
Oral, Vaginal and Anal Sexual Practices among Heterosexual Males and Females Attending a Sexual Health Clinic: A Cross-Sectional Survey in Melbourne, Australia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Procedure
2.2. Data Analyses
3. Results
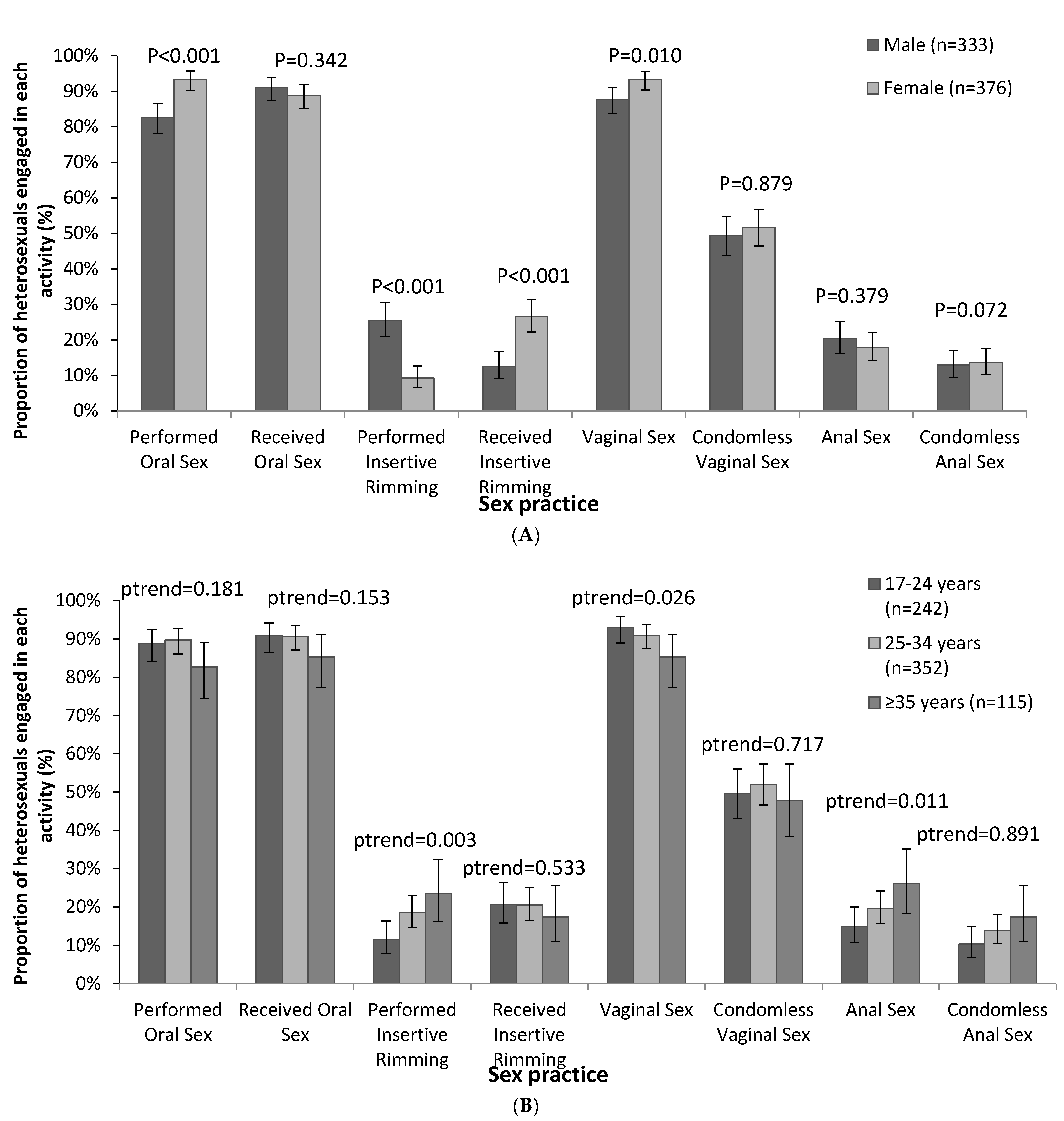
3.1. Sexual Practices
3.2. Associations with Engaging in Anal Sex
3.3. Age Pattern of Sexual Practices
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jasek, E.; Chow, E.P.; Ong, J.J.; Bradshaw, C.S.; Chen, M.Y.; Hocking, J.S.; Lee, D.; Phillips, T.; Temple-Smith, M.; Fehler, G.; et al. Sexually Transmitted Infections in Melbourne, Australia from 1918 to 2016: Nearly a century of data. Commun. Dis. Intell. 2017, 41, E212–E222. [Google Scholar]
- Phillips, T.R.; Fairley, C.K.; Chen, M.Y.; Bradshaw, C.S.; Chow, E.P.F. Risk factors for urethral gonorrhoea infection among heterosexual males in Melbourne, Australia: 2007-17. Sex. Health 2019, 16, 508–513. [Google Scholar] [CrossRef]
- Misson, J.; Chow, E.P.; Chen, M.Y.; Read, T.R.; Bradshaw, C.S.; Fairley, C.K. Trends in gonorrhoea infection and overseas sexual contacts among females attending a sexual health centre in Melbourne, Australia, 2008–2015. Commun. Dis. Intell. 2018, 42, S2209-6051. [Google Scholar]
- Mitchell, H.A.H.; Sonubi, T.; Kuyumdzhieva, G.; Harb, A.; Shah, A.; Glancy, M.; Checchi, M.; Milbourn, H.F.K.; Mohammed, H.; Contributors. Sexually Transmitted Infections and Screening for Chlamydia in England. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1015176/STI_NCSP_report_2020.pdf (accessed on 16 October 2021).
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2018; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2019. [Google Scholar]
- Kirby Institute. HIV, Viral Hepatitis and Sexually Transmissible Infections in Australia: Annual Surveillance Report 2018; Kirby Institute, UNSW Sydney: Sydney, Australia, 2018. [Google Scholar]
- Rissel, C.; Badcock, P.B.; Smith, A.M.; Richters, J.; de Visser, R.O.; Grulich, A.E.; Simpson, J.M. Heterosexual experience and recent heterosexual encounters among Australian adults: The Second Australian Study of Health and Relationships. Sex. Health 2014, 11, 416–426. [Google Scholar] [CrossRef]
- Hess, K.L.; DiNenno, E.; Sionean, C.; Ivy, W.; Paz-Bailey, G.; Group, N.S. Prevalence and Correlates of Heterosexual Anal Intercourse Among Men and Women, 20 U.S. Cities. AIDS Behav. 2016, 20, 2966–2975. [Google Scholar] [CrossRef] [Green Version]
- Habel, M.A.; Leichliter, J.S.; Dittus, P.J.; Spicknall, I.H.; Aral, S.O. Heterosexual Anal and Oral Sex in Adolescents and Adults in the United States, 2011–2015. Sex. Transm. Dis. 2018, 45, 775–782. [Google Scholar] [CrossRef]
- Chow, E.P.; Fairley, C.K. The role of saliva in gonorrhoea and chlamydia transmission to extragenital sites among men who have sex with men: New insights into transmission. J. Int. AIDS Soc. 2019, 22 (Suppl. S6), e25354. [Google Scholar] [CrossRef] [Green Version]
- Cornelisse, V.J.; Williamson, D.; Zhang, L.; Chen, M.Y.; Bradshaw, C.; Hocking, J.S.; Hoy, J.; Howden, B.P.; Chow, E.P.F.; Fairley, C.K. Evidence for a new paradigm of gonorrhoea transmission: Cross-sectional analysis of Neisseria gonorrhoeae infections by anatomical site in both partners in 60 male couples. Sex. Transm. Infect. 2019, 95, 437–442. [Google Scholar] [CrossRef]
- Fairley, C.K.; Cornelisse, V.J.; Hocking, J.S.; Chow, E.P.F. Models of gonorrhoea transmission from the mouth and saliva. Lancet Infect. Dis. 2019, 19, e360–e366. [Google Scholar] [CrossRef]
- Trebach, J.D.; Chaulk, C.P.; Page, K.R.; Tuddenham, S.; Ghanem, K.G. Neisseria gonorrhoeae and Chlamydia trachomatis among women reporting extragenital exposures. Sex. Transm. Dis. 2015, 42, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Bolshenko, B.N.V.; Rakhmatulina, R.M.R. Extragenital sexually transmitted infections: Epidemiology, clinical presentations, diagnosis, and therapy. Akusherstvo I Ginekol. 2018, 10, 41–46. [Google Scholar]
- Musil, K.; Currie, M.; Sherley, M.; Martin, S. Rectal chlamydia infection in women at high risk of chlamydia attending Canberra Sexual Health Centre. Int. J. STD AIDS 2016, 27, 526–530. [Google Scholar] [CrossRef]
- Chow, E.P.F.; Cornelisse, V.J.; Williamson, D.A.; Priest, D.; Hocking, J.S.; Bradshaw, C.S.; Read, T.R.H.; Chen, M.Y.; Howden, B.P.; Fairley, C.K. Kissing may be an important and neglected risk factor for oropharyngeal gonorrhoea: A cross-sectional study in men who have sex with men. Sex Transm. Infect. 2019. [Google Scholar] [CrossRef] [Green Version]
- Cornelisse, V.J.; Bradshaw, C.S.; Chow, E.P.F.; Williamson, D.A.; Fairley, C.K. Oropharyngeal Gonorrhea in Absence of Urogenital Gonorrhea in Sexual Network of Male and Female Participants, Australia, 2018. Emerg. Infect. Dis. 2019, 25, 1373–1376. [Google Scholar] [CrossRef]
- Vodstrcil, L.A.; Hocking, J.S.; Cummings, R.; Chen, M.Y.; Bradshaw, C.S.; Read, T.R.; Sze, J.K.; Fairley, C.K. Computer assisted self interviewing in a sexual health clinic as part of routine clinical care; impact on service and patient and clinician views. PLoS ONE 2011, 6, e18456. [Google Scholar] [CrossRef] [Green Version]
- Phillips, T.; Fairley, C.K.; Walker, S.; Chow, E.P.F. Associations between oral sex practices and frequent mouthwash use in men who have sex with men: Implications for gonorrhoea prevention. Sex. Health 2019, 16, 473–478. [Google Scholar] [CrossRef]
- Chow, E.P.F.; Walker, S.; Read, T.R.H.; Chen, M.Y.; Bradshaw, C.S.; Fairley, C.K. Self-Reported Use of Mouthwash and Pharyngeal Gonorrhoea Detection by Nucleic Acid Amplification Test. Sex. Transm. Dis. 2017, 44, 593–595. [Google Scholar] [CrossRef]
- Chandra, N.L.; Broad, C.; Folkard, K.; Town, K.; Harding-Esch, E.M.; Woodhall, S.C.; Saunders, J.M.; Sadiq, S.T.; Dunbar, J.K. Detection of Chlamydia trachomatis in rectal specimens in women and its association with anal intercourse: A systematic review and meta-analysis. Sex. Transm. Infect. 2018, 94, 320–326. [Google Scholar] [CrossRef] [Green Version]
- Heijne, J.C.M.; van Liere, G.; Hoebe, C.; Bogaards, J.A.; van Benthem, B.H.B.; Dukers-Muijrers, N. What explains anorectal chlamydia infection in women? Implications of a mathematical model for test and treatment strategies. Sex. Transm. Infect. 2017, 93, 270–275. [Google Scholar] [CrossRef] [Green Version]
- Van Liere, G.A.F.S.; Hoebe, C.J.P.A.; Dukers-Muijrers, N.H.T.M. Evaluation of the anatomical site distribution of chlamydia and gonorrhoea in men who have sex with men and in high-risk women by routine testing: Cross-sectional study revealing missed opportunities for treatment strategies. Sex. Transm. Infect. 2014, 90, 58–60. [Google Scholar] [CrossRef]
- Lau, A.; Kong, F.Y.S.; Huston, W.; Chow, E.P.F.; Fairley, C.K.; Hocking, J.S. Factors associated with anorectal Chlamydia trachomatis or Neisseria gonorrhoeae test positivity in women: A systematic review and meta-analysis. Sex. Transm. Infect. 2019, 95, 361–367. [Google Scholar] [CrossRef]
- Frederick, D.; Gillespie, B.J.; Lever, J.; Berardi, V.; Garcia, J.R. Sexual Practices and Satisfaction among Gay and Heterosexual Men in Romantic Relationships: A Comparison Using Coarsened Exact Matching in a U.S. National Sample. J. Sex. Res. 2021, 58, 545–559. [Google Scholar] [CrossRef]
- Herbenick, D.; Reece, M.; Schick, V.; Sanders, S.A.; Dodge, B.; Fortenberry, J.D. Sexual behaviors, relationships, and perceived health status among adult women in the United States: Results from a national probability sample. J. Sex. Med. 2010, 7 (Suppl. S5), 277–290. [Google Scholar] [CrossRef]
- Reece, M.; Herbenick, D.; Schick, V.; Sanders, S.A.; Dodge, B.; Fortenberry, J.D. Sexual behaviors, relationships, and perceived health among adult men in the United States: Results from a national probability sample. J. Sex. Med. 2010, 7 (Suppl. S5), 291–304. [Google Scholar] [CrossRef]
- Lewis, R.; Tanton, C.; Mercer, C.H.; Mitchell, K.R.; Palmer, M.; Macdowall, W.; Wellings, K. Heterosexual Practices Among Young People in Britain: Evidence From Three National Surveys of Sexual Attitudes and Lifestyles. J. Adolesc. Health 2017, 61, 694–702. [Google Scholar] [CrossRef] [Green Version]
- Branfman, J.; Stiritz, S.; Anderson, E. Relaxing the straight male anus: Decreasing homohysteria around anal eroticism. Sexualities 2017, 21, 109–127. [Google Scholar] [CrossRef]
- Wignall, L.; Scoats, R.; Anderson, E.; Morales, L. A qualitative study of heterosexual men’s attitudes toward and practices of receiving anal stimulation. Cult. Health Sex. 2020, 22, 675–689. [Google Scholar] [CrossRef]
- Charleson, F.J.; Fairley, C.K.; Hocking, J.S.; Vodstrcil, L.A.; Bradshaw, C.S.; Chow, E.P.F. Age, ethnic and travel-related disparities in kissing and sexual practices among heterosexual men in Melbourne, Australia. Sex. Health 2020, 17, 279–287. [Google Scholar] [CrossRef]
- Anderson, E.; Ripley, M.; McCormack, M. A Mixed-Method Study of Same-Sex Kissing Among College-Attending Heterosexual Men in the U.S. Sex. Cult. 2018, 23, 26–44. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, A.; Patrick, K.; Heywood, W.; Blackman, P.; Pitts, M. 5th National Survey of Australian Secondary Students and Sexual Health 2013, (ARCSHS Monograph Series No. 97), Australian Research Centre in Sex, Health and Society; La Trobe University: Melbourne, Australia, 2014. [Google Scholar]
- Phillips, T.R.; Fairley, C.K.; Donovan, B.; Ong, J.J.; McNulty, A.; Marshall, L.; Templeton, D.J.; Owen, L.; Ward, A.; Gunathilake, M.; et al. Sexual health service adaptations to the coronavirus disease 2019 (COVID-19) pandemic in Australia: A nationwide online survey. Aust. N. Z. J. Public Health 2021. [Google Scholar] [CrossRef]
- Chow, E.P.F.; Hocking, J.S.; Ong, J.J.; Phillips, T.R.; Fairley, C.K. Sexually Transmitted Infection Diagnoses and Access to a Sexual Health Service before and after the National Lockdown for COVID-19 in Melbourne, Australia. Open Forum Infect. Dis. 2021, 8, ofaa536. [Google Scholar] [CrossRef] [PubMed]
- Coombe, J.; Kong, F.Y.S.; Bittleston, H.; Williams, H.; Tomnay, J.; Vaisey, A.; Malta, S.; Goller, J.L.; Temple-Smith, M.; Bourchier, L.; et al. Love during lockdown: Findings from an online survey examining the impact of COVID-19 on the sexual health of people living in Australia. Sex. Transm. Infect. 2020, 97, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Kilner, A.; Fairley, C.K.; Burrell, S.; Bradshaw, C.S.; Chen, M.Y.; Chow, E.P.F. Age pattern of sexual activities with the most recent partner among men who have sex with men in Melbourne, Australia: A cross-sectional study. BMJ Sex. Reprod. Health 2020, 47, e4. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No. of Individuals (%) | No. of Men (%) | No. of Women (%) | p-Value a | |
|---|---|---|---|---|
| Age (year) | <0.001 * | |||
| 17–24 | 242 (34.1) | 82 (24.6) | 160 (42.5) | |
| 25–34 | 352 (49.7) | 168 (50.5) | 184 (48.9) | |
| ≥35 | 115 (16.2) | 83 (24.9) | 32 (8.5) | |
| Country of birth | 0.002 * | |||
| Australia | 250 (35.3) | 140 (42.0) | 110 (29.3) | |
| Overseas | 445 (62.8) | 188 (56.5) | 257 (68.4) | |
| Unknown/missing | 14 (2.0) | 5 (1.5) | 9 (2.4) | |
| Injecting drug use b | 0.433 | |||
| No | 696 (98.2) | 329 (98.8) | 367 (97.6) | |
| Yes | 5 (0.7) | 2 (0.6) | 3 (0.8) | |
| Declined to answer | 8 (1.1) | 2 (0.6) | 6 (1.6) | |
| Had a regular sex partner b | 0.003 * | |||
| No | 406 (57.3) | 171 (51.4) | 235 (62.5) | |
| Yes | 303 (42.7) | 162 (48.7) | 141 (37.5) | |
| Had a casual sex partner b | <0.001 * | |||
| No | 170 (24.0) | 100 (30.0) | 70 (18.6) | |
| Yes | 539 (76.0) | 233 (70.0) | 306 (81.4) | |
| Had kissing-only partners b | 0.717 | |||
| No | 240 (33.9) | 115 (34.5) | 125 (33.2) | |
| Yes | 469 (66.2) | 218 (65.5) | 251 (66.8) | |
| Any tongue kissing b | 0.332 | |||
| No | 6 (0.9) | 4 (1.2) | 2 (0.5) | |
| Yes | 703 (99.2) | 329 (98.8) | 374 (99.5) | |
| Kissed same-sex partner b | <0.001 * | |||
| No | 646 (91.1) | 320 (96.1) | 326 (86.7) | |
| Yes | 63 (8.9%) | 13 (3.9) | 50 (13.3) | |
| Had sex-only partners b | 0.215 | |||
| No | 468 (66.0) | 212 (63.7) | 256 (68.1) | |
| Yes | 241 (34.0) | 121 (36.3) | 120 (31.9) |
| Mean Total Partner Number (SD) a | Mean Number of Partners for Males (SD) a | Mean Number of Partners for Females (SD) a | p-Value b | |
|---|---|---|---|---|
| Kissing only | 5.5 (14.9) | 5.6 (16.4) | 5.5 (13.6) | 0.484 |
| Sex only | 2.4 (2.4) | 2.4 (2.4) | 2.4 (2.4) | 0.569 |
| Kissing and any sex | 3.6 (8.8) | 3.9 (11.9) | 3.4 (4.6) | 0.215 |
| Performed oral sex c | 2.6 (3.8) | 2.3 (2.3) | 2.8 (4.6) | 0.947 |
| Receptive oral sex d | 2.5 (3.1) | 2.7 (2.6) | 2.4 (2.0) | 0.097 |
| Performed rimming | 1.7 (1.9) | 1.8 (2.2) | 1.3 (0.6) | 0.118 |
| Receptive rimming | 1.5 (1.1) | 1.6 (1.5) | 1.5 (0.9) | 0.243 |
| Vaginal sex | 3.0 (3.9) | 2.9 (2.7) | 3.1 (4.7) | 0.796 |
| Vaginal sex with condom | 2.1 (2.8) | 1.9 (1.8) | 2.2 (3.4) | 0.873 |
| Anal sex | 1.3 (1.0) | 1.2 (0.5) | 1.3 (1.4) | 0.765 |
| Anal sex with condom | 1.2 (0.5) | 1.2 (0.5) | 1.2 (0.5) | 0.683 |
| No. of Individuals (%) | OR (95 %CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 333 (47.0) | 1 (ref) | |||
| Female | 376 (53.3) | 0.8 (0.6–1.2) | 0.379 | ||
| Age (year) | |||||
| 17–24 | 242 (34.1) | 1 (ref) | 1 (ref) | ||
| 25–34 | 352 (49.7) | 1.4 (0.9–2.2) | 0.139 | 1.4 (0.8–2.2) | 0.207 |
| ≥35 | 115 (16.2) | 2.0 (1.2–3.5) | 0.012 | 2.3 (1.2–4.2) | 0.009 * |
| Country of birth | |||||
| Australia | 250 (35.3) | 1 (ref) | |||
| Overseas | 445 (62.8) | 1.0 (0.7–1.5) | 0.923 | ||
| Unknown/missing | 14 (2.0) | 1.2 (0.3–4.4) | 0.807 | ||
| Number of vaginal sex partners | |||||
| ≤2 | 437 (61.6) | 1 (ref) | 1 (ref) | ||
| >2 | 272 (38.4) | 1.8 (1.3–2.7) | 0.002 | 1.4 (0.9–2.1) | 0.174 |
| Performed oral sex a | |||||
| No | 83 (11.7) | 1 (ref) | 1 (ref) | ||
| Yes | 629 (88.3) | 3.3 (1.4–7.8) | 0.006 | 1.5 (0.6–3.0) | 0.358 |
| Received oral sex b | |||||
| No | 72 (10.2) | 1 (ref) | 1 (ref) | ||
| Yes | 637 (89.8) | 3.4 (1.4–8.7) | 0.009 | 1.8 (0.6–4.8) | 0.267 |
| Performed insertive rimming c | |||||
| No | 589 (83.1) | 1 (ref) | 1 (ref) | ||
| Yes | 120 (16.9) | 5.1 (3.3–7.9) | <0.001 | 2.8 (1.8–4.6) | <0.001 * |
| Received rimming d | |||||
| No | 567 (80.0) | 1 (ref) | 1 (ref) | ||
| Yes | 142 (20.0) | 5.7 (3.8–8.7) | <0.001 | 3.8 (2.4–6.0) | <0.001 * |
| Condomless vaginal sex | |||||
| No | 319 (45.0) | 1 (ref) | 1 (ref) | ||
| Yes | 358 (50.5) | 1.9 (1.3–2.8) | 0.001 | 1.5 (0.9–2.3) | 0.091 |
| N/A No vaginal sex | 32 (4.5) | 0.4 (0.1–1.7) | 0.215 | 0.8 (0.2–4.1) | 0.802 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phillips, T.R.; Constantinou, H.; Fairley, C.K.; Bradshaw, C.S.; Maddaford, K.; Chen, M.Y.; Hocking, J.S.; Chow, E.P.F. Oral, Vaginal and Anal Sexual Practices among Heterosexual Males and Females Attending a Sexual Health Clinic: A Cross-Sectional Survey in Melbourne, Australia. Int. J. Environ. Res. Public Health 2021, 18, 12668. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312668
Phillips TR, Constantinou H, Fairley CK, Bradshaw CS, Maddaford K, Chen MY, Hocking JS, Chow EPF. Oral, Vaginal and Anal Sexual Practices among Heterosexual Males and Females Attending a Sexual Health Clinic: A Cross-Sectional Survey in Melbourne, Australia. International Journal of Environmental Research and Public Health. 2021; 18(23):12668. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312668
Chicago/Turabian StylePhillips, Tiffany R., Heidi Constantinou, Christopher K. Fairley, Catriona S. Bradshaw, Kate Maddaford, Marcus Y. Chen, Jane S. Hocking, and Eric P. F. Chow. 2021. "Oral, Vaginal and Anal Sexual Practices among Heterosexual Males and Females Attending a Sexual Health Clinic: A Cross-Sectional Survey in Melbourne, Australia" International Journal of Environmental Research and Public Health 18, no. 23: 12668. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312668