
Severe COVID-19 Complicated by Cerebral Venous Thrombosis in a Newborn Successfully Treated with Remdesivir, Glucocorticoids, and Hyperimmune Plasma

 ,
,
Abstract
:1. Introduction
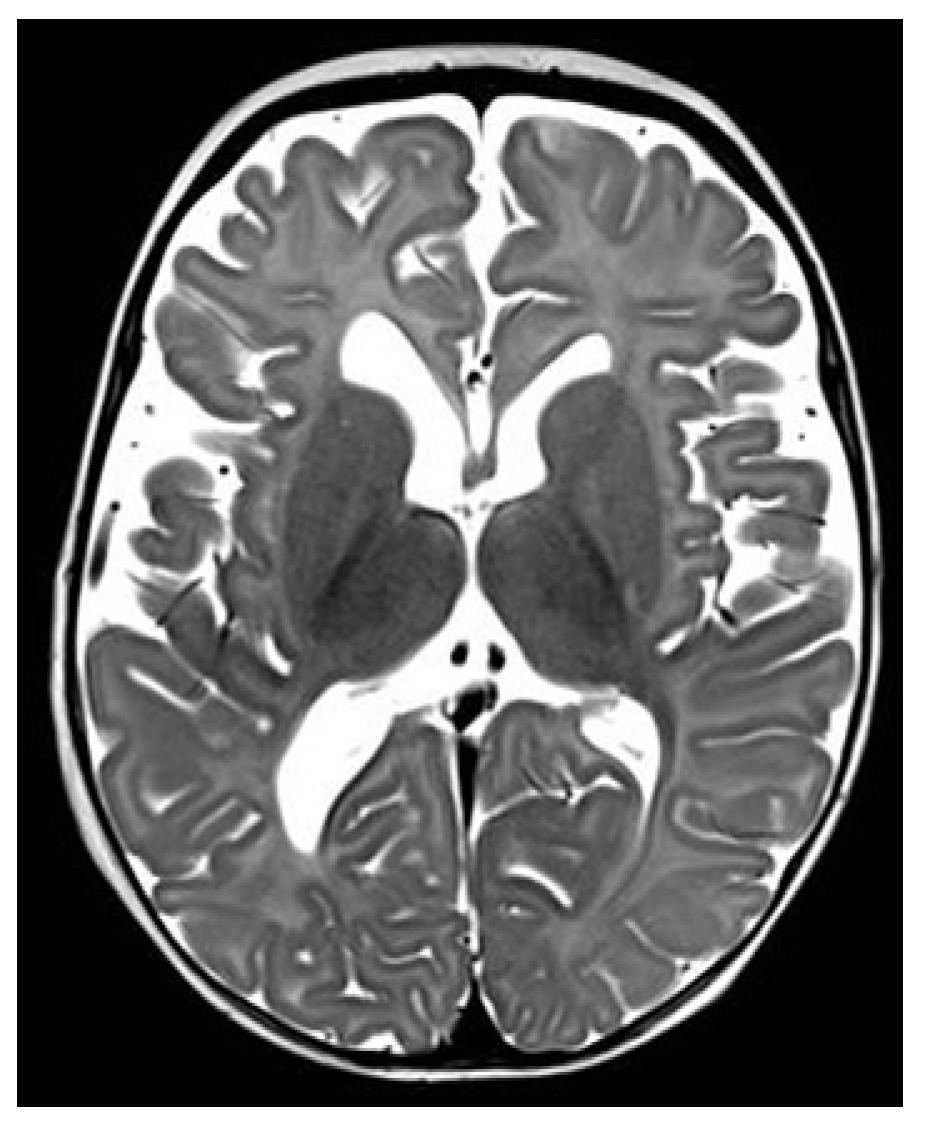
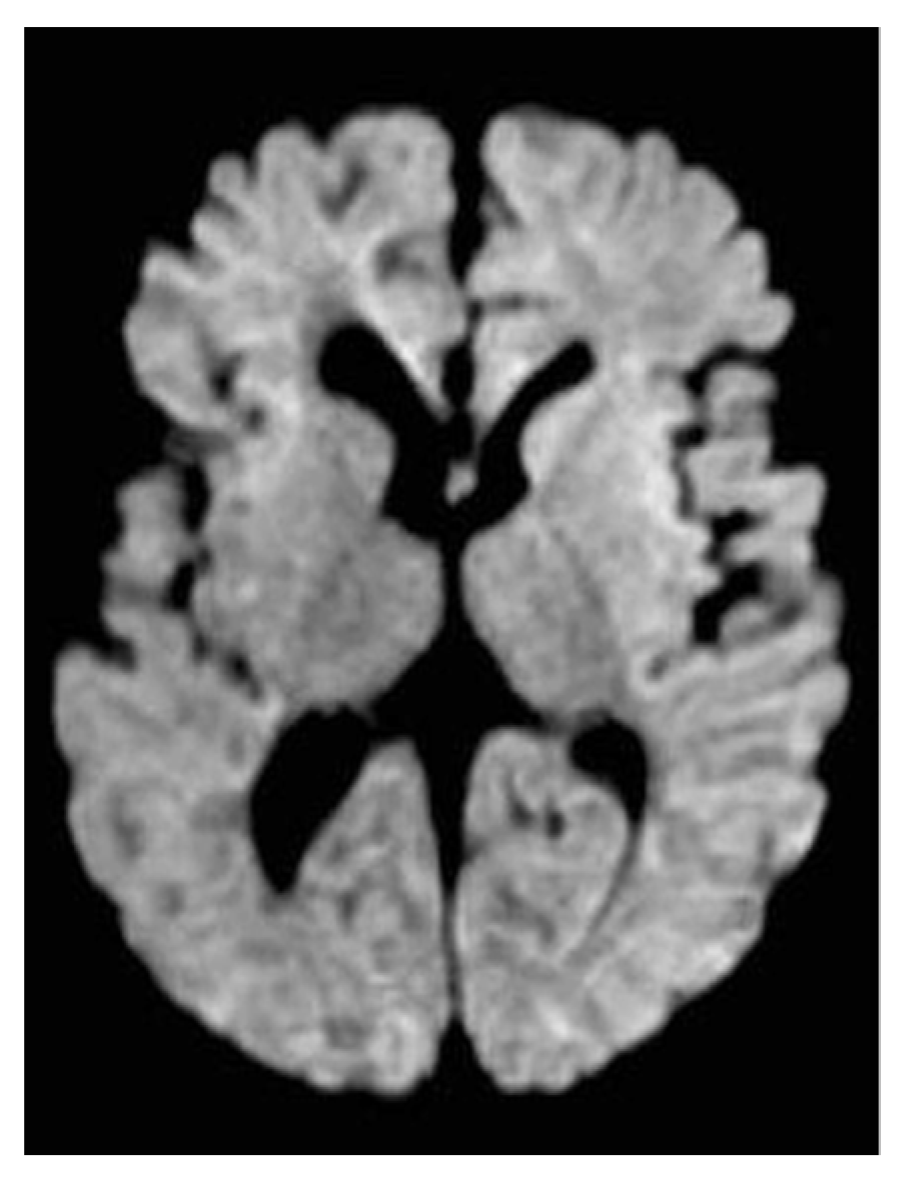
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calo Carducci, F.I.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical transmission of coronavirus disease 2019: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef] [PubMed]
- Yap, M.; Debenham, L.; Kew, T.; Chatterjee, S.R.; Allotey, J.; Stallings, E.; Coomar, D.; Lee, S.I.; Qiu, X.; Yuan, M.; et al. Clinical manifestations, prevalence, risk factors, outcomes, transmission, diagnosis and treatment of COVID-19 in pregnancy and postpartum: A living systematic review protocol. BMJ Open 2020, 10, e041868. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Clinical Management: Living Guidance: 25 January 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 29 September 2021).
- Olivini, N.; Calo Carducci, F.I.; Santilli, V.; De Ioris, M.A.; Scarselli, A.; Alario, D.; Geremia, C.; Lombardi, M.H.; Marabotto, C.; Mariani, R.; et al. A neonatal cluster of novel coronavirus disease 2019: Clinical management and considerations. Ital. J. Pediatr. 2020, 46, 180. [Google Scholar] [CrossRef]
- Yeo, K.T.; Oei, J.L.; De Luca, D.; Schmölzer, G.M.; Guaran, R.; Palasanthiran, P.; Kumar, K.; Buonocore, G.; Cheong, J.; Owen, L.S.; et al. Review of guidelines and recommendations from 17 countries highlights the challenges that clinicians face caring for neonates born to mothers with COVID-19. Acta Paediatr. 2020, 109, 2192–2207. [Google Scholar] [CrossRef]
- Hopwood, A.J.; Jordan-Villegas, A.; Gutierrez, L.D.; Cowart, M.C.; Vega-Montalvo, W.; Cheung, W.L.; McMahan, M.J.; Gomez, M.R.; Laham, F.R. SARS-CoV-2 pneumonia in a newborn treated with remdesivir and COVID-19 convalescent plasma. J. Pediatr. Infect. Dis. Soc. 2021, 10, 691–694. [Google Scholar] [CrossRef]
- Frauenfelder, C.; Brierley, J.; Whittaker, E.; Perucca, G.; Bamford, A. Infant With SARS-CoV-2 Infection Causing Severe Lung Disease Treated with Remdesivir. Pediatrics 2020, 146, e20201701. [Google Scholar] [CrossRef]
- Frampton, D.; Rampling, T.; Cross, A.; Bailey, H.; Heaney, J.; Byott, M.; Scott, R.; Sconza, R.; Price, J.; Margaritis, M.; et al. Genomic characteristics and clinical effect of the emergent SARS-CoV-2 B.1.1.7 lineage in London, UK: A whole-genome sequencing and hospital-based cohort study. Lancet Infect. Dis. 2021, 21, 1246–1256. [Google Scholar] [CrossRef]
- Brookman, S.; Cook, J.; Zucherman, M.; Broughton, S.; Harman, K.; Gupta, A. Effect of the new SARS-CoV-2 variant B.1.1.7 on children and young people. Lancet Child Adolesc. Health 2021, 5, e9–e10. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed on 29 September 2021).
- American Academy of Rheumatology. Available online: https://www.rheumatology.org/Portals/0/Files/ACR-COVID-19-Clinical-Guidance-Summary-MIS-C-Hyperinflammation.pdf (accessed on 7 December 2021).
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Chiotos, K.; Hayes, M.; Kimberlin, D.W.; Jones, S.B.; James, S.H.; Pinninti, S.G.; Yarbrough, A.; Abzug, M.J.; MacBrayne, C.E.; Soma, V.L.; et al. Multicenter interim guidance on use of antivirals for children with COVID-19/SARS-CoV-2. J. Pediatr. Infect. Dis. Soc. 2020, 10, 34–48. [Google Scholar] [CrossRef]
- Maharaj, A.R.; Wu, H.; Hornik, C.P.; Balevic, S.J.; Hornik, C.D.; Smith, P.B.; Gonzalez, D.; Zimmerman, K.O.; Benjamin, D.K.; Cohen-Wolkowiez, M.; et al. Simulated Assessment of Pharmacokinetically Guided Dosing for Investigational Treatments of Pediatric Patients with Coronavirus Disease 2019. JAMA Pediatr. 2020, 174, e202422. [Google Scholar] [CrossRef]
- Wang, Y.; Huo, P.; Dai, R.; Lv, X.; Yuan, S.; Zhang, Y.; Guo, Y.; Li, R.; Yu, Q.; Zhu, K. Convalescent plasma may be a possible treatment for COVID-19: A systematic review. Int. Immunopharmacol. 2021, 91, 107262. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People’s Republic of China. Diagnosis and Treatment of COVID-19 (Trial 8th Edition). Available online: http://www.nhc.gov.cn/yzygj/s7653p/202008/0a7bdf12bd4b46e5bd28ca7f9a7f5e5a.shtml (accessed on 5 November 2020).
- Valk, S.J.; Piechotta, V.; Chai, K.L.; Doree, C.; Monsef, I.; Wood, E.M.; Lamikanra, A.; Kimber, C.; McQuilten, Z.; So-Osman, C.; et al. Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 5, CD013600. [Google Scholar] [CrossRef]
- Food and Drug Administration. Available online: https://www.fda.gov/news-events/press-announcements/fda-expands-authorization-two-monoclonal-antibodies-treatment-and-post-exposure-prevention-covid-19 (accessed on 7 December 2021).
- Magro, G. COVID-19: Review on latest available drugs and therapies against SARS-CoV-2. Coagulation and inflammation cross-talking. Virus Res. 2020, 286, 198070. [Google Scholar] [CrossRef]
- Beslow, L.A.; Linds, A.B.; Fox, C.K.; Kossorotoff, M.; Zambrano, Y.C.Z.; Hernández-Chávez, M.; Hassanein, S.M.A.; Byrne, S.; Lim, M.; Maduaka, N.; et al. Pediatric Ischemic Stroke: An Infrequent Complication of SARS-CoV-2. Ann. Neurol. 2021, 89, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Shirvaliloo, M. Targeting the SARS-CoV-2 3CLpro and NO/cGMP/PDE5 pathway in COVID-19: A commentary on PDE5 inhibitors. Future Cardiol. 2021, 17, 765–768. [Google Scholar] [CrossRef]
- Isidori, A.M.; Giannetta, E.; Pofi, R.; Venneri, M.A.; Gianfrilli, D.; Campolo, F.; Mastroianni, C.M.; Lenzi, A.; D’Ettorre, G. Targeting the NO-cGMP-PDE5 pathway in COVID-19 infection. The DEDALO project. Andrology 2021, 9, 33–38. [Google Scholar] [CrossRef]
- Fletcher-Sandersjöö, A.; Bellander, B.-M. Is COVID-19 associated thrombosis caused by overactivation of the complement cascade? A literature review. Thromb. Res. 2020, 194, 36–41. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Laboratory Findings | Normal Range | Day 1 after Admission | Day 5 after Admission | Day 10 after Admission |
|---|---|---|---|---|
| WBC count per mm3 | 5000–19,500 | 3230 | 1830 | 8960 |
| Lymphocyte count per mm3 | 2000–14,620 | 610 | 480 | 1450 |
| Hemoglobin in g/dL | 12.5–20.5 | 16.8 | 8.6 | 9.8 |
| Platelet per mm3 | 150,000–450,000 | 181,000 | 172,000 | 441,000 |
| C-Reactive protein mg/dL | <0.5 | 0.11 | 0.05 | 0.1 |
| Procalcitonin ng/mL | <0.5 | 1.14 | 0.6 | 0.31 |
| Troponina T high sensitive ng/L | <14 | 54.8 | 77.6 | 41.6 |
| N-Terminal prohormone of Brain Natriuretic Peptide pg/mL | <320 | 3702 | 8115 | 5145 |
| D-Dimer mg/L | <0.5 | 1.77 | 0.76 | 2.41 |
| Fibrinogen mg/dLA | 283–401 | 197 | 67 | 146 |
| Ferritin ug/mL | 30–400 | 1000 | 659 | 402 |
| Lactic Dehydrogenase U/L | 225–600 | 520 | 234 | 317 |
| Serum albumin g/dL | 3.8–5.4 | 2.8 | 3.9 | 4.8 |
| Specimen | Sampling (dd/mm/aa) | SARS-CoV-2 Viral Load (cp/mL log) |
|---|---|---|
| NPS | 06/03/21 | 1.17 × 1010 |
| BAL | 10/03/21 | 2.68 × 109 |
| BAL | 13/03/21 | 1.31 × 109 |
| BAL | 16/03/21 | 1.29 × 106 |
| BAL | 19/03/21 | 1.42 × 105 |
| BAL | 21/03/21 | 1.75 × 106 |
| NPS | 26/03/21 | 1.44 × 103 |
| NPS | 10/04/21 | 1.12 × 103 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cursi, L.; Calo Carducci, F.I.; Chiurchiu, S.; Romani, L.; Stoppa, F.; Lucignani, G.; Russo, C.; Longo, D.; Perno, C.F.; Cecchetti, C.; et al. Severe COVID-19 Complicated by Cerebral Venous Thrombosis in a Newborn Successfully Treated with Remdesivir, Glucocorticoids, and Hyperimmune Plasma. Int. J. Environ. Res. Public Health 2021, 18, 13201. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413201
Cursi L, Calo Carducci FI, Chiurchiu S, Romani L, Stoppa F, Lucignani G, Russo C, Longo D, Perno CF, Cecchetti C, et al. Severe COVID-19 Complicated by Cerebral Venous Thrombosis in a Newborn Successfully Treated with Remdesivir, Glucocorticoids, and Hyperimmune Plasma. International Journal of Environmental Research and Public Health. 2021; 18(24):13201. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413201
Chicago/Turabian StyleCursi, Laura, Francesca Ippolita Calo Carducci, Sara Chiurchiu, Lorenza Romani, Francesca Stoppa, Giulia Lucignani, Cristina Russo, Daniela Longo, Carlo Federico Perno, Corrado Cecchetti, and et al. 2021. "Severe COVID-19 Complicated by Cerebral Venous Thrombosis in a Newborn Successfully Treated with Remdesivir, Glucocorticoids, and Hyperimmune Plasma" International Journal of Environmental Research and Public Health 18, no. 24: 13201. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413201