
The Association between Maternal Experiences of Interpersonal Discrimination and Adverse Birth Outcomes: A Systematic Review of the Evidence


Abstract
:1. Introduction
1.1. Background
1.2. Rationale
- To facilitate, through our review of the evidence, a greater understanding and awareness of the extent to which discrimination “gets under the skin” of minority women and their offspring, eroding their physical health and wellbeing.
- To push this topic to the fore not only in research endeavors, but also importantly in applied health care settings. Specifically, we argue that maternal experiences of discrimination may be operationalized as a risk factor in prenatal and postpartum care and underscores the need for care approaches designed to mitigate the health repercussions associated with discrimination.
2. Materials and Methods
2.1. Protocol
2.2. Literature Search Strategy
- The paper reported empirical studies on the relationship between the maternal experience of interpersonal discrimination and pregnancy- and/or birth-related outcomes.
- The paper reported quantitative results.
- The paper was in English.
- The full text was available.
- The paper had undergone scientific peer review.
2.3. Research Quality Appraisal
3. Results
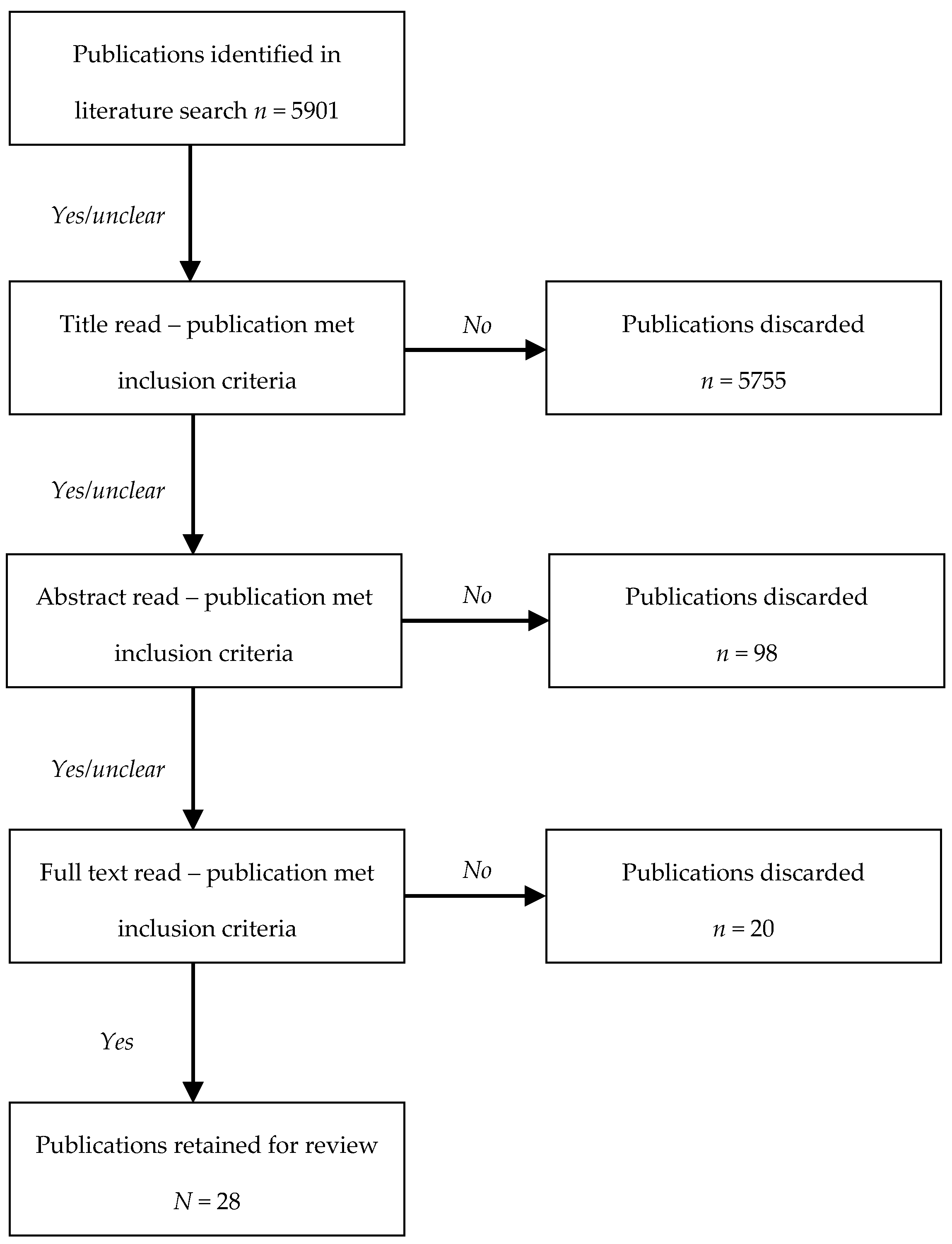
3.1. Literature Search Results
3.2. Study Characteristics and Methodology
3.3. Research Methodology and Quality
3.4. Study Findings
3.4.1. Maternal Experiences of Interpersonal Discrimination and Infant Gestational Age at Birth
3.4.2. Maternal Experiences of Interpersonal Discrimination and Infant Birth Weight
3.4.3. Maternal Experiences of Interpersonal Discrimination and Physiological Pregnancy Outcomes
3.4.4. Preliminary Process Model
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Theoretical, Social, and Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Allen, A.M.; Thomas, M.D.; Michaels, E.K.; Reeves, A.N.; Okoye, U.; Price, M.M.; Hasson, R.E.; Syme, S.L.; Chae, D.H. Racial discrimination, educational attainment, and biological dysregulation among midlife African American women. Psychoneuroendocrinology 2019, 99, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Dailey, D.E. Social stressors and strengths as predictors of infant birth weight in low-income African American women. Nurs. Res. 2009, 58, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Dixon, B.; Rifas-Shiman, S.L.; James-Todd, T.; Ertel, K.; Krieger, N.; Kleinman, K.P.; Rich-Edwards, J.W.; Gillman, M.W.; Taveras, E.M. Maternal experiences of racial discrimination and child weight status in the first 3 years of life. J. Dev. Orig. Health Dis. 2012, 3, 433–441. [Google Scholar] [CrossRef]
- Dominguez, T.P.; Dunkel-Schetter, C.; Glynn, L.M.; Hobel, C.; Sandman, C.A. Racial differences in birth outcomes: The role of general, pregnancy, and racism stress. Health Psychol. 2008, 27, 194–203. [Google Scholar] [CrossRef] [Green Version]
- Olson, D.M.; Severson, E.M.; Verstraeten, B.S.; Ng, J.W.; McCreary, J.K.; Metz, G.A. Allostatic load and preterm birth. Int. J. Mol. Sci. 2015, 16, 29856–29874. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, E.A.; Smart Richman, L. Perceived discrimination and health: A meta-analytic review. Psychol. Bull. 2009, 135, 531–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thayer, Z.; Bécares, L.; Carr, P.A. Maternal experiences of ethnic discrimination and subsequent birth outcomes in Aotearoa New Zealand. BMC Public Health 2019, 19, 1271. [Google Scholar] [CrossRef]
- Shah, P.S.; Zao, J.; Al-Wassia, H.; Shah, V. Pregnancy and neonatal outcomes of aboriginal women: A systematic review and meta-analysis. Women’s Health Issues 2011, 21, 28–39. [Google Scholar] [CrossRef]
- UNICEF. Low Birthweight-A Good Life Starts in the Womb. Available online: https://datauniceforg/topic/nutrition/low-birthweight/ (accessed on 7 September 2020).
- WHO. Preterm Birth. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 1 October 2020).
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Shapiro-Mendoza, C.K.; Barfield, W.D.; Henderson, Z.; James, A.; Howse, J.L.; Iskander, J.; Thorpe, P.G. CDC grand rounds: Public health strategies to prevent preterm birth. Morb. Mortal. Wkly. Rep. 2016, 65, 826–830. [Google Scholar] [CrossRef]
- Giurgescu, C.; McFarlin, B.L.; Lomax, J.; Craddock, C.; Albrecht, A. Racial discrimination and the Black-White gap in adverse birth outcomes: A review. J. Midwifery Women’s Health 2011, 56, 362–370. [Google Scholar] [CrossRef] [Green Version]
- Mantell, C.D.; Craig, E.D.; Stewart, A.W.; Ekeroma, A.J.; Mitchell, E.A. Ethnicity and birth outcome: New Zealand trends 1980–2001: Part 2. Pregnancy outcomes for Maori women. Aust. N. Z. J. Obstet. Gynaecol. 2004, 44, 537–540. [Google Scholar] [CrossRef]
- Blumenshine, P.; Egerter, S.; Barclay, C.J.; Cubbin, C.; Braveman, P.A. Socioeconomic disparities in adverse birth outcomes: A systematic review. Am. J. Prev. Med. 2010, 39, 263–272. [Google Scholar] [CrossRef]
- CDC. Preterm Birth. Available online: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm (accessed on 9 September 2020).
- Rich-Edwards, J.W.; Grizzard, T.A. Psychosocial stress and neuroendocrine mechanisms in preterm delivery. Am. J. Obstet. Gynecol. 2005, 192, S30–S35. [Google Scholar] [CrossRef]
- McEwen, B.S. Allostasis and allostatic load: Implications for neuropsychopharmacology. Neuropsychopharmacology 2000, 22, 108–124. [Google Scholar] [CrossRef]
- Beckie, T.M. A systematic review of allostatic load, health, and health disparities. Biol. Res. Nurs. 2012, 14, 311–346. [Google Scholar] [CrossRef]
- Black, P.H.; Garbutt, L.D. Stress, inflammation and cardiovascular disease. J. Psychosom. Res. 2002, 52, 1–23. [Google Scholar] [CrossRef]
- McEwen, B.S.; Stellar, E. Stress and the individual: Mechanisms leading to disease. Arch. Intern. Med. 1993, 153, 2093–2101. [Google Scholar] [CrossRef] [PubMed]
- Hux, V.J.; Catov, J.M.; Roberts, J.M. Allostatic load in women with a history of low birth weight infants: The national health and nutrition examination survey. J. Women’s Health 2014, 23, 1039–1045. [Google Scholar] [CrossRef] [Green Version]
- Hux, V.J.; Roberts, J.M. A potential role for allostatic load in preeclampsia. Matern. Child Health J. 2015, 19, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominguez, T.P. Adverse birth outcomes in African American women: The social context of persistent reproductive disadvantage. Soc. Work Public Health 2011, 26, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Giscombé, C.L.; Lobel, M. Explaining disproportionately high rates of adverse birth outcomes among African Americans: The impact of stress, racism, and related factors in pregnancy. Psychol. Bull. 2005, 131, 662. [Google Scholar] [CrossRef] [PubMed]
- Giurgescu, C.; Misra, D.P. Psychosocial factors and preterm birth among black mothers and fathers. MCN Am. J. Matern. Child Nurs. 2018, 43, 245–251. [Google Scholar] [CrossRef]
- Alhusen, J.L.; Bower, K.M.; Epstein, E.; Sharps, P. Racial discrimination and adverse birth outcomes: An integrative review. J. Midwifery Women’s Health 2016, 61, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Mutambudzi, M.; Meyer, J.D.; Reisine, S.; Warren, N. A review of recent literature on materialist and psychosocial models for racial and ethnic disparities in birth outcomes in the US, 2000–2014. Ethn. Health 2017, 22, 311–332. [Google Scholar] [CrossRef]
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid.-Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Dole, N.; Savitz, D.A.; Hertz-Picciotto, I.; Siega-Riz, A.M.; McMahon, M.J.; Buekens, P. Maternal stress and preterm birth. Am. J. Epidemiol. 2003, 157, 14–24. [Google Scholar] [CrossRef]
- Dole, N.; Savitz, D.A.; Siega-Riz, A.M.; Hertz-Picciotto, I.; McMahon, M.J.; Buekens, P. Psychosocial factors and preterm birth among African American and White women in central North Carolina. Am. J. Public Health 2004, 94, 1358–1365. [Google Scholar] [CrossRef]
- Krieger, N.; Smith, K.; Naishadham, D.; Hartman, C.; Barbeau, E.M. Experiences of discrimination: Validity and reliability of a self-report measure for population health research on racism and health. Soc. Sci. Med. 2005, 61, 1576–1596. [Google Scholar] [CrossRef] [Green Version]
- Christian, L.M.; Iams, J.D.; Porter, K.; Glaser, R. Epstein-Barr virus reactivation during pregnancy and postpartum: Effects of race and racial discrimination. Brain Behav. Immun. 2012, 26, 1280–1287. [Google Scholar] [CrossRef] [Green Version]
- Collins, J.W., Jr.; David, R.J.; Handler, A.; Wall, S.; Andes, S. Very low birthweight in African American infants: The role of maternal exposure to interpersonal racial discrimination. Am. J. Public Health 2004, 94, 2132–2138. [Google Scholar] [CrossRef]
- Collins, J.W., Jr.; David, R.J.; Symons, R.; Handler, A.; Wall, S.N.; Dwyer, L. Low-income African-American mothers’ perception of exposure to racial discrimination and infant birth weight. Epidemiology 2000, 11, 337–339. [Google Scholar] [CrossRef]
- Gillespie, S.L.; Anderson, C.M. Racial discrimination and leukocyte glucocorticoid sensitivity: Implications for birth timing. Soc. Sci. Med. 2018, 216, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Giurgescu, C.; Zenk, S.N.; Dancy, B.L.; Park, C.G.; Dieber, W.; Block, R. Relationships among neighborhood environment, racial discrimination, psychological distress, and preterm birth in African American women. J. Obstet. Gynecol. Neonatal Nurs. 2012, 41, E51–E61. [Google Scholar] [CrossRef] [Green Version]
- Grobman, W.A.; Parker, C.B.; Willinger, M.; Wing, D.A.; Silver, R.M.; Wapner, R.J.; Simhan, H.N.; Parry, S.; Mercer, B.M.; Haas, D.M. Racial disparities in adverse pregnancy outcomes and psychosocial stress. Obstet. Gynecol 2018, 131, 328–335. [Google Scholar] [CrossRef]
- Hilmert, C.J.; Dominguez, T.P.; Schetter, C.D.; Srinivas, S.K.; Glynn, L.M.; Hobel, C.J.; Sandman, C.A. Lifetime racism and blood pressure changes during pregnancy: Implications for fetal growth. Health Psychol. 2014, 33, 43. [Google Scholar] [CrossRef] [Green Version]
- Lespinasse, A.A.; David, R.J.; Collins, J.W.; Handler, A.S.; Wall, S.N. Maternal support in the delivery room and birthweight among African-American women. J. Natl. Med. Assoc. 2004, 96, 187–195. [Google Scholar] [PubMed]
- Mustillo, S.; Krieger, N.; Gunderson, E.P.; Sidney, S.; McCreath, H.; Kiefe, C.I. Self-reported experiences of racial discrimination and Black–White differences in preterm and low-birthweight deliveries: The CARDIA Study. Am. J. Public Health 2004, 94, 2125–2131. [Google Scholar] [CrossRef]
- Williams, D.R.; Yu, Y.; Jackson, J.S.; Anderson, N.B. Racial differences in physical and mental health: Socio-economic status, stress and discrimination. J. Health Psychol. 1997, 2, 335–351. [Google Scholar] [CrossRef] [Green Version]
- Carty, D.C.; Kruger, D.J.; Turner, T.M.; Campbell, B.; DeLoney, E.H.; Lewis, E.Y. Racism, health status, and birth outcomes: Results of a participatory community-based intervention and health survey. J. Urban Health 2011, 88, 84–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniels, K.P.; Zulema, V.; Chae, D.H.; Allen, A.M. Direct and vicarious racial discrimination at three life stages and preterm labor: Results from the African American Women’s Heart & Health Study. Matern. Child Health J. 2020, 24, 1387. [Google Scholar] [PubMed]
- Earnshaw, V.A.; Rosenthal, L.; Lewis, J.B.; Stasko, E.C.; Tobin, J.N.; Lewis, T.T.; Reid, A.E.; Ickovics, J.R. Maternal experiences with everyday discrimination and infant birth weight: A test of mediators and moderators among young, urban women of color. Ann. Behav. Med. 2013, 45, 13–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thayer, Z.M.; Kuzawa, C.W. Ethnic discrimination predicts poor self-rated health and cortisol in pregnancy: Insights from New Zealand. Soc. Sci. Med. 2015, 128, 36–42. [Google Scholar] [CrossRef]
- Misra, D.; Strobino, D.; Trabert, B. Effects of social and psychosocial factors on risk of preterm birth in black women. Paediatr. Perinat. Epidemiol. 2010, 24, 546–554. [Google Scholar] [CrossRef]
- Slaughter-Acey, J.C.; Talley, L.M.; Stevenson, H.C.; Misra, D.P. Personal versus group experiences of racism and risk of delivering a small-for-gestational age infant in African American women: A life course perspective. J. Urban Health 2019, 96, 181–192. [Google Scholar] [CrossRef]
- Rankin, K.M.; David, R.J.; Collins, J.W., Jr. African American women’s exposure to interpersonal racial discrimination in public settings and preterm birth: The effect of coping behaviors. Ethn. Dis. 2011, 21, 370–376. [Google Scholar] [PubMed]
- Slaughter-Acey, J.C.; Sealy-Jefferson, S.; Helmkamp, L.; Caldwell, C.H.; Osypuk, T.L.; Platt, R.W.; Straughen, J.K.; Dailey-Okezie, R.K.; Abeysekara, P.; Misra, D.P. Racism in the form of micro aggressions and the risk of preterm birth among black women. Ann. Epidemiol. 2016, 26, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bower, K.M.; Geller, R.J.; Perrin, N.A.; Alhusen, J. Experiences of racism and preterm birth: Findings from a pregnancy risk assessment monitoring system, 2004 through 2012. Women’s Health Issues 2018, 28, 495–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendez, D.D.; Hogan, V.K.; Culhane, J.F. Institutional racism, neighborhood factors, stress, and preterm birth. Ethn. Health 2014, 19, 479–499. [Google Scholar] [CrossRef]
- Rosenberg, L.; Palmer, J.R.; Wise, L.A.; Horton, N.J.; Corwin, M.J. Perceptions of racial discrimination and the risk of preterm birth. Epidemiology 2002, 13, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Scholaske, L.; Brose, A.; Spallek, J.; Entringer, S. Perceived discrimination and risk of preterm birth among Turkish immigrant women in Germany. Soc. Sci. Med. 2019, 236, 112427. [Google Scholar] [CrossRef]
- Shiono, P.H.; Rauh, V.A.; Park, M.; Lederman, S.A.; Zuskar, D. Ethnic differences in birthweight: The role of lifestyle and other factors. Am. J. Public Health 1997, 87, 787–793. [Google Scholar] [CrossRef] [Green Version]
- Geronimus, A.T. The weathering hypothesis and the health of African-American women and infants: Evidence and speculations. Ethn. Dis. 1992, 2, 207–221. [Google Scholar]
- Haslam, C.; Jetten, J.; Cruwys, T.; Dingle, G.; Haslam, S.A. The New Psychology of Health: Unlocking the Social Cure; Routledge: London, UK, 2018. [Google Scholar]
- Major, B.; Dovidio, J.F.; Link, B.G. The Oxford Handbook of Stigma, Discrimination, and Health; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Brody, G.H.; Lei, M.K.; Chae, D.H.; Yu, T.; Kogan, S.M.; Beach, S.R. Perceived discrimination among African American adolescents and allostatic load: A longitudinal analysis with buffering effects. Child Dev. 2014, 85, 989–1002. [Google Scholar] [CrossRef] [Green Version]
- Chae, D.H.; Lincoln, K.D.; Adler, N.E.; Syme, S.L. Do experiences of racial discrimination predict cardiovascular disease among African American men? The moderating role of internalized negative racial group attitudes. Soc. Sci. Med. 2010, 71, 1182–1188. [Google Scholar] [CrossRef] [Green Version]
- Forsyth, J.; Schoenthaler, A.; Chaplin, W.F.; Ogedegbe, G.; Ravenell, J. Perceived discrimination and medication adherence in black hypertensive patients: The role of stress and depression. Psychosom. Med. 2014, 76, 229–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geronimus, A.T.; Hicken, M.; Keene, D.; Bound, J. “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. Am. J. Public Health 2006, 96, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Guyll, M.; Matthews, K.A.; Bromberger, J.T. Discrimination and unfair treatment: Relationship to cardiovascular reactivity among African American and European American women. Health Psychol. 2001, 20, 315. [Google Scholar] [CrossRef] [PubMed]
- Mays, V.M.; Cochran, S.D.; Barnes, N.W. Race, race-based discrimination, and health outcomes among African Americans. Annu. Rev. Psychol. 2007, 58, 201–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuru-Jeter, A.; Dominguez, T.P.; Hammond, W.P.; Leu, J.; Skaff, M.; Egerter, S.; Jones, C.P.; Braveman, P. “It’s the skin you’re in”: African-American women talk about their experiences of racism. An exploratory study to develop measures of racism for birth outcome studies. Matern. Child Health J. 2009, 13, 29. [Google Scholar] [CrossRef]
- Braveman, P.; Heck, K.; Egerter, S.; Dominguez, T.P.; Rinki, C.; Marchi, K.S.; Curtis, M. Worry about racial discrimination: A missing piece of the puzzle of Black-White disparities in preterm birth? PLoS ONE 2017, 12, e0186151. [Google Scholar] [CrossRef]
- Brown-Iannuzzi, J.L.; Hoffman, K.M.; Payne, B.K.; Trawalter, S. The invisible man: Interpersonal goals moderate inattentional blindness to African Americans. J. Exp. Psychol. Gen. 2014, 143, 33. [Google Scholar] [CrossRef] [Green Version]
- Franklin, A.J.; Boyd-Franklin, N. Invisibility syndrome: A clinical model of the effects of racism on African-American males. Am. J. Orthopsychiatry 2000, 70, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Smart Richman, L.; Leary, M.R. Reactions to discrimination, stigmatization, ostracism, and other forms of interpersonal rejection: A multimotive model. Psychol. Rev. 2009, 116, 365. [Google Scholar] [CrossRef] [PubMed]
- Torres-Harding, S.; Turner, T. Assessing racial microaggression distress in a diverse sample. Eval. Health Prof. 2015, 38, 464–490. [Google Scholar] [CrossRef] [PubMed]
- Sutton, A.J. Publication bias. In The Handbook of Research Synthesis and Meta-Analysis, 2nd ed.; Russell Sage Foundation: New York, NY, USA, 2009; pp. 435–452. [Google Scholar]
- Simons, R.L.; Lei, M.; Beach, S.R.H.; Barr, A.B.; Simons, L.G.; Gibbons, F.X.; Philibert, R.A. Discrimination, segregation, and chronic inflammation: Testing the weathering explanation for the poor health of Black Americans. Dev. Psychol. 2018, 54, 1993–2006. [Google Scholar] [CrossRef] [PubMed]
- Schmeer, K.K.; Tarrence, J. Racial-ethnic disparities in inflammation: Evidence of weathering in childhood? J. Health Soc. Behav. 2018, 59, 411–428. [Google Scholar] [CrossRef]
- Forde, A.T.; Crookes, D.M.; Suglia, S.F.; Demmer, R.T. The weathering hypothesis as an explanation for racial disparities in health: A systematic review. Ann. Epidemiol. 2019, 33, 1–18. [Google Scholar] [CrossRef]
- Turner, R.N.; West, K. Behavioural consequences of imagining intergroup contact with stigmatized outgroups. Group Process. Intergroup Relat. 2012, 15, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Bailey, Z.D.; Krieger, N.; Agénor, M.; Graves, J.; Linos, N.; Bassett, M.T. Structural racism and health inequities in the USA: Evidence and interventions. Lancet 2017, 389, 1453–1463. [Google Scholar] [CrossRef]
- Visionary Vanguard Group Inc. The JJ Way®: Community-Based Maternity Center, Final Evaluation Report; Commonsense Childbirth: Winter Garden, FL, USA, 2017; Available online: http://www.commonsensechildbirth.org/wp-content/uploads/2019/07/The-JJ-Way%C2%AE-Community-based-Maternity-Center-Evaluation-Report-2017-1.pdf (accessed on 4 February 2021).
- Larrabee Sonderlund, A.; Thilsing, T.; Sondergaard, J. Should social disconnectedness be included in primary-care screening for cardiometabolic disease? A systematic review of the relationship between everyday stress, social connectedness, and allostatic load. PLoS ONE 2019, 14, 1–22. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Location | Population (N) | Research Design | Discrimination Measure (Scale Name) | Covariates | Outcome Variables | Findings | Research Quality |
|---|---|---|---|---|---|---|---|---|
| Bower et al. (2018) [51] | 12 states, USA | Non-Hispanic Black mothers (N = 11,582). | Cross-sectional |
|
|
|
| Moderate |
| Carty et al. (2011) [43] | Saginaw County, MI, USA | Mothers (N = 629, Black n = 407, White n = 222). | Cross-sectional |
|
|
|
| Moderate |
| Christian et al. (2012) [33] | OH, USA | Pregnant women (N = 56, Black n = 38, White n = 18). | Longitudinal |
|
|
|
| Moderate |
| Collins et al. (2000) [35] | Chicago, IL, USA | Black women (N = 85). Mothers of very-low-birth-weight (VLBW) children (n = 25) vs. mothers of healthy-weight children (n = 60). | Case-control study. |
|
|
|
| Moderate |
| Collins et al. (2004) [34] | Chicago, IL, USA | Black women (N = 312). Mothers of VLBW children (n = 104) vs. mothers of normal-weight children (n = 208). | Case-control study. |
|
|
|
| Moderate |
| Daiely et al. (2009) [2] | Northern CA, USA | Pregnant Black women (N = 108) | Prospective cohort study. |
|
|
|
| Moderate |
| Daniels et al. (In press) [44] | San Francisco Bay Area, CA, USA | Black women (N = 173) | Cross-sectional |
|
|
|
| Moderate |
| Dixon et al. (2012) [3] | Eastern MA, USA | Mother-infant pairs (N = 539; Black n = 294, Hispanic n = 127, Asian n = 110, Other n = 8) in Eastern MA. | Prospective cohort study. |
|
|
|
| Strong |
| Dole et al. (2003) [30] | Central NC, USA | Pregnant women (N = 1962; Black n = 707, White n = 1134, other n = 121). | Prospective cohort study. |
|
|
|
| Strong |
| Dole et al. (2004) [31] | Central NC, USA | Pregnant women (N = 1898; Black n = 727, White n = 1174). | Prospective cohort study. |
|
|
|
| Strong |
| Dominguez et al. (2008) [4] | Los Angeles, CA, USA | Pregnant women (N = 124; Black n = 51, White n = 73). | Prospective, repeated-measures observational study. |
|
|
|
| Moderate |
| Earnshaw et al. (2013) [45] | New York, NY, USA | Pregnant Black/Latina women (N = 420, Black n = 158, Latina n = 262). | Prospective cohort study. |
|
|
|
| Strong |
| Gillespie and Anderson (2018) [36] | OH, USA | Pregnant Black women (N = 96). | Prospective cohort study. |
|
|
|
| Moderate |
| Giurgescu et al. (2012) [37] | Chicago, IL, USA | Black mothers (N = 72). | Descriptive correlational comparative study. |
|
|
|
| Weak |
| Grobman et al. (2018) [38] | Nine states, USA | Pregnant women (N = 9470; Black n = 1307, White n = 5721, Hispanic n = 1586, Asian n = 379, other n = 477) | Cross-sectional study. |
|
|
|
| Moderate |
| Hilmert et al. (2014) [39] | Los Angeles and Orange counties, CA, USA | Pregnant Black women (N = 39). | Prospective cohort study. |
|
|
|
| Moderate |
| Lespinasse et al. (2004) [40] | Chicago, IL, USA | Black mothers of very-low-birth-weight infants (<1500 g) (n = 104) vs. healthy weight infants (approx. 2500 g) (n = 208). | Case-control study. |
|
|
|
| Strong |
| Mendez et al. (2014) [52] | Philadelphia, PA, USA | Pregnant women (N = 3462). | Cross-sectional study. |
|
|
|
| Weak |
| Misra et al. (2010) [47] | Baltimore, MD, USA | Pregnant Black women (N = 832). | Hybrid retrospective and prospective cohort study. |
|
|
|
| Strong |
| Mustillo et al. (2004) [41] | Birmingham, AL, Chicago, IL., Oakland, CA, Minneapolis, MN, USA | Pregnant women, Chicago, IL., Oakland, CA., Minneapolis, MN. (N = 352). | Prospective cohort study. |
|
|
|
| Strong |
| Rankin et al. (2011) [49] | Chiacgo, IL, USA | Black mothers (N = 277). | Case-control, repeated measures study. |
|
|
|
| Strong |
| Rosenberg et al. (2002) [53] | 12 states, USA | Non-Hispanic Black mothers (N = 4966). Mothers of preterm children (n = 422) and normal-term children (n = 4544). | Case-control study. |
|
|
|
| Strong |
| Scholaske et al. (2019) [54] | Germany | Non-immigrant German women (n = 2308) and Turkish immigrants (n = 217). | Longitudinal nation-wide panel study |
|
|
|
| Moderate |
| Shiono et al. (1997) [55] | Chicago, IL, and New York, NY, USA | Pregnant Black, Chinese, Dominican, Puerto Rican, Mexican, and White women (N = 1150). | Cross-sectional study. |
|
|
|
| Weak |
| Slaughter-Acey et al. (2016) [50] | Detroit, MI, USA | Black women (N = 1410). | Retrospective cohort study. |
|
|
|
| Strong |
| Slaughter-Acey et al. (2019) [48] | Baltimore, MD, USA | Black women (N = 778). | Hybrid retrospective and prospective cohort study. |
|
|
|
| Strong |
| Thayer et al. (2019) [7] | Aotearoa, New Zealand | Pregnant Māori (n = 510), Pacific (n = 452), Asian (n = 691) women (N = 1653). | Longitudinal cohort study. |
|
|
|
| Strong |
| Thayer and Kuzawa (2015) [46] | Auckland, New Zealand | Pregnant women (N = 64). | Prospective cohort study. |
|
|
|
| Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larrabee Sonderlund, A.; Schoenthaler, A.; Thilsing, T. The Association between Maternal Experiences of Interpersonal Discrimination and Adverse Birth Outcomes: A Systematic Review of the Evidence. Int. J. Environ. Res. Public Health 2021, 18, 1465. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041465
Larrabee Sonderlund A, Schoenthaler A, Thilsing T. The Association between Maternal Experiences of Interpersonal Discrimination and Adverse Birth Outcomes: A Systematic Review of the Evidence. International Journal of Environmental Research and Public Health. 2021; 18(4):1465. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041465
Chicago/Turabian StyleLarrabee Sonderlund, Anders, Antoinette Schoenthaler, and Trine Thilsing. 2021. "The Association between Maternal Experiences of Interpersonal Discrimination and Adverse Birth Outcomes: A Systematic Review of the Evidence" International Journal of Environmental Research and Public Health 18, no. 4: 1465. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041465