
Quantifying the Costs to Different Funders over Five-Years for Women Diagnosed with Breast Cancer in Queensland, Australia: A Data Linkage Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assigning Costs
2.3. Statistical Analysis
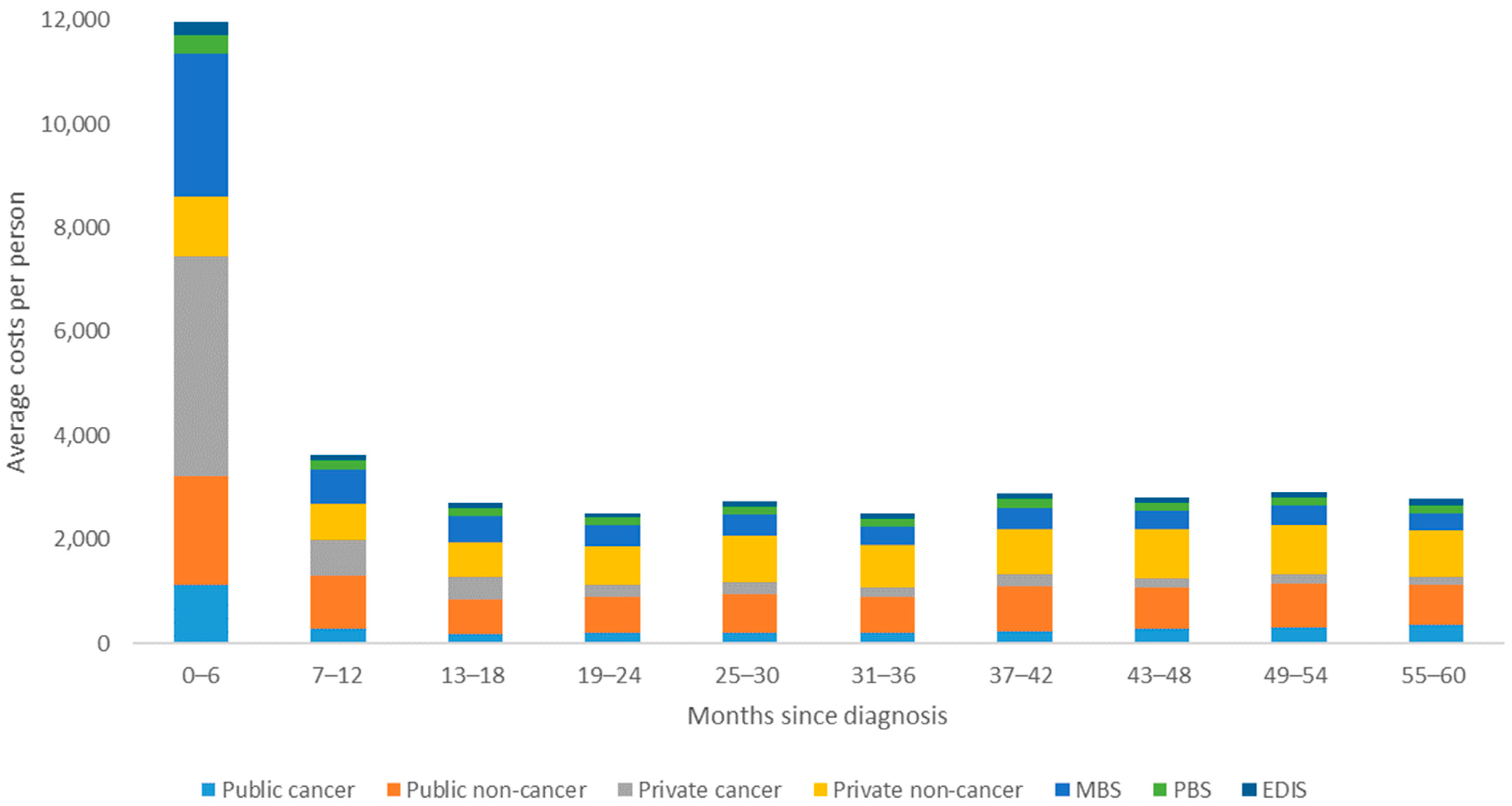
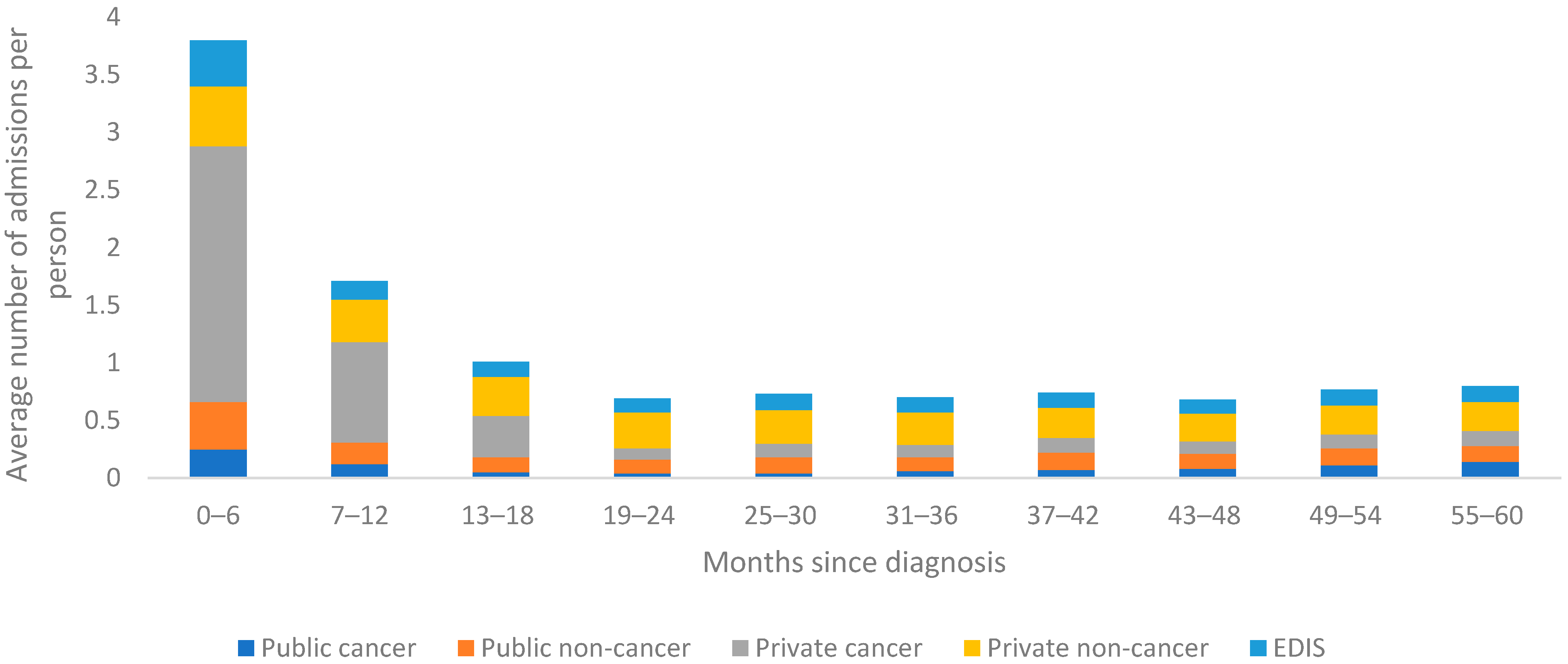
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Institute of Health and Welfare (AIHW). Cancer in Australia 2017; Cancer Series no 101 Cat no CAN 100; AIHW: Canberra, Australia, 2017.
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare (AIHW). Cancer Data in Australia; AIHW: Canberra, Australia, 2020. Available online: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia/ (accessed on 15 October 2021).
- Smith, T.; Hillner, B.E. Bending the Cost Curve in Cancer Care. N. Engl. J. Med. 2011, 364, 2060–2065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karikios, D.J.; Schofield, D.; Salkeld, G.; Mann, K.P.; Trotman, J.; Stockler, M.R. Rising cost of anticancer drugs in Australia. Intern. Med. J. 2014, 44, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare (AIHW). Hospital Resources 2017–2018: Australian Hospital Statistics; Cat no HSE 233; AIHW: Canberra, Australia, 2019.
- Australian Government. Medicare Levy Reduction for Low-Income Earners. Australian Taxation Office. Medicare Levy Web site. 2017. Available online: https://www.ato.gov.au/individuals/medicare-levy/medicare-levyreduction-for-low-income-earners/ (accessed on 13 October 2021).
- Department of Human Services. Australian Government rebate on Private Health Insurance. Australian Government. 2019. Available online: https://www.humanservices.gov.au/individuals/services/medicare/australiangovernment-rebate-private-health-insurance#a2 (accessed on 9 September 2021).
- Callander, E.; Shand, A.; Ellwood, D.; Fox, H.; Nassar, N. Financing Maternity and Early Childhood Healthcare in The Australian Healthcare System: Costs to Funders in Private and Public Hospitals Over the First 1000 Days. Int. J. Heal. Policy Manag. 2020, 2021, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare (AIHW). Health System Expenditure on Cancer and Other Neoplasms in Australia, 2015–2016; Cancer Series No. 131 Cat No 142; AIHW: Canberra, Australia, 2021.
- Park, J.; Look, K.A. Health Care Expenditure Burden of Cancer Care in the United States. Inq. J. Heal. Care Organ. Provis. Financ. 2019, 56, 0046958019880696. [Google Scholar] [CrossRef] [PubMed]
- Zaorsky, N.G.; Khunsriraksakul, C.; Acri, S.L.; Liu, D.J.; Ba, D.M.; Lin, J.L.; Liu, G.; Segel, J.E.; Drabick, J.J.; Mackley, H.B.; et al. Medical Service Use and Charges for Cancer Care in 2018 for Privately Insured Patients Younger Than 65 Years in the US. JAMA Netw. Open 2021, 4, e2127784. [Google Scholar] [CrossRef] [PubMed]
- Goldsbury, D.E.; Yap, S.; Weber, M.F.; Veerman, L.; Rankin, N.; Banks, E.; Canfell, K.; O’Connell, D.L. Health services costs for cancer care in Australia: Estimates from the 45 and up Study. PLoS ONE 2018, 13, e0201552. [Google Scholar] [CrossRef]
- Livingston, P.M.; Craike, M.; Considine, J. Unplanned presentations to emergency departments due to chemotherapy induced complications: Opportunities for improving service delivery. Australas. Emerg. Nurs. J. 2011, 14, 62–68. [Google Scholar] [CrossRef]
- Deloitte Access Economics. Financial Impacts of Breast Cancer in Australia: Breast Cancer Network Australia; Deloitte Access Economics: Canberra, Australia, 2017. [Google Scholar]
- Gordon, L.G.; Elliott, T.M.; Olsen, C.M.; Pandeya, N.; Whiteman, D.C. Out-of-pocket medical expenses for Queenslanders with a major cancer. Med. J. Aust. 2018, 208, 497. [Google Scholar] [CrossRef] [PubMed]
- Bates, N.; Callander, E.; Lindsay, D.; Watt, K. Patient co-payments for women diagnosed with breast cancer in Australia. Support. Care Cancer 2020, 28, 2217–2227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagsi, R.; Pottow, J.A.; Griffith, K.A.; Bradley, C.; Hamilton, A.S.; Graff, J.; Katz, S.J.; Hawley, S.T. Long-Term Financial Burden of Breast Cancer: Experiences of a Diverse Cohort of Survivors Identified Through Population-Based Registries. J. Clin. Oncol. 2014, 32, 1269–1276. [Google Scholar] [CrossRef] [Green Version]
- Callander, E.; Topp, S.M.; Larkins, S.; Sabesan, S.; Bates, N. Quantifying Queensland patients with cancer health service usage and costs: Study protocol. BMJ Open 2017, 7, e014030. [Google Scholar] [CrossRef] [PubMed]
- Bates, N.; Callander, E.; Lindsay, D.; Watt, K. CancerCostMod: A model of the healthcare expenditure, patient resource use, and patient co-payment costs for Australian cancer patients. Heal. Econ. Rev. 2018, 8, 1–12. [Google Scholar] [CrossRef]
- Youlden, D.R.; Cramb, S.M.; Baade, P. Current Status of Female Breast Cancer in Queensland: 1982 to 2006; Viertel Centre for Research in Cancer Control, Cancer Council Queensland: Brisbane, Australia, 2009. [Google Scholar]
- Baade, P.D.; Turrell, G.; Aitken, J.F. Geographic remoteness, area-level socio-economic disadvantage and advanced breast cancer: A cross-sectional, multilevel study. J. Epidemiol. Community Heal. 2011, 65, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Independent Hospital Pricing Authority (IHPA). National Hospital Cost Data Collection (NHCDC) Darlinghurst Independent Hospital Pricing Authority. Available online: https://www.ihpa.gov.au/what-we-do/nhcdc (accessed on 22 August 2021).
- Independent Hospital Pricing Authority (IHPA). National Efficient Price Determination Darlinghurst Independent Hospital Pricing Authority. Available online: https://www.ihpa.gov.au/what-we-do/national-efficient-price-determination (accessed on 22 August 2021).
- Australian Government Department of Health. Archived Private Hospital Data Bureau (PHDB) Annual Reports Canberra: Commonwealth of Australia. 2017. Available online: http://health.gov.au/internet/main/publishing.nsf/Content/health-casemix-data-collections-publications-PHDBAnnualReportsArchived (accessed on 22 August 2021).
- Reserve Bank of Australia. Inflation Calculator Sydney, Australia: Reserve Bank of Australia. 2021. Available online: http://www.rba.gov.au/calculator/ (accessed on 23 August 2021).
- Francisci, S.; Guzzinati, S.; Capodaglio, G.; Pierannunzio, D.; Mallone, S.; Tavilla, A.; Lopez, T.; Busco, S.; Mazzucco, W.; Angiolini, C.; et al. Patterns of care and cost profiles of women with breast cancer in Italy: EPICOST study based on real world data. Eur. J. Health Econ. 2020, 21, 1003–1013. [Google Scholar] [CrossRef]
- Prang, K.-H.; Canaway, R.; Bismark, M.; Dunt, D.; Miller, J.A.; Kelaher, M. Public performance reporting and hospital choice: A cross-sectional study of patients undergoing cancer surgery in the Australian private healthcare sector. BMJ Open 2018, 8, e020644. [Google Scholar] [CrossRef]
- Dasgupta, P.; Youl, P.H.; Pyke, C.; Aitken, J.F.; Baade, P.D. Geographical disparity in breast reconstruction following mastectomy has reduced over time. ANZ J. Surg. 2016, 87, E183–E187. [Google Scholar] [CrossRef]
- AIHW. MyHospitals. 2017. Available online: http://www.myhospitals.gov.au/ (accessed on 29 September 2021).
- Cheng, T.C.; de New, J.; Yong, J. Cream skimming and hospital transfers in a mixed public-private system. Soc. Sci. Med. 2015, 132, 156–164. [Google Scholar] [CrossRef]
- Youl, P.; Philpot, S.; Moore, J.; Theile, D.E. Population-based picture of breast reconstruction in Queensland, Australia. ANZ J. Surg. 2021, 91, 695–700. [Google Scholar] [CrossRef]
- Schultz, P.N.; Beck, M.L.; Stava, C.; Vassilopoulou-Sellin, R. Health profiles in 5836 long-term cancer survivors. Int. J. Cancer 2003, 104, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.A.; Kwan, L.; Stanton, A.L.; Bower, J.E.; Belin, T.R. Physical and Psychosocial Recovery in the Year After Primary Treatment of Breast Cancer. J. Clin. Oncol. 2011, 29, 1101–1109. [Google Scholar] [CrossRef] [PubMed]
- Porter-Steele, J.; Tjondronegoro, D.; Seib, C.; Young, L.; Anderson, D. ‘Not one size fits all’: A brief review of models of care for women with breast cancer in Australia. Cancer Forum. 2017, 41, 13–19. [Google Scholar]
- Ward, R.L.; Laaksonen, A.M.; Van Gool, K.; Pearson, S.-A.; Daniels, B.; Bastick, P.; Norman, R.; Hou, C.; Haywood, P.; Haas, M. Cost of cancer care for patients undergoing chemotherapy: The Elements of Cancer Care study. Asia-Pac. J. Clin. Oncol. 2015, 11, 178–186. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Age group | |
| 18–44 years | 1247 (23.2) |
| 45–64 years | 2184 (40.6) |
| 65 years and above | 1952 (36.2) |
| Indigenous status | |
| Indigenous women | 83 (1.5) |
| Remoteness | |
| Metropolitan | 2675 (49.9) |
| Regional | 2278 (42.4) |
| Remote | 411 (7.7) |
| Index of Relative Socio-Economic Disadvantage | |
| Quintile 1 (most disadvantaged) | 361 (6.7) |
| Quintile 2 | 225 (4.2) |
| Quintile 3 | 907 (16.9) |
| Quintile 4 | 2434 (45.4) |
| Quintile 5 (least disadvantaged) | 1437 (26.8) |
| Breast cancer stage | |
| Early | 2468 (46) |
| Regional/advanced | 2439 (45) |
| Unknown | 476 (9) |
| Healthcare Type | Cost Type | Mean (SD) Cost Per Person | Sum Cost Over 5 Years |
|---|---|---|---|
| Public hospitals | Cancer related costs | $3349 (10,599) | $18,029,931 |
| Non-cancer related costs | $9174 (25,381) | $49,381,115 | |
| Total cost | $12,523 (29,726) | $67,411,046 | |
| Private hospitals | Cancer related costs | $6772 ($11,103) | $36,453,528 |
| Non-cancer related costs | $8555 ($25,001) | $46,049,002 | |
| Total cost | $15,327 ($29,538) | $82,502,530 | |
| Emergency departments | $1132 (2306) | $6,091,598 | |
| Medicare Benefits Schedule | $6578 ($7248) | $35,407,985 | |
| Pharmaceutical Benefits Scheme | $1836 (1489) | $9,885,472 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindsay, D.; Callander, E. Quantifying the Costs to Different Funders over Five-Years for Women Diagnosed with Breast Cancer in Queensland, Australia: A Data Linkage Study. Int. J. Environ. Res. Public Health 2021, 18, 12918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412918
Lindsay D, Callander E. Quantifying the Costs to Different Funders over Five-Years for Women Diagnosed with Breast Cancer in Queensland, Australia: A Data Linkage Study. International Journal of Environmental Research and Public Health. 2021; 18(24):12918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412918
Chicago/Turabian StyleLindsay, Daniel, and Emily Callander. 2021. "Quantifying the Costs to Different Funders over Five-Years for Women Diagnosed with Breast Cancer in Queensland, Australia: A Data Linkage Study" International Journal of Environmental Research and Public Health 18, no. 24: 12918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412918