Analysis of the Different Approaches Adopted in the Italian Regions to Care for Patients Affected by COVID-19


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
- Number of diagnosed cases
- Number of patients affected by COVID-19 that are: hospitalized in a ward, hospitalized in an ICU, and confined to home
- Number of deaths
- Number of recoveries
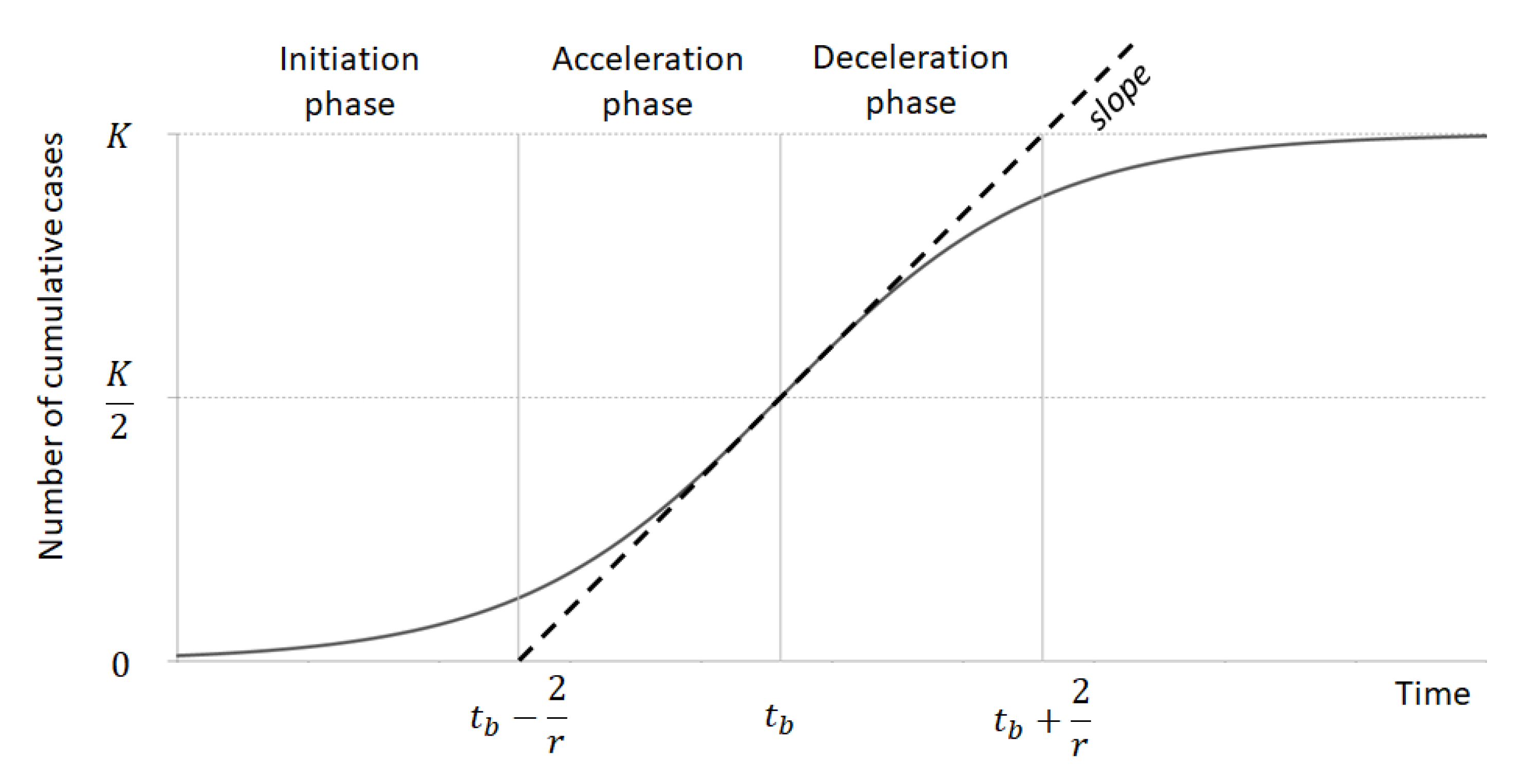
2.2. Data Modelling in Identification of Epidemic Phases
- C(t) represents the cumulative number of cases at a given time t;
- K is the maximum number of cumulative cases K (to be) reached by the relevant region at the end of the epidemic;
- A describes the position of the curve with respect to the x axis;
- r indicates the slope of the curve in the acceleration and deceleration phases of the epidemic period.
- Initiation for t < tp − (2/r), when the number of cases slowly, exponentially increase.
- Acceleration for tp − 2/r < t < tp when the number of cases rapidly increase over time with an aggressive infection spread.
- Deceleration for tp < t < tp + 2/r when the number of daily cases start decreasing and the cumulative cases start decelerating and the infection starts becoming less aggressive.
- Preparation for t > tp + 2/r when few number of daily cases are diagnosed and the curve tend to K.
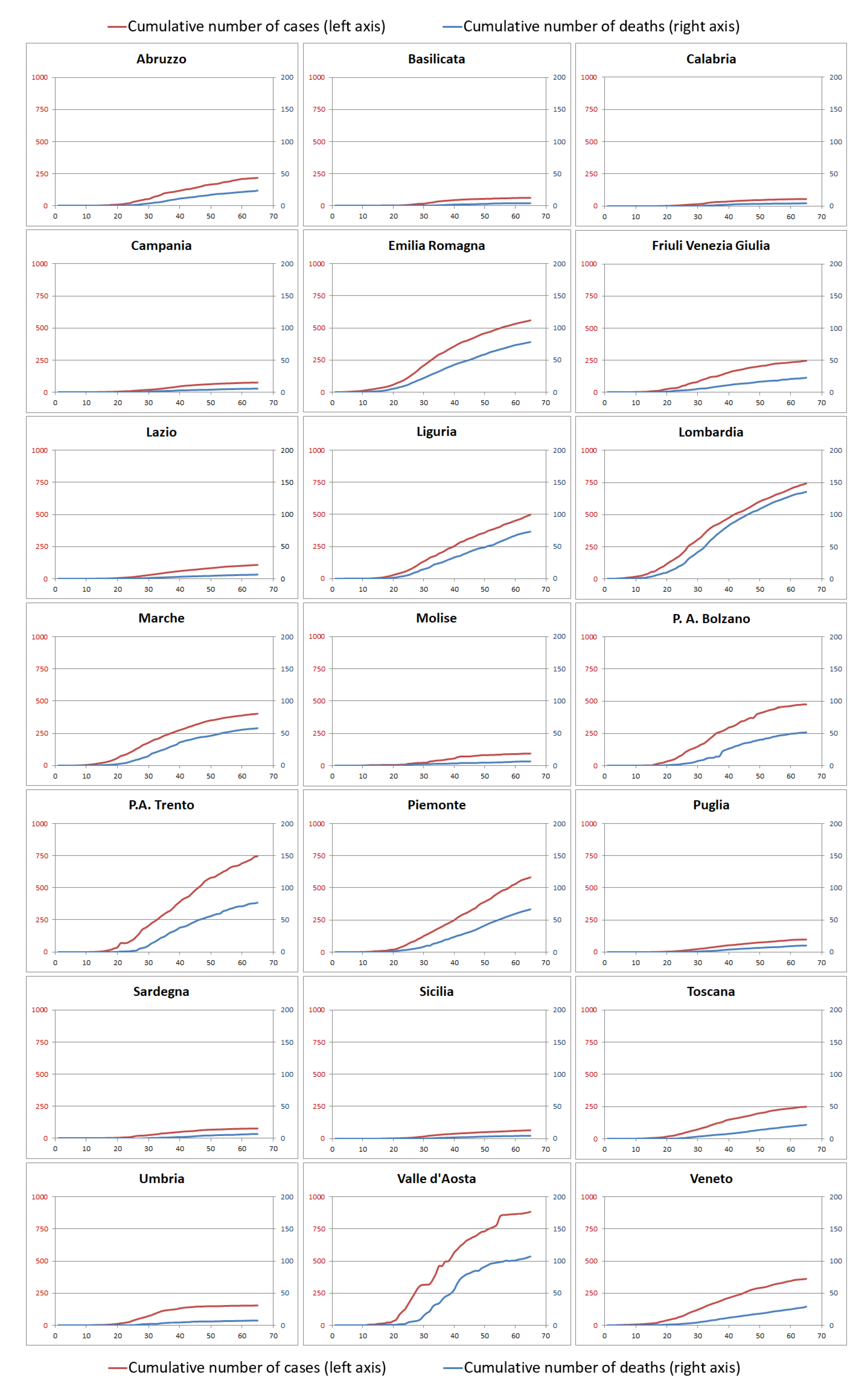
3. Results
3.1. Data Analysis
- Regions with low prevalence (lower than 33% of the maximum number of cases per 100,000 inhabitants): Calabria, Sicilia, Basilicata, Campania, Sardegna, Molise, Puglia, Lazio, Umbria, Abruzzo, Friuli Venezia Giulia, Toscana;
- Regions with medium prevalence (between 33% and 66% of the maximum number of cases per 100,000 inhabitants): Veneto, Marche, P.A. Bolzano, Liguria, Emilia-Romagna, Piemonte;
- Regions with high prevalence (higher than 66% of the maximum number of cases per 100,000 inhabitants): P.A. Trento, Lombardia, Valle d’Aosta.
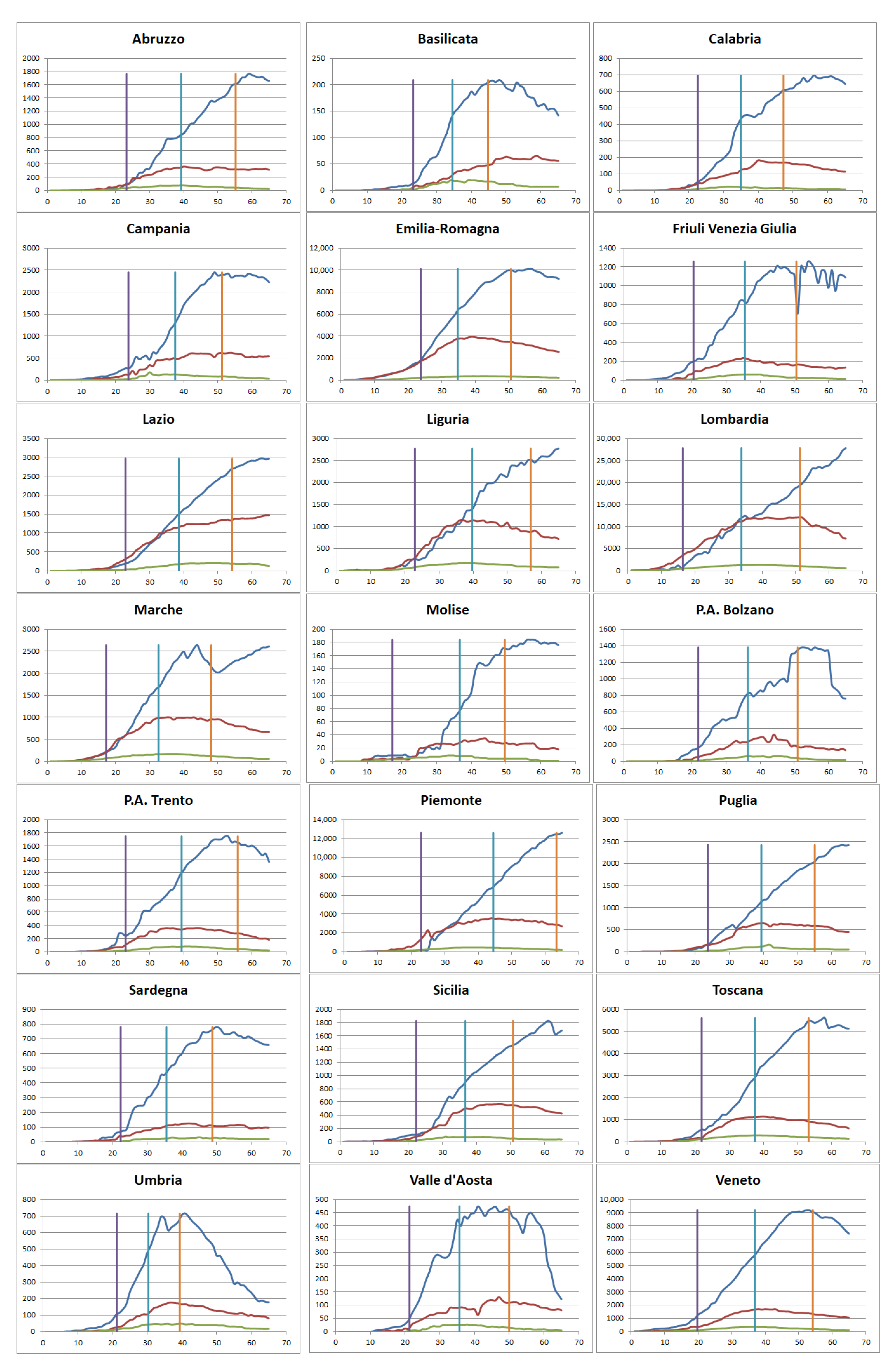
3.2. Application of the Model and Patient Management
- Patients treated predominantly at home even from the initial phase. This pattern is even more evident during the subsequent phases. Regions that belong to this group are: Campania, Friuli, P.A. Bolzano, P.A. Trento, Sardegna, Toscana, Umbria, Val d’Aosta, Veneto. Among these regions, Veneto represents an important case study as the home care approach is adopted already during the first days of contagion.
- Mixed approach where nearly half of the patients are treated in the hospital and the other half are confined at home. This is shown particularly during the first phase, while subsequently the home care approach progressively increases during the second and, even more, during the third phase. Regions within this group are: Abruzzo, Basilicata, Calabria, Emilia Romagna, Marche, Puglia. Among them, Emilia Romagna represents an interesting case study for two main reasons: the number of cases and the home care pattern is quite similar to the one of the Veneto region during the second and third phases.
- Similar to the previous one, this group adopts a mixed approach also in the second phase of the infection. Home care began to be prevalent during the third phase. Regions that adopt this pattern are: Liguria, Molise, Sicilia.
- Patients treated predominantly at hospital in particular during the initial phase. Subsequently, these regions adopt a mixed approach during the second phase and then a home care approach during the third phase. Regions within this group are: Lazio, Lombardia, Piemonte. Among them, Lombardia represents an interesting and widely analyzed case study considering in particular the high ratio between hospital and home care as well as the fact that the mixed approach is adopted only during the second part of the acceleration phase. Similarly, this region tends to hospitalize an important number of patients also during the third phase with a predominant home care model adopted only at the end of the deceleration phase.
- the ratio between hospitalized patients and those confined at home to specify the approach adopted by each region in term of level of hospitalization vs. home care;
- the death rate as well as the recoveries to capture the impact of the virus in the specific region.
4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Region | Start: End Days | Ward (Days) | ICU (Days) | Home (Days) | Ward/Home (Days) | Active | Deaths | Recoveries | Total Cases |
|---|---|---|---|---|---|---|---|---|---|
| Initiation phase | |||||||||
| Abruzzo | 1:23 | 7.13 (37.92) | 2.43 (11.75) | 6.82 (22.52) | 1.04 (1.68) | 16.38 | 0.45 | 0.53 | 17.37 |
| Basilicata | 1:24 | 1.58 (4.57) | 0.35 (2.29) | 2.81 (16.18) | 0.56 (0.28) | 4.75 | 0.00 | 0.00 | 4.75 |
| Calabria | 1:23 | 2.29 (10.35) | 0.51 (1.84) | 2.91 (11.02) | 0.79 (0.94) | 5.71 | 0.05 | 0.05 | 5.81 |
| Campania | 1:24 | 2.18 (14.68) | 0.41 (2.97) | 4.66 (32.20) | 0.47 (0.46) | 7.25 | 0.15 | 0.48 | 7.89 |
| Emilia Romagna | 1:19 | 21.16 (144.18) | 2.88 (19.43) | 21.14 (142.51) | 1.00 (1.01) | 45.18 | 4.52 | 1.15 | 50.85 |
| Friuli Venezia Giulia | 1:20 | 5.51 (19.40) | 0.90 (3.53) | 15.86 (71.67) | 0.35 (0.27) | 22.27 | 1.07 | 1.40 | 24.74 |
| Lazio | 1:23 | 5.32 (26.05) | 0.75 (4.27) | 3.26 (16.58) | 1.64 (1.57) | 9.33 | 0.39 | 0.58 | 10.29 |
| Liguria | 1:23 | 19.15 (102.62) | 5.44 (30.68) | 17.74 (83.66) | 1.08 (1.23) | 42.34 | 3.84 | 3.65 | 49.84 |
| Lombardia | 1:16 | 33.1 (161.01) | 4.65 (30.55) | 6.4 (63.97) | 5.17 (2.52) | 44.15 | 4.67 | 8.94 | 57.75 |
| Marche | 1:17 | 13.81 (60.98) | 4.30 (21.3) | 11.92 (55.51) | 1.16 (1.1) | 30.03 | 1.17 | 0.00 | 31.21 |
| Molise | 1:24 | 2.26 (21.00) | 1.94 (13.89) | 2.59 (36.19) | 0.88 (0.58) | 6.79 | 0.32 | 1.94 | 9.05 |
| P.A. Bolzano | 1:22 | 10.08 (44.3) | 2.09 (6.84) | 32.51 (135.93) | 0.31 (0.33) | 44.68 | 1.14 | 0.00 | 45.82 |
| P.A. Trento | 1:23 | 19.84 (92.72) | 4.08 (17.62) | 44.32 (219.75) | 0.45 (0.42) | 68.24 | 1.30 | 1.85 | 71.40 |
| Piemonte | 1:26 | 35.15 (264.52) | 6.39 (46.76) | 32.46 (73.56) | 1.08 (3.6) | 73.99 | 4.77 | 0.18 | 78.94 |
| Puglia | 1:24 | 3.85 (22.26) | 0.74 (2.19) | 4.34 (19.08) | 0.89 (1.17) | 8.92 | 0.47 | 0.05 | 9.44 |
| Sardegna | 1:22 | 2.36 (8.06) | 0 (0) | 4.00 (16.84) | 0.59 (0.48) | 6.36 | 0.12 | 0.00 | 6.48 |
| Sicilia | 1:23 | 1.71 (8.65) | 0.56 (1.77) | 2.22 (16.46) | 0.77 (0.53) | 4.48 | 0.06 | 0.16 | 4.70 |
| Toscana | 1:22 | 4.68 (34.55) | 2.86 (15.08) | 14.95 (65.94) | 0.31 (0.52) | 22.49 | 0.37 | 0.29 | 23.16 |
| Umbria | 1:21 | 2.82 (10.49) | 1.47 (6.77) | 11.39 (48.38) | 0.25 (0.22) | 15.67 | 0.11 | 0.34 | 16.13 |
| Valle d’Aosta | 1:21 | 7.90 (35.56) | 2.37 (2.37) | 33.98 (141.45) | 0.23 (0.25) | 44.25 | 0.79 | 0.00 | 45.04 |
| Veneto | 1:20 | 7.46 (52.14) | 2.43 (15.33) | 26.29 (149.97) | 0.28 (0.35) | 36.18 | 1.12 | 2.18 | 39.48 |
| Acceleration phase | |||||||||
| Abruzzo | 24:39 | 18.73 (313.34) | 3.26 (72.65) | 56.49 (587.54) | 0.33 (0.53) | 94.87 | 10.09 | 8.57 | 113.52 |
| Basilicata | 25:35 | 4.04 (33.76) | 2.81 (23.38) | 23.03 (150.86) | 0.18 (0.22) | 34.64 | 0.70 | 0.18 | 35.52 |
| Calabria | 24:35 | 4.03 (52.22) | 0.46 (11.37) | 19.23 (131.93) | 0.21 (0.4) | 29.43 | 1.27 | 0.61 | 31.31 |
| Campania | 25:38 | 6.02 (86.37) | 1.8 (26.73) | 18.81 (177.82) | 0.32 (0.49) | 33.88 | 2.54 | 1.83 | 38.25 |
| Emilia Romagna | 20:35 | 63.52 (875.38) | 4.61 (93.65) | 123.39 (1256.21) | 0.51 (0.7) | 236.70 | 32.42 | 25.64 | 294.76 |
| Friuli Venezia Giulia | 21:36 | 13.31 (223.55) | 4.03 (53.92) | 51.53 (691.28) | 0.26 (0.32) | 91.15 | 8.79 | 23.42 | 123.36 |
| Lazio | 24:39 | 14.5 (225.39) | 2.32 (29.95) | 22.67 (227.29) | 0.64 (0.99) | 48.82 | 3.14 | 6.26 | 58.21 |
| Liguria | 24:40 | 54.32 (966.93) | 5.64 (162.9) | 73.6 (894.55) | 0.74 (1.08) | 175.90 | 33.25 | 44.84 | 253.98 |
| Lombardia | 17:34 | 78.11 (1377.51) | 8.51 (176.69) | 113.64 (1131.25) | 0.69 (1.22) | 244.41 | 59.28 | 89.37 | 393.06 |
| Marche | 18:33 | 49.97 (708.97) | 6.25 (131.67) | 99.42 (984.5) | 0.5 (0.72) | 185.68 | 21.89 | 0.65 | 208.22 |
| Molise | 25:37 | 7.11 (104.05) | 0.65 (31.34) | 23.27 (162.86) | 0.31 (0.64) | 37.81 | 2.91 | 5.82 | 46.53 |
| P.A. Bolzano | 23:36 | 33.84 (431.94) | 9.7 (95.25) | 120.53 (1310.64) | 0.28 (0.33) | 208.74 | 14.07 | 29.09 | 251.90 |
| P.A. Trento | 24:39 | 43.02 (849.32) | 10.38 (170.98) | 172.65 (2072.87) | 0.25 (0.41) | 294.30 | 34.68 | 42.47 | 371.44 |
| Piemonte | 27:45 | 44.52 (1281.63) | 3.26 (179.35) | 128.87 (1812.19) | 0.35 (0.71) | 250.65 | 31.43 | 34.58 | 316.66 |
| Puglia | 25:39 | 12.06 (157.52) | 2.17 (26.85) | 22.81 (239.57) | 0.53 (0.66) | 45.96 | 3.55 | 1.70 | 51.21 |
| Sardegna | 23:36 | 4.48 (63.31) | 1.45 (13.99) | 25.38 (241.84) | 0.18 (0.26) | 37.68 | 1.70 | 1.94 | 41.32 |
| Sicilia | 24:37 | 8.27 (84.22) | 0.87 (16.7) | 15.97 (140.31) | 0.52 (0.6) | 29.59 | 1.61 | 1.47 | 32.67 |
| Toscana | 23:38 | 25.27 (364.54) | 5.08 (100.92) | 65.67 (690.85) | 0.38 (0.53) | 118.51 | 6.77 | 4.87 | 130.14 |
| Umbria | 22:30 | 9.02 (74.88) | 3.38 (28.3) | 42.29 (283.72) | 0.21 (0.26) | 70.37 | 2.14 | 0.56 | 73.07 |
| Valle d’Aosta | 22:36 | 64.8 (771.28) | 18.18 (204.67) | 282.12 (2953.13) | 0.23 (0.26) | 409.34 | 39.51 | 12.64 | 461.50 |
| Veneto | 21:37 | 26.78 (390.5) | 4.83 (93.27) | 92.21 (1225.38) | 0.29 (0.32) | 160.00 | 9.72 | 16.88 | 186.60 |
| Deceleration phase | |||||||||
| Abruzzo | 40:55 | −1.52 (405.17) | −2.58 (68.48) | 58.69 (1524.14) | −0.03 (0.27) | 149.46 | 19.19 | 19.94 | 188.59 |
| Basilicata | 36:45 | 2.81 (74.2) | −0.18 (31.12) | 10.2 (320.88) | 0.28 (0.23) | 47.47 | 2.46 | 2.29 | 52.22 |
| Calabria | 36:47 | 2.24 (99.39) | −0.25 (9.54) | 8.67 (311.09) | 0.26 (0.32) | 40.08 | 3.31 | 2.55 | 45.95 |
| Campania | 39:51 | 2.4 (129.75) | −0.81 (21.79) | 17.57 (465.34) | 0.14 (0.28) | 53.04 | 4.46 | 7.11 | 64.62 |
| Emilia Romagna | 36:51 | −6.65 (1339.63) | −0.11 (127.26) | 79.63 (3098.27) | −0.08 (0.43) | 309.56 | 60.78 | 95.92 | 466.26 |
| Friuli Venezia Giulia | 37:51 | −5.18 (223.22) | −2.63 (53.92) | −9.45 (1331.69) | 0.55 (0.17) | 73.89 | 16.93 | 116.30 | 207.11 |
| Lazio | 40:54 | 2.76 (323.21) | 0.1 (49.94) | 19.77 (550.53) | 0.14 (0.59) | 71.46 | 5.63 | 16.58 | 93.67 |
| Liguria | 41:57 | −17.23 (1110.29) | −4.55 (147.78) | 69.82 (2352.79) | −0.25 (0.47) | 223.94 | 61.30 | 141.95 | 427.19 |
| Lombardia | 35:51 | 9.22 (2014.93) | −1.96 (215.97) | 71.06 (2540.64) | 0.13 (0.79) | 322.73 | 111.11 | 177.72 | 611.56 |
| Marche | 34:48 | −1.24 (953.42) | −2.87 (146.85) | 28.93 (2250.64) | −0.04 (0.42) | 210.50 | 44.89 | 84.11 | 339.50 |
| Molise | 38:50 | −0.32 (128.28) | −1.29 (22.62) | 29.08 (591.65) | −0.01 (0.22) | 65.27 | 4.85 | 12.93 | 83.04 |
| P.A. Bolzano | 37:51 | −10.27 (717.3) | −4.37 (159.13) | 103.23 (2813.49) | −0.1 (0.25) | 297.34 | 40.68 | 77.19 | 415.21 |
| P.A. Trento | 40:56 | −11.31 (1029.57) | −6.86 (197.5) | 89.38 (4946.66) | −0.13 (0.21) | 365.51 | 66.76 | 222.72 | 654.98 |
| Piemonte | 46:63 | −14.3 (1334.25) | −4.77 (132.91) | 122.39 (4215.3) | −0.12 (0.32) | 353.98 | 64.39 | 147.76 | 566.12 |
| Puglia | 40:55 | −1.26 (241.98) | −1.43 (34.79) | 23.15 (648.68) | −0.05 (0.37) | 66.42 | 7.74 | 9.89 | 84.05 |
| Sardegna | 37:49 | −0.24 (91.6) | 0.12 (20.36) | 17.14 (519.36) | −0.01 (0.18) | 54.70 | 4.42 | 8.30 | 67.43 |
| Sicilia | 38:51 | 0.97 (152.43) | −0.38 (18.25) | 10.89 (343.87) | 0.09 (0.44) | 41.08 | 3.47 | 5.06 | 49.61 |
| Toscana | 39:53 | −4.81 (420.69) | −2.25 (101.96) | 65.38 (1764.66) | −0.07 (0.24) | 176.83 | 15.64 | 19.92 | 212.39 |
| Umbria | 31:39 | 7.44 (161.71) | 0.45 (46.01) | 21.54 (639.05) | 0.35 (0.25) | 99.80 | 4.29 | 23.12 | 127.20 |
| Valle d’Aosta | 37:50 | 13.43 (1135.58) | −8.69 (228.38) | 45.83 (5021.98) | 0.29 (0.23) | 459.92 | 90.88 | 181.76 | 732.55 |
| Veneto | 38:54 | −6.54 (535.25) | −3.24 (96.22) | 66.2 (2839.7) | −0.1 (0.19) | 216.42 | 20.91 | 76.02 | 313.35 |
References
- European Centre for Disease Prevention and Control (ECED). COVID-19. Available online: https://www.ecdc.europa.eu/en/covid-19-pandemic (accessed on 19 January 2021).
- Pisano, G.P.; Sadun, R.; Zanini, M. Lessons from Italy’s Response to Coronavirus. Harvard Business Review. 2020. Available online: https://hbr.org/2020/03/lessons-from-italys-response-to-coronavirus (accessed on 19 January 2021).
- Carra, L. Vittorio Carreri: L’epidemia si Combatte Anche sul Territorio. Scienza in Rete. 2020. Available online: https://www.scienzainrete.it/articolo/vittorio-carreril%E2%80%99epidemia-si-combatte-anche-sul-territorio/luca-carra/2020-03-26 (accessed on 19 January 2021).
- Monacelli, T.; Polo, M. Covid-19, Ecco le Differenze tra Lombardia E Veneto. 2020. Available online: https://www.startmag.it/mondo/covid-19-lombardia-veneto/ (accessed on 19 January 2021).
- Gaeta, G. Data analysis for the COVID-19 early dynamics in Northern Italy. arXiv 2020, arXiv:2003.02062. [Google Scholar]
- Binkin, N.; Salmaso, S.; Michieletto, F.; Russo, F. Protecting Our Health Care Workers while Protecting our Communities during the COVID-19 Pandemic: A Comparison of Approaches and Early Outcomes in Two Italian Regions, Italy. MedRxiv Prepr. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.04.10.20060707v2 (accessed on 19 January 2021).
- Boccia, S.; Cascini, F.; McKee, M.; Ricciardi, W. How the Italian NHS Is Fighting Against the COVID-19 Emergency. Front. Public Health 2020, 8, 167. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Pandemic Influenza Preparedness and Response: A WHO Guidance Document; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Pandemic Intervals Framework (PIF). Available online: https://www.cdc.gov/flu/pandemic-resources/national-strategy/intervals-framework.html (accessed on 19 January 2021).
- Italian Civil Protection Department. Open Data on COVID-19. 2020. Available online: https://github.com/pcm-dpc/COVID-19 (accessed on 19 January 2021).
- Italian Civil Protection Department Website. COVID-19 Daily Report. Available online: http://www.protezionecivile.gov.it/ (accessed on 19 January 2021).
- Italian National Institute of Statistics (ISTAT). Resident Population. Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_POPRES1 (accessed on 19 January 2021).
- Pecoraro, F.; Luzi, D.; Clemente, F. Analysis of the Different Approaches Adopted in the Italian Regions to Care for Patients Affected by COVID-19. 2020. Available online: https://zenodo.org/record/3865424#.Xt87ejozY2w (accessed on 19 January 2021).
- Tátrai, D.; Várallyay, Z. COVID-19 Epidemic Outcome Predictions Based on Logistic Fitting and Estimation of its Reliability. arXiv 2020, arXiv:2003.14160. [Google Scholar]
- Villalobos-Arias, M. Using generalized logistics regression to forecast population infected by Covid-19. arXiv 2020, arXiv:2004.02406. [Google Scholar]
- Batista, M. Estimation of the Final Size of The Second Phase of Coronavirus Epidemic by the Logistic Model. MedRxiv Prepr. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.03.11.20024901v2 (accessed on 19 January 2021).
- Jia, L.; Li, K.; Jiang, Y.; Guo, X. Prediction and analysis of Coronavirus Disease 2019. arXiv 2020, arXiv:2003.05447. [Google Scholar]
- Boccia, S.; Ricciardi, W.; Ioannidis, J.P. What other countries can learn from Italy during the COVID-19 pandemic. JAMA Intern. Med. 2020, 180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lilleri, D.; Zavaglio, F.; Gabanti, E.; Gerna, G.; Arbustini, E. Analysis of the SARS-CoV-2 epidemic in Italy: The role of local and interventional factors in the control of the epidemic. PLoS ONE 2020, 15, e0242305. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Júnior, L.C.; Bomfim, E.; da Silveira, D.S.C.; Pessanha, R.M.; Schuab, S.I.P.C.; Lima, R.A.G. Effectiveness of mass testing for control of COVID-19: A systematic review protocol. BMJ Open 2020, 10, e040413. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, F.L.; Bacigalupo, I.; Salvi, E.; Lacorte, E.; Piscopo, P.; Mayer, F.; Ancidoni, A.; Remoli, G.; Bellomo, G.; Losito, G.; et al. The Italian national survey on Coronavirus disease 2019 epidemic spread in nursing homes. Int. J. Geriatr. Psychiatry 2020. [Google Scholar] [CrossRef]
- Comas-Herrera, A.; Zalakaín, J.; Litwin, C.; Hsu, A.T.; Lane, N.; Fernández, J.L. Mortality Associated with COVID-19 Outbreaks in Care Homes: Early International Evidence. LTCcovid. org, International Long-Term Care Policy Network. Available online: https://ltccovid.org/wp-content/uploads/2020/04/Mortality-associated-with-COVID-12-April-4.pdf (accessed on 19 January 2021).
- Pesaresi, F. Il Covid-19 Nelle Strutture Residenziali Per Anziani. 2020. Available online: https://www.luoghicura.it/dati-e-tendenze/2020/05/ il-covid-19-nelle-strutture-residenziali-per-anziani/ (accessed on 19 January 2021).
- Pecoraro, F.; Clemente, F.; Luzi, D. The efficiency in the ordinary hospital bed management in Italy: An in-depth analysis of intensive care unit in the areas affected by COVID-19 before the outbreak. PLoS ONE 2020, 15, e0239249. [Google Scholar] [CrossRef] [PubMed]
- Rozanova, L.; Temerev, A.; Flahault, A. Comparing the Scope and Efficacy of COVID-19 Response Strategies in 16 Countries: An Overview. Int. J. Environ. Res. Public Health. 2020, 17, 9421. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, C.; Odone, A.; Gianfredi, V.; Bossi, E.; Bucci, D.; Oradini-Alacreu, A.; Frascella, B.; Capraro, M.; Chiappa, F.; Blandi, L.; et al. The spread of COVID-19 in six western metropolitan regions: A false myth on the excess of mortality in Lombardy and the defense of the city of Milan. Acta Biomed. 2020, 91, 23–30. [Google Scholar] [PubMed]
- Ortenzi, F.; Albanese, E.; Fadda, M.A. Transdisciplinary Analysis of COVID-19 in Italy: The Most Affected Country in Europe. Int. J. Environ. Res. Public Health. 2020, 17, 9488. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, F.; Luzi, D.; Clemente, F. The efficiency in the ordinary hospital bed management: A comparative analysis in four European countries before the COVID-19 outbreak. PLoS ONE 2021, accepted. [Google Scholar]
- Shah, A.S.; Wood, R.; Gribben, C.; Caldwell, D.; Bishop, J.; Weir, A.; Kennedy, S.; Reid, M.; Smith-Palmer, A.; Goldberg, D.; et al. Risk of hospital admission with coronavirus disease 2019 in healthcare workers and their households: Nationwide linkage cohort study. BMJ 2020, 371. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.Y.; Lo, E.S.; Huang, Z.; Kim, J.H.; Hung, H.; Hung, K.K.; Wong, E.L.; Wong, S.Y.; Gobat, N. Characteristics and well-being of urban informal home care providers during COVID-19 pandemic: A population-based study. BMJ Open 2020, 10, e041191. [Google Scholar] [CrossRef] [PubMed]
- Anelli, S.; Baratta, C.; Barberini, E.; Gargiulo, G.; Lucarini, S.; Pecoraro, F.; Clemente, F. COVID-19 emergency: Study of the hospitalization system and responses in organizational models in different Italian regions. Smart eLAB. 2020, 15, 1–16. (In Italia) [Google Scholar] [CrossRef]



| Region | Start: End Day | Ward (Days) | ICU (Days) | Home (Days) | Ward/Home (Days) | Active | Deaths | Recoveries | Total Cases |
|---|---|---|---|---|---|---|---|---|---|
| Emilia Romagna | 1:19 | 21.16 (144.18) | 2.88 (19.43) | 21.14 (142.51) | 1.00 (1.01) | 45.18 | 4.52 | 1.15 | 50.85 |
| Lombardia | 1:16 | 33.1 (161.01) | 4.65 (30.55) | 6.4 (63.97) | 5.17 (2.52) | 44.15 | 4.67 | 8.94 | 57.76 |
| Veneto | 1:20 | 7.46 (52.14) | 2.43 (15.33) | 26.29 (149.97) | 0.28 (0.35) | 36.18 | 1.12 | 2.18 | 39.48 |
| Emilia Romagna | 20:35 | 63.52 (875.38) | 4.6 (93.65) | 123.4 (1256.21) | 0.51 (0.70) | 191.52 | 27.9 | 24.49 | 243.91 |
| Lombardia | 17:34 | 78.11 (1377.51) | 8.5 (176.69) | 113.65 (1131.25) | 0.69 (1.22) | 200.26 | 54.61 | 80.43 | 335.3 |
| Veneto | 21:37 | 26.78 (390.50) | 4.83 (93.27) | 92.21 (1225.38) | 0.29 (0.32) | 123.82 | 8.6 | 14.7 | 147.12 |
| Emilia Romagna | 36:51 | −6.65 (1339.63) | −0.11 (127.66) | 79.62 (3098.27) | −0.08 (0.43) | 72.86 | 28.36 | 70.28 | 171.5 |
| Lombardia | 35:51 | 9.23 (2014.93) | −1.96 (215.97) | 71.06 (2540.64) | 0.13 (0.79) | 78.32 | 51.83 | 88.35 | 218.51 |
| Veneto | 38:54 | −6.54 (535.25) | −3.24 (96.22) | 66.2 (2839.70) | −0.10 (0.19) | 56.42 | 11.19 | 59.14 | 126.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pecoraro, F.; Luzi, D.; Clemente, F. Analysis of the Different Approaches Adopted in the Italian Regions to Care for Patients Affected by COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 848. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030848
Pecoraro F, Luzi D, Clemente F. Analysis of the Different Approaches Adopted in the Italian Regions to Care for Patients Affected by COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(3):848. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030848
Chicago/Turabian StylePecoraro, Fabrizio, Daniela Luzi, and Fabrizio Clemente. 2021. "Analysis of the Different Approaches Adopted in the Italian Regions to Care for Patients Affected by COVID-19" International Journal of Environmental Research and Public Health 18, no. 3: 848. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030848