
Recovery Capital among Migrants and Ethnic Minorities in Recovery from Problem Substance Use: An Analysis of Lived Experiences


Abstract
:1. Introduction
2. Materials and Methods
3. Results
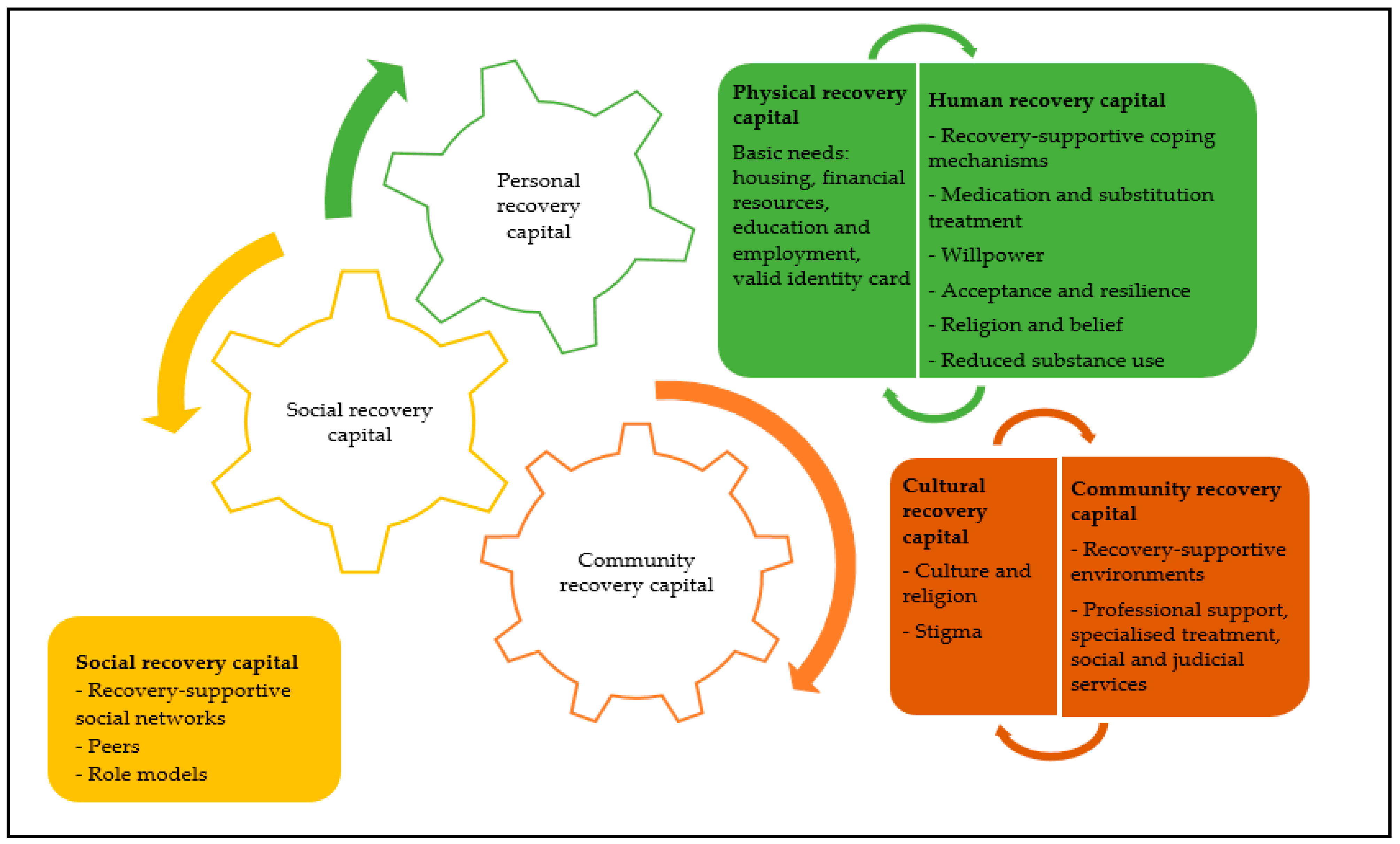
3.1. Personal Recovery Capital
3.1.1. Physical Recovery Capital
(Those) Who are homeless people, who sleep on the street, that’s why they use everything. (…) That’s why he does bad things. But if somebody helped these people, I think maybe he changes his life. (…) You know why I know? Because I was on the street here.(Tomáš, 31 years old, #27)
What’s the problem? Drugs are the problem. Let’s work on that drug problem, but that doesn’t work out because you don’t have the papers.(Amir, 39 years old, #22)
3.1.2. Human Recovery Capital
Recovery-Supportive Coping Mechanisms
You don’t feel well and then you start using to suppress your emotions. (…) I had built up walls about my past, I didn’t dare to speak about my emotions. (…) To be clean, you have to handle your problems. You have to go back to the past, where it all went wrong.(Abdel, 47 years old, #17)
Medication and Substitution Treatment
Better I drink methadone, I don’t use that shit (heroin), and I’m good. My body is good, I don’t think bad things in my mind. I relax. I take the medication. I’m happy. (…) Of course. I don’t want to drink the medication all my life. I want to stop, but slowly. (…) Methadone is okay, it helps you, but the methadone is the same like drugs, no? It kills you like drugs.(Tomáš, 31 years old, #27)
Willpower: From Necessity to Intrinsic Motivation
I have to keep gritting my teeth. The internal fight saying: no, no, no. That demands a lot of willpower.(Abbas, 37 years old, #3)
This is not my life, you know my point… (…) It is no good to steal. I like to build my life, live here, have a family. I lost too much. (…) I like being again who I have been before.(Michal, 26 years old, #25)
Acceptance and Resilience
That’s the life that I was given and it’s fucked up, but I try to make the best of it. I try to see everything positive and I know, it’s full of discrimination, racism, dishonesty, but that’s life.(Amir, 39 years old, #22)
Religion and Belief
One day I told myself: now it’s enough. I’ll take the Bible, go to church, light some candles. The book of Jesus will help me. And that’s how I lost everything (referring to substance use), little by little. Somebody asks me, you want a drag? I say no, I take the book and I read. I have to get stronger. I’m a good Catholic.(Miroslav, 30 years old, #16)
Reduced Substance Use
The longer you are sober, the stronger you are against the craving. So, sobriety is a helping element for recovery.(Amina, 38 years old, #24)
3.2. Social Recovery Capital
The support of others means a lot. We are so used of doing it alone, but eventually you won’t do it alone. I won’t. I couldn’t get rid of my addiction alone.(Enzo, 27 years old, #14)
That friend who took me to X (substance use treatment center) yesterday. He has the same problem as me. (…) He is actually my biggest support figure. He motivates me to go to the mosque. He tells me to stop taking heroin and stuff.(Kerem, 26 years old, #10)
3.3. Community Recovery Capital
3.3.1. Recovery-Supportive Environments
It is difficult to stop using drugs in Belgium, because you have it everywhere. And almost all your friends are on drugs. (…) In Turkey, we live in a village with 10,000 inhabitants and there are no dealers there. So if you want to smoke weed, for example, you have to drive 100 km by car. If you want to smoke heroin, you have to drive 150 km. That’s how I was able to stop.(Kerem, 26 years old, #10)
I missed everything at home. It was hard to leave everything behind, no contact with the outside world, it’s not easy. After that (admission in a therapeutic community), I was clean for a few months, but you go back to where it all started. If you put that person back in the place where he comes from, where all his user friends are, the chance for relapse is a lot bigger then when he starts over somewhere else.(Adil, 37 years old, #3)
3.3.2. Professional Support
From complete safety and follow-up to no safety at all and no follow-up, it is sometimes very difficult. (…) You overestimate yourself. (…) But you do not take into account or you do not realize that it actually happened in a safe environment and that you should not compare that with reality.(Muhammed, 32 years old, #31)
I was in prison for three years. I was clean, but I never worked on myself, on my personality. You talk about your case and about what you did, but you don’t talk about what you want in life.(Abbad, 47 years old, #18)
I was in prison for thirteen months, where I was clean. And then through (social service of prison) I got in contact with a center for mental health. I saw it (prison) as an opportunity to become clean, because I thought, I can’t get this shit here. (…) It was Ramadan also, so that was an extra opportunity to quit. But it was not easy, because unfortunately, it ((drugs) is offered a lot in prison.(Muhammed, 32 years old, #31)
3.3.3. Cultural Recovery Capital
Belief, culture, maintaining my values and norms, that is an important anchor in my recovery.(Hamid, 31 years old, #28)
People look at you askew. I’m brown, that’s one thing, and then I smoke too, that’s not good huh.(Murat, 35 years old, #34)
4. Discussion
4.1. Recovery Capital and Barriers Experienced by MEM
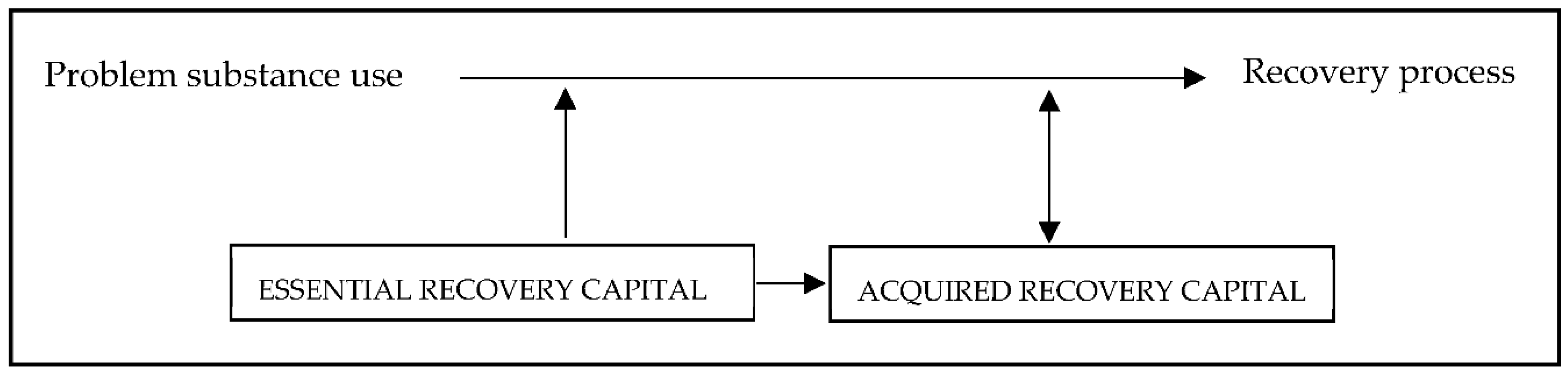
4.2. The Interwovenness of Different Forms of Recovery Capital
4.3. Limitations and Further Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Kock, C.; Decorte, T.; Vanderplasschen, W.; Derluyn, I.; Sacco, M. Studying ethnicity, problem substance use and treatment: From epidemiology to social change. Drugs Educ. Prev. Policy 2017, 24, 230–239. [Google Scholar] [CrossRef]
- Vertovec, S. Super-diversity and its implications. Ethn. Racial Stud. 2007, 30, 1024–1054. [Google Scholar] [CrossRef]
- Alegria, M.; Carson, N.J.; Goncalves, M.; Keefe, K. Disparities in treatment for substance use disorders and co-occurring disorders for ethnic/racial minority youth. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Savage, J.E.; Mezuk, B. Psychosocial and contextual determinants of alcohol and drug use disorders in the National Latino and Asian American Study. Drug Alcohol Depend. 2014, 139, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caetano, R.; Clark, C.L.; Tam, T. Alcohol consumption among racial/ethnic minorities: Theory and research. Alcohol Health Res. World 1998, 22, 233–241. [Google Scholar]
- Szaflarski, M.; Cubbins, L.A.; Ying, J. Epidemiology of alcohol abuse among US immigrant populations. J. Immigr. Minority Health 2011, 13, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Pouille, A.; De Kock, C.; Vander Laenen, F.; Vanderplasschen, W. Recovery capital among migrants and ethnic minorities: A qualitative systematic review of first-person perspectives. J. Ethn. Subst. Abuse 2020, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Alegría, M.; Pescosolido, B.A.; Williams, S.; Canino, G. Culture, Race/Ethnicity and Disparities: Fleshing Out the Socio-Cultural Framework for Health Services Disparities. In Handbook of the Sociology of Health, Illness, and Healing: A Blueprint for the 21st Century; Pescosolido, B.A., Martin, J.K., McLeod, J.D., Rogers, A., Eds.; Springer: New York, NY, USA, 2011; pp. 363–382. [Google Scholar]
- Cloud, W.; Granfield, R. Conceptualizing Recovery Capital: Expansion of a Theoretical Construct. Subst. Use Misuse 2008, 43, 1971–1986. [Google Scholar] [CrossRef]
- Fomiatti, R.; Moore, D.; Fraser, S. The improvable self: Enacting model citizenship and sociality in research on ‘new recovery’. Addict. Res. Theory 2018, 27, 527–538. [Google Scholar] [CrossRef]
- White, W.; Cloud, W. Recovery capital: A primer for addictions professionals. Counselor 2008, 9, 22–27. [Google Scholar]
- Laudet, A.B.; White, W.L. Recovery capital as prospective predictor of sustained recovery, life satisfaction, and stress among former poly-substance users. Subst. Use Misuse 2008, 43, 27–54. [Google Scholar] [CrossRef] [Green Version]
- Hewitt, A.J. After the Fire: Post Traumatic Growth in Recovery from Addictions. Ph.D. Thesis, University of Bath, Bath, UK, 2007. [Google Scholar]
- Harper, D.; Speed, E. Uncovering Recovery: The Resistible Rise of Recovery and Resilience. Stud. Soc. Justice 2012, 6, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Klevan, T.; Bank, R.-M.; Borg, M.; Karlsson, B.; Krane, V.; Ogundipe, E.; Semb, R.; Sommer, M.; Sundet, R.; Sælør, K.T.; et al. Part I: Dynamics of Recovery: A Meta-Synthesis Exploring the Nature of Mental Health and Substance Abuse Recovery. Int. J. Environ. Res. Public Health 2021, 18, 7761. [Google Scholar] [CrossRef]
- Bellaert, L.; Martinelli, T.; Vanderplasschen, W.; Best, D.; Mheen, D.; Laenen, F. Chasing a pot of gold: An analysis of emerging recovery-oriented addiction policies in Flanders (Belgium) and The Netherlands. Drugs Educ. Prev. Pol. 2021, 28, 399–410. [Google Scholar] [CrossRef]
- Best, D.; Laudet, A.B. The Potential of Recovery Capital; Royal Society for the Arts, RSA: London, UK, 2010. [Google Scholar]
- Best, D.; Vanderplasschen, W.; Van de Mheen, D.; De Maeyer, J.; Colman, C.; Vander Laenen, F.; Irving, J.; Andersson, C.; Edwards, M.; Bellaert, L.; et al. REC-PATH (Recovery Pathways): Overview of a Four-Country Study of Pathways to Recovery from Problematic Drug Use. Alcohol Treat. Q. 2018, 36, 517–529. [Google Scholar] [CrossRef] [Green Version]
- Onken, S.; Dumont, J.; Ridgway, P.; Dornan, D.; Ralph, R. Mental Health Recovery: What Helps and What Hinders? A National Research Project for the Development of Recovery Facilitating System Performance Indicators Phase One Research Report: A National Study of Consumer Perspectives on What Helps and Hinders Recovery; National Association of State Mental Health Program Directors (NASMHPD) National Technical Assistance Center (NTAC): Alexandria, VA, USA, 2002. [Google Scholar]
- Skogens, L.; von Greiff, N. Recovery capital in the process of change—differences and similarities between groups of clients treated for alcohol or drug problems. Eur. J. Soc. Work 2014, 17, 58–73. [Google Scholar] [CrossRef]
- Fiscella, K.; Franks, P.; Gold, M.R.; Clancy, C.M. Inequality in Quality Addressing Socioeconomic, Racial, and Ethnic Disparities in Health Care. JAMA 2000, 283, 2579–2584. [Google Scholar] [CrossRef]
- Stuart, S.R.; Tansey, L.; Quayle, E. What we talk about when we talk about recovery: A systematic review and best-fit framework synthesis of qualitative literature. J. Ment. Health 2017, 26, 291–304. [Google Scholar] [CrossRef]
- Noppe, J.; Vanweddingen, M.; Doyen, G.; Stuyck, K.; Feys, Y.; Buysschaert, P. Vlaamse Migratie—En Integratiemonitor; Agentschap Binnenlands Bestuur: Brussels, Belgium, 2018. [Google Scholar]
- Mehdiyar, M.; Andersson, R.; Hjelm, K. HIV-positive migrants’ experience of living in Sweden. Glob. Health Action 2020, 13, 1715324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benoit, C.; Jansson, M.; Millar, A.; Phillips, R. Community-academic research on hard-to-reach populations: Benefits and challenges. Qual. Health Res. 2005, 15, 263–282. [Google Scholar] [CrossRef]
- Alvarez, R.A.; Vasquez, E.; Mayorga, C.C.; Feaster, D.J.; Mitrani, V.B. Increasing minority research participation through community organization outreach. West. J. Nurs. Res. 2006, 28, 541–560. [Google Scholar] [CrossRef] [Green Version]
- Muhib, F.B.; Lin, L.S.; Stueve, A.; Miller, R.L.; Ford, W.L.; Johnson, W.D.; Smith, P.J. A venue-based method for sampling hard-to-reach populations. Public Health Rep. 2001, 116 (Suppl. 1), 216–222. [Google Scholar] [CrossRef] [Green Version]
- Calsyn, R.J.; Klinkenberg, W.D.; Morse, G.A.; Miller, J.; Cruthis, R. Recruitment, engagement, and retention of people living with HIV and co-occurring mental health and substance use disorders. AIDS Care 2004, 16 (Suppl. 1), S56–S70. [Google Scholar] [CrossRef]
- Guest, G.; Bunce, A.; Johnson, L. How Many Interviews Are Enough? Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Hennessy, E.A. Recovery capital: A systematic review of the literature. Addict. Res. Theory 2017, 25, 349–360. [Google Scholar] [CrossRef]
- Hong, H.C.; Min, A.; Choi, S. Living with the Late Effects of Childhood Cancer Treatment: A Descriptive Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 8392. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Best, D.; Lubman, D.I. The recovery paradigm, a model of hope and change for alcohol and drug addiction. Aust. Fam. Physician 2012, 41, 593–597. [Google Scholar] [PubMed]
- Irish, A.; Bowen, E.A.; Hawthorne, A.N.; Palombi, L. “Me, the street, and a backpack”: Employment, income, and physical capital in rural recovery. J. Soc. Work Pract. Addict. 2020, 20, 194–207. [Google Scholar] [CrossRef]
- Gainsbury, S.M. Cultural Competence in the Treatment of Addictions: Theory, Practice and Evidence. Clin. Psychol. Psychother. 2017, 24, 987–1001. [Google Scholar] [CrossRef] [PubMed]
- De Kock, C.; Blomme, E.; Antoine, J. Non-national clients in Belgian substance use treatment. Drugs Alcohol Today 2020. ahead-of-print. [Google Scholar] [CrossRef]
- Burgess, D.J.; Ding, Y.; Hargreaves, M.; van Ryn, M.; Phelan, S. The association between perceived discrimination and underutilization of needed medical and mental health care in a multi-ethnic community sample. J. Health Care Poor Underserved 2008, 19, 894–911. [Google Scholar] [CrossRef]
- Du Plessis, G. The integrated recovery model for addiction treatment and recovery. J. Integral Theory Pract. 2010, 5, 68–87. [Google Scholar]
- Vandevelde, S.; Vanderplasschen, W.; Broekaert, E. Cultural responsiveness in SAT: A qualitative study using professionals and clients’ perspectives. Int. J. Soc. Welf. 2003, 12, 221–228. [Google Scholar] [CrossRef]
- Giacco, D.; Matanov, A.; Priebe, S. Providing mental healthcare to immigrants. Curr. Opin. Psychiatry 2014, 27, 282–288. [Google Scholar] [CrossRef] [Green Version]
- Straussner, S.L.A. Ethnocultural Issues in substance abuse treatment: An overview. In Ethnocultural Factors in Substance Abuse Treatment; Straussner, S.L.A., Ed.; Guilford Press: New York, NY, USA, 2001; pp. 3–28. [Google Scholar]
- Whitley, R. “Thank you God”: Religion and recovery from dual diagnosis among low-income African Americans. Transcult. Psychiatry 2012, 49, 87–104. [Google Scholar] [CrossRef]
- Leamy, M.; Bird, V.; Boutillier, C.L.; Williams, J.; Slade, M. Conceptual framework for personal recovery in mental health: Systematic review and narrative synthesis. Br. J. Psychiatry 2011, 199, 445–452. [Google Scholar] [CrossRef] [Green Version]
- Beraldo, L.; Gil, F.; Ventriglio, A.; de Andrade, A.G.; da Silva, A.G.; Torales, J.; Gonçalves, P.D.; Bhugra, D.; Castaldelli-Maia, J.M. Spirituality, religiosity and addiction recovery: Current perspectives. Curr. Drug Res. Rev. 2019, 11, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Roystonn, K.; Cetty, L.; Jeyagurunathan, A.; Devi, F.; Abdin, E.; Tan, S.T.; Tang, C.; Verma, S.; Subramaniam, M. Quality of Life and Its Associations with Religiosity and Religious Coping among Outpatients with Psychosis in Singapore. Int. J. Environ. Res. Public Health 2021, 18, 7200. [Google Scholar] [CrossRef]
- Cheney, A.M.; Booth, B.M.; Borders, T.F.; Curran, G.M. The Role of Social Capital in African Americans’ Attempts to Reduce and Quit Cocaine Use. Subst. Use Misuse 2016, 51, 777–787. [Google Scholar] [CrossRef]
- Malinakova, K.; Tavel, P.; Meier, Z.; van Dijk, J.P.; Reijneveld, S.A. Religiosity and Mental Health: A Contribution to Understanding the Heterogeneity of Research Findings. Int. J. Environ. Res. Public Health 2020, 17, 494. [Google Scholar] [CrossRef] [Green Version]
- Dekkers, A.; De Ruysscher, C.; Vanderplasschen, W. Perspectives of cocaine users on addiction recovery: A qualitative study following a CRA + vouchers programme. Drugs Educ. Prev. Policy 2020, 27, 282–296. [Google Scholar] [CrossRef]
- Best, D.; Beckwith, M.; Haslam, C.; Alexander Haslam, S.; Jetten, J.; Mawson, E.; Lubman, D.I. Overcoming alcohol and other drug addiction as a process of social identity transition: The social identity model of recovery (SIMOR). Addict. Res. Theory 2016, 24, 111–123. [Google Scholar] [CrossRef]
- Moran, G.; Russo-Netzer, P. Understanding Universal Elements in Mental Health Recovery: A Cross-Examination of Peer Providers and a Non-Clinical Sample. Qual. Health Res. 2015, 26, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Van Steenberghe, T.; Vanderplasschen, W.; Bellaert, L.; De Maeyer, J. Photovoicing interconnected sources of recovery capital of women with a drug use history. Drugs Educ. Prev. Policy 2021, 28, 411–425. [Google Scholar] [CrossRef]
- Rudzinski, K.; McDonough, P.; Gartner, R.; Strike, C. Is there room for resilience? A scoping review and critique of substance use literature and its utilization of the concept of resilience. Subst. Abuse Treat. Prev. Policy 2017, 12, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anthony, W.A. Recovery from mental illness: The guiding vision of the mental health service system in the 1990′s. Psychosoc. Rehabil. J. 1993, 16, 11–23. [Google Scholar] [CrossRef]
- Donovan, D.M.; Ingalsbe, M.H.; Benbow, J.; Daley, D.C. 12-Step Interventions and Mutual Support Programs for Substance Use Disorders: An Overview. Soc. Work. Public Health 2013, 28, 313–332. [Google Scholar] [CrossRef] [PubMed]
- Zemore, S.E.; Gilbert, P.A.; Pinedo, M.; Tsutsumi, S.; McGeough, B.; Dickerson, D.L. Racial/Ethnic Disparities in Mutual Help Group Participation for Substance Use Problems. Alcohol Res. 2021, 41, 3. [Google Scholar] [CrossRef] [PubMed]
- McCarron, H.; Griese, E.R.; Dippel, E.; McMahon, T.R. Cultural and Social Predictors of Substance Abuse Recovery among American Indian and Non-American Indian Pregnant and Parenting Women. J. Psychoact. Drugs 2018, 50, 322–330. [Google Scholar] [CrossRef]
- Brown, S.; Tracy, E.M.; Jun, M.; Park, H.; Min, M.O. Personal Network Recovery Enablers and Relapse Risks for Women with Substance Dependence. Qual. Health Res. 2014, 25, 371–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price-Robertson, R.; Obradovic, A.; Morgan, B. Relational recovery: Beyond individualism in the recovery approach. Adv. Ment. Health 2017, 15, 108–120. [Google Scholar] [CrossRef]
- Neale, J.; Stevenson, C. Social and recovery capital amongst homeless hostel residents who use drugs and alcohol. Int. J. Drug Policy 2015, 26, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tortelli, A.; Sauze, D.; Skurnik, N. Social capital, mental health and migration. Ann. Med. Psychol. 2017, 175, 573–576. [Google Scholar] [CrossRef]
- Duff, C. Exploring the role of ‘enabling places’ in promoting recovery from mental illness: A qualitative test of a relational model. Health Place 2012, 18, 1388–1395. [Google Scholar] [CrossRef]
- Vanderplasschen, W.; Rapp, R.C.; Wolf, J.R.; Broekaert, E. The development and implementation of case management for substance use disorders in North America and Europe. Psychiatr. Serv. 2004, 55, 913–922. [Google Scholar] [CrossRef]
- De Kock, C.; Mascia, C.; Laudens, F.; Toyinbo, L.; Leclerq, S.; Hensgens, P.; Jacobs, D.; Decorte, T. Mapping & Enhancing Substance Use Treatment for Migrants and Ethinc Minorities. Final Report; Belgian Science Policy Office: Brussels, Belgium, 2020. [Google Scholar]
- Room, R. Stigma, social inequality and alcohol and drug use. Drug Alcohol Rev. 2005, 24, 143–155. [Google Scholar] [CrossRef]
- Beyers, J. Religion and culture: Revisiting a close relative. HTS Theol. Stud. 2017, 73, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Best, D.; Day, E.; McCarthy, T.; Darlington, I.; Pinchbeck, K. The Hierarchy of Needs and care planning in addiction services: What Maslow can tell us about addressing competing priorities? Addict. Res. Theory 2008, 16, 305–307. [Google Scholar] [CrossRef]
- Savic, M.; Bathish, R. Rethinking agency, strengths and change in desistance and recovery In Strengths-Based Approaches to Crime and Substance Use; Best, D., Colman, C., Eds.; Routledge: London, UK, 2019; pp. 105–122. [Google Scholar]
- Ashford, R.; Brown, A.; Ryding, R.; Curtis, B. Building Recovery Ready Communities: The Recovery Ready Ecosystem Model and Community Framework. Addict. Res. Theory 2020, 28, 1–11. [Google Scholar] [CrossRef]
- De Ruysscher, C.; Tomlinson, P.; Vanheule, S.; Vandevelde, S. Questioning the professionalization of recovery: A collaborative exploration of a recovery process. Disabil. Soc. 2019, 34, 797–818. [Google Scholar] [CrossRef]
- Robinson, O.C. Sampling in Interview-Based Qualitative Research: A Theoretical and Practical Guide. Qual. Res. Psychol. 2014, 11, 25–41. [Google Scholar] [CrossRef]
- Bergen, N.; Labonté, R. “Everything Is Perfect, and We Have No Problems”: Detecting and Limiting Social Desirability Bias in Qualitative Research. Qual. Health Res. 2019, 30, 783–792. [Google Scholar] [CrossRef]
- Hunter, S.V. Analysing and representing narrative data: The long and winding road. Curr. Narrat. 2010, 1, 44–54. [Google Scholar]
- De Kock, C.; Decorte, T. Exploring problem use, discrimination, ethnic identity and social networks. Drugs Alcohol Today 2017, 17, 269–279. [Google Scholar] [CrossRef]
- De Kock, C. Cultural competence and derivatives in substance use treatment for migrants and ethnic minorities: What’s the problem represented to be? Soc. Theor. Health 2020, 18, 358–394. [Google Scholar] [CrossRef]
- Slade, M. Everyday solutions for everyday problems: How mental health systems can support recovery. Psychiatr. Serv. 2012, 63, 702–704. [Google Scholar] [CrossRef] [Green Version]
- Hanauer, M.; Sielbeck-Mathes, K.; Berny, L. Invariance of a recovery capital scale across gender, ethnicity, and sexual orientation in a substance use disorder treatment program. Am. J. Drug Alcohol Abuse 2019, 45, 254–263. [Google Scholar] [CrossRef] [PubMed]
- De Kock, C. Risk factors and dangerous classes in a European context: The consequences of ethnic framing of and among Turkish drug users in Ghent, Belgium. In Risk and Substance Use; MacGregor, S., Thom, B., Eds.; Routledge: London, UK, 2020. [Google Scholar]



{kind=link}
{kind=link}
| Nr. of Respondent (Indicated by # in Text) | Country of Origin | Gender | Age | 1st-, 2nd- or 3rd-Generation MEM (Age at Immigration) | Self-Identified Problem Substance (s) | Current Self-Identified Substance Use |
|---|---|---|---|---|---|---|
| 1 | Haïti | F | 36 | 1st (4) | Cannabis Cocaine | Sporadic cocaine use |
| 2 | Slovakia | M | 32 | 1st (26) | Alcohol | None |
| 3 | Morocco | M | 37 | 2nd | Cocaine | None |
| 4 | Algeria | M | 43 | 2nd | Heroin (Methadone) | Controlled methadone use |
| 5 | Morocco | M | 41 | 1st (23) | Alcohol Cocaine | None |
| 6 | Burundi | M | 29 | 1st (4) | Alcohol Cannabis Cocaine | None |
| 7 | Turkey | M | 40 | 2nd | MDMA Cocaine | Sporadic cocaine use |
| 8 | Russia | M | 33 | 1st (16) | Alcohol Heroin (Methadone) | Non-problematic alcohol use Controlled methadone use |
| 9 | Italy | M | 51 | 1st (11) | Heroin (Methadone) | Controlled methadone use |
| 10 | Turkey | M | 26 | 2nd | Alcohol Cannabis Heroin Benzodiazepines (Methadone) (Suboxone) | Sporadic cannabis use Regular poly-substance use |
| 11 | Algeria | M | 38 | 2nd | Amphetamines Cocaine Heroin | None |
| 12 | England | M | 53 | 1st (27) | Alcohol Cannabis | Controlled cannabis use |
| 13 | Rwanda | M | 25 | 1st (4) | Alcohol Cannabis | None |
| 14 | Switzerland/Italy | M | 27 | 2nd | Cannabis Benzodiazepines Amphetamines Cocaine | None |
| 15 | Morocco | F | 44 | 2nd | Heroin (Methadone) | Sporadic heroin use Controlled methadone use |
| 16 | Slovakia | M | 30 | 1st (9) | Heroin (Methadone) | Controlled methadone use |
| 17 | Morocco | M | 47 | 2nd | Cocaine | None |
| 18 | Turkey | M | 41 | 2nd | Amphetamines | None |
| 19 | Morocco | M | 39 | 2nd | Cannabis Alcohol Cocaine | None |
| 20 | Belgium/Algeria | M | 33 | 2nd | Alcohol Speed GHB | None |
| 21 | Turkey | M | 50 | 1st (7) | Heroin (Methadone) | Controlled heroin and methadone use |
| 22 | Morocco | M | 39 | 2nd | Cocaine | None |
| 23 | Belgium/Algeria | F | 60 | 2nd | Cocaine Heroïne (Methadone) | None |
| 24 | Belgium/Morocco | F | 38 | 2nd | Cocaïne Benzodiazepines | None |
| 25 | Slovakia | M | 26 | 1st (21) | Heroïn (Methadone | Controlled methadone use |
| 26 | Portugal | M | 44 | 1st (41) | Heroïn (Methadone) | Controlled methadone use |
| 27 | Slovakia | M | 31 | 1st (11) | Heroïn (Methadone) | Controlled methadone use |
| 28 | Morocco | M | 31 | 1st (17) | Cannabis Alcohol Cocaine | None |
| 29 | Ireland | M | 46 | 1st (28) | Alcohol Amphetamines Cocaine | Controlled amphetamine and sporadic alchol use |
| 30 | Turkey | M | 37 | 2nd | Cocaine Benzodiazepines | Sporadic cannabis use |
| 31 | Morocco | M | 32 | 2nd | Cocaine | None |
| 32 | Turkey | M | 45 | 2nd | Heroin | Regular heroin use |
| 33 | Turkey | M | 18 | 3rd | Cocaine Amphetamines | Regular cocaine and amphetamine use |
| 34 | Turkey | M | 35 | 2nd | Cannabis | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pouille, A.; Bellaert, L.; Vander Laenen, F.; Vanderplasschen, W. Recovery Capital among Migrants and Ethnic Minorities in Recovery from Problem Substance Use: An Analysis of Lived Experiences. Int. J. Environ. Res. Public Health 2021, 18, 13025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413025
Pouille A, Bellaert L, Vander Laenen F, Vanderplasschen W. Recovery Capital among Migrants and Ethnic Minorities in Recovery from Problem Substance Use: An Analysis of Lived Experiences. International Journal of Environmental Research and Public Health. 2021; 18(24):13025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413025
Chicago/Turabian StylePouille, Aline, Lore Bellaert, Freya Vander Laenen, and Wouter Vanderplasschen. 2021. "Recovery Capital among Migrants and Ethnic Minorities in Recovery from Problem Substance Use: An Analysis of Lived Experiences" International Journal of Environmental Research and Public Health 18, no. 24: 13025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413025