
Dental Care for a Child with Congenital Hydrocephalus: A Case Report with 12-Month Follow-Up

 ,
, 

Abstract
:1. Introduction
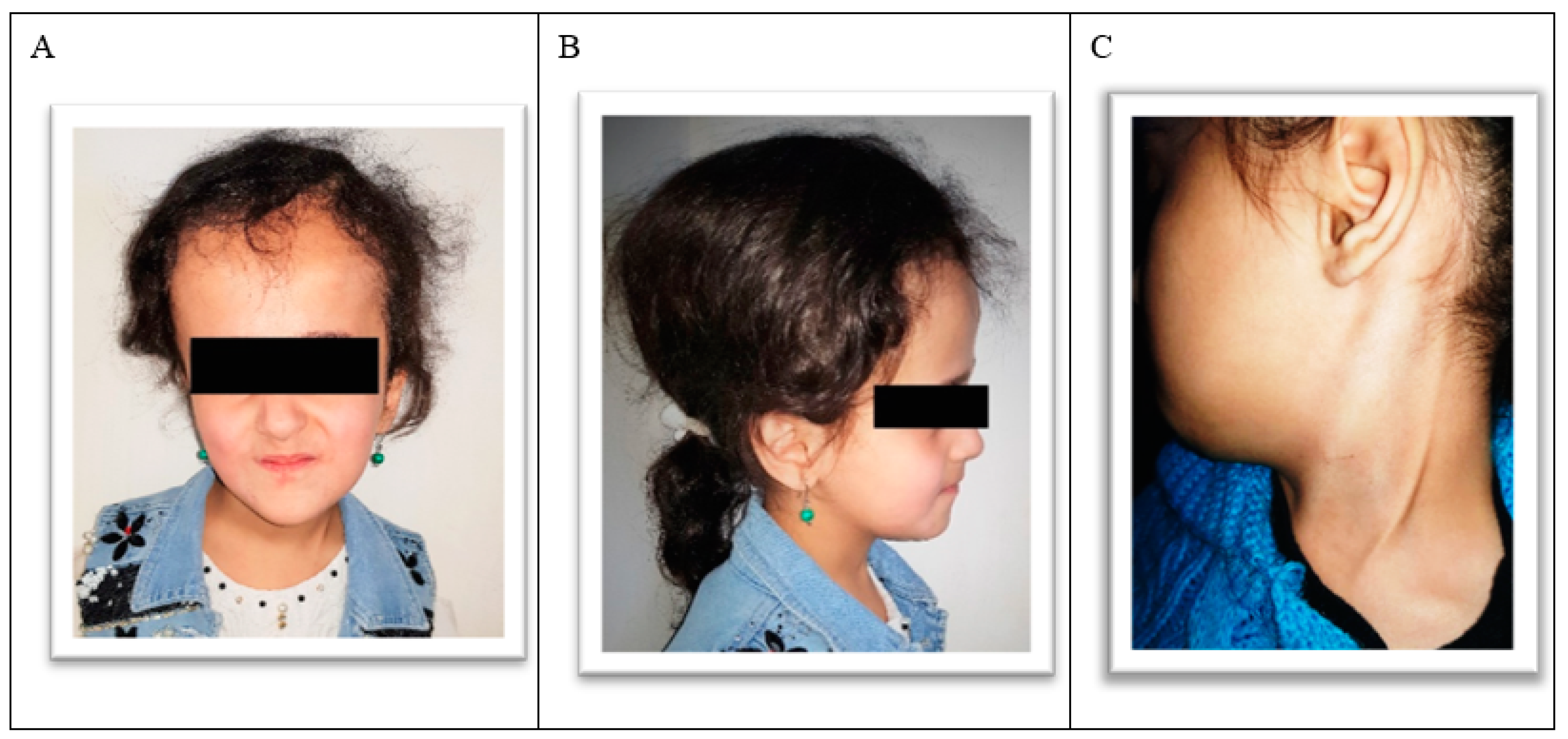
2. Case Report
- Toothbrushing and flossing instruction and the establishment of a caries prevention plan: Chlorhexidine mouthwash (0.12%) and gel (0.2%) were prescribed for an initial period of two to three weeks help resolve gingivitis, and the parents were encouraged to supervise the child’s toothbrushing using a high-concentration fluoridated toothpaste.
- Consultation with the child’s physician.
- Treatment of all carious lesions.
- Orthodontic treatment.
- Maintenance and recalls.
- A detailed discussion with patient and parents regarding the treatment plan.
3. Management
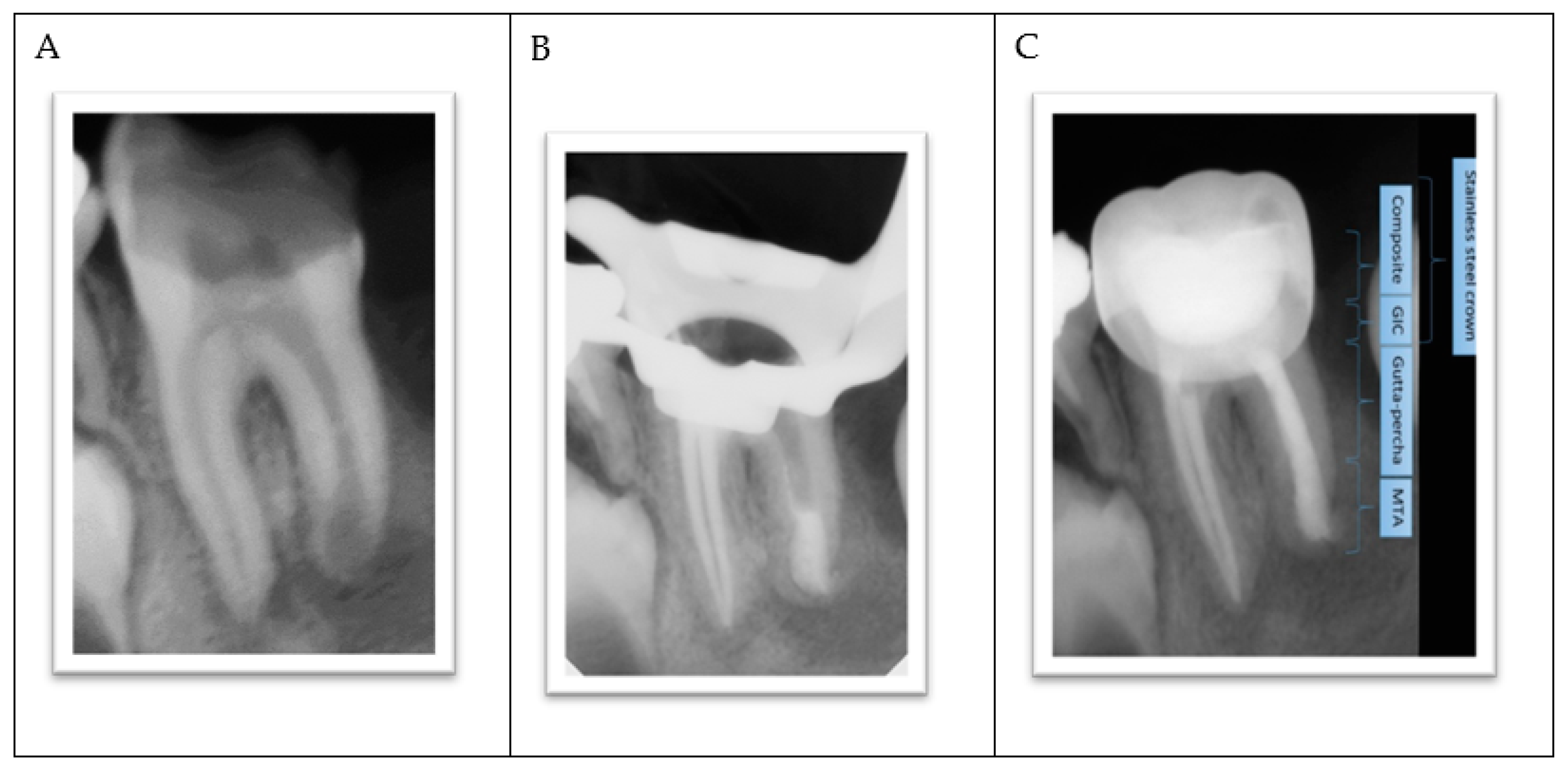
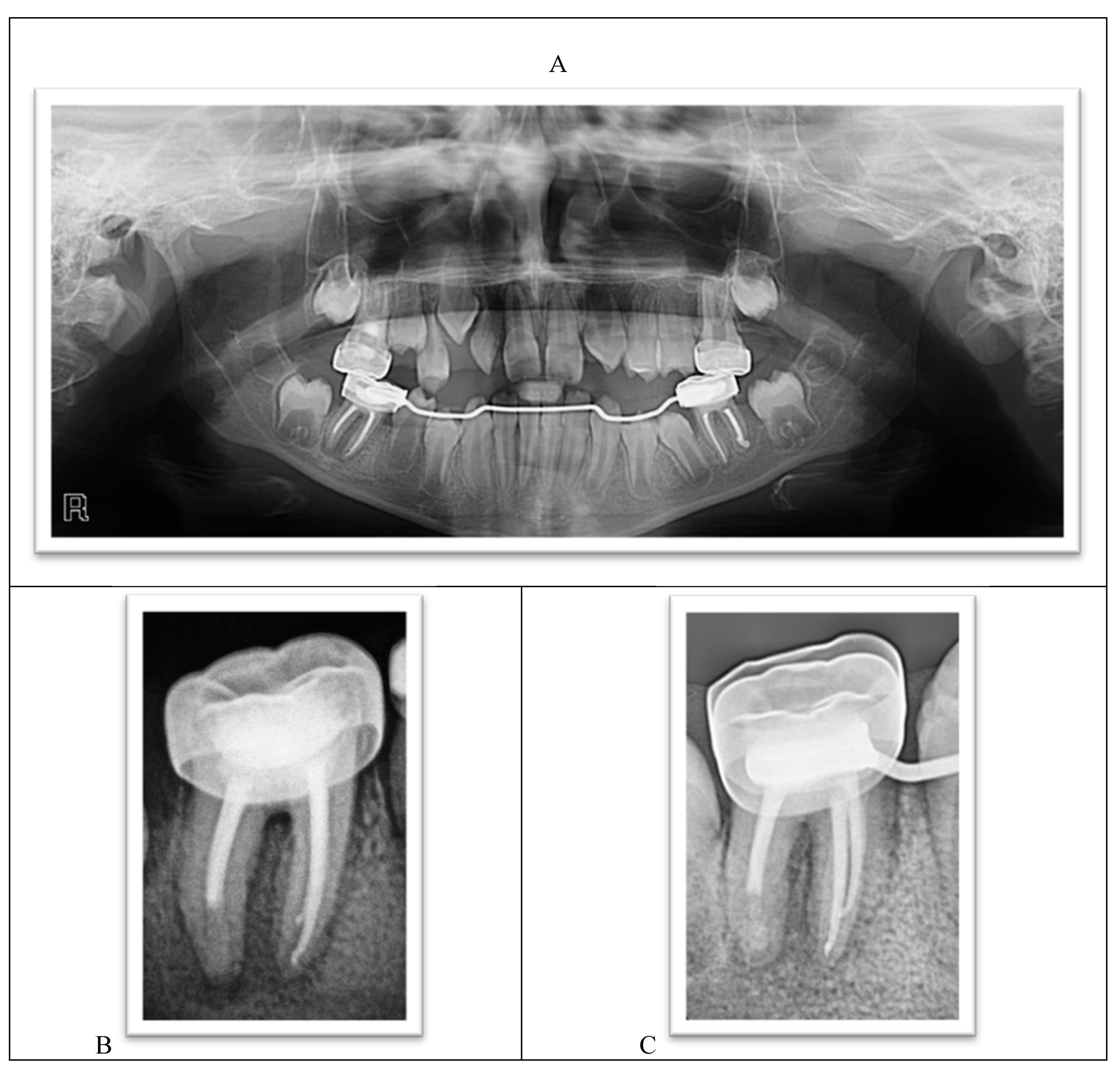
- The procedure involved local anesthesia, a rubber dam, and removal of caries.
- Working length was established using a radiograph.
- Copious irrigation with 2.5% sodium hypochlorite NaOCl, followed by minimal mechanical instrumentation of the root canal walls and additional irrigation with Q-mix (Dentsply Sirona) and ultrasonic activation was performed.
- Mesial canals were obturated with gutta-percha using a lateral condensation technique while the distal root was treated with MTA as an apical plug because there was no apical stop.
- A moist cotton pellet was placed in the canal to facilitate MTA setting, and the access cavity was restored using a glass ionomer cement.
- The next day, the setting of the MTA plug was verified, and the remaining portion of the root canal was filled with gutta-percha using lateral condensation. The pulp chamber was cleaned and the coronal access double-sealed with a bonded resin composite.
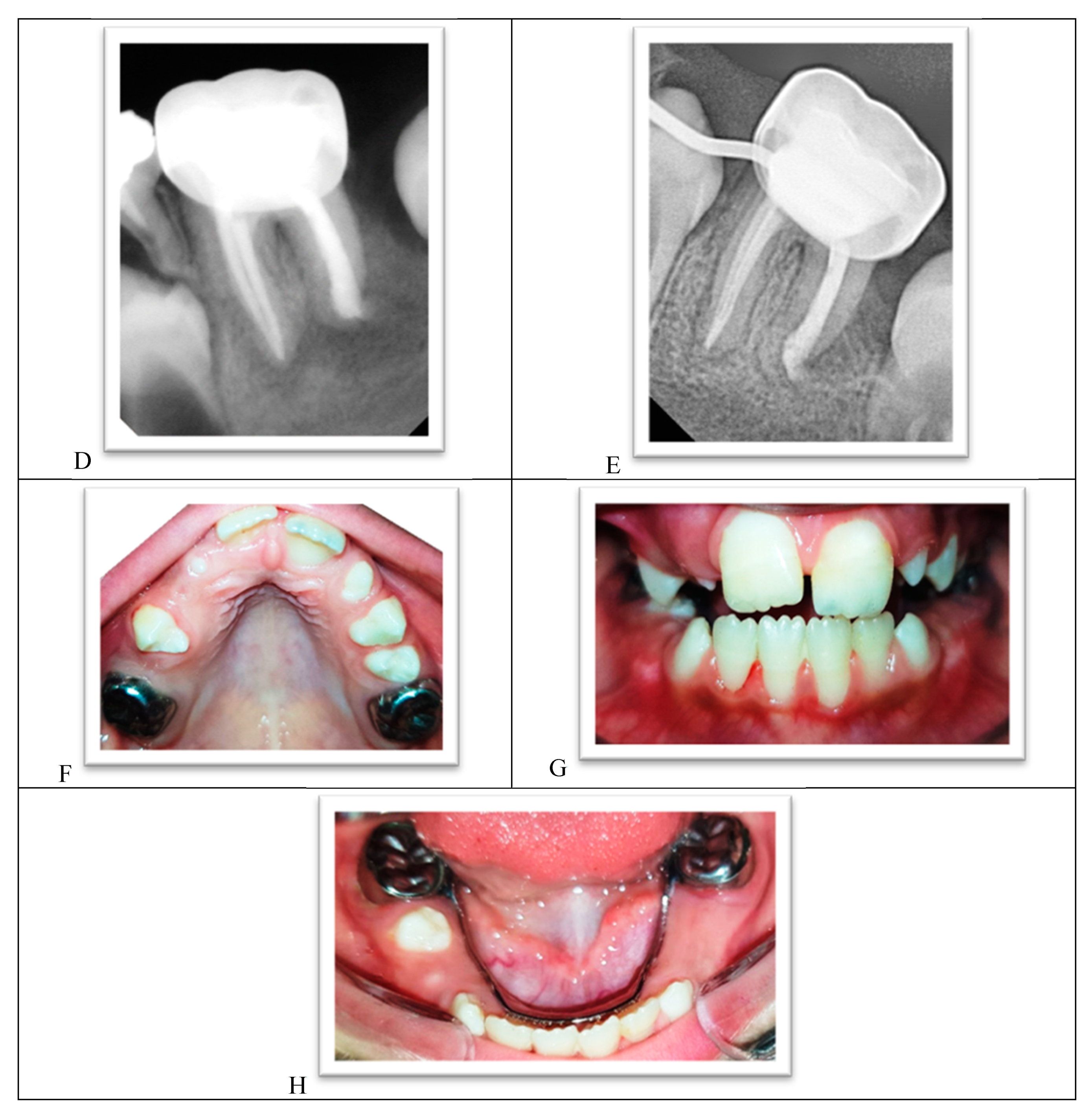
- A stainless steel crown was inserted.
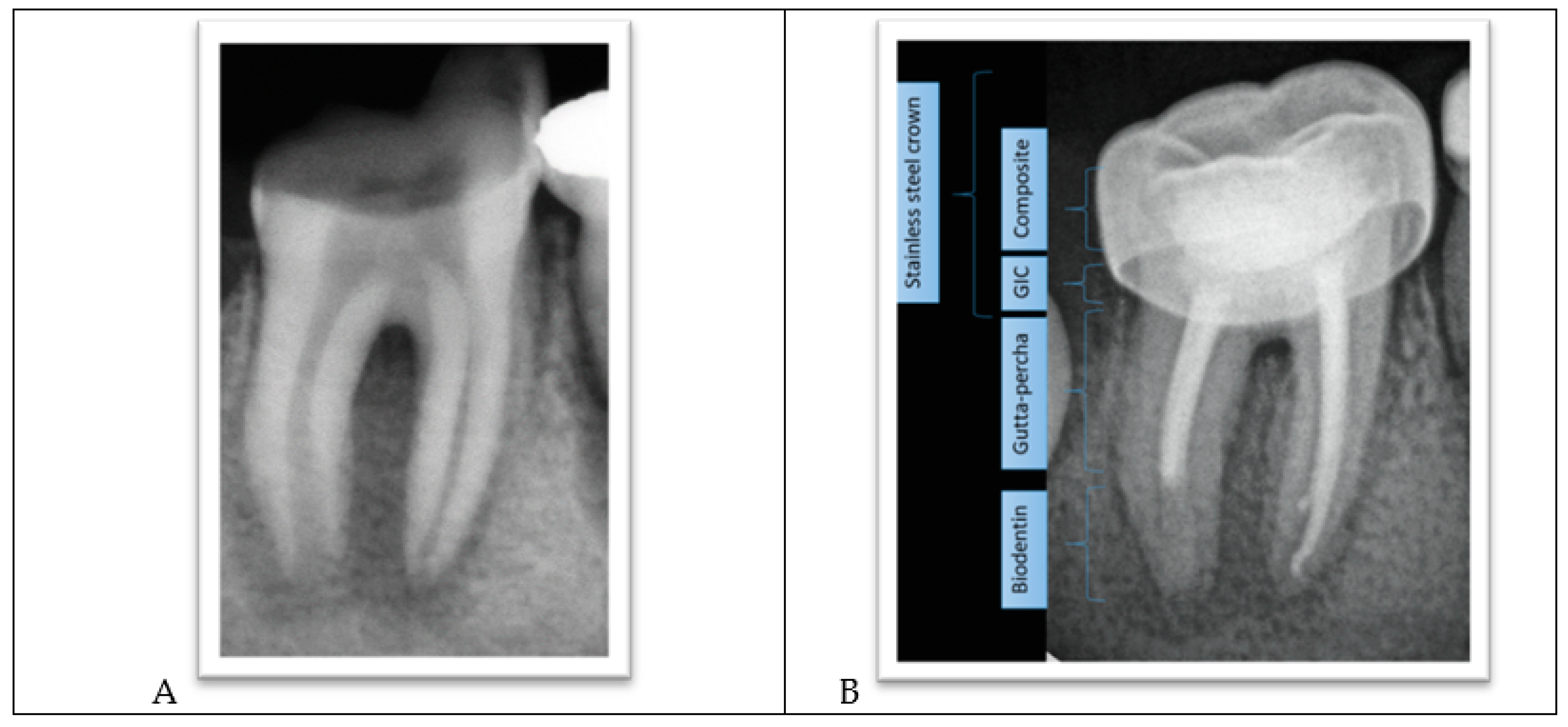
- The procedure involved local anesthesia and rubber dam isolation.
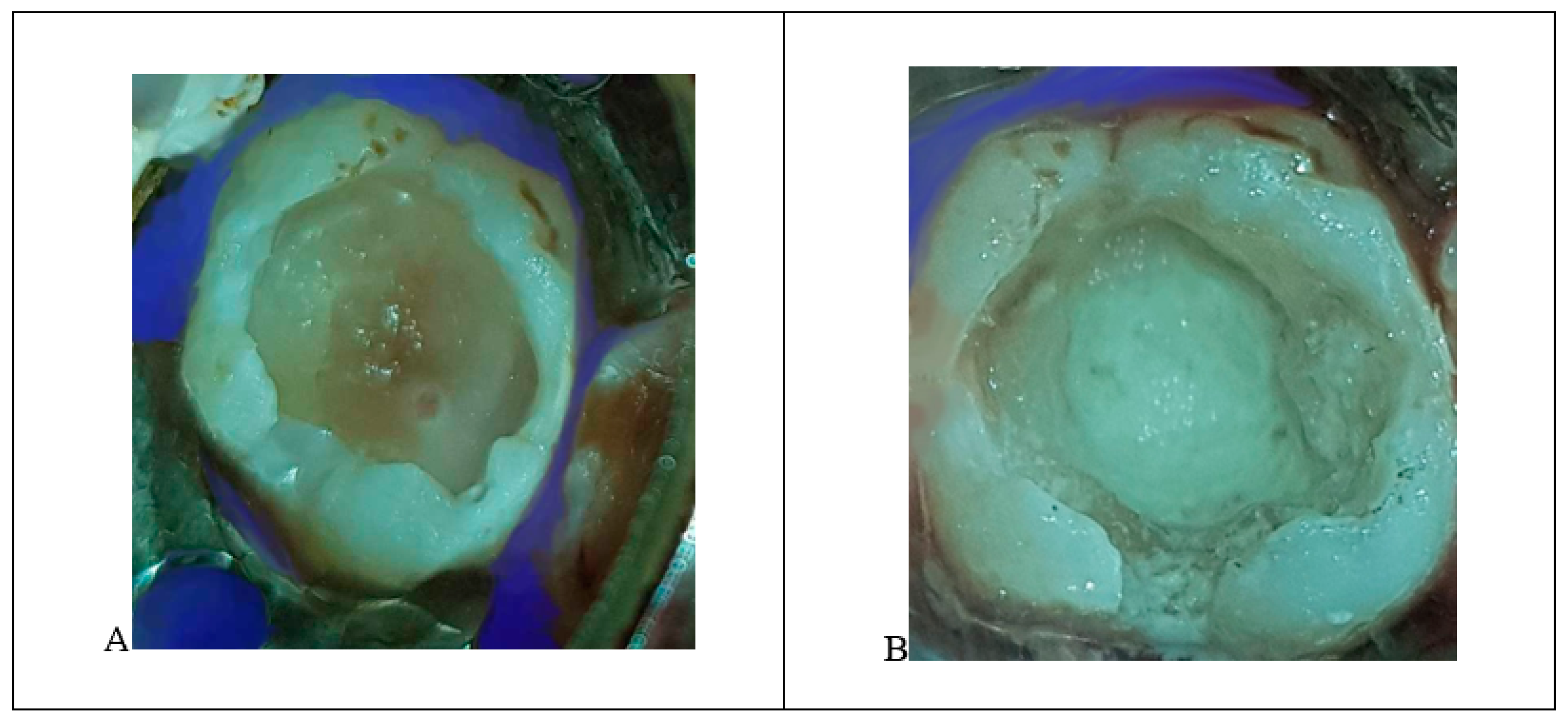
- A pinpoint pulp exposure happened (Figure 6A).
- A coronal pulpotomy was completed by removal of coronal pulp tissue.
- Hemostasis was achieved using 5% sodium hypochlorite and MTA placed as a dressing material over pulp orifices (Figure 6B).
- The tooth was restored like teeth #36 and #46.
Clinical and Radiographic Follow-Up
4. Prognosis and Discussion
Complications and Alternative Treatment Plans
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Acs, G.; Cozzi, E. Antibiotic prophylaxis for patients with hydrocephalus shunts: A survey of pediatric dentistry and neurosurgery program directors. Pediatr. Dent. 1992, 14, 246–250. [Google Scholar] [PubMed]
- Akhter, R.; Hassan, N.M.M.; Martin, E.F.; Muhit, M.; Smithers-Sheedy, H.; Badawi, N.; Khandaker, G. Caries experience and oral health-related quality of life (OHRQoL) of children and adolescents with cerebral palsy in a low-resource setting. BMC Oral Health 2019, 19, 15. [Google Scholar] [CrossRef] [PubMed]
- Akinwonmi, B.A.; Kolawole, K.A.; Folayan, M.O.; Adesunloye, A.M. Orthodontic treatment need of children and adolescents with special healthcare needs resident in Ile-Ife, Nigeria. Eur. Arch. Paediatr. Dent. 2020, 21, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Aptekar, A.; Sandor, G.K. Point of care. What precautions and measures do I have to consider when treating a patient with ventriculoperitoneal vs ventriculoatrial shunt? J. Can. Dent. Assoc. 2006, 72, 627–628. [Google Scholar]
- Ausili, E.; Tabacco, F.; Focarelli, B.; Nucera, E.; Patriarca, G.; Rendeli, C. Prevalence of latex allergy in spina bifida: Genetic and environmental risk factors. Eur. Rev. Med. Pharmacol. Sci. 2007, 11, 149–153. [Google Scholar] [PubMed]
- Becker, A.; Shapira, J.; Chaushu, S. Orthodontic treatment for disabled children--a survey of patient and appliance management. J. Orthod. 2001, 28, 39–44. [Google Scholar] [CrossRef]
- Becker, A.; Shapira, J.; Chaushu, S. Orthodontic treatment for the special needs child. Semin. Orthod. 2004, 10, 281–292. [Google Scholar] [CrossRef]
- Bignardi, L.; Prates, T.; De Rossi, A.; Nelson-Filho, P.; de Carvalho, F.K.; de Siqueira Mellara, T.; de Queiroz, A.M. Strategies and dental care in the treatment of patients with myelomeningocele. Spec. Care Dent. 2018, 38, 89–94. [Google Scholar] [CrossRef]
- De Castilho, L.S.; Abreu, M.H.N.G.; Pires ESouza, L.G.A.; Romualdo, L.T.A.; Souza ESilva, M.E.; Resende, V.L.S. Factors associated with anterior open bite in children with developmental disabilities. Spec. Care Dent. 2018, 38, 46–50. [Google Scholar] [CrossRef]
- De Morais Gallarreta, F.W.; Bernardotti, F.P.; de Freitas, A.C.; de Queiroz, A.M.; Faria, G. Characteristics of individuals with hydrocephalus and their dental care needs. Spec. Care Dent. 2010, 30, 72–76. [Google Scholar] [CrossRef]
- Den Hollander, N.S.; Vinkesteijn, A.; Schmitz-van Splunder, P.; Catsman-Berrevoets, C.E.; Wladimiroff, J.W. Prenatally diagnosed fetal ventriculomegaly; prognosis and outcome. Prenat. Diagn. 1998, 18, 557–566. [Google Scholar] [CrossRef]
- Deshpande, A.N.; Pradhan, N.R.; Patel, K.S.; Mulchandani, V.R. Consequences of Severe Epileptic Attack in a 3-year-old Girl with Congenital Hydrocephalus. Contemp. Clin. Dent. 2018, 9, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Revankar, A.V. Spina bifida and dental care: Key clinical issues. J. Calif. Dent. Assoc. 2012, 40, 868–869. [Google Scholar] [PubMed]
- Huggare, J.A.; Kantomaa, T.J.; Rönning, O.V.; Serlo, W.S. Craniofacial morphology in shunt-treated hydrocephalic children. Cleft Palate J. 1986, 23, 261–269. [Google Scholar] [PubMed]
- Kahle, K.T.; Kulkarni, A.V.; Limbrick, D.D., Jr.; Warf, B.C. Hydrocephalus in children. Lancet 2016, 387, 788–799. [Google Scholar] [CrossRef]
- Kalyvas, A.V.; Kalamatianos, T.; Pantazi, M.; Lianos, G.D.; Stranjalis, G.; Alexiou, G.A. Maternal environmental risk factors for congenital hydrocephalus: A systematic review. Neurosurg. Focus 2016, 41, E3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kestle, J.R.; Walker, M.L.; Strata Investigators. A multicenter prospective cohort study of the Strata valve for the management of hydrocephalus in pediatric patients. J. Neurosurg. 2005, 102 (Suppl. 2), 141–145; [Google Scholar] [CrossRef]
- Kinsman, S.L.; Johnston, M.V. Hydrocephalus. In Nelson Textbook of Pediatrics E-Book, 21st ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Kuru, E.; Eden, E. Success of Two Caries Risk Assessment Tools in Children: A Pilot Study With a 3-Year Follow-Up. Int. Q. Community Health Educ. 2020, 40, 317–320. [Google Scholar] [CrossRef]
- Limbrick, D.D., Jr.; Baksh, B.; Morgan, C.D.; Habiyaremye, G.; McAllister, J.P., 2nd; Inder, T.E.; Mercer, D.; Holtzman, D.M.; Strahle, J.; Wallendorf, M.J.; et al. Cerebrospinal fluid biomarkers of infantile congenital hydrocephalus. PLoS ONE 2017, 12, e0172353. [Google Scholar] [CrossRef]
- Löppönen, T.; Saukkonen, A.L.; Serlo, W.; Tapanainen, P.; Ruokonen, A.; Knip, M. Accelerated pubertal development in patients with shunted hydrocephalus. Arch. Dis. Child. 1996, 74, 490–496. [Google Scholar] [CrossRef] [Green Version]
- Moazzam, A.A.; Nehrer, E.; Da Silva, S.L.; Polido, J.C.; Arakelyan, A.; Habibian, M.; Krieger, M.D. The association between dental health and procedures and developing shunt infections in pediatric patients. J. Neurosurg. Pediatr. 2014, 14, 508–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirttiniemi, P.; Lahtela, P.; Huggare, J.; Serlo, W. Head posture and dentofacial asymmetries in surgically treated muscular torticollis patients. Acta Odontol. Scand. 1989, 47, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Pirttiniemi, P.; Poikela, A.; Huggare, J.; Löppönen, T. Dental maturation in children with shunt-treated hydrocephalus. Cleft Palate Craniofac. J. 2004, 41, 651–654. [Google Scholar] [CrossRef] [PubMed]
- Poonia, A.; Chengappa, M.D.; Mitra, R.; Jain, P.; Ghavri, T. Full-mouth Rehabilitation of a Ventriculoperitoneal Shunt-treated Hydrocephalic Pediatric Patient: A Case Report. Int. J. Clin. Pediatr. Dent. 2020, 13, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Rajasekharan, S.; Martens, L.C.; Cauwels, R.G.E.C.; Anthonappa, R.P. Biodentine™ material characteristics and clinical applications: A 3 year literature review and update. Eur. Arch. Paediatr. Dent. 2018, 19, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, C. Relationship between Dental Procedures and Shunt Infections in Hydrocephalic Patients: A Narrative Review. J. Clin. Pediatr. Dent. 2018, 42, 67–71. [Google Scholar] [CrossRef]
- Sacar, S.; Turgut, H.; Toprak, S.; Cirak, B.; Coskun, E.; Yilmaz, O.; Tekin, K. A retrospective study of central nervous system shunt infections diagnosed in a university hospital during a 4-year period. BMC Infect Dis. 2006, 6, 43. [Google Scholar] [CrossRef] [Green Version]
- Seda, G.; Tsai, S.; Lee-Chiong, T. Medication effects on sleep and breathing. Clin. Chest Med. 2014, 35, 557–569. [Google Scholar] [CrossRef]
- Schubert-Bast, S.; Berghaus, L.; Filmann, N.; Freiman, T.; Strzelczyk, A.; Kieslich, M. Risk and risk factors for epilepsy in shunt-treated children with hydrocephalus. Eur. J. Paediatr. Neurol. 2019, 23, 819–826. [Google Scholar] [CrossRef]
- Shaheen, R.; Sebai, M.A.; Patel, N.; Ewida, N.; Kurdi, W.; Altweijri, I.; Sogaty, S.; Almardawi, E.; Seidahmed, M.Z.; Alnemri, A.; et al. The genetic landscape of familial congenital hydrocephalus. Ann. Neurol. 2017, 81, 890–897. [Google Scholar] [CrossRef]
- Stojicic, S.; Shen, Y.; Qian, W.; Johnson, B.; Haapasalo, M. Antibacterial and smear layer removal ability of a novel irrigant, QMiX. Int. Endod. J. 2012, 45, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Stone, S.S.; Warf, B.C. Combined endoscopic third ventriculostomy and choroid plexus cauterization as primary treatment for infant hydrocephalus: A prospective North American series. J. Neurosurg. Pediatr. 2014, 14, 439–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tully, H.M.; Dobyns, W.B. Infantile hydrocephalus: A review of epidemiology, classification and causes. Eur. J. Med. Genet. 2014, 57, 359–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, J.; Okamoto, K.; Ohashi, T.; Natsumeda, M.; Hasegawa, H.; Oishi, M.; Miyatake, S.; Matsumoto, N.; Fujii, Y. Malignant Hyperthermia and Cerebral Venous Sinus Thrombosis After Ventriculoperitoneal Shunt in Infant with Schizencephaly and COL4A1 Mutation. World Neurosurg. 2019, 127, 446–450. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Procedure | Recommendation | Modification | Further Information |
|---|---|---|---|
| Medical history | A careful history of general health, associated systemic condition | ||
| Antibiotic prophylaxis | Consider with reservation in invasive dental procedures | May be indicated for ventriculoatrial (VA) shunts rather than ventriculoperitoneal (VP) shunts | Infective endocarditis prophylaxis recommended for patients with underlying cardiac conditions associated with the highest risk of adverse outcome from infective endocarditisfor dental procedures that
|
| VP shunt | Be careful not to compress the catheter during dental treatment | Use pillows and cushions to support the patient’s head | |
| Intraoral radiographs | Place the radiograph film within a plastic bag 4 cm by 23 cm to avoid the risk of swallowing/suffocation | Let caregiver control the intraoral position of the film | |
| Prevention | Educate caregivers about the importance of daily oral health care Diet counseling More frequent dental visits More frequent fluoride application or higher fluoride concentration | Demonstrate to caregivers the oral devices used to hold the patient’s mouth open during brushing |
| Diagnosis | Problem List |
|---|---|
| • Congenital hydrocephalus | ◾ Hyposalivation |
| • Malocclusion | ◾ Poorly compliant parents |
| • Mild to moderate gingivitis | High caries risk and poor oral hygiene due to [22]: |
| Special health needs Visible cavitations Enamel demineralization or hypomineralization Lowsocioeconomic status Insufficient oral hygiene measured with the aid of a plaque score High sugar intake measured by a dietary chart Medications that impair saliva flow (Tegretol) Poor toothbrushing performed only on days of dental treatment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsayed Tolibah, Y.; Kouchaji, C.; Lazkani, T.; Abbara, M.T.; Jbara, S.; Baghdadi, Z.D. Dental Care for a Child with Congenital Hydrocephalus: A Case Report with 12-Month Follow-Up. Int. J. Environ. Res. Public Health 2021, 18, 1209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031209
Alsayed Tolibah Y, Kouchaji C, Lazkani T, Abbara MT, Jbara S, Baghdadi ZD. Dental Care for a Child with Congenital Hydrocephalus: A Case Report with 12-Month Follow-Up. International Journal of Environmental Research and Public Health. 2021; 18(3):1209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031209
Chicago/Turabian StyleAlsayed Tolibah, Yasser, Chaza Kouchaji, Thuraya Lazkani, Mohammad Tamer Abbara, Saffana Jbara, and Ziad D. Baghdadi. 2021. "Dental Care for a Child with Congenital Hydrocephalus: A Case Report with 12-Month Follow-Up" International Journal of Environmental Research and Public Health 18, no. 3: 1209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031209