
Gender and Observed Complexity in Palliative Home Care: A Prospective Multicentre Study Using the HexCom Model

 , ,
, ,
Abstract
:1. Background
2. Objectives
3. Methods
4. Results
5. Discussion
Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marshall, D.; Myers, J. Complexity Science and Palliative Care: Drawing from Complex Adaptive Systems Theories to Guide Our Successes. J. Palliat. Med. 2018, 21, 1210–1211. [Google Scholar] [CrossRef] [PubMed]
- Kimbell, B.; A Murray, S.; Macpherson, S.; Boyd, K. Embracing inherent uncertainty in advanced illness. BMJ 2016, 354, i3802. [Google Scholar] [CrossRef] [PubMed]
- Carduff, E.; Johnston, S.; Winstanley, C.; Morrish, J.; Murray, S.A.; Spiller, J.; Finucane, A. What does ‘complex’ mean in palliative care? Triangulating qualitative findings from 3 settings. BMC Palliat. Care 2018, 17, 12. [Google Scholar] [CrossRef] [Green Version]
- Grembowski, D.; Schaefer, J.; Johnson, K.E.; Fischer, H.; Moore, S.L.; Tai-Seale, M.; Ricciardi, R.; Fraser, J.R.; Miller, D.; LeRoy, L. A Conceptual Model of the Role of Complexity in the Care of Patients With Multiple Chronic Conditions. Med. Care 2014, 52, S7–S14. [Google Scholar] [CrossRef] [PubMed]
- Halpern, S.D. Toward Evidence-Based End-of-Life Care. N. Engl. J. Med. 2015, 373, 2001–2003. [Google Scholar] [CrossRef]
- Holland, J.H. Studying Complex Adaptive Systems. J. Syst. Sci. Complex. 2006, 19, 1–8. [Google Scholar] [CrossRef]
- Von Bertalanffy, L. Teoría General De Sistemas: Fundamentos, Desarrolo, Aplicaciones; 7 reimpres; Fondo de Cultura Económica: Mexico City, Mexico, 1989. [Google Scholar]
- Pask, S.; Pinto, C.; Bristowe, K.; Van Vliet, L.; Nicholson, C.J.; Evans, C.; George, R.; Bailey, K.; Davies, J.M.; Guo, P.; et al. A framework for complexity in palliative care: A qualitative study with patients, family carers and professionals. Palliat. Med. 2018, 32, 1078–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valls Llobet, C. Mujeres Invisibles Para la Medicina, 2nd ed.; Capitan Swing: Madrid, Spain, 2020; 479p. [Google Scholar]
- Sorge, R.E.; Totsch, S.K. Sex Differences in Pain. J. Neurosci. Res. 2016, 95, 1271–1281. [Google Scholar] [CrossRef]
- Johnson, M.M.; Gilligan, C. In a Different Voice: Psychological Theory and Women’s Development. Contemp. Sociol. A J. Rev. 1983, 12, 448. [Google Scholar] [CrossRef]
- Gott, M.; Morgan, T.; Williams, L. Gender and palliative care: A call to arms. Palliat. Care Soc. Pr. 2020, 14. [Google Scholar] [CrossRef]
- Falk, H.; Henoch, I.; Ozanne, A.; Öhlen, J.; Ung, E.J.; Fridh, I.; Sarenmalm, E.K.; Falk, K. Differences in Symptom Distress Based on Gender and Palliative Care Designation Among Hospitalized Patients. J. Nurs. Sch. 2016, 48, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Eikemo, T.A.; Øversveen, E. Social Inequalities in health: Challenges, knowledge gaps, key debates and the need for new data. Scand. J. Public Health 2018, 47, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, N.; Ward-Griffin, C.; McWilliam, C.; Stajduhar, K. Discourses Reproducing Gender Inequities in Hospice Palliative Home Care. Can. J. Nurs. Res. 2018, 50, 189–201. [Google Scholar] [CrossRef]
- Busquet-Duran, X.; Jiménez-Zafra, E.M.; Manresa-Domínguez, J.-M.; Tura-Poma, M.; Bosch-delaRosa, O.; Moragas-Roca, A.; Galera Padilla, M.C.; Moreno, S.M.; Martínez-Losada, E.; Crespo-Ramírez, S.; et al. Describing Complexity in Palliative Home Care Through HexCom: A Cross-Sectional, Multicenter Study. J Multidiscip Healthc. 2020, 13, 297. Available online: https://www.dovepress.com/describing-complexity-in-palliative-home-care-through-hexcom-a-cross-s-peer-reviewed-article-JMDH (accessed on 1 October 2021). [CrossRef] [PubMed] [Green Version]
- Busquet-Duran, X.; Jiménez-Zafra, E.; Tura-Poma, M.; la Rosa, O.B.-D.; Moragas-Roca, A.; Martin-Moreno, S.; Martínez-Losada, E.; Crespo-Ramírez, S.; Lestón-Lado, L.; Salamero-Tura, N.; et al. Assessing Face Validity of the HexCom Model for Capturing Complexity in Clinical Practice: A Delphi Study. Healthcare 2021, 9, 165. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.; de Graaf, E.; Teunissen, S. A systematic review of classifications systems to determine complexity of patient care needs in palliative care. Palliat. Med. 2021, 35, 636–650. [Google Scholar] [CrossRef] [PubMed]
- Santaeugènia, S.J.; Contel, J.C.; Vela, E.; Cleries, M.; Amil, P.; Melendo-Azuela, E.M.; Gil-Sánchez, E.; Mir, V.; Amblàs-Novellas, J. Characteristics and Service Utilization by Complex Chronic and Advanced Chronic Patients in Catalonia: A Retrospective Seven-Year Cohort-Based Study of an Implemented Chronic Care Program. Int. J. Environ. Res. Public Health 2021, 18, 9473. [Google Scholar] [CrossRef]
- Esteban-Pérez, M.; Fernández-Ballart, J.; Boira-Senlí, R.; Martínez-Serrano, T.; Nadal-Ventura, S.; Castells-Trilla, G. Concordancia entre la complejidad observada desde diferentes niveles asistenciales en pacientes crónicos complejos, con enfermedad avanzada o al final de la vida mediante un modelo de abordaje de la complejidad. Med. Paliat. 2018, 25, 236. Available online: https://www.elsevier.es/es-revista-medicina-paliativa-337-avance-resumen-concordancia-entre-complejidad-observada-desde-S1134248X18300028 (accessed on 1 October 2021). [CrossRef]
- World Palliative Care Alliance. Global Atlas of Palliative Care at the End of Life. 2014. Available online: http://https://www.who.int/nmh/Global_Atlas_of_Palliative_Care.pdf (accessed on 1 October 2021).
- Etkind, S.N.; Bone, A.E.; Gomes, B.; Lovell, N.; Evans, C.J.; Higginson, I.J.; Murtagh, F.E.M. How many people will need palliative care in 2040? Past trends, future projections and implications for services. BMC Med. 2017, 15, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrasco-Zafra, M.I.; Gómez-García, R.; Ocaña-Riola, R.; Martín-Roselló, M.L.; Blanco-Reina, E. Level of Palliative Care Complexity in Advanced Cancer Patients: A Multinomial Logistic Analysis. J. Clin. Med. 2020, 9, 1960. [Google Scholar] [CrossRef]
- Nipp, R.D.; Greer, J.A.; El-Jawahri, A.; Traeger, L.; Gallagher, E.R.; Park, E.R.; Jackson, V.A.; Pirl, W.; Temel, J.S. Age and Gender Moderate the Impact of Early Palliative Care in Metastatic Non-Small Cell Lung Cancer. Oncologist 2015, 21, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Acquati, C.; Kayser, K. Dyadic Coping Across the Lifespan: A Comparison Between Younger and Middle-Aged Couples With Breast Cancer. Front. Psychol. 2019, 10, 404. [Google Scholar] [CrossRef] [PubMed]
- Forma, L.; Aaltonen, M.; Raitanen, J.; Anthun, K.S.; Kalseth, J. Place of death among older people in Finland and Norway. Scand. J. Public Health 2020, 48, 817–824. [Google Scholar] [CrossRef]
- Wilson, D.M.; Birch, S. A scoping review of research to assess the frequency, types, and reasons for end-of-life care setting transitions. Scand. J. Public Health 2018, 48, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Ullrich, A.; Grube, K.; Hlawatsch, C.; Bokemeyer, C.; Oechsle, K. Exploring the gender dimension of problems and needs of patients receiving specialist palliative care in a German palliative care unit—The perspectives of patients and healthcare professionals. BMC Palliat. Care 2019, 18, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifart, C.; Knorrenschild, J.R.; Hofmann, M.; Nestoriuc, Y.; Rief, W.; von Blanckenburg, P. Let us talk about death: Gender effects in cancer patients’ preferences for end-of-life discussions. Support. Care Cancer 2020, 28, 4667–4675. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, K.; Prigerson, H.G.; Paulk, E.; Temel, J.; Finlay, E.; Marr, L.; McCorkle, R.; Rivera, L.; Munoz, F.; Maciejewski, P.K. Gender differences in the evolution of illness understanding among patients with advanced cancer. J. Support. Oncol. 2013, 11, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, F.; Hoerger, M.; Norton, S.A.; Guancial, E.; Epstein, R.M.; Duberstein, P.R. Preference for Palliative Care in Cancer Patients: Are Men and Women Alike? J. Pain Symptom. Manag. 2018, 56, 1–6. Available online: https://0-linkinghub-elsevier-com.brum.beds.ac.uk/retrieve/pii/S088539241830174X (accessed on 1 October 2021). [CrossRef] [PubMed] [Green Version]
- Antolin, A.; Jimenez, S.; Gonzalez, M.; Gomez, E.; Sánchez, M.; Miró, O. Characteristics and use of advance directives in a tertiary hospital. Rev. Clínica Española (Engl. Ed.) 2014, 214, 296–302. [Google Scholar] [CrossRef]
- Tuca, A.; Viladot, M.; Barrera, C.; Chicote, M.; Casablancas, I.; Cruz, C.; Font, E.; Marco-Hernández, J.; Padrosa, J.; Pascual, A.; et al. Prevalence of ethical dilemmas in advanced cancer patients (secondary analysis of the PALCOM study). Support. Care Cancer 2020, 29, 3667–3675. [Google Scholar] [CrossRef] [PubMed]
- Gott, M.; Frey, R.; Wiles, J.; Rolleston, A.; Teh, R.; Moeke-Maxwell, T.; Kerse, N. End of life care preferences among people of advanced age: LiLACS NZ. BMC Palliat. Care 2017, 16, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, S.; Smith, T.F.; Neufeld, E.; Fisher, K.; Ebihara, S. The wish to die among palliative home care clients in Ontario, Canada: A cross-sectional study. BMC Palliat. Care 2016, 15, 24. [Google Scholar]
- Ohnsorge, K.; Rehmann-Sutter, C.; Streeck, N.; Gudat, H. Wishes to die at the end of life and subjective experience of four different typical dying trajectories. A qualitative interview study. PLoS ONE 2019, 14, e0210784. [Google Scholar] [CrossRef]
- Cai, J.; Guerriere, D.N.; Zhao, H.; Coyte, P.C. Socioeconomic Differences in and Predictors of Home-Based Palliative Care Health Service Use in Ontario, Canada. Int. J. Environ. Res. Public Health 2017, 14, 802. [Google Scholar] [CrossRef] [Green Version]
- Bany Hamdan, A.; Al-odeh, F.; Javison, S.; AlSuheil, A.; Alshammary, S.; AlHarbi, M. Religious Belief and Social Support Among Cancer Patients in Saudi Arabia. Cureus. 16 February 2020. Available online: https://www.cureus.com/articles/25899-religious-belief-and-social-support-among-cancer-patients-in-saudi-arabia (accessed on 1 October 2021).
- Hvidt, N.C.; Mikkelsen, T.B.; Zwisler, A.D.; Tofte, J.B.; Hvidt, E.A. Spiritual, religious, and existential concerns of cancer survivors in a secular country with focus on age, gender, and emotional challenges. Support. Care Cancer 2019, 27, 4713–4721. [Google Scholar] [CrossRef] [Green Version]
- Benedicto, C. Malestares de género y socialización: El feminismo como grieta. Rev. La Asoc. Española Neuropsiquiatría 2018, 38, 607–625. [Google Scholar]
- Van Wijmen, M.P.S.; Pasman, H.R.W.; Widdershoven, G.A.M.; Onwuteaka-Philipsen, B.D. Continuing or forgoing treatment at the end of life? Preferences of the general public and people with an advance directive. J. Med. Ethics 2014, 41, 599–606. [Google Scholar] [CrossRef]
- Van Deijck, R.H.; Hasselaar, J.G.; Verhagen, S.C.; Vissers, K.C.; Koopmans, R.T. Determinants of the Administration of Continuous Palliative Sedation: A Systematic Review. J. Palliat. Med. 2013, 16, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Franchini, L.; Ercolani, G.; Ostan, R.; Raccichini, M.; Samolsky-Dekel, A.; Malerba, M.; Melis, A.; Varani, S.; Pannuti, R. Caregivers in home palliative care: Gender, psychological aspects, and patient’s functional status as main predictors for their quality of life. Support. Care Cancer 2019, 28, 3227–3235. [Google Scholar] [CrossRef]
- Hertler, C.; Seiler, A.; Gramatzki, D.; Schettle, M.; Blum, D. Sex-specific and gender-specific aspects in patient-reported outcomes. ESMO Open 2020, 5, e000837. [Google Scholar] [CrossRef]
- Greenwood, B.N.; Carnahan, S.; Huang, L. Patient–physician gender concordance and increased mortality among female heart attack patients. Proc. Natl. Acad. Sci. USA 2018, 115, 8569–8574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yakimchuk, E. Making Sense of Gender Inequities in Hospice Palliative Home Care. Can. J. Nurs. Res. 2019, 51, 131–132. [Google Scholar] [CrossRef]
- Torkelson, D.J.; Seed, M.S. Gender Differences in the Roles and Functions of Inpatient Psychiatric Nurses. J. Psychosoc. Nurs. Ment. Health Serv. 2011, 49, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Elmståhl, S.; Lundholm-Auoja, N.; Ekström, H.; Sandin Wranker, L. Being an older family caregiver does not impact healthcare and mortality: Data from the study ‘Good Aging in Skåne’. Scand. J. Public Health 2020. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| HexCom-Clin2019 Model for the care of people with advanced disease and/or end of life situation. Extended version for the assessment of needs and resources. OBSERVED CARE COMPLEXITY. | ||||||
| NEEDS: Identify the patient’s areas of discomfort and relate it to the possibility of response from the service. Mark the level of complexity of the affected areas: L Low, M Medium, H High. Mark N for areas Not evaluated/Not applicable. COMPLEXITY AND INTERPRETATION LEVELS: L—Low (little difficulty). Guarantees of being able to attend to the situation with the resources of the service. M—Medium (moderate difficulty). Guarantees of taking on the situation with the support of other professionals and/or specialised teams. H—High (refractory difficulty). Little chance of change. It is necessary to escort and/or probably refer to another resource/level of care. | ||||||
| Area | Sub-Area | N | L | M | H | |
| CLINIC | PHYSICAL | Physical discomfort due to symptoms (pain, dyspnoea...) and/or injuries (tumorous ulcer...). | ||||
| THERAPEUTICS | Difficulty in adherence to prescriptions and/or access to drugs/techniques. | |||||
| PSYCHO-EMOTIONAL | PERSONALITY | Psychological vulnerability: rigid personality traits with difficulty adapting to changes (perfectionism, thoroughness, control...), or psychopathology (alcoholism, drug addiction, psychiatric disease, dementia with behavioural disturbance, delirium...). | ||||
| EMOTIONAL | Maladaptive emotional distress (intense, persistent, interfering with relationships and functionality). | |||||
| SPIRITUAL | SENSE | Deep distress with feelings of rupture due to illness, with difficulty finding meaning in the situation, feelings of incoherence with the actions and decisions taken throughout life. | ||||
| CONNECTION | Deep distress with isolation and rupture of relationships, feelings of guilt, does not feel at peace with others or that they are one of them, difficulty forgiving, inability to use insight. | |||||
| TRANSCENDENCE | Deep distress with difficulty facing everything that will come, in the face of the unknown: panic at dying, at disappearing, the future of those left, difficulty seeing what they will leave, feelings of injustice. | |||||
| SOCIAL AND FAMILY | RELATIONAL | Relational distress in the family environment that makes patient care difficult. | ||||
| EMOTIONAL | Emotional maladjustment of the caregiver/s (intense, persistent, hindering relationships and functionality) and which makes patient care difficult. | |||||
| PRACTICE | Distress due to difficulty in managing the basic needs of the patient (hygiene, food, safety...). | |||||
| EXTERNAL | Distress due to the lack of effective external support for the cohabiting nucleus. | |||||
| MONEY | Financial distress and/or difficulties in hiring external help and/or accessing resources. | |||||
| ETHICS | INFORMATION | Distress due to difficulties in the management of information concerning diagnosis and/or prognosis. | ||||
| CLINICAL DECISIONS | Difficulties in clinical decision making (adequacy of diagnostic and/or therapeutic effort). | |||||
| DESIRE TO ADVANCE DEATH | Desire to advance death (DAD) in any degree: thought, intention, decision, plan and/or explicit request. | |||||
| DIRECT RELATIONSHIP WITH DEATH/DYING PROCESS | LOCATION | Difficulties in planning the place to die (no agreement between patient-caregiver) or request to change location. | ||||
| SITUATION IN THE LAST DAYS (LDS) | Difficulties in managing the dying process (maladaptive denial of the situation, refractory symptoms, difficult sedation). | |||||
| MOURNING | Risk factors during mourning. | |||||
| COMPLEXITY LEVEL: The highest observed in any of the affected sub-areas: | ||||||
| ≤80 Years N: 892 (53.2%) | >80 Years N: 785 (46.8%) | Total N: 1677 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Women | Men | p | Women | Men | p | Women | Men | p | |
| 326 (36.5%) | 566 (63.5%) | 410 (52.2%) | 375 (47.8%) | 736 (43.9%) | 941 (56.1%) | ||||
| Type a | 0.664 | 0.015 | 0.000 | ||||||
| Cancer | 260 (79.8%) | 469 (82.9%) | 214 (52.2%) | 226 (60.3%) | 474 (64.4%) | 695 (73.9%) | |||
| Organ failure | 28 (8.6%) | 48 (8.5%) | 85 (20.7%) | 85 (22.7%) | 113 (15.4%) | 133 (14.1%) | |||
| Neurologic | 16 (4.9%) | 23 (4.1%) | 26 (6.3%) | 11 (2.9%) | 42 (5.7%) | 34 (3.6%) | |||
| Dementia | 14 (4.3%) | 16 (2.8%) | 65 (15.9%) | 40 (10.7%) | 79 (10.7%) | 56 (6.0%) | |||
| Frailty | 8 (2.5%) | 10 (1.8%) | 20 (4.9%) | 13 (3.5%) | 28 (3.8%) | 23 (2.4%) | |||
| Functional impairment b | 267 (81.9%) | 431 (76.1%) | 0.045 | 397 (96.8%) | 338 (90.1%) | 0.000 | 664 (90.2%) | 769 (81.7%) | 0.000 |
| Cognitive impairment c | 67 (20.6%) | 113 (20.0%) | 0.833 | 184 (44.9%) | 137 (36.5%) | 0.018 | 251 (34.1%) | 250 (26.6%) | 0.001 |
| PADES assistance in days d | 43 (16–105) | 39 (15–93) | 0.314 | 39 (12–106) | 31 (11–68) | 0.038 | 41 (14–105) | 35 (14–87) | 0.077 |
| Caregiver: partner | 149 (46.6%) | 431 (76.7%) | 0.000 | 34 (8.4%) | 169 (45.9%) | 0.000 | 183 (25.2%) | 600 (64.5%) | 0.000 |
| Professional caregiver | 65 (21.2%) | 69 (12.9%) | 0.002 | 218 (54.9%) | 149 (41.2%) | 0.000 | 283 (40.3%) | 218 (24.3%) | 0.000 |
| ≤80 Years | >80 Years | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Women | Men | p | Women | Men | p | Women | Men | p | |
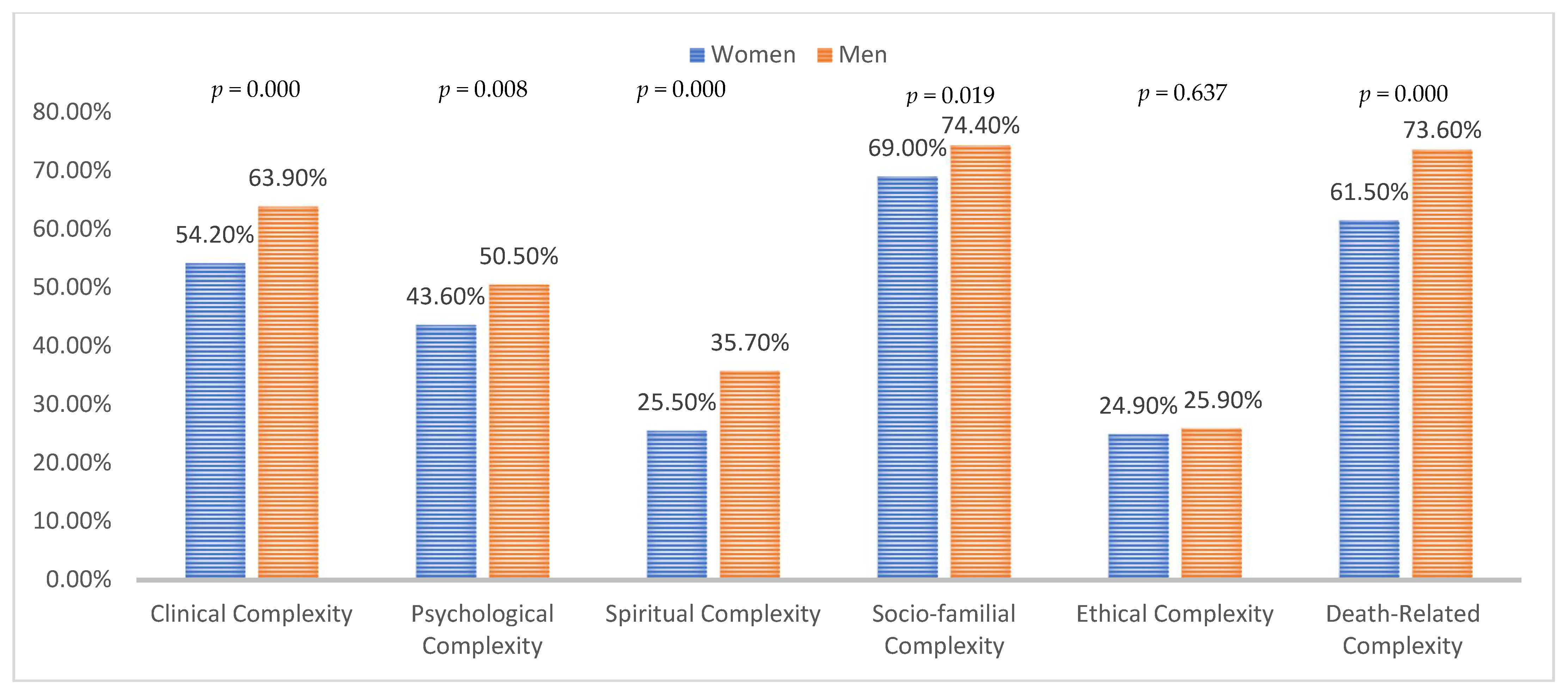
| Clinical Complexity | 198 (65.6%) | 366 (68.2%) | 0.442 | 166 (45.0%) | 202 (57.4%) | 0.001 | 364 (54.2%) | 568 (63.9%) | 0.000 |
| Physical | 175 (57.9%) | 342 (63.7%) | 0.101 | 154 (41.7%) | 180 (51.1%) | 0.011 | 329 (49.0%) | 522 (58.7%) | 0.000 |
| Therapeutical | 130 (43.0%) | 203 (37.9%) | 0.142 | 101 (27.4%) | 119 (33.8%) | 0.061 | 231 (34.4%) | 322 (36.3%) | 0.453 |
| Psychological Complexity | 156 (52.3%) | 297 (56.1%) | 0.293 | 129 (36.3%) | 146 (42.0%) | 0.127 | 285 (43.6%) | 443 (50.5%) | 0.008 |
| Personality | 72 (23.9%) | 154 (28.7%) | 0.132 | 82 (22.3%) | 76 (21.7%) | 0.823 | 154 (23.1%) | 230 (25.9%) | 0.193 |
| Emotional | 129 (42.9%) | 257 (47.9%) | 0.156 | 90 (24.5%) | 115 (32.8%) | 0.015 | 219 (32.8%) | 372 (41.9%) | 0.000 |
| Spiritual Complexity | 109 (36.5%) | 221 (41.8%) | 0.133 | 59 (16.4%) | 91 (26.4%) | 0.001 | 168 (25.5%) | 312 (35.7%) | 0.000 |
| Meaning | 82 (27.2%) | 169 (31.5%) | 0.194 | 42 (11.4%) | 70 (19.9%) | 0.002 | 124 (18.6%) | 239 (26.9%) | 0.000 |
| Connection | 36 (12.0%) | 70 (13.1%) | 0.646 | 21 (5.7%) | 35 (10.0%) | 0.035 | 57 (8.5%) | 105 (11.8%) | 0.036 |
| transcendence | 74 (24.6%) | 167 (31.1%) | 0.046 | 28 (7.6%) | 47 (13.4%) | 0.012 | 102 (15.3%) | 214 (24.1%) | 0.000 |
| Socio-familial Complexity | 231 (76.7%) | 414 (77.2%) | 0.870 | 230 (62.7%) | 246 (70.1%) | 0.036 | 461 (69.0%) | 660 (74.4%) | 0.019 |
| Relational | 71 (23.6%) | 128 (23.8%) | 0.935 | 71 (19.3%) | 70 (19.9%) | 0.840 | 142 (21.3%) | 198 (22.3%) | 0.623 |
| Emotional | 165 (54.8%) | 299 (55.8%) | 0.787 | 125 (34.1%) | 142 (40.5%) | 0.076 | 290 (43.4%) | 441 (49.7%) | 0.014 |
| Practical | 137 (45.5%) | 260 (48.6%) | 0.391 | 100 (27.2%) | 159 (45.3%) | 0.000 | 237 (35.5%) | 419 (47.3%) | 0.000 |
| External | 157 (52.2%) | 286 (53.4%) | 0.739 | 170 (46.2%) | 186 (53.0%) | 0.068 | 327 (48.9%) | 472 (53.2%) | 0.090 |
| Financial | 59 (19.6%) | 109 (20.3%) | 0.799 | 32 (8.7%) | 36 (10.3%) | 0.489 | 91 (13.6%) | 145 (16.3%) | 0.142 |
| Ethical Complexity | 84 (28.0%) | 149 (28.2%) | 0.959 | 80 (22.3%) | 77 (22.5%) | 0.942 | 164 (24.9%) | 226 (25.9%) | 0.637 |
| Information | 32 (10.6%) | 63 (11.8%) | 0.623 | 23 (6.3%) | 34 (9.7%) | 0.088 | 55 (8.2%) | 97 (10.9%) | 0.075 |
| STE | 61 (20.3%) | 96 (17.9%) | 0.402 | 65 (17.7%) | 47 (13.4%) | 0.111 | 126 (18.9%) | 143 (16.1%) | 0.157 |
| DHD | 20 (6.6%) | 37 (6.9%) | 0.887 | 25 (6.8%) | 30 (8.5%) | 0.382 | 45 (6.7%) | 67 (7.6%) | 0.537 |
| Complexity with Death | 230 (76.4%) | 431 (80.4%) | 0.173 | 181 (49.3%) | 222 (63.2%) | 0.000 | 411 (61.5%) | 653 (73.6%) | 0.000 |
| Location | 190 (63.1%) | 356 (66.4%) | 0.337 | 132 (36.0%) | 174 (49.6%) | 0.000 | 322 (48.2%) | 530 (59.8%) | 0.000 |
| SLD | 51 (16.9%) | 101 (18.8%) | 0.494 | 54 (14.7%) | 50 (14.2%) | 0.858 | 105 (15.7%) | 151 (17.0%) | 0.492 |
| Mourning | 151 (50.2%) | 238 (44.4%) | 0.109 | 80 (21.8%) | 87 (24.8%) | 0.343 | 231 (34.6%) | 325 (36.6%) | 0.402 |
| >80 Years | Gender: Man | |||
|---|---|---|---|---|
| OR (CI95%) | p | OR (CI95%) | p | |
| Clinical Complexity | 0.53 (0.43–0.65) | 0.000 | 1.36 (1.11–1.68) | 0.004 |
| Physical | 0.56 (0.46–0.69) | 0.000 | 1.36 (1.11–1.67) | 0.003 |
| Therapeutical | 0.67 (0.54–0.83) | 0.000 | 1.02 (0.82–1.26) | 0.862 |
| Psychological Complexity | 0.54 (0.44–0.67) | 0.000 | 1.21 (0.98–1.49) | 0.070 |
| Personality | 0.78 (0.61–0.98) | 0.035 | 1.12 (0.89–1.43) | 0.333 |
| Emotional | 0.49 (0.39–0.60) | 0.000 | 1.34 (1.08–1.66) | 0.008 |
| Spiritual Complexity | 0.43 (0.34–0.54) | 0.000 | 1.45 (1.15–1.82) | 0.001 |
| Meaning | 0.45 (0.35–0.58) | 0.000 | 1.45 (1.13–1.87) | 0.003 |
| Connection | 0.61 (0.43–0.86) | 0.005 | 1.34 (0.95–1.88) | 0.098 |
| transcendence | 0.31 (0.23–0.41) | 0.000 | 1.52 (1.16–1.98) | 0.002 |
| Socio-familial Complexity | 0.60 (0.48–0.75) | 0.000 | 1.21 (0.97–1.52) | 0.098 |
| Relational | 0.79 (0.62–1.01) | 0.057 | 1.02 (0.80–1.31) | 0.846 |
| Emotional | 0.49 (0.40–0.60) | 0.000 | 1.16 (0.94–1.43) | 0.159 |
| Practical | 0.66 (0.54–0.81) | 0.000 | 1.54 (1.25–1.90) | 0.000 |
| External | 0.89 (0.73–1.09) | 0.272 | 1.17 (0.95–1.43) | 0.132 |
| Financial | 0.42 (0.31–0.57) | 0.000 | 1.09 (0.82–1.46) | 0.544 |
| Ethical Complexity | 0.74 (0.58–0.94) | 0.012 | 1.01 (0.80–1.28) | 0.931 |
| Information | 0.70 (0.49–0.99) | 0.046 | 1.30 (0.91–1.85) | 0.144 |
| STE | 0.77 (0.59–1.01) | 0.061 | 0.79 (0.61–1.04) | 0.092 |
| DHD | 1.16 (0.79–1.71) | 0.454 | 1.16 (0.78–1.72) | 0.470 |
| Complexity with Death | 0.36 (0.29–0.45) | 0.000 | 1.53 (1.22–1.91) | 0.000 |
| Location | 0.41 (0.34–0.51) | 0.000 | 1.42 (1.15–1.75) | 0.001 |
| SLD | 0.77 (0.58–1.01) | 0.062 | 1.06 (0.80–1.39) | 0.693 |
| Mourning | 0.35 (0.28–0.43) | 0.000 | 0.93 (0.75–1.16) | 0.520 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busquet-Duran, X.; Moreno-Gabriel, E.; Jiménez-Zafra, E.M.; Tura-Poma, M.; Bosch-DelaRosa, O.; Moragas-Roca, A.; Martin-Moreno, S.; Martínez-Losada, E.; Crespo-Ramírez, S.; Lestón-Lado, L.; et al. Gender and Observed Complexity in Palliative Home Care: A Prospective Multicentre Study Using the HexCom Model. Int. J. Environ. Res. Public Health 2021, 18, 12307. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312307
Busquet-Duran X, Moreno-Gabriel E, Jiménez-Zafra EM, Tura-Poma M, Bosch-DelaRosa O, Moragas-Roca A, Martin-Moreno S, Martínez-Losada E, Crespo-Ramírez S, Lestón-Lado L, et al. Gender and Observed Complexity in Palliative Home Care: A Prospective Multicentre Study Using the HexCom Model. International Journal of Environmental Research and Public Health. 2021; 18(23):12307. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312307
Chicago/Turabian StyleBusquet-Duran, Xavier, Eduard Moreno-Gabriel, Eva Maria Jiménez-Zafra, Magda Tura-Poma, Olga Bosch-DelaRosa, Anna Moragas-Roca, Susana Martin-Moreno, Emilio Martínez-Losada, Silvia Crespo-Ramírez, Lola Lestón-Lado, and et al. 2021. "Gender and Observed Complexity in Palliative Home Care: A Prospective Multicentre Study Using the HexCom Model" International Journal of Environmental Research and Public Health 18, no. 23: 12307. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312307