 | 9 8 6 4 | 33.4 29.6 22.2 14.8 |
| Households with children | ||
| Yes No | 8 19 | 29.6 70.4 |
| Gender | ||
| Female Male | 34 25 | 57.6 42.4 |
| Occupational status | ||
| Active members Unemployed Students Retired | 16 17 13 13 | 27.2 28.8 22.0 22.0 |
| Highest Level of Education (adults, n = 47) | ||
| 1–4 years 5–6 years 7–9 years 10–12 years >12 years | 12 7 12 15 1 | 25.5 15.0 25.5 31.9 2.1 |
| Nationality | ||
| Portuguese Brazilian | 50 9 | 84.7 15.3 |
| Food insecurity | ||
| Food security Low insecurity Moderate insecurity Severe insecurity | 3 13 3 8 | 11.1 48.2 11.1 29.6 |
| Body mass index | ||
| Underweight Healthy weight Overweight Obese | 1 28 17 13 | 1.7 47.5 28.8 22.0 |
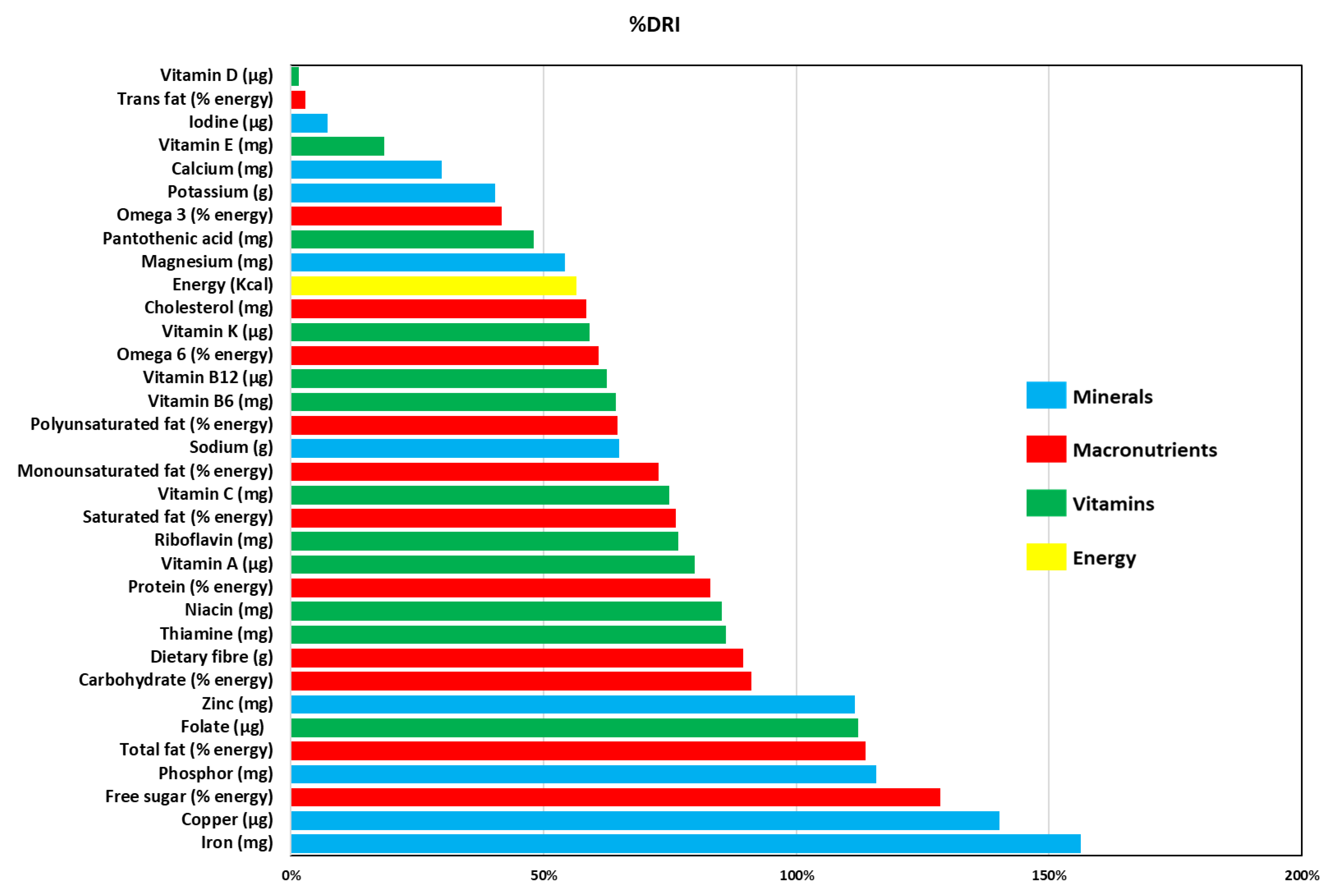
| Mean Value of Nutrients Distributed per Person and per Day | ||
|---|---|---|
| Nutrients | Mean Value | % DRI |
| Energy (Kcal) | 1244.4 | 56.6 |
| Protein (% energy) | 18.68 | 83.0 |
| Carbohydrate (% energy) | 50.08 | 91.1 |
| Free sugar (% energy) | 13.16 | 128.5 |
| Total fat (% energy) | 31.27 | 113.7 |
| Saturated fat (% energy) | 9.16 | 76.2 |
| Monounsaturated fat (% energy) | 12.74 | 72.8 |
| Polyunsaturated fat (% energy) | 5.17 | 64.6 |
| Trans fat (% energy) | 0.04 | 2.9 |
| Cholesterol (mg) | 175.50 | 58.5 |
| Omega 3 (% energy) | 0.38 | 41.7 |
| Omega 6 (% energy) | 4.57 | 60.9 |
| Dietary fiber (g) | 24.6 | 98.4 |
| Vitamin A (µg) | 638.7 | 79.8 |
| Thiamine (mg) | 0.99 | 86.1 |
| Riboflavin (mg) | 0.92 | 76.7 |
| Niacin (mg) | 12.8 | 85.3 |
| Pantothenic acid (mg) | 2.4 | 48.0 |
| Vitamin B6 (mg) | 1.03 | 64.4 |
| Folate (µg) | 448.9 | 112.2 |
| Vitamin B12 (µg) | 1.5 | 62.5 |
| Vitamin C (mg) | 61.7 | 74.8 |
| Vitamin D (µg) | 0.23 | 1.5 |
| Vitamin E (mg) | 2.76 | 18.4 |
| Vitamin K (µg) | 62.0 | 59.0 |
| Calcium (mg) | 328.4 | 29.9 |
| Copper (µg) | 1262.5 | 140.3 |
| Iodine (µg) | 10.9 | 7.3 |
| Iron (mg) | 12.5 | 156.3 |
| Magnesium (mg) | 200.7 | 54.2 |
| Phosphor (mg) | 810.7 | 115.8 |
| Potassium (g) | 1.9 | 40.4 |
| Sodium (g) | 1.3 | 65.0 |
| Zinc (mg) | 10.6 | 111.6 |
| Nutrients | Food Security and Low Insecurity | Moderate and Severe Insecurity | Mann–Whitney U-Test | Median Test |
|---|---|---|---|---|
| Energy (Kcal) | 1540.7 ± 1810.5 | 813.6 ± 344.0 | 0.394 | 1.000 |
| Protein (% energy) | 18.44 ± 2.679 | 18.84 ± 4.755 | 0.394 | 0.440 |
| Carbohydrates (% energy) | 52.43 ± 8.291 | 46.84 ± 7.756 | 0.481 | 0.704 |
| Free sugar (% energy) | 12.97 ± 2.105 | 13.43 ± 2.819 | 0.394 | 0.704 |
| Total fat (% energy) | 29.35 ± 6.689 | 34.03 ± 4.184 | 0.099 | 0.252 |
| Saturated fat (% energy) | 8.564 ± 2.184 | 9.978 ± 1.554 | 0.148 | 0.252 |
| Monounsaturated fat (% energy) | 11.96 ± 3.171 | 13.87 ± 1.811 | 0.195 | 0.704 |
| Polyunsaturated fat (% energy) | 4.807 ± 0.9055 | 5.708 ± 1.075 | 0.030 | 0.252 |
| Trans fat (% energy) | 0.0556 ± 0.1305 | 0.1000 ± 0.0205 | 0.342 | 0.183 |
| Cholesterol (mg) | 187.3 ± 152.5 | 158.4 ± 103.0 | 0.865 | 0.704 |
| Omega 3 (% energy) | 0.3590 ± 0.162 | 0.3987 ± 0.1294 | 0.544 | 0.704 |
| Omega 6 (% energy) | 4.252 ± 0.859 | 5.032 ± 1.015 | 0.023 | 0.252 |
| Dietary fiber (g) | 34.81 ± 78.76 | 9.642 ± 9.998 | 0.089 | 0.120 |
| Vitamin A (µg) | 707.4 ± 537.0 | 538.7 ± 312.7 | 1.000 | 1.000 |
| Thiamine (mg) | 1.26 ± 1.29 | 0.614 ± 0.249 | 0.110 | 0.440 |
| Riboflavin (mg) | 1.087 ± 0.853 | 0.666 ± 0.284 | 0.318 | 0.440 |
| Niacin (mg) | 14.64 ± 9.802 | 10.25 ± 7.318 | 0.342 | 0.440 |
| Pantothenic acid (mg) | 3.082 ± 3.457 | 1.513 ± 0.757 | 0.121 | 0.440 |
| Vitamin B6 (mg) | 1.342 ± 1.742 | 0.565 ± 0.315 | 0.342 | 0.440 |
| Folate (µg) | 656.6 ± 1756.8 | 146.9 ± 57.23 | 0.178 | 0.440 |
| Vitamin B12 (µg) | 1.674 ± 1.331 | 1.321 ± 0.8019 | 0.827 | 1.000 |
| Vitamin C (mg) | 77.54 ± 55.70 | 38.37 ± 13.42 | 0.121 | 0.440 |
| Vitamin D (µg) | 0.2417 ± 0.2356 | 0.2060 ± 0.2813 | 0.368 | 0.440 |
| Vitamin E (mg) | 3.486 ± 4.169 | 1.698 ± 0.9425 | 0.544 | 1.000 |
| Vitamin K (µg) | 73.60 ± 51.83 | 45.08 ± 19.44 | 0.195 | 1.000 |
| Calcium (mg) | 422.8 ± 552.7 | 191.14 ± 73.89 | 0.099 | 0.440 |
| Copper (µg) | 1.819 ± 3.654 | 0.4256 ± 0.1861 | 0.162 | 0.440 |
| Iodine (µg) | 13.27 ± 11.87 | 7.499 ± 3.334 | 0.212 | 0.120 |
| Iron (mg) | 16.52 ± 30.10 | 6.551 ± 2.555 | 0.212 | 1.000 |
| Magnesium (mg) | 280.28 ± 511.77 | 97.31 ± 44.68 | 0.121 | 0.440 |
| Phosphor (mg) | 1061.5 ± 793.3 | 445.9 ± 194.9 | 0.394 | 1.000 |
| Potassium (g) | 2526.9 ± 3433.3 | 1035.5 ± 399.5 | 0.272 | 0.440 |
| Sodium (g) | 1528.8 ± 863.5 | 1063.3 ± 485.5 | 0.272 | 1.000 |
| Zinc (mg) | 13.13 ± 16.31 | 6.855 ± 2.372 | 0.610 | 0.704 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nogueira, A.; Alves, F.; Vaz-Fernandes, P. The Nutritional Content of Rescued Food Conveyed by a Food Aid Organization. Int. J. Environ. Res. Public Health 2021, 18, 12212. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212212
Nogueira A, Alves F, Vaz-Fernandes P. The Nutritional Content of Rescued Food Conveyed by a Food Aid Organization. International Journal of Environmental Research and Public Health. 2021; 18(22):12212. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212212
Chicago/Turabian StyleNogueira, Anne, Fátima Alves, and Paula Vaz-Fernandes. 2021. "The Nutritional Content of Rescued Food Conveyed by a Food Aid Organization" International Journal of Environmental Research and Public Health 18, no. 22: 12212. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212212