
Bibliometric Analysis on Research Trend of Accidental Falls in Older Adults by Using Citespace—Focused on Web of Science Core Collection (2010–2020)



Abstract
:1. Introduction
2. Method
2.1. Data Selected
2.2. Data Analysis Method
3. Result
3.1. Analysis Results and Visualization
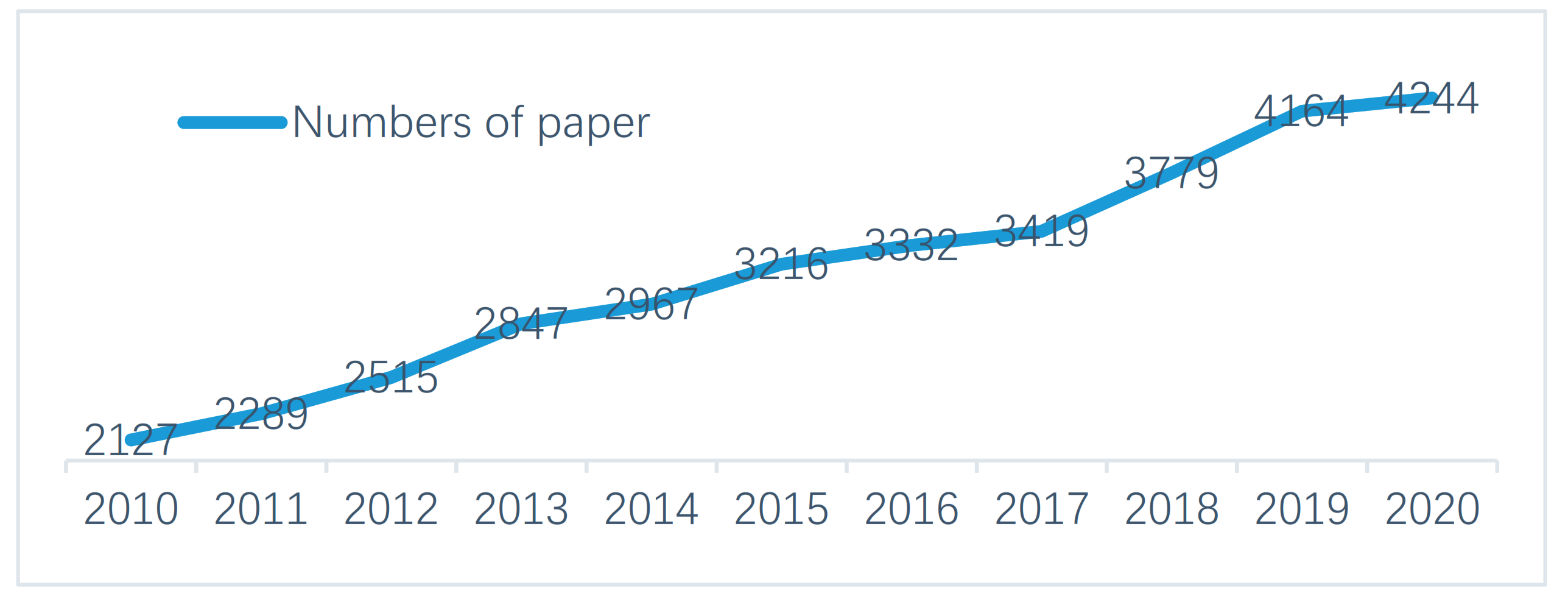
3.1.1. Basic Statistical Analysis
3.1.2. Distribution of Journal Papers
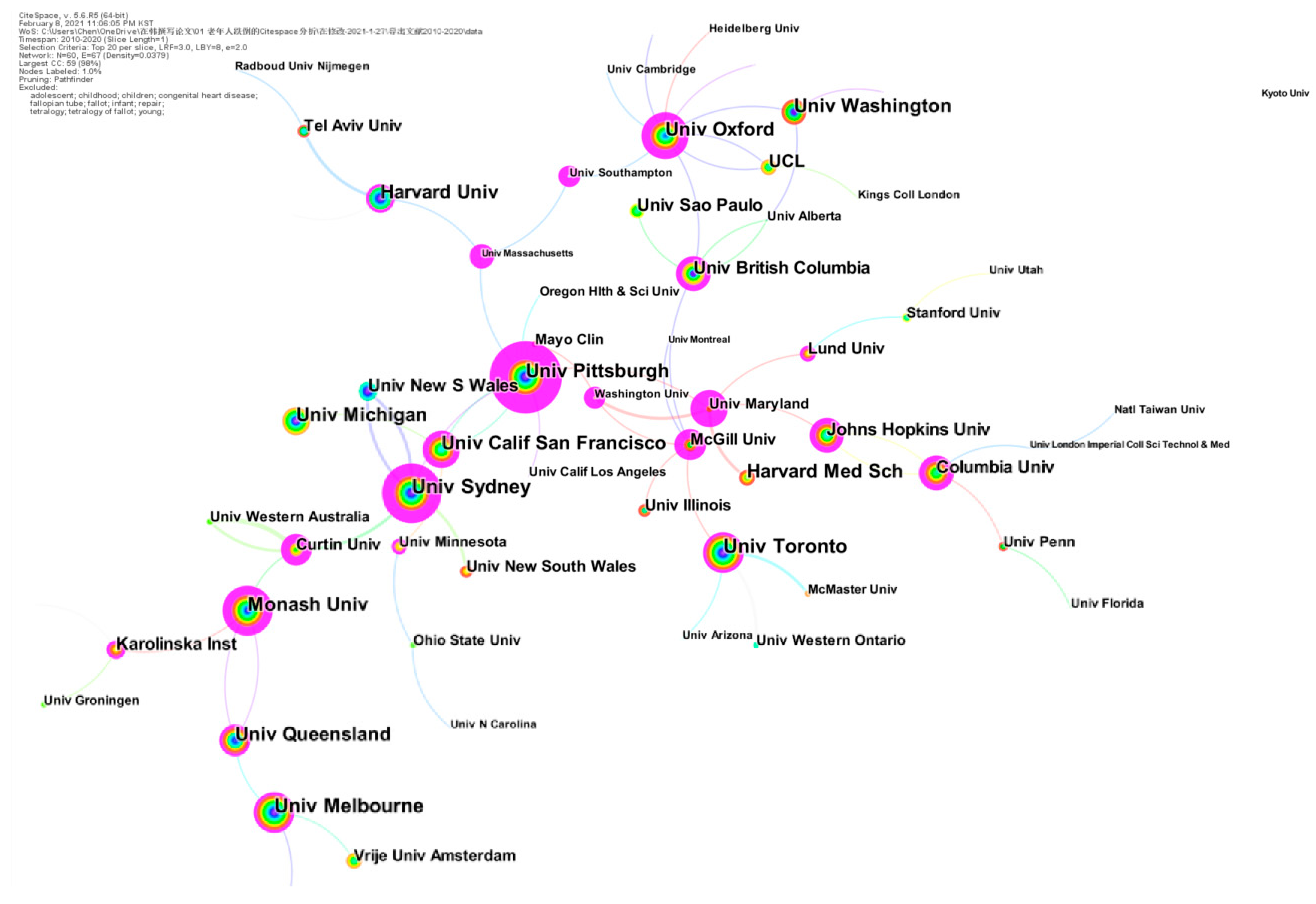
3.1.3. Co-Institution Analysis
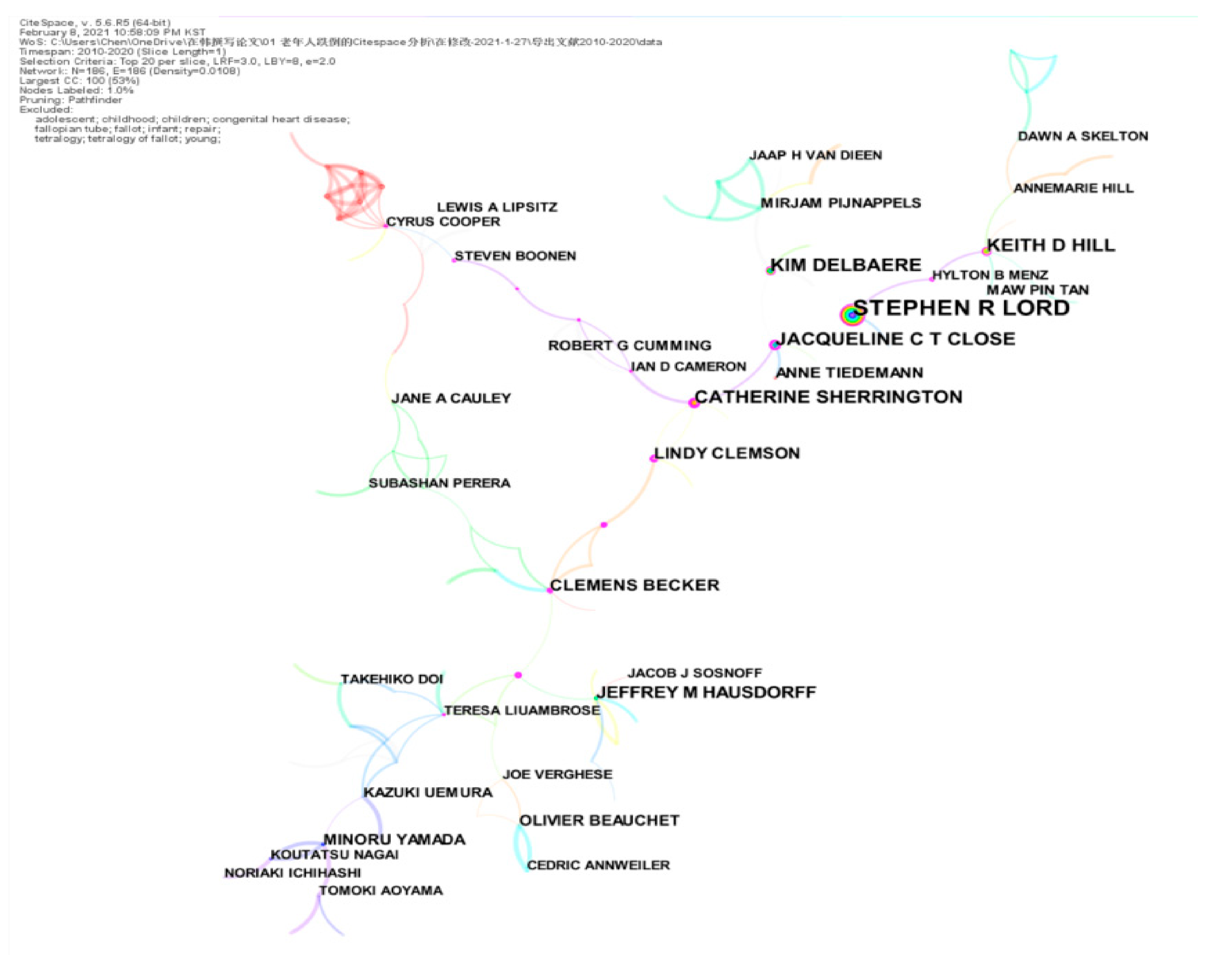
3.1.4. Co-Author Analysis
3.2. Keyword Cluster Analysis
3.2.1. Keyword Analysis
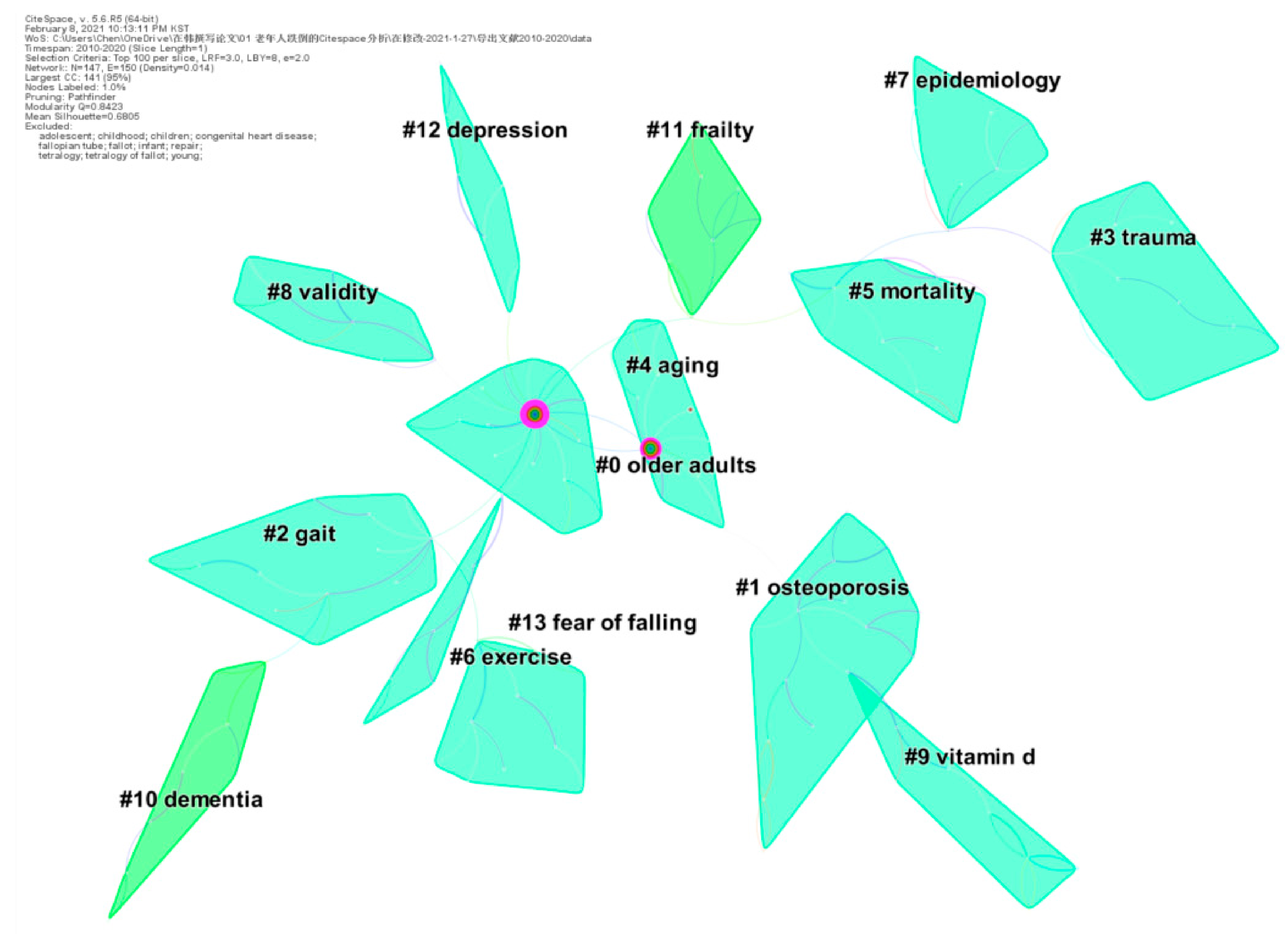
3.2.2. Keyword Cluster Analysis
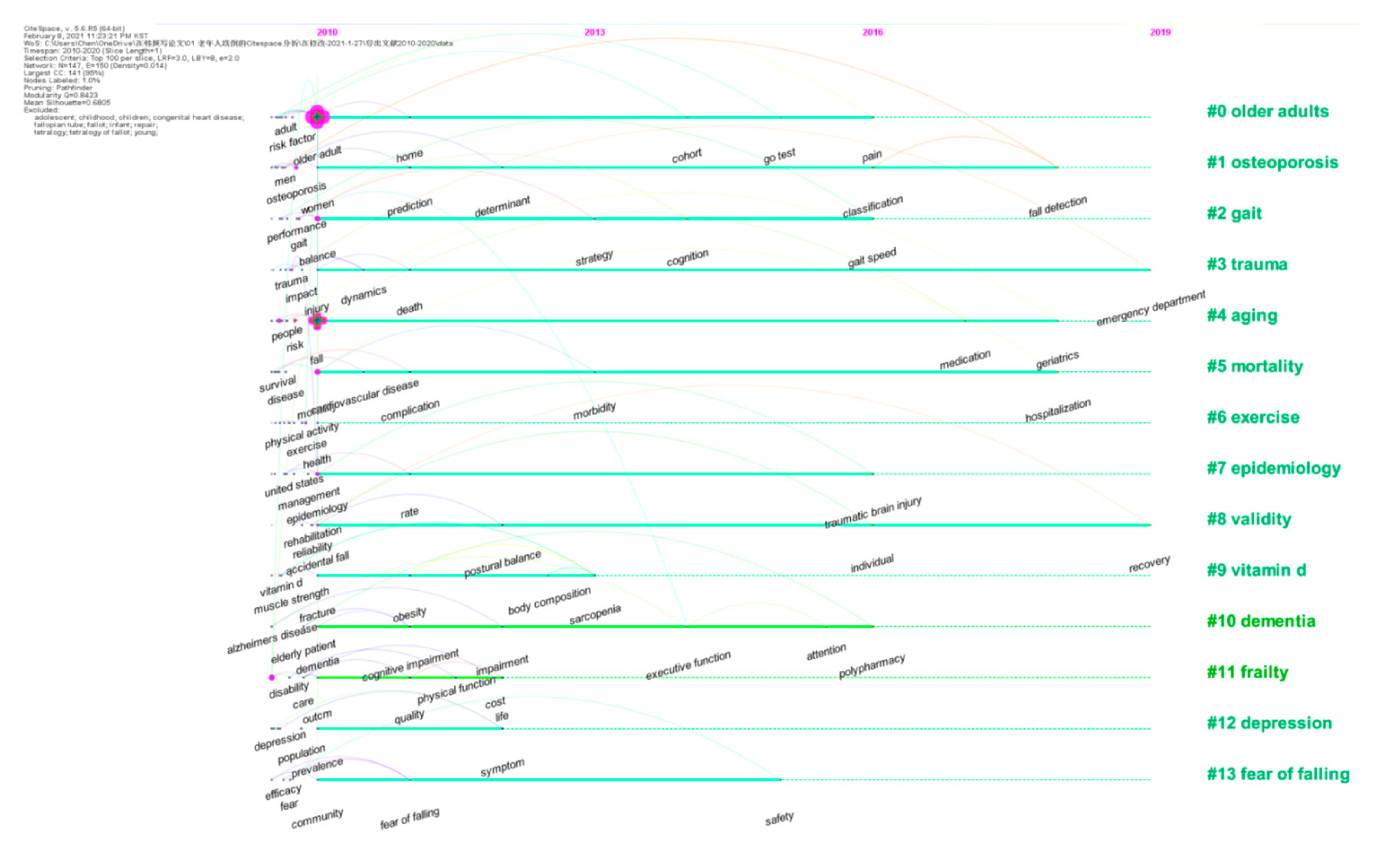
3.2.3. Research Hot Spots and Path Analysis
3.2.4. Keywords Citation Bursts Analysis
4. Discussion
4.1. Main Research Scholars’ Views
4.2. Main Clusters Analysis
4.3. Keywords Citation Bursts
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Web of Science Core Collection

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Set | Results | |
|---|---|---|
| #10 | 34,899 | #9 AND #6 |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #9 | 1,834,798 | #18 OR #17 |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #8 | 134,166 | TOPIC: (Elderly) AND DOCUMENT TYPES: (Article OR Review) AND LANGUAGE: (English) |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #7 | 1,784,189 | TOPIC: (Aged) AND DOCUMENT TYPES: (Article OR Review) AND LANGUAGE: (English) |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #6 | 181,751 | #5 OR #4 OR #3 OR #2 OR #1 |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #5 | 73 | TOPIC: ("Slip and Fall") AND DOCUMENT TYPES: (Article OR Review) AND LANGUAGE: (English) |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #4 | 3 | TOPIC: ("Fall and Slip") AND DOCUMENT TYPES: (Article OR Review) AND LANGUAGE: (English) |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #3 | 16 | TOPIC: ("Fall*, Accidental") AND DOCUMENT TYPES: (Article OR Review) AND LANGUAGE: (English) |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #2 | 181,751 | TOPIC: (Fall*) AND DOCUMENT TYPES: (Article OR Review) AND LANGUAGE: (English) |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 | ||
| #1 | 1704 | TOPIC: ("Accidental Fall*") AND DOCUMENT TYPES: (Article OR Review) AND LANGUAGE: (English) |
| Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC Timespan=2010-2020 |
Appendix B. PubMed
Appendix C. Embase
| Set | Results | |
|---|---|---|
| #8 | #3 AND #6 AND ([article]/lim OR [review]/lim) AND [english]/lim AND [humans]/lim AND [2010–2020]/py | 15,588 |
| #7 | #3 AND #6 | 33,343 |
| #6 | #4 OR #5 | 3,293,154 |
| #5 | ‘elderly’:ab,ti | 356,182 |
| #4 | ‘aged’/exp | 3,213,541 |
| #3 | #1 OR #2 | 90,715 |
| #2 | ‘falls’:ab,ti OR ‘accidental falls’:ab,ti OR ‘falls, accidental’:ab,ti OR ‘accidental fall’:ab,ti OR ‘fall, accidental’:ab,ti | 67,327 |
| #1 | ‘falling’/exp | 41,962 |
Appendix D. Scopus
References
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S.; Lancet Physical Activity Series Working, G. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Qato, D.M.; Wilder, J.; Schumm, L.P.; Gillet, V.; Alexander, G.C. Changes in prescription and over-the-counter medication and dietary supplement use among older adults in the United States, 2005 vs. 2011. JAMA Intern. Med. 2016, 176, 473–482. [Google Scholar] [CrossRef]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and Fall Injuries Among Adults Aged ≥ 65 Years—United States, 2014. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, 37–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boelens, C.; Hekman, E.E.G.; Verkerke, G.J. Risk factors for falls of older citizens. Technol. Health Care 2013, 21, 521–533. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. The medical costs of fatal falls and fall injuries among older adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, C.; Fairhall, N.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Sherrington, C. Exercise for falls prevention in community-dwelling older adults: Trial and participant characteristics, interventions and bias in clinical trials from a systematic review. BMJ Open Sport Exerc. Med. 2019, 5, e000663. [Google Scholar] [CrossRef] [Green Version]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1, CD012424. [Google Scholar] [CrossRef]
- Jianhua, H.; Zhigang, H. Review on the application of citespace at home and abroad. J. Mod. Inf. Ser. 2013, 33, 99–103. [Google Scholar]
- Chen, Y.; Chen, C.; Liu, Z.; Hu, Z.; Wang, X. The methodology function of CiteSpace mapping knowledge domains. Stud. Sci. Sci. 2015, 33, 242–253. [Google Scholar]
- Lord, S.R.; Delbaere, K.; Sturnieks, D.L. Aging. Handb. Clin. Neurol. 2018, 159, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M. Tailor-made programs for preventive falls. Jpn. J. Clin. Med. 2014, 72, 1821–1826. [Google Scholar]
- Rizzoli, R.; Stevenson, J.C.; Bauer, J.M.; van Loon, L.J.; Walrand, S.; Kanis, J.A.; Cooper, C.; Brandi, M.L.; Diez-Perez, A.; Reginster, J.Y.; et al. The role of dietary protein and vitamin D in maintaining musculoskeletal health in postmenopausal women: A consensus statement from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Maturitas 2014, 79, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Paintin, J.; Cooper, C.; Dennison, E. Osteosarcopenia. Br. J. Hosp. Med. (Lond.) 2018, 79, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.; Clemson, L.; Lovarini, M.; Willis, K.; Lord, S.R.; Sherrington, C. Cultural influences on exercise participation and fall prevention: A systematic review and narrative synthesis. Disabil. Rehabil. 2016, 38, 724–732. [Google Scholar] [CrossRef]
- Lee, D.C.; Day, L.; Hill, K.; Clemson, L.; McDermott, F.; Haines, T.P. What factors influence older adults to discuss falls with their health-care providers? Health Expect 2015, 18, 1593–1609. [Google Scholar] [CrossRef] [Green Version]
- Lord, S.R.; Close, J.C.T. New horizons in falls prevention. Age Ageing 2018, 47, 492–498. [Google Scholar] [CrossRef]
- Kayama, H.; Okamoto, K.; Nishiguchi, S.; Yamada, M.; Kuroda, T.; Aoyama, T. Effect of a Kinect-based exercise game on improving executive cognitive performance in community-dwelling elderly: Case control study. J Med. Internet Res. 2014, 16, e61. [Google Scholar] [CrossRef] [Green Version]
- Yamada, M.; Aoyama, T.; Hikita, Y.; Takamura, M.; Tanaka, Y.; Kajiwara, Y.; Nagai, K.; Uemura, K.; Mori, S.; Tanaka, B. Effects of a DVD-based seated dual-task stepping exercise on the fall risk factors among community-dwelling elderly adults. Telemed. J. E Health 2011, 17, 768–772. [Google Scholar] [CrossRef]
- Clemson, L.; Mackenzie, L.; Ballinger, C.; Close, J.C.; Cumming, R.G. Environmental interventions to prevent falls in community-dwelling older people: A meta-analysis of randomized trials. J. Aging Health 2008, 20, 954–971. [Google Scholar] [CrossRef]
- Da Silva, R.B.; Costa-Paiva, L.; Morais, S.S.; Mezzalira, R.; Ferreira Nde, O.; Pinto-Neto, A.M. Predictors of falls in women with and without osteoporosis. J. Orthop. Sports Phys. Ther. 2010, 40, 582–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, X.; Deng, H.; Shen, X.; Lei, Q. Effect of balance training on falls in patients with osteoporosis: A systematic review and meta-analysis. J. Rehabil. Med. 2018, 50, 577–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shier, V.; Trieu, E.; Ganz, D.A. Implementing exercise programs to prevent falls: Systematic descriptive review. Inj. Epidemiol. 2016, 3, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, P.D. Management of severe osteoporosis. Expert. Opin. Pharmacother. 2016, 17, 473–488. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, A.; Sudarsky, L. Balance and gait problems in the elderly. Handb. Clin. Neurol. 2012, 103, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Kyrdalen, I.L.; Thingstad, P.; Sandvik, L.; Ormstad, H. Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother. Res. Int. 2019, 24, e1743. [Google Scholar] [CrossRef] [Green Version]
- Montero-Odasso, M.; Sarquis-Adamson, Y.; Song, H.Y.; Bray, N.W.; Pieruccini-Faria, F.; Speechley, M. Polypharmacy, gait performance, and falls in community-dwelling older adults. Results from the Gait and Brain Study. J. Am. Geriatr. Soc. 2019, 67, 1182–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delbaere, K.; Close, J.C.; Mikolaizak, A.S.; Sachdev, P.S.; Brodaty, H.; Lord, S.R. The Falls Efficacy Scale International (FES-I). A comprehensive longitudinal validation study. Age Ageing 2010, 39, 210–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosscher, R.J.; Raymakers, E.R.; Trompe, E.A.; Smit, J.H. Fear of falling: Psychometric aspects of Tinetti’s Falls Efficacy Scale. Tijdschr. Gerontol. Geriatr. 2005, 36, 5–10. [Google Scholar] [CrossRef]
- Kumar, A.; Delbaere, K.; Zijlstra, G.A.; Carpenter, H.; Iliffe, S.; Masud, T.; Skelton, D.; Morris, R.; Kendrick, D. Exercise for reducing fear of falling in older people living in the community: Cochrane systematic review and meta-analysis. Age Ageing 2016, 45, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Qi, B.; Jin, S.; Qian, H.; Zou, Y. Bibliometric Analysis of Chronic Traumatic Encephalopathy Research from 1999 to 2019. Int. J. Environ. Res. Public Health 2020, 17, 5411. [Google Scholar] [CrossRef] [PubMed]
- Injury, G.B.D.T.B.; Spinal Cord Injury, C. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 56–87. [Google Scholar] [CrossRef] [Green Version]
- Stevens, J.A.; Corso, P.S.; Finkelstein, E.A.; Miller, T.R. The costs of fatal and non-fatal falls among older adults. Inj. Prev. 2006, 12, 290–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- VanItallie, T.B. Traumatic brain injury (TBI) in collision sports: Possible mechanisms of transformation into chronic traumatic encephalopathy (CTE). Metabolism 2019, 100, 153943. [Google Scholar] [CrossRef]
- Brown, C.V.; Ali, S.; Fairley, R.; Lai, B.K.; Arthrell, J.; Walker, M.; Tips, G. Risk factors for falls among hospitalized trauma patients. Am. Surg. 2013, 79, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Berkova, M.; Berka, Z. Falls: A significant cause of morbidity and mortality in elderly people. Vnitr. Lek. 2018, 64, 1076–1083. [Google Scholar] [PubMed]
- Cheng, P.; Wang, L.; Ning, P.; Yin, P.; Schwebel, D.C.; Liu, J.; Qi, J.; Hu, G.; Zhou, M. Unintentional falls mortality in China, 2006–2016. J. Glob. Health 2019, 9, 010603. [Google Scholar] [CrossRef]
- Hartholt, K.A.; Lee, R.; Burns, E.R.; van Beeck, E.F. Mortality from falls among us adults aged 75 years or older, 2000–2016. JAMA 2019, 321, 2131–2133. [Google Scholar] [CrossRef] [Green Version]
- Hartholt, K.A.; van Beeck, E.F.; van der Cammen, T.J.M. Mortality from falls in dutch adults 80 years and older, 2000–2016. JAMA 2018, 319, 1380–1382. [Google Scholar] [CrossRef]
- Padrón-Monedero, A.; Damián, J.; Pilar Martin, M.; Fernández-Cuenca, R. Mortality trends for accidental falls in older people in Spain, 2000–2015. BMC Geriatr. 2017, 17, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiadaliri, A.A.; Rosengren, B.E.; Englund, M. Fall-related mortality in southern Sweden: A multiple cause of death analysis, 1998–2014. Inj. Prev. 2019, 25, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, H.; Koyama, T.; Zamami, Y.; Tatebe, Y.; Funahashi, T.; Shinomiya, K.; Kitamura, Y.; Hinotsu, S.; Sendo, T.; Rakugi, H.; et al. Fall-related mortality trends in older Japanese adults aged ≥65 years: A nationwide observational study. BMJ Open 2019, 9, e033462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayalon, L. Satisfaction with aging results in reduced risk for falling. Int. Psychogeriatr. 2016, 28, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Tom, S.E.; Adachi, J.D.; Anderson, F.A., Jr.; Boonen, S.; Chapurlat, R.D.; Compston, J.E.; Cooper, C.; Gehlbach, S.H.; Greenspan, S.L.; Hooven, F.H.; et al. Frailty and fracture, disability, and falls: A multiple country study from the global longitudinal study of osteoporosis in women. J. Am. Geriatr. Soc. 2013, 61, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Frailty as a predictor of future falls among community-dwelling older people: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2015, 16, 1027–1033. [Google Scholar] [CrossRef]
- Clemson, L.; Fiatarone Singh, M.A.; Bundy, A.; Cumming, R.G.; Manollaras, K.; O’Loughlin, P.; Black, D. Integration of balance and strength training into daily life activity to reduce rate of falls in older people (the LiFE study): Randomised parallel trial. BMJ 2012, 345, e4547. [Google Scholar] [CrossRef] [Green Version]
- Mirelman, A.; Rochester, L.; Maidan, I.; Del Din, S.; Alcock, L.; Nieuwhof, F.; Rikkert, M.O.; Bloem, B.R.; Pelosin, E.; Avanzino, L.; et al. Addition of a non-immersive virtual reality component to treadmill training to reduce fall risk in older adults (V-TIME): A randomised controlled trial. Lancet 2016, 388, 1170–1182. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-García, J.D.; Hita-Contreras, F.; de la Torre-Cruz, M.; Fábrega-Cuadros, R.; Aibar-Almazán, A.; Cruz-Díaz, D.; Martínez-Amat, A. Risk of falls in healthy older adults: Benefits of high-intensity interval training using lower body suspension exercises. J. Aging Phys. Act. 2019, 27, 325–333. [Google Scholar] [CrossRef]
- Thomas, S.; Mackintosh, S.; Halbert, J. Does the ’Otago exercise programme’ reduce mortality and falls in older adults? A systematic review and meta-analysis. Age Ageing 2010, 39, 681–687. [Google Scholar] [CrossRef] [Green Version]
- Holroyd, C.R.; Cooper, C.; Harvey, N.C. Vitamin D and the postmenopausal population. Menopause Int. 2011, 17, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C. Vitamin D and falls—The dosage conundrum. Nat. Rev. Endocrinol. 2016, 12, 680–684. [Google Scholar] [CrossRef] [PubMed]
- Uusi-Rasi, K.; Patil, R.; Karinkanta, S.; Kannus, P.; Tokola, K.; Lamberg-Allardt, C.; Sievänen, H. Exercise and vitamin D in fall prevention among older women: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 703–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolland, M.J.; Grey, A.; Avenell, A. Effects of vitamin D supplementation on musculoskeletal health: A systematic review, meta-analysis, and trial sequential analysis. Lancet Diabetes Endocrinol. 2018, 6, 847–858. [Google Scholar] [CrossRef] [Green Version]
- Dennison, E.M.; Sayer, A.A.; Cooper, C. Epidemiology of sarcopenia and insight into possible therapeutic targets. Nat. Rev. Rheumatol. 2017, 13, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the european working group on sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Codes, I.-C. Sarcopenia. Available online: https://www.icd10data.com/ICD10CM/Codes/M00-M99/M60-M63/M62-/M62.84 (accessed on 1 October 2016).
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Orav, J.E.; Kanis, J.A.; Rizzoli, R.; Schlögl, M.; Staehelin, H.B.; Willett, W.C.; Dawson-Hughes, B. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos Int. 2015, 26, 2793–2802. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; van Schoor, N.M.; Lips, P.; Visser, M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: The longitudinal aging study amsterdam. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Cawthon, P.M.; Lui, L.Y.; Taylor, B.C.; McCulloch, C.E.; Cauley, J.A.; Lapidus, J.; Orwoll, E.; Ensrud, K.E. Clinical definitions of sarcopenia and risk of hospitalization in community-dwelling older men: The osteoporotic fractures in men study. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1383–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevitt, M.C.; Cummings, S.R. Type of fall and risk of hip and wrist fractures: The study of osteoporotic fractures. The Study of Osteoporotic Fractures Research Group. J. Am. Geriatr. Soc. 1993, 41, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Kulik, C. Components of a Comprehensive Fall-risk Assessment. In Special Supplement to American Nurse Today—Best Practices for Falls Reduction: A Practical Guide. 2011. Available online: http://www.americannursetoday.com/Article.aspx?id=7634&fid=7364. (accessed on 19 May 2014).
- Avanecean, D.; Calliste, D.; Contreras, T.; Lim, Y.; Fitzpatrick, A. Effectiveness of patient-centered interventions on falls in the acute care setting compared to usual care: A systematic review. JBI Database Syst. Rev. Implement Rep. 2017, 15, 3006–3048. [Google Scholar] [CrossRef] [PubMed]
- Toots, A.; Wiklund, R.; Littbrand, H.; Nordin, E.; Nordstrom, P.; Lundin-Olsson, L.; Gustafson, Y.; Rosendahl, E. The effects of exercise on falls in older people with dementia living in nursing homes: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2019, 20, 835–842.e1. [Google Scholar] [CrossRef] [Green Version]
- Peek, K.; Bryant, J.; Carey, M.; Dodd, N.; Freund, M.; Lawson, S.; Meyer, C. Reducing falls among people living with dementia: A systematic review. Dementia 2020, 19, 1621–1640. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Iaboni, A.; Flint, A.J. The complex interplay of depression and falls in older adults: A clinical review. Am. J. Geriatr. Psychiatry 2013, 21, 484–492. [Google Scholar] [CrossRef] [Green Version]
- Daly, R.M.; Dalla Via, J.; Duckham, R.L.; Fraser, S.F.; Helge, E.W. Exercise for the prevention of osteoporosis in postmenopausal women: An evidence-based guide to the optimal prescription. Braz. J. Phys. Ther. 2019, 23, 170–180. [Google Scholar] [CrossRef]
- Gia, T.N.; Sarker, V.K.; Tcarenko, I.; Rahmani, A.M.; Westerlund, T.; Liljeberg, P.; Tenhunen, H. Energy efficient wearable sensor node for IoT-based fall detection systems. Microprocess. Microsyst. 2018, 56, 34–46. [Google Scholar]
- Xu, T.; Zhou, Y.; Zhu, J. New advances and challenges of fall detection systems: A survey. Appl. Sci. 2018, 8, 418. [Google Scholar] [CrossRef] [Green Version]
- Malasinghe, L.P.; Ramzan, N.; Dahal, K. Remote patient monitoring: A comprehensive study. J. Ambient Intell. Humaniz. Comput. 2019, 10, 57–76. [Google Scholar] [CrossRef] [Green Version]
- Peel, N.M. Epidemiology of falls in older age. Can. J. Aging 2011, 30, 7–19. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Global Report on Falls Prevention in Older Age. Available online: https://www.who.int/ageing/publications/Falls_prevention7March.pdf?ua=1 (accessed on 23 December 2020).
- Wales, K.; Clemson, L.; Lannin, N.A.; Cameron, I.D.; Salked, G.; Gitlin, L.; Rubenstein, L.; Barras, S.; Mackenzie, L.; Davies, C. Occupational therapy discharge planning for older adults: A protocol for a randomised trial and economic evaluation. BMC Geriatr. 2012, 12, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gale, C.R.; Westbury, L.D.; Cooper, C.; Dennison, E.M. Risk factors for incident falls in older men and women: The English longitudinal study of ageing. BMC Geriatr. 2018, 18, 117. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Cooper, C.; Aihie Sayer, A. Prevalence and risk factors for falls in older men and women: The English Longitudinal Study of Ageing. Age Ageing 2016, 45, 789–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, J.A.; Ballesteros, M.F.; Mack, K.A.; Rudd, R.A.; DeCaro, E.; Adler, G. Gender differences in seeking care for falls in the aged Medicare population. Am. J. Prev. Med. 2012, 43, 59–62. [Google Scholar] [CrossRef]





| No. | Journal Title | IF | Amount | Country | Research Area |
|---|---|---|---|---|---|
| 1 | PLoS One | 2.740 | 609 | USA | Science & Technology-Other Topics (Q2) |
| 2 | Gait & Posture | 2.349 | 425 | Ireland | Neuroscience & Neurology (Q3) Orthopedics (Q2) Sport Sciences (Q2) |
| 3 | BMC Geriatrics | 3.077 | 366 | England | Geriatrics & Gerontology (Q2) |
| 4 | Journal of the American Geriatrics Society | 4.180 | 321 | USA | Geriatrics & Gerontology (Q1) |
| 5 | Archives of Gerontology and Geriatrics | 2.128 | 272 | Ireland | Geriatrics & Gerontology (Q3) |
| 6 | Osteoporosis International | 3.864 | 271 | England | Endocrinology & Metabolism (Q2) |
| 7 | Aging Clinical and Experimental Research | 2.697 | 264 | Italy | Geriatrics & Gerontology (Q3) |
| 8 | BMJ Open | 2.496 | 219 | England | General & Internal Medicine (Q2) |
| 9 | Journal of the American Medical Directors Association | 4.367 | 197 | USA | Geriatrics & Gerontology (Q1) |
| 10 | Age and Ageing | 4.902 | 196 | England | Geriatrics & Gerontology (Q1) |
| No. | Co-Authorship Papers | Burst | Centrality | Sigma |
|---|---|---|---|---|
| 1 | Stephen R Lord | Minoru Yamada | Cooper Cyrus | Catherine Sherrington |
| 2 | Kim Delbaere | Koutatsu Nagai | Mirjam Pijnappels | Clemens Becker |
| 3 | Catherine Sherrington | Kazuki Uemura | Teresa Liu-Ambrose | Jacqueline C T Close |
| 4 | Keith D Hill | Anne-Marie Hill | Keith D Hill | Jorunn L Helbostad |
| 5 | Jacqueline CT Close | Noriaki Ichihashi | Jeffrey M Hausdorff | Lindy Clemson |
| Researcher | H-Index | Sum of Cited | Research Areas |
|---|---|---|---|
| Cooper Cyrus | 144 | 106,019 | Osteoporosis & Osteoarthritis & Epidemiology |
| Stephen R Lord | 93 | 91,427 | Falls in Older People |
| Jeffrey M Hausdorff | 76 | 28,247 | Gait & Neurodynamic |
| Catherine Sherrington | 52 | 11,620 | Health & Exercise & falls & Ageing & Rehabilitation |
| Keith D Hill | 44 | 6778 | Falls prevention & Exercise & Rehabilitation |
| Teresa Liu-Ambrose | 41 | 5789 | Fall prevention & Healthy aging |
| Jacqueline C T Close | 40 | 6746 | Gait & Gerontology & Geriatric Assessment |
| Kim Delbaere | 38 | 4792 | Ageing & Accidental falls & Fear of falling & Cognitive function |
| Clemens Becker | 36 | 4654 | Falls & Exercise & Rehabilitation |
| Jorunn L Helbostad | 31 | 3476 | Movement disorders and falls at old age |
| Minoru Yamada | 28 | 2501 | Gerontology & Rehabilitation |
| Mirjam Pijnappels | 28 | 2787 | The effects of aging on neuromuscular and cognitive aspects of mobility |
| Noriaki Ichihashi | 26 | 2192 | Rehabilitation & Physical therapy |
| Lindy Clemson | 25 | 2972 | Ageing & Occupational Therapy |
| Kazuki Uemura | 23 | 1802 | Rehabilitation & Welfare engineering |
| Koutatsu Nagai | 17 | 816 | Gerontology & Physical Therapy |
| Anne-Marie Hill | 16 | 1043 | Falls prevention & Patient education |
| Clusters | Silhouette | Size | Log-Likelihood (LLR) |
|---|---|---|---|
| #0 older adults | 15 | 1 | Risk factor, mobility, pain, prevention, quality of life |
| #1 osteoporosis | 14 | 0.968 | Fall detection, bone mineral density, classification, machine learning, fracture, wearable sensors |
| #2 gait | 13 | 0.985 | Balance, walking, postural control, variability, parkinsons disease, gait analysis |
| #3 trauma | 12 | 0.966 | Injury, impact, emergency department, frailty, suicide |
| #4 aging | 11 | 1 | Hip fracture, falls, vitamin d supplementation, prescription, Romberg test |
| #5 mortality | 11 | 1 | Blood pressure, survival, surgery, hypertension, morbidity, disease |
| #6 exercise | 10 | 0.971 | Physical activity, health, intervention, randomized controlled trial, fitness, social participation |
| #7 epidemiology | 9 | 0.956 | Traumatic brain injury, management, trend, diagnosis, rehabilitation |
| #8 validity | 9 | 0.967 | Reliability, women health, knee pain, lower extremity, inertial sensors, practice guidelines |
| #9 vitamin d | 8 | 1 | Sarcopenia, fractures, physical performance, obesity, muscle strength, osteosarcopenia, |
| #10 dementia | 8 | 0.966 | Cognitive impairment, polypharmacy, motoric cognitive risk syndrome, attention, long-term care |
| #11 frailty | 8 | 0.952 | Care, quality, patient, comprehensive geriatric assessment, disability, |
| #12 depression | 7 | 0.96 | Prevalence, population, mental health, sleep quality, behavior, anxiety, |
| #13 fear of falling | 6 | 0.918 | Efficacy, safety, exercise, nurses, fear, physical activity monitoring |
| Keywords | Year | Strength | Begin | End | 2010–2020 |
|---|---|---|---|---|---|
| vitamin d | 2010 | 25.7615 | 2010 | 2013 | ▃▃▃▃▂▂▂▂▂▂▂ |
| infection | 2010 | 34.6606 | 2010 | 2012 | ▃▃▃▂▂▂▂▂▂▂▂ |
| double blind | 2010 | 22.0649 | 2010 | 2011 | ▃▃▂▂▂▂▂▂▂▂▂ |
| growth | 2010 | 4.5875 | 2010 | 2012 | ▃▃▃▂▂▂▂▂▂▂▂ |
| history | 2010 | 36.0171 | 2010 | 2013 | ▃▃▃▃▂▂▂▂▂▂▂ |
| community | 2010 | 10.2497 | 2010 | 2011 | ▃▃▂▂▂▂▂▂▂▂▂ |
| guideline | 2010 | 30.1278 | 2010 | 2013 | ▃▃▃▃▂▂▂▂▂▂▂ |
| hypertension | 2010 | 28.7127 | 2010 | 2015 | ▃▃▃▃▃▃▂▂▂▂▂ |
| randomized controlled trial | 2010 | 16.4364 | 2010 | 2011 | ▃▃▂▂▂▂▂▂▂▂▂ |
| older people | 2010 | 55.1187 | 2010 | 2014 | ▃▃▃▃▃▂▂▂▂▂▂ |
| postmenopausal women | 2010 | 16.4984 | 2010 | 2012 | ▃▃▃▂▂▂▂▂▂▂▂ |
| bone mineral density | 2010 | 2.6016 | 2010 | 2011 | ▃▃▂▂▂▂▂▂▂▂▂ |
| older women | 2010 | 31.0928 | 2010 | 2013 | ▃▃▃▃▂▂▂▂▂▂▂ |
| dynamics | 2010 | 26.5791 | 2011 | 2012 | ▂▃▃▂▂▂▂▂▂▂▂ |
| home | 2010 | 48.2979 | 2011 | 2014 | ▂▃▃▃▃▂▂▂▂▂▂ |
| follow up | 2010 | 16.818 | 2012 | 2017 | ▂▂▃▃▃▃▃▃▂▂▂ |
| controlled trial | 2010 | 23.878 | 2012 | 2013 | ▂▂▃▃▂▂▂▂▂▂▂ |
| postural balance | 2010 | 15.4265 | 2012 | 2017 | ▂▂▃▃▃▃▃▃▂▂▂ |
| rate | 2010 | 25.3309 | 2013 | 2014 | ▂▂▂▃▃▂▂▂▂▂▂ |
| body composition | 2010 | 32.8776 | 2013 | 2014 | ▂▂▂▃▃▂▂▂▂▂▂ |
| prediction | 2010 | 2.6749 | 2013 | 2014 | ▂▂▂▃▃▂▂▂▂▂▂ |
| fall prevention | 2010 | 25.6649 | 2013 | 2014 | ▂▂▂▃▃▂▂▂▂▂▂ |
| consequence | 2010 | 27.3192 | 2014 | 2015 | ▂▂▂▂▃▃▂▂▂▂▂ |
| cohort | 2010 | 43.2065 | 2014 | 2018 | ▂▂▂▂▃▃▃▃▃▂▂ |
| safety | 2010 | 28.2582 | 2015 | 2016 | ▂▂▂▂▂▃▃▂▂▂▂ |
| attention | 2010 | 33.7397 | 2016 | 2017 | ▂▂▂▂▂▂▃▃▂▂▂ |
| experience | 2010 | 13.7373 | 2016 | 2018 | ▂▂▂▂▂▂▃▃▃▂▂ |
| pain | 2010 | 28.5537 | 2016 | 2018 | ▂▂▂▂▂▂▃▃▃▂▂ |
| individual | 2010 | 33.4865 | 2016 | 2020 | ▂▂▂▂▂▂▃▃▃▃▃ |
| trial | 2010 | 9.7152 | 2016 | 2017 | ▂▂▂▂▂▂▃▃▂▂▂ |
| symptom | 2010 | 32.2689 | 2016 | 2020 | ▂▂▂▂▂▂▃▃▃▃▃ |
| gait speed | 2010 | 23.6379 | 2016 | 2017 | ▂▂▂▂▂▂▃▃▂▂▂ |
| life | 2010 | 16.1569 | 2017 | 2018 | ▂▂▂▂▂▂▂▃▃▂▂ |
| classification | 2010 | 37.0551 | 2018 | 2020 | ▂▂▂▂▂▂▂▂▃▃▃ |
| fall detection | 2010 | 48.4538 | 2018 | 2020 | ▂▂▂▂▂▂▂▂▃▃▃ |
| cost | 2010 | 16.6557 | 2018 | 2020 | ▂▂▂▂▂▂▂▂▃▃▃ |
| hospitalization | 2010 | 37.8174 | 2018 | 2020 | ▂▂▂▂▂▂▂▂▃▃▃ |
| gender | 2010 | 27.1045 | 2018 | 2020 | ▂▂▂▂▂▂▂▂▃▃▃ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, B.; Shin, S. Bibliometric Analysis on Research Trend of Accidental Falls in Older Adults by Using Citespace—Focused on Web of Science Core Collection (2010–2020). Int. J. Environ. Res. Public Health 2021, 18, 1663. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041663
Chen B, Shin S. Bibliometric Analysis on Research Trend of Accidental Falls in Older Adults by Using Citespace—Focused on Web of Science Core Collection (2010–2020). International Journal of Environmental Research and Public Health. 2021; 18(4):1663. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041663
Chicago/Turabian StyleChen, Boyuan, and Sohee Shin. 2021. "Bibliometric Analysis on Research Trend of Accidental Falls in Older Adults by Using Citespace—Focused on Web of Science Core Collection (2010–2020)" International Journal of Environmental Research and Public Health 18, no. 4: 1663. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041663