
What Is on the Menu?—A Quantitative Analysis on Label Format among (Potential) Restaurant Guests and Restaurant Owners


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Research Instrument
2.3. Menu Labeling Formats
2.4. Statistical Analyses
3. Results
3.1. (Potential) Restaurant Guests
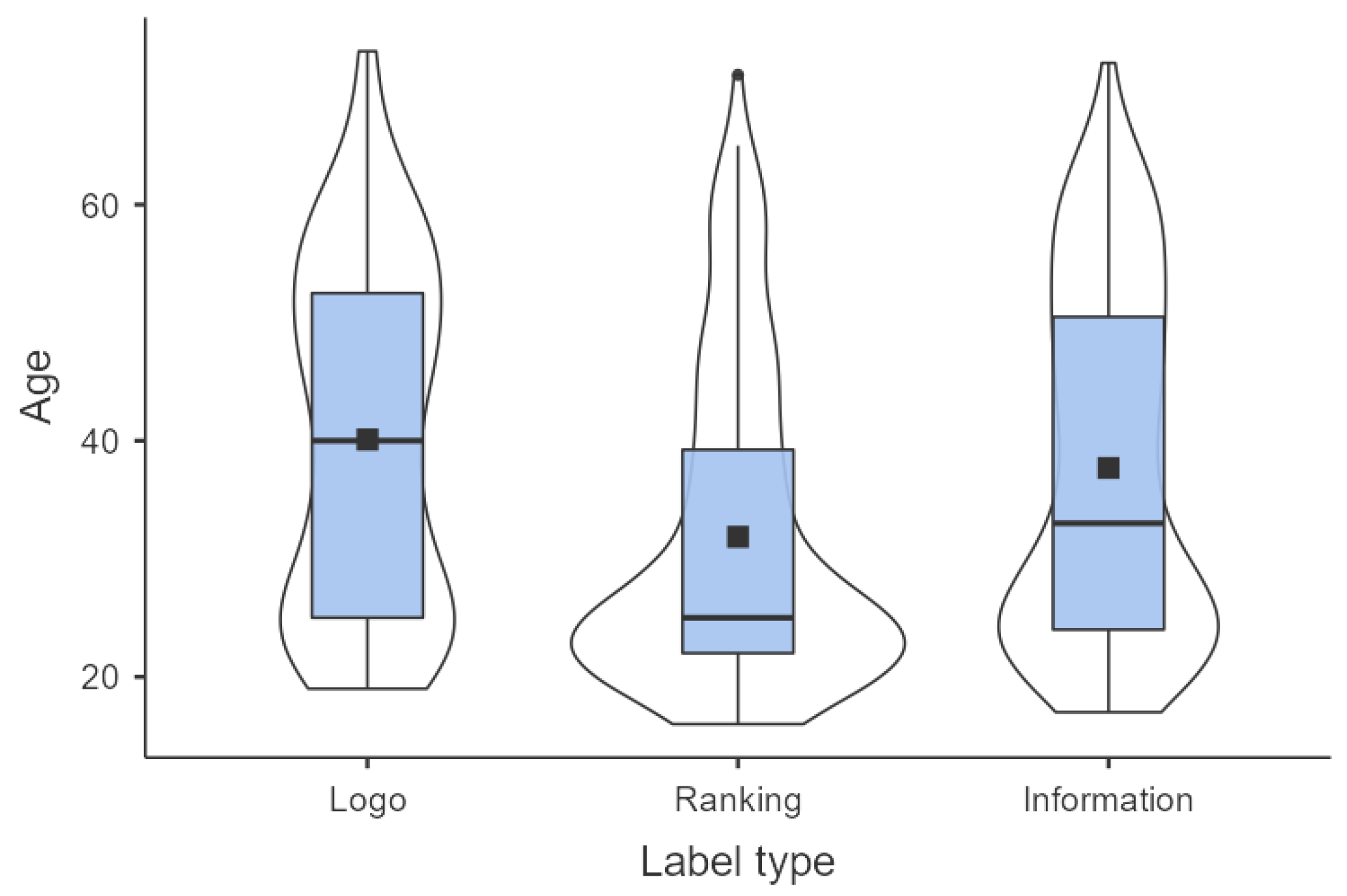
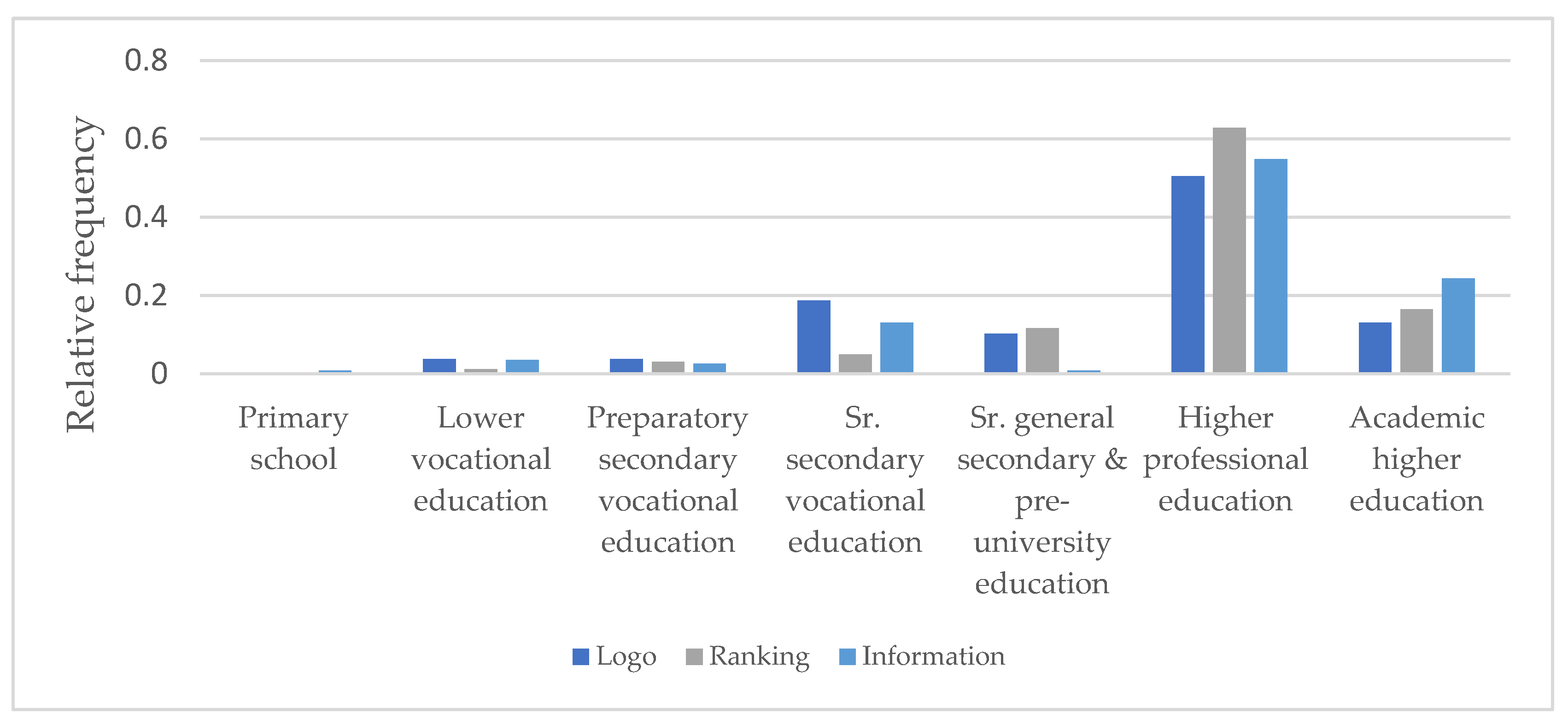
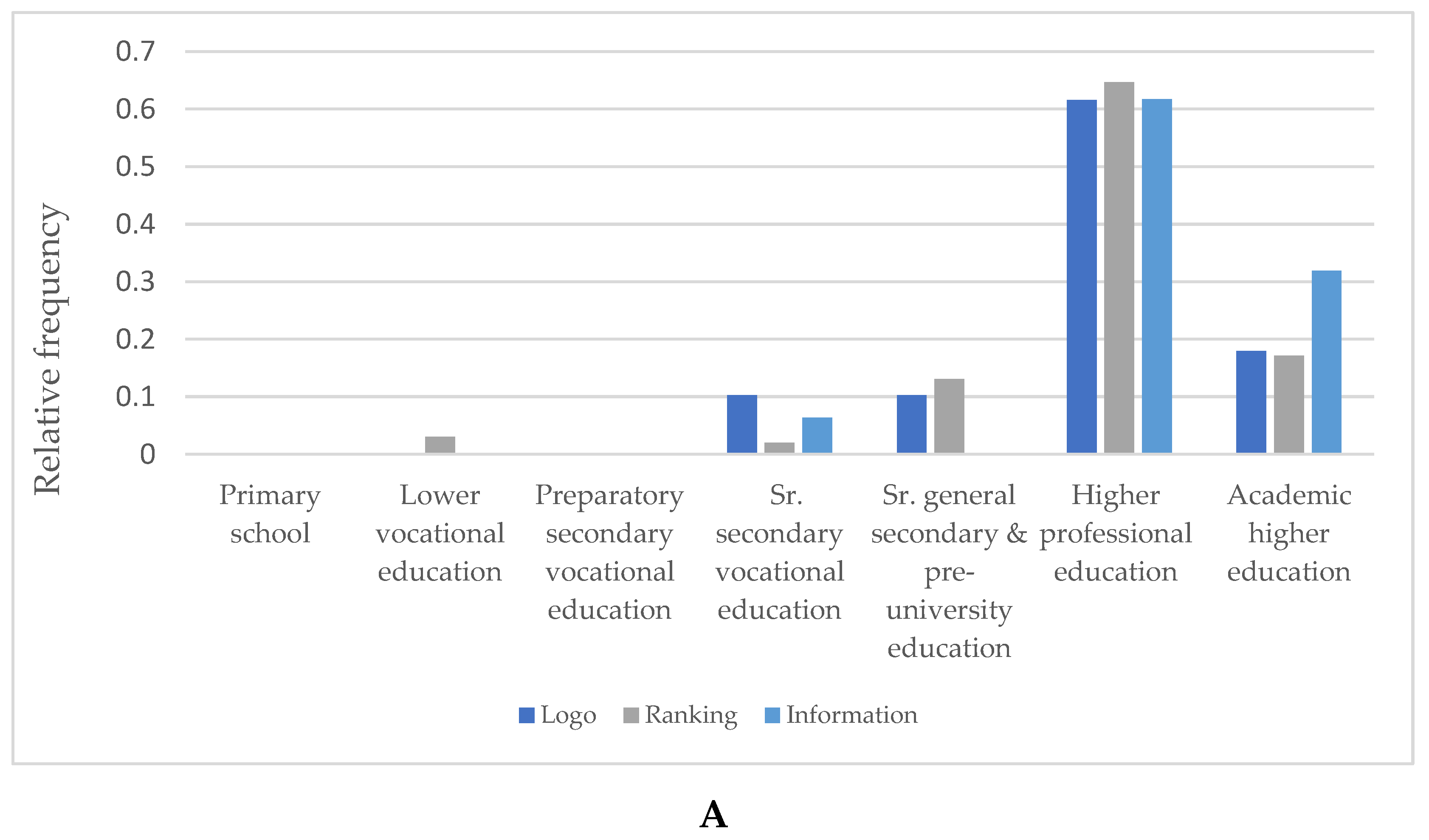
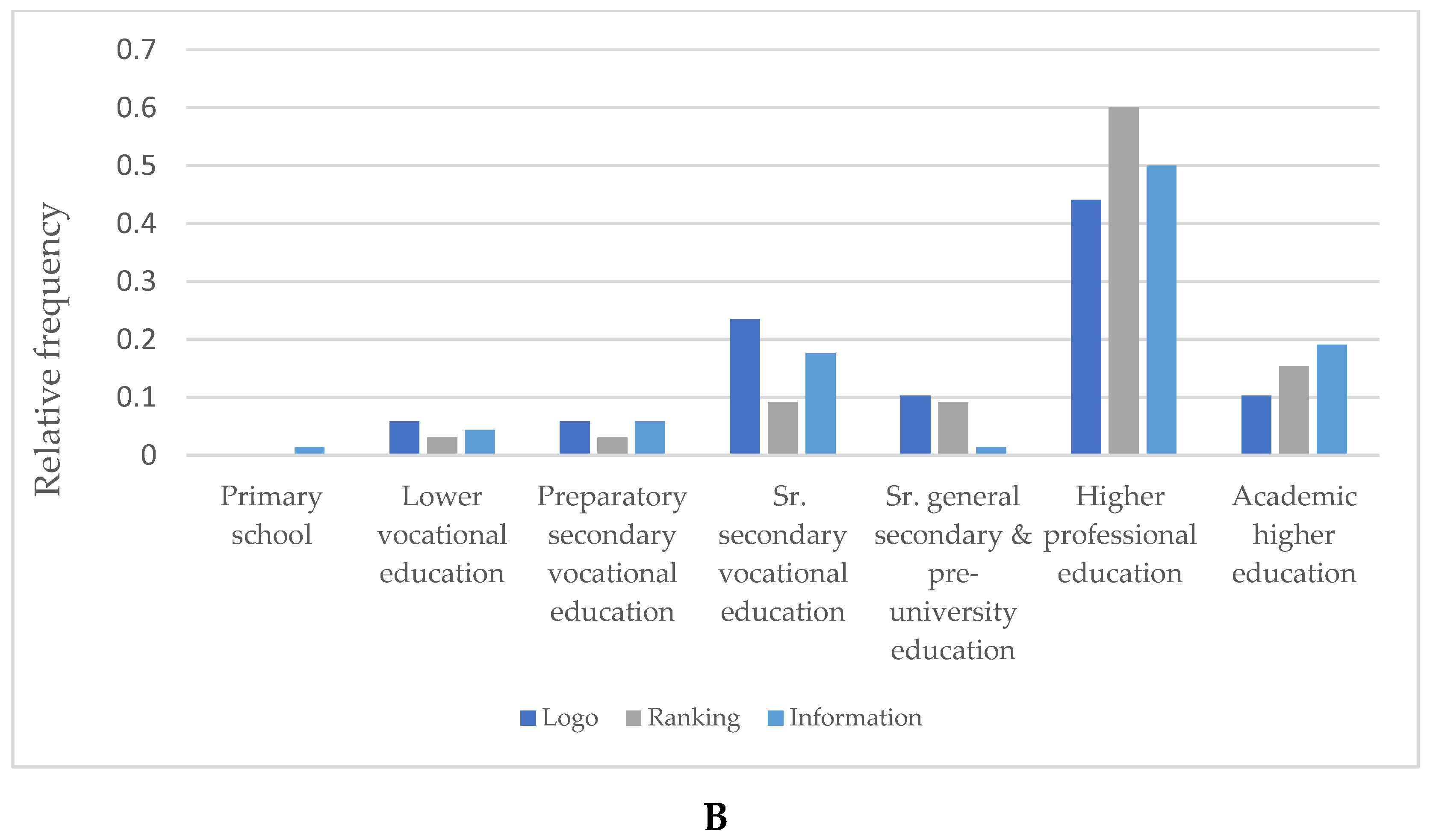
3.1.1. Overall Characteristics
3.1.2. Label Preference
3.2. Restaurant Owners
4. Discussion
4.1. (Potential) Restaurant Guests
4.2. Restaurant Owners
4.3. Limitations of the Study
4.4. Implications for the Future
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 27 September 2021).
- Hendriks, E.M.; Zantinge, C. Overgewicht|Cijfers & Context|Huidige Situatie|Volksgezondheidenzorg.Info. Available online: https://www.volksgezondheidenzorg.info/onderwerp/overgewicht/cijfers-context/huidige-situatie#!node-overgewicht-volwassenen (accessed on 27 September 2021).
- RIVM. DNFCS 2012–2016, 1–79 Years|RIVM. Available online: https://www.rivm.nl/en/dutch-national-food-consumption-survey/overview-surveys/dnfcs-2012-2016 (accessed on 27 September 2021).
- Lachat, C.; Nago, E.; Verstraeten, R.; Roberfroid, D.; Van Camp, J.; Kolsteren, P. Eating out of home and its association with dietary intake: A systematic review of the evidence. Obes. Rev. 2012, 13, 329–346. [Google Scholar] [CrossRef]
- Roberto, C.A.; Schwartz, M.B.; Brownell, K.D. Review and Special Articles Rationale and Evidence for Menu-Labeling Legislation. AMEPRE 2009, 37, 546–551. [Google Scholar] [CrossRef]
- Thomas, E. Food for thought: Obstacles to menu labelling in restaurants and cafeterias. Public Health Nutr. 2016, 19, 2185–2189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wansink, B.; Love, K. Slim by design: Menu strategies for promoting high-margin, healthy foods. Int. J. Hosp. Manag. 2014, 42, 137–143. [Google Scholar] [CrossRef]
- Fernandes, A.C.; Oliveira, R.C.; Proença, R.P.C.; Curioni, C.C.; Rodrigues, V.M.; Fiates, G.M.R. Influence of menu labeling on food choices in real-life settings: A systematic review. Nutr. Rev. 2016, 74, 534–548. [Google Scholar] [CrossRef] [PubMed]
- Patiño, S.R.-G.; Zhou, M.; Gomes, F.D.S.; Lemaire, R.; Hedrick, V.; Serrano, E.; Kraak, V.I. Effects of Menu Labeling Policies on Transnational Restaurant Chains to Promote a Healthy Diet: A Scoping Review to Inform Policy and Research. Nutrients 2020, 12, 1544. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Economos, C.D.; Spiker, M.L.; Vercammen, K.A.; VanEpps, E.M.; Block, J.P.; Elbel, B.; Story, M.; Roberto, C.A. A Systematic Review of Calorie Labeling and Modified Calorie Labeling Interventions: Impact on Consumer and Restaurant Behavior. Obesity 2017, 25, 2018–2044. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Soto, M.J.; Dunn, C.G.; Moran, A.J.; Block, J.P. Calorie and nutrient trends in large U.S. chain restaurants, 2012–2018. PLoS ONE. 2020, 15, e0228891. [Google Scholar] [CrossRef] [Green Version]
- Littlewood, J.A.; Lourenço, S.; Iversen, C.L.; Hansen, G.L. Menu labelling is effective in reducing energy ordered and consumed: A systematic review and meta-analysis of recent studies. Public Health Nutr. 2016, 19, 2106–2121. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.; Warin, L. Impact of food labelling systems on food choices and eating behaviours: A systematic review and meta-analysis of randomized studies. Obes. Rev. 2016, 17, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Cantu-Jungles, T.M.; McCormack, L.A.; Slaven, J.E.; Slebodnik, M.; Eicher-Miller, H.A. A Meta-Analysis to Determine the Impact of Restaurant Menu Labeling on Calories and Nutrients (Ordered or Consumed) in U.S. Adults. Nutrients 2017, 9, 1088. [Google Scholar] [CrossRef]
- Long, M.W.; Tobias, D.K.; Cradock, A.L.; Batchelder, H.; Gortmaker, S.L. Systematic Review and Meta-analysis of the Impact of Restaurant Menu Calorie Labeling. Am. J. Public Health 2015, 105, e11–e24. [Google Scholar] [CrossRef] [PubMed]
- Berry, C.; Burton, S.; Howlett, E.; Newman, C.L. Understanding the Calorie Labeling Paradox in Chain Restaurants: Why Menu Calorie Labeling Alone May Not Affect Average Calories Ordered. J. Public Policy Mark. 2019, 38, 192–213. [Google Scholar] [CrossRef]
- Hammond, D.; Goodman, S.; Hanning, R.; Daniel, S. A randomized trial of calorie labeling on menus. Prev. Med. 2013, 57, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Breck, A.; Cantor, J.; Martinez, O.; Elbel, B. Who reports noticing and using calorie information posted on fast food restaurant menus? Appetite 2014, 81, 30–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoefkens, C.; Veettil, P.C.; Van Huylenbroeck, G.; Van Camp, J.; Verbeke, W. What nutrition label to use in a catering environment? A discrete choice experiment. Food Policy 2018, 37, 741–750. [Google Scholar] [CrossRef]
- Vyth, E.L.; Van Der Meer, E.W.C.; Seidell, J.C.; Steenhuis, I.H.M. A nutrition labeling intervention in worksite cafeterias: An implementation evaluation across two large catering companies in the Netherlands. Health Promot. Int. 2012, 27, 230–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roodenburg, A.J.C.; Popkin, B.M.; Seidell, J.C. Development of international criteria for a front of package food labelling system: The International Choices Programme. Eur. J. Clin. Nutr. 2011, 65, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Rogers, E.M. Diffusion of Innovations; Simon and Schuster: New York, NY, USA, 2010. [Google Scholar]
- Ellison, B.; Lusk, J.L.; Davis, D. Looking at the label and beyond: The effects of calorie labels, health consciousness, and demographics on caloric intake in restaurants. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutta-Bergman, M.J. Health Attitudes, Health Cognitions, and Health Behaviors among Internet Health Information Seekers: Population-Based Survey. J. Med. Internet Res. 2004, 6, e908. [Google Scholar] [CrossRef]
- Moore, G.C.; Benbasat, I. Development of an Instrument to Measure the Perceptions of Adopting an Information Technology Innovation. Inform. Syst. Res. 1991, 2, 92–222. [Google Scholar] [CrossRef] [Green Version]
- Vyth, E.L.; Steenhuis, I.H.M.; Mallant, S.F.; Mol, Z.L.; Brug, J.; Temminghoff, M.; Feunekes, G.I.; Jansen, L.; Verhagen, H.; Seidell, J.C. A Front-of-Pack Nutrition Logo: A Quantitative and Qualitative Process Evaluation in the Netherlands. J. Health Commun. 2009, 14, 631–645. [Google Scholar] [CrossRef] [PubMed]
- Grunert, K.G.; Wills, J.M.; Fernández-Celemín, L. Nutrition knowledge, and use and understanding of nutrition information on food labels among consumers in the UK. Appetite 2010, 55, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Navarro, D.J.; FoxCroft, D.R. Learning Statistics with Jamovi. Available online: http://learnstatswithjamovi.com (accessed on 27 September 2021).
- Roodenburg, A.J.C. Nutrient profiling for front of pack labelling: How to align logical consumer choice with improvement of products? Proc. Nutr. Soc. 2017, 76, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Jaehee, P.D.; Lee, H.E. Cognitive Factors of Using Health Apps: Systematic Analysis of Relationships Among Health Consciousness, Health Information Orientation, eHealth Literacy, and Health App Use Efficacy. J. Med. Internet Res. 2014, 16, e3283. [Google Scholar] [CrossRef]
- Prasad, A.; Strijnev, A.; Zhang, Q. What can grocery basket data tell us about health consciousness? Int. J. Res. Mark. 2008, 25, 301–309. [Google Scholar] [CrossRef]
- Roodenburg, A.J.C.; Payens, I.A.J.; Vrijhof, C. Menu labeling in traditional restaurants: Opportunities, barriers and needs. In Proceedings of the IUNS 20th–ICN, Spain, Granada, 15–20 September 2013. [Google Scholar]
- Grunert, K.G.; Wills, J.M. A review of European research on consumer response to nutrition information on food labels. J. Public Health 2007, 15, 385–399. [Google Scholar] [CrossRef] [Green Version]
- Velema, E.; Vyth, E.L.; Hoekstra, T.; Steenhuis, I.H. Nudging and social marketing techniques encourage employees to make healthier food choices: A randomized controlled trial in 30 worksite cafeterias in The Netherlands. Am. J. Clin. Nutr. 2018, 107, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Carins, J.E.; Rundle-Thiele, S.R. Eating for the better: A social marketing review (2000–2012). Public Health Nutr. 2014, 17, 1628–1639. [Google Scholar] [CrossRef] [Green Version]
- Wright, B.; Bragge, P. Interventions to promote healthy eating choices when dining out: A systematic review of reviews. Br. J. Health Psychol. 2018, 23, 278–295. [Google Scholar] [CrossRef]
- Dalrymple, J.C.; Radnitz, C.; Loeb, K.L.; Keller, K.L. Optimal defaults as a strategy to improve selections from children’s menus in full-service theme park dining. Appetite 2020, 152, 104697. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Logo (n = 107) | Ranking (n = 164) | Information (n = 115) | p-Value | |
|---|---|---|---|---|
| mean (SD) | 40.1 (14.7) a | 31.9 (13.2) b | 37.7 (14.7) a | <0.001 (ANOVA) |
| min–median–max | 19–40–73 a | 16–25–71 b | 17–33–72 a | <0.001 (KW) |
| 1 | 2 | 3 | 4 | 5 | Average Likert Score | |
|---|---|---|---|---|---|---|
| A. Perceived difficulty of implementing menu labeling * (5-point Likert Scale—1 = easy, 5 = difficult) | 10% | 33.3% | 30.8% | 20.5% | 5.1% | 2.8 |
| B. Distinctive value of menu labeling (5-point Likert Scale 1 = no distinctive value, 5 = distinctive value) | 7.3% | 34.1% | 34.1% | 17.1% | 7.3% | 2.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanssen, N.S.J.; Linschooten, J.O.; van Lieverloo, J.H.M.; Roodenburg, A.J.C. What Is on the Menu?—A Quantitative Analysis on Label Format among (Potential) Restaurant Guests and Restaurant Owners. Int. J. Environ. Res. Public Health 2021, 18, 12500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312500
Hanssen NSJ, Linschooten JO, van Lieverloo JHM, Roodenburg AJC. What Is on the Menu?—A Quantitative Analysis on Label Format among (Potential) Restaurant Guests and Restaurant Owners. International Journal of Environmental Research and Public Health. 2021; 18(23):12500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312500
Chicago/Turabian StyleHanssen, Nadja S. J., Joost O. Linschooten, J. Hein M. van Lieverloo, and Annet J. C. Roodenburg. 2021. "What Is on the Menu?—A Quantitative Analysis on Label Format among (Potential) Restaurant Guests and Restaurant Owners" International Journal of Environmental Research and Public Health 18, no. 23: 12500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312500