
Effect of Forest Therapy on Depression and Anxiety: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
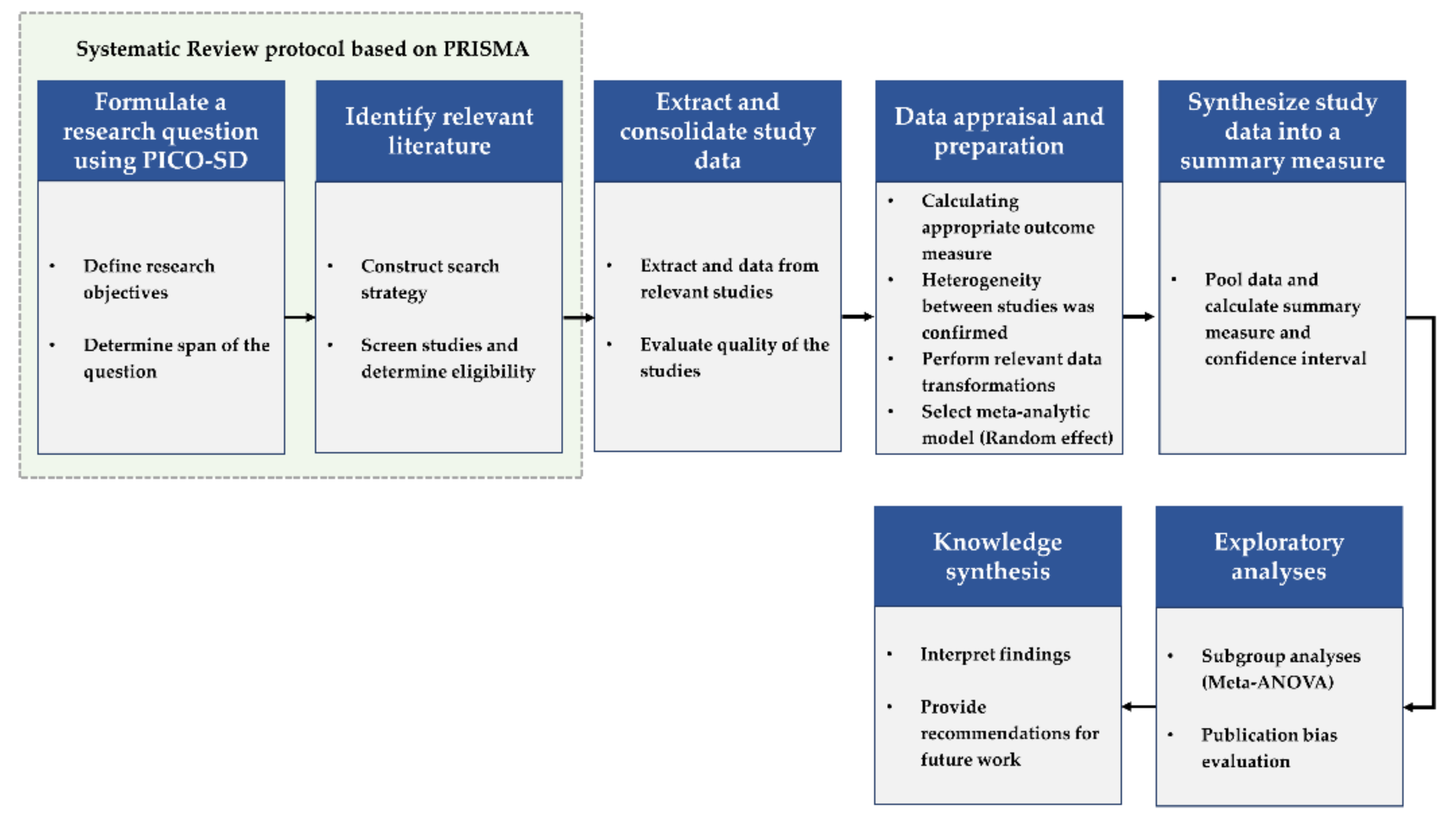
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk-of-Bias (ROB) Assessment
2.5. Meta-Analyses
3. Results
3.1. Search Results
3.2. Characteristics of Selected Studies
3.2.1. Format and Content of Forest Therapy
3.2.2. Depression or Anxiety Measures

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Study Design | Participants | Sample Size (Intervention/Control) | Intervention | Control | Duration (Time/Frequency) | Outcome |
|---|---|---|---|---|---|---|---|---|
| Bielinis et al. (2019) [54] | Poland | RCT (2 group) | Grauduate students—nonforestry course (20.97 ± 0.65 y) | 32 (16/16) | Forest recreation—relaxation: standing and viewing | Urban street environment at the urban point | 1 day (15 min/NA) | POMS: T-A *#↓ D *# |
| Jun et al. (2019) [55] | Republic of Korea | RCT (2 group) | Mild cognitive impairments (65~100 y) | 57 (28/29) | Forest therapy program—getting closer to the forest: making a natural objects, observing the habitats of animal, etc., | Daily routine activities | 8 sessions (120 min/Once a week) | GDSSF *#↓ |
| Bang et al. (2016) [56] | Republic of Korea | RCT (2 group) | University staffs (42.22 ± 11.44/37.37 ± 9.32 y) | 45 (18/27) | Walking in the urban forest during lunch time | Daily routine activities | 10 sessions (40 min/Twice a week) | BDI: N/A |
| Chun et al. (2016) [57] | Republic of Korea | RCT (2 group) | Chronic alcoholics (45.26 ± 3.89 y) | 92 (47/45) | (1) Forest therapy program—forest walking, experiencing the forest through all five senses, meditation, etc., (2) Staying at a recreational forest site | Staying in an urban hotel | 3 Night 4 Days | (1) STAI #↓ (2) BDI *↓ (3) HRSD *↓ |
| Shin et al. (2012) [58] | Republic of Korea | RCT (2 group) | Chronic alcoholics (45.26 ± 3.89 y) | 92 (47/45) | Forest therapy camp −Interacting with nature/forest, challenge, self-introspection, etc., | Daily routine activities | 9 days | BDI #↓ |
| Bang et al. (2018) [59] | Republic of Korea | Quasi-experimental design (2 group) | Elementary students (11~13 y) | 52 (24/28) | Health Promotion Program using urban forest—five senses experience in urban forest, forest walking/exercise, and playing with natural materials etc., | Routine programs (e.g., supplementary learning such as math or English, reading, art) | 10 sessions (120 min/Once a week) | CDI *#↓ |
| Bang et al. (2017) [60] | Republic of Korea | Quasi-experimental design (2 group) | University students & Graduate students (24.3 ± 4.19 y) | 99 (51/48) | Campus forest-walking program | Daily routine activities | 6 sessions (60 min/Once a week) | BDI *#↓ |
| Choi et al. (2016) [61] | Republic of Korea | Quasi-experimental design (2 group) | Middle aged woman (53.9 ± 2.69/55.5 ± 1.84 y) | 20 (11/9) | Forest walking | Treadmill walking | 36 sessions (80 min/Three times a week) | SRI: Depression #↓ |
| Han et al. (2016) [62] | Republic of Korea | Quasi-experimental design (2 group) | Full-time employees (41.6 ± 6.5/37.5 ± 8.4 y) | 61 (33/28) | Forest therapy program− forest walking, music therapy, stimaltion bodily exercise, mindfulness-based meditation, herbal tea time, etc., | Weekend routines except visiting natural environments | One night two days | BDI #↓ |
| Oh (2016) [63] | Republic of Korea | Quasi-experimental design (3 group) | Middle aged woman (40~56 y) | 60 (20/20/20) | (1) Forest therapy program—exercise, relaxation, diet, etc., (2) Urban forest therapy | Daily routine activities | 4 sessions (300 min/Once a week) | KDS *#↓ |
| Kim, M et al. (2015) [64] | Republic of Korea | Quasi-experimental design (2 group) | Psychiatric inpatients (35~56 y) | 20 (10/10) | Forest therapy program−handkerchief dyeing, decorating the frame with natural object, group work, etc., | Daily routine activities | 10 sessions (NA/5 times a week) | (1) POMS: T-A: N/A D: N/A (2) BDI: N/A |
| Kim, Y et al. (2015) [65] | Republic of Korea | Quasi-experimental design (2 group) | Cancer patients (30~79 y) | 53 (37/26) | Forest therapy program−wildflow exploration, playing in the forest, mindfulness, flower tea therapy, sharing feelings, etc., | Daily routine activities | 3 days (120 min) | (1) HADS #↓ Depresion #↓ Anxiety #↓ (2) POMS: T #↓ D #↓ |
| Choi et al. (2014) [66] | Republic of Korea | Quasi-experimental design (2 group) | Cancer patients (more than 50 y) | 53 (26/27) | Forest therapy program−forest walking and abdominal breathing, touching wood, meditation, cooperativity activities, etc., | Daily routine activities | 8 sessions (120 min/Once a week) | ZSDS *#↓ |
| Kim and Lee (2014) [67] | Republic of Korea | Quasi-experimental design (2 group) | University students | 67 (35/32) | Forest therapy program− greeting with objects in forest, meditation, forest walking, mandara made from rope, my look in forest, etc., | Daily routine activities | 8 sessions (50 min/Twice a week) | STAI #↓ |
| Lim et al. (2014) [68] | Republic of Korea | Quasi-experimental design (3 group) | Elderly people (50~99 y) | 64 (22/21/21) | (1) Forest therapy program− being familiar with forest, activating sense of nature, feeling happyness in forest, etc., (2) Forest therapy in indoor | Daily routine activities | 11 sessions (90 min/Once a week) | GDSSF *#↓ |
| Shin (2012) [69] | Republic of Korea | Quasi-experimental design (2 group) | Infants (71~73 month) | 63 (25/38) | Forest Kindergarten Education Programforest walking, nature observation activities, drawing and exploring in the forest, etc., | Basic curriculum | 7 months | KPDSS: Anxiety #↓ |
| Woo et al. (2012) [70] | Republic of Korea | Quasi-experimental design (4 group) | Major depressive disorders (43.39 ± 12.14/44.26 ± 13.49/48.40 ± 15.00/48.79 ± 9.63 y) | 81 (28/21/15/17) | (1) Forest therapy program−Mindfulness-based cognitive behavior therapy, forest activities, meditation, promoting interpersonal relationships, etc., (2) Hospital program (3) Forest bathing | Conducted same activities in the indoor | 4 sessions (180 min/Once a week) | (1) HRSD #↓ (2) BDI: N/A (3) MADRS #↓ |
| Cho et al. (2011) [71] | Republic of Korea | Quasi-experimental design (2 group) | Childrens (8~12 y) | 240 (120/120) | Forest experience camp—forest festival, forest walking, field day in the forest, forest mission impossible, and playing in the forest, etc., | Daily routine activities | 2 Night 3 Days | CDI *↓ |
| Kim (2011) [72] | Republic of Korea | Quasi-experimental design (2 group) | Middle school students (14~16 y) | 80 (40/40) | Forest therapy program− create an ecological map, talking to nature, to bring out the sense of nature, etc., | General class | 10 sessions (NA/Once a week) | CES-D *↓ |
| Song (2009) [73] | Republic of Korea | Quasi-experimental design (2 group) | Unmarried mothers (10 s~30 s) | 75 (35/35) | Forest therapy program− forest meditation, reviving the dull senses, prenatal care in the forest, etc., | Daily routine activities | 24 sessions (120 min/Twice a week) | (1) BDI *↓ (2) STAI *↓ |
3.3. Quality Assessment
3.4. Effects of Forest Therapy on Depression
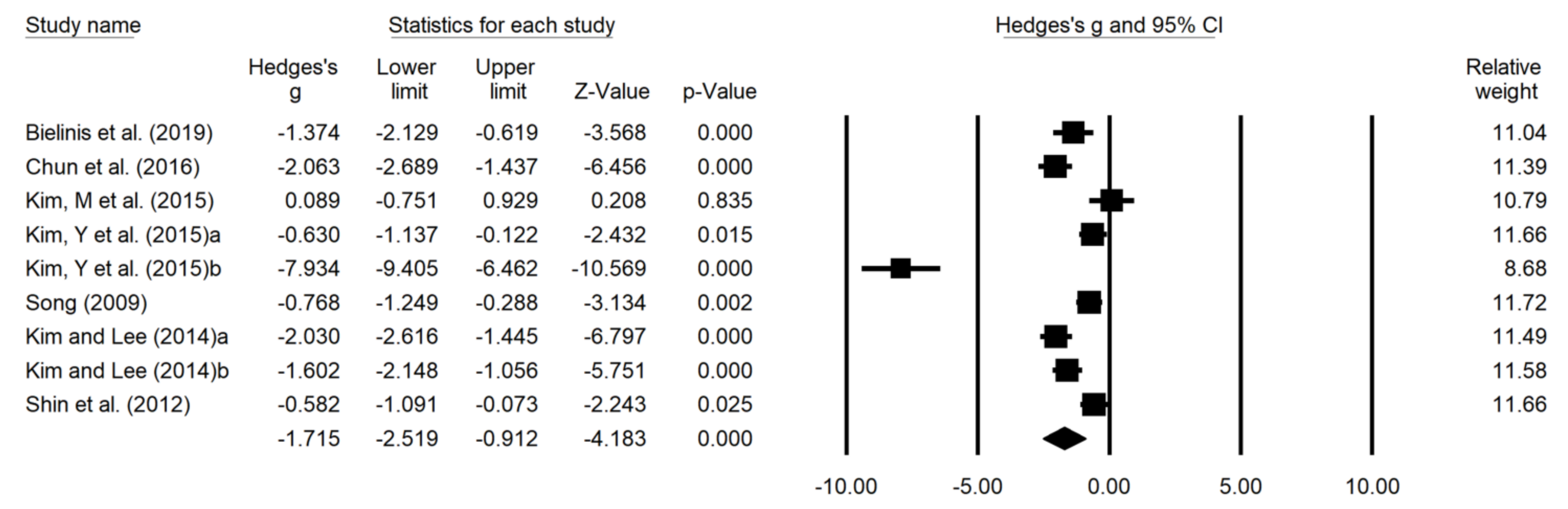
3.5. Effects of Forest Therapy on Anxiety
3.6. Verification of Heterogeneity of Effect Size: Analysis of Modulating Effect
3.6.1. Depression
3.6.2. Anxiety
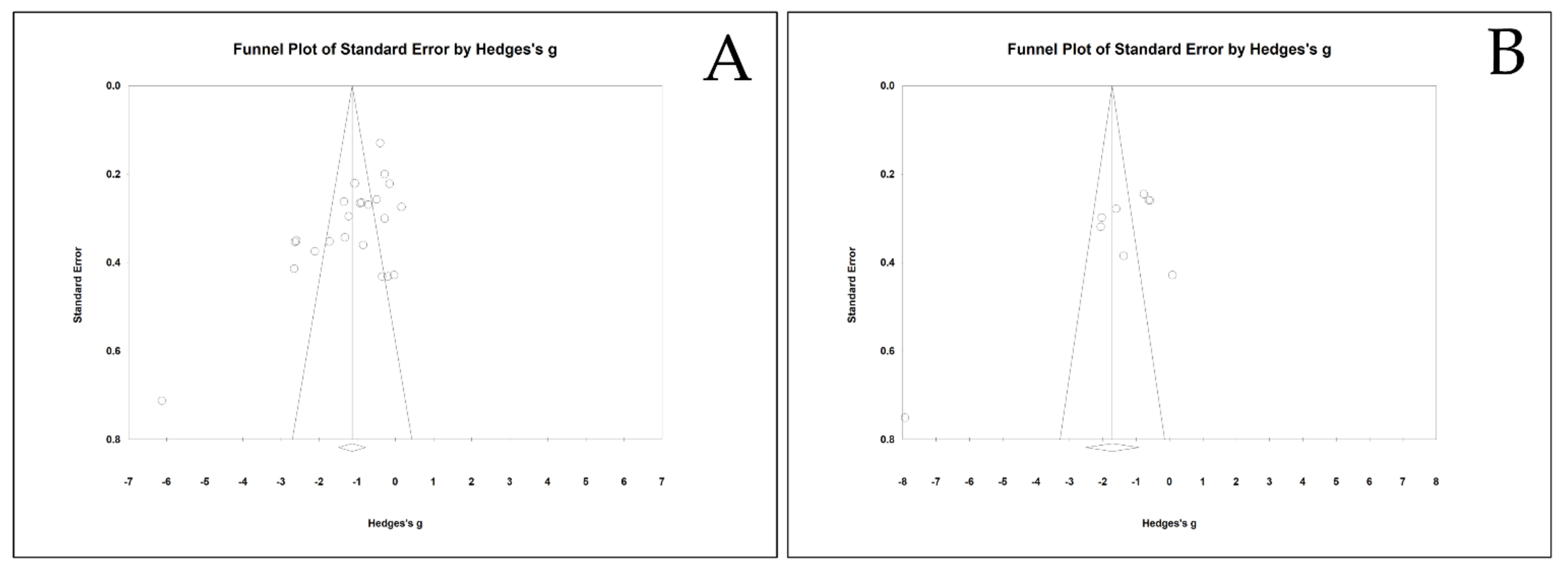
3.7. Publication Bias
4. Discussion
4.1. Summary of Findings
4.2. Limitations
4.3. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Database | Keyword | Records |
|---|---|---|
| Scopus | TITLE-ABS-KEY ((“forest*” OR “forest exposure” OR “forest bathing” OR “forest healing” OR “forest therapy” OR “shinrin-yoku” OR “urban forest*” OR “green space” OR “greenspace” OR “urban green*” OR “green exercise” OR “tree*” OR “garden*” OR “park” OR “parks” OR “landscape*” OR “horticulture*” OR “wood*” OR “natural environment*” OR “green infrastructure*” OR “greenness” OR “nature-based” OR “outdoor*” OR “recreation”) AND (“depress*” OR “depression” OR “depressive disorder” OR “anxiety*” OR “anxiety disorder” OR “Hamilton Rating Scales for Depression” OR “Hamilton Depression Rating Scale” OR “Beck Depression Inventory” OR “Hospital Anxiety and Depression Scale” OR “Montgomery-Asberg Depression Rating Scale” OR “Zung Self-Rating Depression Scale” OR “mental health”)) | 20,711 |
| PubMED | (“forest*”[Title/Abstract] OR “forest exposure”[Title/Abstract] OR “forest bathing”[Title/Abstract] OR “forest healing”[Title/Abstract] OR “forest therapy”[Title/Abstract] OR “shinrin-yoku”[Title/Abstract] OR “urban forest*”[Title/Abstract] OR “green space”[Title/Abstract] OR “greenspace”[Title/Abstract] OR “urban green*”[Title/Abstract] OR “green exercise”[Title/Abstract] OR “tree*”[Title/Abstract] OR “garden*”[Title/Abstract] OR “park”[Title/Abstract] OR “parks”[Title/Abstract] OR “landscape*”[Title/Abstract] OR “horticulture*”[Title/Abstract] OR “wood*”[Title/Abstract] OR “natural environment*”[Title/Abstract] OR “green infrastructure*”[Title/Abstract] OR “greenness”[Title/Abstract] OR “nature-based”[Title/Abstract] OR “outdoor*”[Title/Abstract] OR “recreation”[Title/Abstract]) AND (“depress*”[Title/Abstract] OR “depression”[Title/Abstract] OR “depressive disorder”[Title/Abstract] OR “anxiety*”[Title/Abstract] OR “anxiety disorder”[Title/Abstract] OR “Hamilton Rating Scales for Depression”[Title/Abstract] OR “Hamilton Depression Rating Scale”[Title/Abstract] OR “Beck Depression Inventory”[Title/Abstract] OR “Hospital Anxiety[Title/Abstract] AND Depression Scale”[Title/Abstract] OR “Montgomery-Asberg Depression Rating Scale”[Title/Abstract] OR “Zung Self-Rating Depression Scale”[Title/Abstract] OR “mental health”[Title/Abstract]) | 5777 |
| MEDLINE | TI ( “forest*” OR “forest exposure” OR “forest bathing” OR “forest healing” OR “forest therapy” OR “shinrin-yoku” OR “urban forest*” OR “green space” OR “greenspace” OR “urban green*” OR “green exercise” OR “tree*” OR “garden*” OR “park” OR “parks” OR “landscape*” OR “horticulture*” OR “wood*” OR “natural environment*” OR “green infrastructure*” OR “greenness” OR “nature-based” OR “outdoor*” OR “recreation” ) AND TI ( “depress*” OR “depression” OR “depressive disorder” OR “anxiety*” OR “anxiety disorder” OR “Hamilton Rating Scales for Depression” OR “Hamilton Depression Rating Scale” OR “Beck Depression Inventory” OR “Hospital Anxiety and Depression Scale” OR “Montgomery-Asberg Depression Rating Scale” OR “Zung Self-Rating Depression Scale” OR “mental health”) | 352 |
| Web of Science | (TS = (“forest*” OR “forest exposure” OR “forest bathing” OR “forest healing” OR “forest therapy” OR “shinrin-yoku” OR “urban forest*” OR “green space” OR “greenspace” OR “urban green*” OR “green exercise” OR “tree*” OR “garden*” OR “park” OR “parks” OR “landscape*” OR “horticulture*” OR “wood*” OR “natural environment*” OR “green infrastructure*” OR “greenness” OR “nature-based” OR “outdoor*” OR “recreation”)) AND TS = (“depress*” OR “depression” OR “depressive disorder” OR “anxiety*” OR “anxiety disorder” OR “Hamilton Rating Scales for Depression” OR “Hamilton Depression Rating Scale” OR “Beck Depression Inventory” OR “Hospital Anxiety and Depression Scale” OR “Montgomery-Asberg Depression Rating Scale” OR “Zung Self-Rating Depression Scale” OR “mental health”) | 14,138 |
| EMBASE | (‘forest exposure’:ab,ti OR ‘urban green’:ab,ti OR ‘landscape’:ab,ti OR ‘forest bathing’:ab,ti OR ‘forest therapy’:ab,ti OR ‘forest healing’:ab,ti OR ‘urban forest’:ab,ti OR greenspace:ab,ti OR park:ab,ti OR ‘green exercise’:ab,ti) AND (depression:ab,ti OR ‘depressive disorder’:ab,ti OR anxiety:ab,ti OR ‘anxiety disorder’:ab,ti) | 853 |
| RISS | 전체: 숲 <AND> 전체: 우울 | 113 |
| 전체: 숲 <AND> 전체: 불안 | 167 | |
| 전체: 산림 <AND> 전체: 우울 | 103 | |
| 전체: 산림 <AND> 전체: 불안 | 107 | |
| 전체: 도시숲 <AND> 전체: 우울 | 25 | |
| 전체: 도시숲 <AND> 전체: 불안 | 37 | |
| 전체: 자연 <AND> 전체: 우울 | 1099 | |
| 전체: 자연 <AND> 전체: 불안 | 3539 | |
| 전체: 산림치유 <AND> 전체: 우울 | 59 | |
| 전체: 산림치유 <AND> 전체: 불안 | 28 | |
| DBpia | 전체 = 숲 AND 전체 = 우울 | 175 |
| 전체 = 숲 AND 전체 = 불안 | 266 | |
| 전체 = 산림 AND 전체 = 우울 | 1028 | |
| 전체 = 산림 AND 전체 = 불안 | 4962 | |
| 전체 = 도시숲 AND 전체 = 우울 | 104 | |
| 전체 = 도시숲 AND 전체 = 불안 | 173 | |
| 전체 = 자연 AND 전체 = 우울 | 27,048 | |
| 전체 = 자연 AND 전체 = 불안 | 82,345 | |
| 전체 = 산림치유 AND 전체 = 우울 | 443 | |
| 전체 = 산림치유 AND 전체 = 불안 | 935 |
| 5 Randomized Controlled Trials—Revised Cochrane Risk-Of-Bias Assessment Tool for Randomized Controlled Trial (ROB 2.0) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Study | Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall | ||
| Bielinis et al. (2019) [54] | Low | Low | Low | Some concerns | Low | Some concerns | ||
| Jun et al. (2019) [55] | Some concerns | Low | Low | Some concerns | Low | Some concerns | ||
| Bang et al. (2016) [56] | High | Low | Low | Some concerns | Low | High | ||
| Chun et al. (2016) [57] | Some concerns | Low | Low | Some concerns | Low | Some concerns | ||
| Shin et al. (2012) [58] | High | Low | Low | Some concerns | Low | High | ||
| 15 Quasi-experimental studies—Risk-of-bias in non-randomized studies—of interventions tool (ROBINS-I) | ||||||||
| Study | Baseline confounding | Selection of participants | Classification of<break/>interventions | Deviation from intended interventions | Missing data | Measurement of outcomes | Selection of reported results | Overall |
| Bang et al. (2018) [59] | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Bang et al. (2017) [60] | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Choi et al. (2016) [61] | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Han et al. (2016) [62] | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Oh (2016) [63] | Low | Low | Low | Low | Low | High | Low | High |
| Kim, M et al.(2015) [64] | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Kim, Y et al. (2015) [65] | Low | Low | Low | Low | Low | High | Low | High |
| Choi et al. (2014) [66] | Low | Low | Low | Low | Low | High | Low | High |
| Kim and Lee (2014) [67] | Low | Low | Low | Low | Low | High | Low | High |
| Lim et al. (2014) [68] | Low | Low | Low | Low | Low | High | Low | High |
| Shin (2012) [69] | Low | Low | Low | Low | Low | High | Low | High |
| Woo et al. (2012) [70] | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Cho et al. (2011) [71] | Low | Low | Low | Low | Low | High | Low | High |
| Kim (2011) [72] | Low | Low | Low | Low | Low | High | Low | High |
| Song (2009) [73] | Low | Low | Low | Low | Low | High | Low | High |

| Egger’s Regression Intercept | ||||||
|---|---|---|---|---|---|---|
| Intercept | 95% Lower Limt | 95% Upper Limit | t | df | p-value | |
| Depressoin | −5.024 | −8.237 | −1.811 | 3.252 | 21.000 | 0.004 |
| Anxiety | −9.448 | −18.757 | −0.139 | 2.400 | 7.000 | 0.047 |
| Duval and Tweedies’s Trim and Fill—Random Effects Model | ||||||
| Studies Trimmed | Point Estimate (Heggins’s g) | 95% Lower Limit | 95% Upper Limit | Q-value | ||
| Depression | Observed values | –1.152 | –1.515 | –0.789 | 206.838 | |
| Adjusted values | 3 | –1.342 | –1.734 | –0.949 | 314.582 | |
| Anxiety | Observed values | –1.715 | –2.519 | –0.912 | 120.259 | |
| Adjusted values | 3 | –2.476 | –3.497 | –1.456 | 374.969 | |
Appendix B
| Section and Topic | Item # | Checklist item | Page |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | 4 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | 4 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | 4 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | 3 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | 6 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | 4 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | 4 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | 4 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | 4 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | 4 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | 5 |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | 5 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | 5 | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | 5 | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | 5 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | 5 | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | 5 | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | 5 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | 5 |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | 5 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | 6 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | 6 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | 9 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | 10 |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | 10 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | 10 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | 10–12 | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | 12 | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | 12 |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | 12 |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | 12 |
| 23b | Discuss any limitations of the evidence included in the review. | 16 | |
| 23c | Discuss any limitations of the review processes used. | 16 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | 17 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | 16 |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | 16 | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | - | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | 18 |
| Competing interests | 26 | Declare any competing interests of review authors. | 18 |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | 18 |
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: A web-based crosssectional survey. MedRxiv 2020, 288, 112954. [Google Scholar]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Fried, E.I. The 52 symptoms of major depression: Lack of content overlap among seven common depression scales. J. Affect. Disord. 2017, 208, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Gorman, J.M. Comorbid depression and anxiety spectrum disorders. Depress Anxiety 1996, 4, 160–168. [Google Scholar] [CrossRef]
- Cuijpers, P.; Noma, H.; Karyotaki, E.; Vinkers, C.H.; Cipriani, A.; Furukawa, T.A. A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry 2020, 19, 92–107. [Google Scholar] [CrossRef] [PubMed]
- Bostwick, J.M. A Generalist’s Guide to Treating Patients With Depression with an Emphasis on Using Side Effects to Tailor Antidepressant Therapy. Mayo Clin. Proc. 2010, 85, 538–550. [Google Scholar] [CrossRef] [Green Version]
- Robert, T.S. Sexual Dysfunction Associated with Antidepressant Therapy. Urol. Clin. N. Am. 2007, 34, 575–579. [Google Scholar]
- Carvalho, A.F.; Sharma, M.S.; Brunoni, A.R.; Vieta, E.; Fava, G.A. The safety, tolerability and risks associated with the use of newer generation antidepressant drugs: A critical review of the literature. Psychother. Psychosom. 2016, 85, 270–288. [Google Scholar] [CrossRef]
- Ravindran, L.N.; Stein, M.B. The pharmacologic treatment of anxiety disorders: A review of progress. J. Clin. Psychiatry 2010, 71, 839–854. [Google Scholar] [CrossRef]
- Farach, F.J.; Pruitt, L.D.; Jun, J.J.; Jerud, A.B.; Zoellner, L.A.; Roy-Byrne, P.P. Pharmacological treatment of anxiety disorders: Current treatments and future directions. J. Anxiety Disord. 2012, 26, 833–843. [Google Scholar] [CrossRef] [Green Version]
- Selzer, R.; Blashki, G.; Ellen, S.; Norman, T. Depression and anxiety: Pharmacological treatment in general practice. Aust. Fam. Physician 2007, 36, 222–228. [Google Scholar]
- Garakani, A.; Murrough, J.W.; Freire, R.C.; Thom, R.P.; Larkin, K.; Buono, F.D.; Iosifescu, D.V. Pharmacotherapy of anxiety disorders: Current and emerging treatment options. Focus 2021, 19, 222–242. [Google Scholar] [CrossRef] [PubMed]
- Warner, C.H.; Bobo, W.; Warner, C.M.; Reid, S.; Rachal, J. Antidepressant discontinuation syndrome. Am. Fam. Physician 2006, 74, 449–456. [Google Scholar] [PubMed]
- Harvey, B.H.; Slabbert, F.N. New insights on the antidepressant discontinuation syndrome. Hum. Psychopharmacol. 2014, 29, 503–516. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J. Consult. Clin. Psychol. 2010, 78, 169. [Google Scholar] [CrossRef] [PubMed]
- Fumero, A.; Peñate, W.; Oyanadel, C.; Porter, B. The effectiveness of mindfulness-based interventions on anxiety disorders. a systematic meta-review. Eur. J. Psychol. Educ. 2020, 10, 52. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Smits, J.A. Cognitive-behavioral therapy for adult anxiety disorders: A meta-analysis of randomized placebo-controlled trials. J. Clin. Psychiatry 2008, 69, 621–632. [Google Scholar] [CrossRef]
- Cuijpers, P.; Berking, M.; Andersson, G.; Quigley, L.; Kleiboer, A.; Dobson, K.S. A meta-analysis of cognitive-behavioural therapy for adult depression, alone and in comparison with other treatments. Can. J. Psychiatry 2013, 58, 376–385. [Google Scholar] [CrossRef] [Green Version]
- Jayakody, K.; Gunadasa, S.; Hosker, C. Exercise for anxiety disorders: Systematic review. Br. J. Sports Med. 2014, 48, 187–196. [Google Scholar] [CrossRef]
- Kvam, S.; Kleppe, C.L.; Nordhus, I.H.; Hovland, A. Exercise as a treatment for depression: A meta-analysis. J. Affect. Disord. 2016, 202, 67–86. [Google Scholar] [CrossRef]
- De Manincor, M.; Bensoussan, A.; Smith, C.A.; Barr, K.; Schweickle, M.; Donoghoe, L.L.; Bourchier, S.; Fahey, P. Individualized yoga for reducing depression and anxiety, and improving well-being: A randomized controlled trial. Depress. Anxiety 2016, 33, 816–828. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H.; Anheyer, D.; Lauche, R.; Dobos, G. A systematic review of yoga for major depressive disorder. J. Affect. Disord. 2017, 213, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Doimo, I.; Masiero, M.; Gatto, P. Forest and wellbeing: Bridging medical and forest research for effective forest-based initiatives. Forests 2020, 11, 791. [Google Scholar] [CrossRef]
- Wolf, K.L.; Lam, S.T.; McKeen, J.K.; Richardson, G.R.; van den Bosch, M.; Bardekjian, A.C. Urban trees and human health: A scoping review. Int. J. Environ. Res. Public Health 2020, 17, 4371. [Google Scholar] [CrossRef] [PubMed]
- Li, Q. What is Forest Medicine? In Forest Medicine; Nova Science Publisher: New York, NY, USA, 2013. [Google Scholar]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Wakayama, Y.; Kawada, T.; Ohira, T.; Takayama, N.; et al. A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins in female subjects. J. Biol. Regul. Homeost. Agents 2008, 22, 45–55. [Google Scholar] [PubMed]
- Park, B.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of shinrin-yoku (taking in the atmosphere of the forest)—Using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Sung, J.; Woo, J.; Kim, W.; Lim, S.; Chung, E. The effect of cognitive behavior Therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [CrossRef]
- Furuhashi, S. Physiological evaluation of the effects of Shinrin-yoku (taking in the atmosphere of the forest) in Kayanodaira highland, Kijimadaira village, Nagano prefecture. Kanto J. For. Res. 2007, 58, 219–222. [Google Scholar]
- Park, B.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15, 18. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, H.; Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Analysis of individual variations in autonomic responses to urban and forest environments. Evid. Based Complement. Altern. Med. 2015, 2015, 671094. [Google Scholar] [CrossRef]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, E.; Imai, M.; Okawa, M.; Miyaura, T.; Miyazaki, S. A before and after comparison of the effects of forest walking on the sleep of a community-based sample of people with sleep complaints. Biopsychosoc. Med. 2011, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolling, A.; Nilsson, H.; Lundell, Y. Stress recovery in forest or handicraft environments—An intervention study. Urban For. Urban Green 2017, 27, 162–172. [Google Scholar] [CrossRef]
- Bielinis, E.; Takayama, N.; Boiko, S.; Omelan, A.; Bielinis, L. The effect of winter forest bathing on psychological relaxation of young Polish adults. Urban For. Urban Green 2018, 29, 276–283. [Google Scholar] [CrossRef]
- Pretty, J.; Peacock, J.; Hine, R.; Sellens, M.; South, N.; Griffin, M. Green exercise in the UK countryside: Effects on health and psychological well-being, and implications for policy and planning. J. Environ. Plan. Manag. 2007, 50, 211–231. [Google Scholar] [CrossRef]
- Joung, D.; Song, C.; Ikei, H.; Okuda, T.; Igarashi, M.; Koizumi, H.; Miyazaki, Y.; Bum-Jin, P.; Toshitaka, Y.; Michiko, T.; et al. Physiological and psychological effects of olfactory stimulation with D-limonene. Adv Hortic. Sci. 2014, 28, 90–94. [Google Scholar]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effects of walking in a forest on young women. Int. J. Environ. Res. Public Health 2019, 16, 229. [Google Scholar] [CrossRef] [Green Version]
- Triguero-Mas, M.; Gidlow, C.J.; Martínez, D.; De Bont, J.; Carrasco-Turigas, G.; Martínez-Íñiguez, T.; Hurst, G.; Masterson, D.; Donaire-Gonzalez, D.; Seto, E.; et al. The effect of randomised exposure to different types of natural outdoor environments compared to exposure to an urban environment on people with indications of psychological distress in Catalonia. PLoS ONE 2017, 12, e0172200. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.; Choi, H.; Bang, K.S.; Kim, S.; Song, M.; Lee, B. Effects of Forest Therapy on Depressive Symptoms among Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2017, 14, 321. [Google Scholar] [CrossRef]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 1–11. [Google Scholar] [CrossRef]
- Wen, Y.; Yan, Q.; Pan, Y.; Gu, X.; Liu, Y. Medical empirical research on forest bathing (Shinrin-yoku): A systematic review. Environ. Health Prev. Med. 2019, 24, 70. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Richardson, M.; Sheffield, D. Effects of Shinrin-Yoku (forest bathing) and nature therapy on mental health: A systematic review and meta-analysis. Int. J. Ment. Health Addict. 2020, 1–25. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bach Pages, A.; Peñuelas, J.; Clarà, J.; Llusià, J.; Campillo i López, F.; Maneja, R. How should forests be characterized in regard to human health? Evidence from existing literature. Int. J. Environ. Res. Public Health 2020, 17, 1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grilli, G.; Sacchelli, S. Health benefits derived from forest: A review. Int. J. Environ. Res. Public Health 2020, 17, 6125. [Google Scholar] [CrossRef] [PubMed]
- Rajoo, K.S.; Karam, D.S.; Abdullah, M.Z. The physiological and psychosocial effects of forest therapy: A systematic review. Urban For. Urban Green. 2020, 54, 126744. [Google Scholar] [CrossRef]
- Mikolajewicz, N.; Komarova, S.V. Meta-analytic methodology for basic research: A practical guide. Front. Physiol. 2019, 10, 203. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomized trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral-Sciences Perceptual and Motor Skills; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Updated September 2020); The Cochrane Collaboration: London, UK, 2020; Available online: www.training.cochrane.org/handbook (accessed on 30 June 2021).
- Bielinis, E.; Łukowski, A.; Omelan, A.; Boiko, S.; Takayama, N.; Grebner, D.L. The effect of recreation in a snow-covered forest environment on the psychological wellbeing of young adults: Randomized controlled study. Forests 2019, 10, 827. [Google Scholar] [CrossRef] [Green Version]
- Jun, A.Y.; Lee, K.S.; Lee, S.M. Effects of the forest experience intervention program on depression, cognitive function, and quality of life in the elderly people with mild cognitive impairment. Korean J. Health Educ. Promot. 2019, 36, 73–82. [Google Scholar] [CrossRef]
- Bang, K.S.; Lee, I.S.; Kim, S.J.; Song, M.K.; Park, S.E. The Effects of Urban Forest-walking Program on Health Promotion Behavior, Physical Health, Depression, and Quality of Life: A Randomized Controlled Trial of Office-workers. J. Korean Acad. Nurs. 2016, 46, 140–148. [Google Scholar] [CrossRef] [Green Version]
- Chun, M.H.; Chang, M.C.; Lee, S.J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S. The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bang, K.S.; Kim, S.; Song, M.K.; Kang, K.I.; Jeong, Y. The effects of a health promotion program using urban forests and nursing student mentors on the perceived and psychological health of elementary school children in vulnerable populations. Int. J. Environ. Res. Public Health 2018, 15, 1977. [Google Scholar] [CrossRef] [Green Version]
- Bang, K.S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.K.; Park, B.J.; Song, M.K. The effects of a campus forest-walking program on undergraduate and graduate students’ physical and psychological health. Int. J. Environ. Res. Public Health 2017, 14, 728. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.H.; Kim, H.J.; Shin, C.S.; Yeon, P.S.; Lee, J.S. The Effect of 12-Week Forest Walking on Functional Fitness, Self-Efficacy, and Stress in the Middle-Aged Women. J. Korean Inst. For. Recreat. 2016, 20, 27–38. [Google Scholar] [CrossRef]
- Han, J.W.; Choi, H.; Jeon, Y.H.; Yoon, C.H.; Woo, J.M.; Kim, W. The effects of forest therapy on coping with chronic widespread pain: Physiological and psychological differences between participants in a forest therapy program and a control group. Int. J. Environ. Res. Public Health 2016, 13, 255. [Google Scholar] [CrossRef] [Green Version]
- Oh, J. Effects of the Forest Healing on Stress, Fatigue and Depression of Middle-Aged Women. Master’s Thesis, Wonkwang Digital University, Iksan, Korea, 2016. [Google Scholar]
- Kim, M.H.; Shim, B.S.; Wi, A.J.; Yoon, B.S.; Han, Y.H.; Oh, E.M.; An, K.W. The Influence of Forest Experience Program on Physiological and Psychological States in Psychiatric Inpatients. J. Korean For. Soc. 2015, 104, 133–139. [Google Scholar] [CrossRef]
- Kim, Y.G.; Lee, S.H.; Kim, Y.H.; Eum, J.O.; Yim, Y.R.; Ha, T.G.; Shin, C.S. The Influence of Forest Activity Intervention on Anxiety, Depression, Profile of Mood States(POMS) and Hope of Cancer Patients. J. Korean Inst. For. Recreat. 2015, 19, 65–74. [Google Scholar]
- Choi, Y.H.; Ha, Y.S. The Effectiveness of a Forest-experience-integration Intervention for Community Dwelling Cancer Patients’ Depression and Resilience. J. Korean Acad. Community Health Nurs. 2014, 25, 109–118. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.J.; Lee, S.S. Effects of Forest Therapy Program in School Forest on Employment Stress and Anxiety of University Students. J. Korean Soc. People Plants Environ. 2014, 17, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.S.; Kim, D.J.; Yeoun, P.S. Changes in Depression Degree and Self-esteem of Senior Citizens in a Nursing Home According to Forest Therapy Program. J. Korean Inst. For. Recreat. 2014, 18, 1–11. [Google Scholar]
- Shin, J.Y. The Development and Effects of the Forest Kindergarten Education Program Focusing on Expressive Life Area. Korean Soc. Early Child. Teach. Educ. 2012, 2, 163–188. [Google Scholar]
- Woo, J.M.; Park, S.M.; Lim, S.K.; Kim, W. Synergistic Effect of Forest Environment and Therapeutic Program for the Treatment of Depression. J. Korean For. Soc. 2012, 101, 677–685. [Google Scholar]
- Cho, Y.M.; Shin, W.S.; Yeon, P.S.; Lee, H.E. The Influence of Forest Experience Program on Children from Low Income Families, Sociality and Depression. J. Korean Inst. For. Recreat. 2011, 15, 69–75. [Google Scholar]
- Kim, Y. The Influence of Forest Therapeutic Program on the Depression and Self-Esteem of Middle School Students in WEEclass. Master’s Thesis, Chungbuk National University, Cheongju, Korea, 2011. [Google Scholar]
- Song, J. The Effect of Forest Therapy on Improvement of Self-esteem and Alleviation of Depression and Anxiety Disorder of Unwed Mother. Ph.D. Thesis, Chungbuk National University, Cheongju, Korea, 2009. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Rosa, C.D.; Larson, L.R.; Collado, S.; Profice, C.C. Forest therapy can prevent and treat depression: Evidence from meta-analyses. Urban For. Urban Green. 2020, 57, 126943. [Google Scholar] [CrossRef]
- Stier-Jarmer, M.; Throner, V.; Kirschneck, M.; Immich, G.; Frisch, D.; Schuh, A. The psychological and physical effects of forests on human health: A systematic review of systematic reviews and meta-analyses. Int. J. Environ. Res. Public Health 2021, 18, 1770. [Google Scholar] [CrossRef] [PubMed]
- Furuyashiki, A.; Tabuchi, K.; Norikoshi, K.; Kobayashi, T.; Oriyama, S. A comparative study of the physiological and psychological effects of forest bathing (Shinrin-yoku) on working age people with and without depressive tendencies. Environ. Health Prev. Med. 2019, 24, 46–57. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kobayashi, M.; Miura, T.; Li, Q.; Kagawa, T.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effects of viewing forest landscape on middle-aged hypertensive men. Urban For. Urban Green. 2017, 21, 247–252. [Google Scholar] [CrossRef]
- Sonntag-Öström, E.; Stenlund, T.; Nordin, M.; Lundell, Y.; Ahlgren, C.; Fjellman-Wiklund, A.; Järvholm, L.S.; Dolling, A. Nature’s effect on my mind”—Patients qualitative experiences of a forest-based rehabilitation programme. Urban For. Urban Green. 2015, 14, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y. A Meta-Analysis on Effects of Forest Therapy Program. Ph.D. Thesis, Chungbuk National University, Cheongju, Korea, 2019. [Google Scholar]
- Christup, H. The effect of dance therapy on the concept of body image. In Therapy in Motion; Costonis, M., Ed.; University of Illinois: Urbana, IL, USA, 2017; pp. 153–161. [Google Scholar]
- Igawahara, K.; Kagawa, T.; Takayama, N.; Park, B.J. Research on the effect which a guide brings about in a forest walk. J. Jpn. Inst. Landsc. Arch. 2007, 70, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.G.; Shin, W.S. Forest Therapy Alone or with a Guide: Is There a Difference between Self-Guided Forest Therapy and Guided Forest Therapy Programs? Int. J. Environ. Res. Public Health 2021, 18, 6957. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.M.; Kim, D.J.; Lee, K.H.; Lee, H.E.; Lee, Y.J. A study on effect of forest related programs based on the meta-analysis. J. Korean Inst. For. Recreat. 2015, 19, 1–13. [Google Scholar]
- Park, K.R.; Shin, D.Y. The structure and content analysis of youth Resilience improvement program: Focusing on the articles published in domestic journals (1999–2016). Korean J. Youth Stud. 2018, 25, 199–224. [Google Scholar] [CrossRef]
- Kwon, K.I.; Jung, S.L. Group Counseling; Hakjusa: Seoul, Korea, 2013. [Google Scholar]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; CUP Archive: Cambridge, UK, 1989. [Google Scholar]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Simons, R.F. Stress recovery during exposure to. Artic. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Lee, K.E.; Williams, K.J.H.; Sargent, L.D.; Williams, N.S.G.; Johnson, K.A. 40-s green roof views sustain attention: The role of micro-breaks in attention restoration. J. Environ. Psychol. 2015, 42, 182–189. [Google Scholar] [CrossRef]
- Ohly, H.; White, M.P.; Wheeler, B.W.; Bethel, A.; Ukoumunne, O.C.; Nikolaou, V.; Garside, R. Attention restoration theory: A systematic review of the attention restoration potential of exposure to natural environments. J. Toxicol. Environ. Health B 2016, 19, 305–343. [Google Scholar] [CrossRef] [Green Version]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Nix, G.A.; Ryan, R.M.; Manly, J.B.; Deci, E.L. Revitalization through self-regulation: The effects of autonomous and controlled motivation on happiness and vitality. J. Exp. Soc. Psychol. 1999, 35, 266–284. [Google Scholar] [CrossRef] [Green Version]
- Bowler, D.; Buyung-Ali, L.; Knight, T.; Pullin, A. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [Green Version]
- Tsunetsugu, Y.; Lee, J.; Park, B.; Tyrväinen, L.; Kagawa, T.; Miyazaki, Y. Physiological and psychological effects of viewing urban forest landscapes assessed by multiple measurements. Landsc. Urban Plan. 2013, 113, 90–93. [Google Scholar] [CrossRef]
- Hartig, T. Restoration in nature: Beyond the conventional narrative. In Nature and Psychology: Biological, Cognitive, Developmental, and Social Pathways to Well-Being; Schutte, A., Torquati, J., Stevens, J.R., Eds.; Springer: New York, NY, USA, 2021; in press. [Google Scholar]
- Nukarinen, T.; Rantala, J.; Korpela, K.; Browning, M.H.; Istance, H.O.; Surakka, V.; Raisamo, R. Measures and modalities in restorative virtual natural environments: An integrative narrative review. Comput. Hum. Behav. 2021, 126, 107008. [Google Scholar] [CrossRef]
- Ryan, R.M.; Weinstein, N.; Bernstein, J.; Brown, K.W.; Mistretta, L.; Gagné, M. Vitalizing effects of being outdoors and in nature. J. Environ. Psychol. 2010, 30, 159–168. [Google Scholar] [CrossRef]
- Anderson, A.P.; Mayer, M.D.; Fellows, A.M.; Cowan, D.R.; Hegel, M.T.; Buckey, J.C. Relaxation with Immersive Natural Scenes Presented Using Virtual Reality. Aerosp. Med. Hum. Perform. 2017, 88, 520–526. [Google Scholar] [CrossRef]
- Hartig, T. Restorative environments. In Encyclopedia of Applied Psychology; Spielberger, C., Ed.; Academic Press: San Diego, CA, USA, 2004; Volume 3, pp. 273–279. [Google Scholar]
- Song, C.; Ikei, H.; Park, B.J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Association between the psychological effects of viewing forest landscapes and trait anxiety level. Int. J. Environ. Res. Public Health. 2020, 17, 5479. [Google Scholar] [CrossRef]
- Jo, H.; Song, C.; Ikei, H.; Enomoto, S.; Kobayashi, H.; Miyazaki, Y. Physiological and Psychological Effects of Forest and Urban Sounds Using High-Resolution Sound Sources. Int. J. Environ. Res. Public Health 2019, 16, 15. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Zhao, X.; Zeng, Z.; Qiu, X. The influence of audio-visual interactions on psychological responses of young people in urban green areas: A case study in two parks in China. Int. J. Environ. Res. Public Health 2019, 16, 1845. [Google Scholar] [CrossRef] [Green Version]
- Ochiai, H.; Song, C.; Jo, H.; Oishi, M.; Imai, M.; Miyazaki, Y. Relaxing Effect Induced by Forest Sound in Patients with Gambling Disorder. Sustainability 2020, 12, 5969. [Google Scholar] [CrossRef]
- Abe, T.; Hisama, M.; Tanimoto, S.; Shibayama, H.; Mihara, Y.; Nomura, M. Antioxidant effects and antimicrobial activities of phytoncide. Biocontrol. Sci. 2008, 13, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.J.; Wakayama, Y.; et al. Visiting a forest, but not a city, increases human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2008, 21, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Šimpraga, M.; Ghimire, R.P.; Van Der Straeten, D.; Blande, J.D.; Kasurinen, A.; Sorvari, J.; Holopainen, T.; Adriaenssens, S.; Holopainen, J.K.; Kivimaenpaa, M. Unravelling the functions of biogenic volatiles in boreal and temperate forest ecosystems. Eur. J. For. Res. 2019, 138, 763–787. [Google Scholar] [CrossRef] [Green Version]
- Antonelli, M.; Donelli, D.; Barbieri, G.; Valussi, M.; Maggini, V.; Firenzuoli, F. Forest Volatile Organic Compounds and Their Effects on Human Health: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2020, 17, 6506. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.E.; Shin, W.S.; Yeoun, P.S.; Cho, Y.M.; Yeom, S.H. Effects of inhalation of essential oil (Chamaecyparis obtusa) on stress and depression in college students. J. Korean Inst. For. Recreat. 2011, 15, 61–68. [Google Scholar]
- Linck, V.M.; da Silva, A.L.; Figueiró, M.; Caramão, E.B.; Moreno, P.R.H.; Elisabetsky, E. Effects of inhaled Linalool in anxiety, social interaction and aggressive behavior in mice. Phytomedicine 2010, 17, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Souto-Maior, F.N.; de Carvalho, F.L.; de Morais, L.C.S.L.; Netto, S.M.; de Sousa, D.P.; de Almeida, R.N. Anxiolytic-like effects of inhaled linalool oxide in experimental mouse anxiety models. Pharmacol. Biochem. Behav. 2011, 100, 259–263. [Google Scholar] [CrossRef] [Green Version]
- Guzmán-Gutiérrez, S.L.; Gómez-Cansino, R.; García-Zebadúa, J.C.; Jiménez-Pérez, N.C.; Reyes-Chilpa, R. Antidepressant activity of Litsea glaucescens essential oil: Identification of β-pinene and linalool as active principles. J. Ethnopharmacol. 2012, 143, 673–679. [Google Scholar] [CrossRef]
- Guzmán-Gutiérrez, S.L.; Bonilla-Jaime, H.; Gómez-Cansino, R.; Reyes-Chilpa, R. Linalool and β-pinene exert their antidepressant-like activity through the monoaminergic pathway. Life Sci. 2015, 128, 24–29. [Google Scholar] [CrossRef]
- Ikei, H.; Song, C.; Miyazaki, Y. Physiological Effects of Touching Wood. Int. J. Environ. Res. Public Health 2017, 14, 7. [Google Scholar] [CrossRef]
- Koga, K.; Iwasaki, Y. Psychological and physiological effect in humans of touching plant foliage—using the semantic differential method and cerebral activity as indicators. J. Physiol. Anthropol. 2013, 32, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lederbogen, F.; Kirsch, P.; Haddad, L.; Streit, F.; Tost, H.; Schuch, P.; Wüst, S.; Pruessner, J.C.; Rietschel, M.; Deuschle, M.; et al. City living and urban upbringing affect neural social stress processing in humans. Nature 2011, 474, 498–501. [Google Scholar] [CrossRef]
- McKenzie, K.; Murray, A.; Booth, T. Do urban environments increase the risk of anxiety, depression and psychosis? an epidemiological study. J. Affect. Disord. 2013, 150, 1019–1024. [Google Scholar] [CrossRef] [Green Version]
- Sundquist, K.; Frank, G.; Sundquist, J.A.N. Urbanisation and incidence of psychosis and depression: Follow-up study of 4.4 million women and men in Sweden. Br. J. Psychiatry 2004, 184, 293–298. [Google Scholar] [CrossRef] [Green Version]
- Peen, J.; Schoevers, R.A.; Beekman, A.T.; Dekker, J. The current status of urban-rural differences in psychiatric disorders. Acta Psychiatr. Scand. 2010, 121, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.K.; Srivastava, M.; Tiwary, N.K.; Kumar, A. Prevalence of depression and anxiety among children in rural and suburban areas of Eastern Uttar Pradesh: A cross-sectional study. Fam. Med. Prim. Care. 2018, 7, 21. [Google Scholar]
- Gori, A.; Giannini, M.; Topino, E.; Cacioppo, M.; Palmieri, G.; De Sanctis, E.; Loscalzo, Y.; Burgassi, C.; Manzi, C.; Giovannelli, P.; et al. Mental health and rural communities: Prevalence of psychopathology among children and preadolescents in a mountainous area of Italy. J. Psychopathol. 2021, 27, 90–98. [Google Scholar]
- World Health Organization. Urban Population Growth. Available online: http://www.who.int (accessed on 14 August 2021).
- Buckley, R.; Brough, P.; Hague, L.; Chauvenet, A.; Fleming, C.; Roche, E.; Sofija, E.; Harris, N. Economic value of protected areas via visitor mental health. Nat. Commun. 2019, 10, 5005. [Google Scholar] [CrossRef] [PubMed]
- Becker, D.A.; Browning, M.H.; Kuo, M.; Van Den Eeden, S.K. Is green land cover associated with less health care spending? Promising findings from county-level Medicare spending in the continental United States. Urban For. Urban Green. 2019, 41, 39–47. [Google Scholar] [CrossRef]
- Blackhart, G.C.; Minnix, J.A.; Kline, J.P. Can EEG asymmetry patterns predict future development of anxiety and depression? A preliminary study. Biol. Psychol. 2006, 72, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Thibodeau, R.; Jorgensen, R.S.; Kim, S. Depression, anxiety, and resting frontal EEG asymmetry: A meta-analytic review. J. Abnorm. Psychol. 2006, 115, 715–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, B.H.; Thayer, J.F. Autonomic balance revisited: Panic anxiety and heart rate variability. J. Psychosom. Res. 1998, 44, 133–151. [Google Scholar] [CrossRef]
- Kemp, A.H.; Quintana, D.S.; Felmingham, K.L.; Matthews, S.; Jelinek, H.F. Depression, comorbid anxiety disorders, and heart rate variability in physically healthy, unmedicated patients: Implications for cardiovascular risk. PLoS ONE 2012, 7, e30777. [Google Scholar] [CrossRef] [PubMed]
- Dettori, J. Loss to follow-up. Evid. Based Spine Care J. 2011, 2, 7–10. [Google Scholar] [CrossRef] [Green Version]
- Kjaergard, L.L.; Villumsen, J.; Gluud, C. Reported methodologic quality and discrepancies between large and small randomized trials in meta-analyses. Ann. Intern. Med. 2001, 135, 982–989. [Google Scholar] [CrossRef]




| PICO-SD | Inclusion Criteria |
|---|---|
| Population | Studies with humans, healthy or not. |
| Intervention | Studies must include experimental conditions in which participants were directly exposed to the forest environments. Direct natural exposure should not expose participants to natural virtual landscapes (e.g., images or videos of nature projected onto the screen or viewed using virtual reality goggles) but to outdoor environments containing forest elements. |
| Comparison | Studies including at least one control group |
| Outcomes | Any outcome related to depression or anxiety |
| Setting | Studies of environments that primary study authors described as a forest |
| Study design | Randomized controlled trials (RCTs) or quasi-RCTs |
| Subgroups | Subgroup by Factors | k | Pooled Hedges’s g (95% CI) | Test of Null | Heterogeneity | |||
|---|---|---|---|---|---|---|---|---|
| Z-Value | p-Value | Q-Value | df (Q) | p-Value | ||||
| Participant | Overall | 23 | 1.133 (−1.490 to −0.776) | −6.220 | <0.001 | 5.793 | 3 | 0.122 |
| Chronic disease | 3 | 1.009 (−1.974 to −0.043) | −2.048 | 0.041 | ||||
| Healthy | 10 | 1.242 (−1.783 to −0.701) | −4.501 | <0.001 | ||||
| Infants & children & adolescent | 3 | 0.136 (−1.082 to 0.809) | −0.282 | 0.778 | ||||
| Mental disorders | 7 | 1.522 (−2.190 to −0.854) | −4.466 | <0.001 | ||||
| Activity type | Overall | 23 | 1.139 (−1.513 to −0.765) | −5.965 | <0.001 | 0.085 | 1 | 0.770 |
| Day | 7 | 1.221 (−1.888 to −0.554) | −3.587 | <0.001 | ||||
| Session | 16 | 1.101 (−1.553 to −0.649) | −4.775 | <0.001 | ||||
| Activity content | Overall | 22 | 1.148 (−1.518 to −0.777) | −6.074 | <0.001 | 3.595 | 1 | 0.058 |
| Forest therapy program | 19 | 1.291 (−1.690 to −0.892) | −6.344 | <0.001 | ||||
| Forest walking | 3 | 0.252 (−1.249 to 0.745) | −0.496 | 0.620 | ||||
| Time | Overall | 19 | 1.018 (−1.393 to −0.644) | −5.324 | <0.001 | 10.418 | 2 | 0.005 |
| Less than 60 min | 5 | 0.356 (−1.089 to 0.376) | −0.953 | 0.340 | ||||
| Within 61 to 120 min | 9 | 0.862 (−1.396 to −0.327) | −3.161 | 0.002 | ||||
| More than 121 min | 5 | 2.035 (−2.790 to −1.279) | −5.279 | <0.001 | ||||
| Duration | Overall | 23 | 1.141 (−1.520 to −0.761) | −5.891 | <0.001 | 3.025 | 2 | 0.220 |
| 1~3 weeks | 10 | 1.018 (−1.589 to −0.447) | −3.492 | <0.001 | ||||
| 4~7 weeks | 6 | 1.712 (−2.471 to −0.952) | −4.418 | <0.001 | ||||
| 8~12 weeks | 7 | 0.854 (−1.537 to −0.171) | −2.452 | 0.014 | ||||
| Subgroups | Subgroup by Factors | k | Pooled Hedges’s g (95% CI) | Test of Null | Heterogeneity | |||
|---|---|---|---|---|---|---|---|---|
| Z-Value | p-Value | Q-Value | df (Q) | p-Value | ||||
| Participant | Overall | 7 | 2.184 (−3.249 to −1.119) | −4.019 | <0.001 | 2.644 | 1 | 0.104 |
| Chronic disease | 3 | 3.236 (−4.892 to −1.580) | −3.829 | <0.001 | ||||
| Healthy | 4 | 1.442 (−2.832 to −0.051) | −2.032 | 0.042 | ||||
| Activity type | Overall | 9 | 1.728 (−2.573 to −0.883) | −4.008 | <0.001 | 3.903 | 1 | 0.048 |
| Day | 4 | 2.711 (−4.001 to −1.420) | −4.118 | <0.001 | ||||
| Session | 5 | 0.990 (−2.108 to 0.129) | −1.734 | 0.083 | ||||
| Time | Overall | 7 | 1.899 (−3.049 to −0.749) | −3.236 | 0.001 | 1.733 | 1 | 0.188 |
| Less than 60 min | 4 | 1.242 (−2.752 to 0.268) | −1.612 | 0.107 | ||||
| Within 61 to 120 min | 3 | 2.807 (−4.582 to −1.032) | −3.100 | 0.002 | ||||
| Duration | Overall | 8 | 1.901 (−2.886 to −0.916) | −3.782 | <0.001 | 2.731 | 1 | 0.098 |
| Within a week | 4 | 2.753 (−4.164 to −1.342) | −3.824 | <0.001 | ||||
| 2~4 weeks | 4 | 1.091 (−2.467 to 0.285) | −1.554 | 0.120 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeon, P.-S.; Jeon, J.-Y.; Jung, M.-S.; Min, G.-M.; Kim, G.-Y.; Han, K.-M.; Shin, M.-J.; Jo, S.-H.; Kim, J.-G.; Shin, W.-S. Effect of Forest Therapy on Depression and Anxiety: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12685. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312685
Yeon P-S, Jeon J-Y, Jung M-S, Min G-M, Kim G-Y, Han K-M, Shin M-J, Jo S-H, Kim J-G, Shin W-S. Effect of Forest Therapy on Depression and Anxiety: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(23):12685. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312685
Chicago/Turabian StyleYeon, Poung-Sik, Jin-Young Jeon, Myeong-Seo Jung, Gyeong-Min Min, Ga-Yeon Kim, Kyung-Mi Han, Min-Ja Shin, Seong-Hee Jo, Jin-Gun Kim, and Won-Sop Shin. 2021. "Effect of Forest Therapy on Depression and Anxiety: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 23: 12685. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312685