2.1. Literature Review
Many scholars pay attention to the impact of population aging on economic growth. Aging population has led to some huge economic consequences. The potential economic impacts of population aging are discussed in many papers. According to the existing research conclusions, the research about the economic impacts of population aging can be summarized into three categories: The first category of literature believes that population aging will have a negative impact on economic growth (Bloom et al., 2010 [
2]; Daniele et al., 2019 [
3]). This category of literature mainly demonstrates the negative effect of population aging on economic growth from the following three perspectives. First, the aging of the population will lead to a decrease in the proportion of the working-age population and labor force growth rate (Cutler et al., 1990 [
4]). At the same time, the aging of the population will also change the overall productivity level of the society. Population aging can also indirectly hamper economic growth by raising labor costs (Cepar and Troha, 2015 [
5]). Second, according to the life cycle theory, people have a high motivation to save when they are young. People have negative savings when they retire, so the deepening of population aging lowers the national savings rate (Heijdra and Ligthart, 2006 [
6]; Auerbach and Kotlikoff, 1987 [
7]; Auerbach et al., 1989 [
8]; Miles, 1999 [
9]; Hviding and Merette, 1998 [
10]). The decrease in savings reduces the level of physical capital investment, which is decreases economic growth. The dual pressures of decreasing government revenue and increasing social security expenditures such as old-age pension and medical care will seriously restrict the government’s ability to guide investment. Third, population aging could lower interest rates. The capital will flow from countries with more aging to those with less aging (Liu and McKibbin, 2020 [
11]).
The second category of literature argues that population aging has a beneficial impact on economic growth (Nagarajan et al., 2016 [
12]; Maity and Sinha, 2020 [
13]). First, population aging is caused by both the increase in life expectancy and the decrease in fertility rate. Although the decrease in fertility rate has a negative impact on economic growth, the increase in life expectancy has a positive impact on economic growth. The latter dominates the former (Prettner, 2013 [
14]). Second, the aging of population improves the investment opportunities of human capital (Choi and Shin, 2015 [
15]) and increases the years of schooling (Fougère and Mérette, 1999 [
16]). As population aging extends life expectancy and reduces people’s preference for raising offspring (Ladd and Murray, 2001 [
17]), people begin to pay more attention to the improvement of individual labor productivity instead of pursuing the increase of family labor force. To obtain higher labor remuneration in the future (Poterba, 1998 [
18]), people increase their investment in education, technical training, and other fields to improve their and their family members’ skill level (Boucekkine et al., 2002 [
19]; Gradstein and Kaganovich, 2004 [
20]), which will promote technological progress. Then, population aging can also promote the upgrading of industrial structure (Boriss et al., 2011 [
21]) and technological innovation through two other ways. The first is the learning by doing effect. With the increase of the average age of working population, experience and skill levels of work force increases, which improves the efficiency of innovation work. The second is that the labor shortage caused by population aging prompts the transformation of economic growth pattern and emphasis on technological progress, which in turn triggers the redistribution of social resources and promotes the technical progress and innovation in order to increase the economic merit (Lee and Mason, 2010 [
22]).
The third category of literature considers that the relationship between population aging and economic growth is complex, uncertain, and nonlinear. In the study of the relationship between population age structure and economic growth in OECD countries, An and Jeon (2006) found that population aging and economic growth present an inverted U-shaped relationship [
23]. Barro and Wolf (1989) pointed out that, when life expectancy increases from 60 to 69, the GDP per capita growth rises steadily. When the life expectancy exceeds 70, the GDP per capita growth rate declines but remains higher than in countries with low life expectancy [
24]. Futagami and Nakajima (2001) explored how population aging affects economic growth by constructing an endogenous growth model with life-cycle savings. The results indicate that population aging is not necessarily bad for economic growth [
25]. Liu Xiao-yong (2013) studied the influence of the population aging on the economic growth of provinces based on provincial panel data for 1989–2009 in China, and their research results suggest that there is an inverted U-shaped relationship between population aging and economic growth. The proportion of the elderly population has a decreasing positive effect on the inter-provincial economic growth rate, but, after crossing the inflection point, its effect changes from positive to negative [
26].
The relationship between health investment and economic growth has been considered by many scholars for a long time, but no unified conclusion has been reached. In simple terms, the economic resources including labor and commodities used for healthcare comprise health investment. To some extent, health spending improves the labor productivity and continues to pay off for a long time (Mushkin, 1962 [
27]). Government and residents are two main bodies of health investment. To meet people’s needs of high-quality medical and health services, the government increases investment in the medical establishment to improve the quality of medical service and increase medical resources (Castro, 2020 [
28]). Residents invest in their health in the following ways: medical insurance, health checkup, fitness investment, health consultation, etc. Some scholars found that the economic growth rate is much higher than the increase rates of physical capital and labor force (Barro and Sala-i-Martin, 1995 [
29]). Thus, they proposed the issue of “the impact on economic growth from population quality change”. Most papers discuss this issue from the viewpoint of human capital, and they argue that health investment promotes economic growth. As an investment, health determines the total amount of time that laborers can spend on economic and non-economic productive activities directly (Grossman, 1972 [
30]). A healthy workforce would promote the human capital accumulation process. Human capital plays a much bigger role in economic growth than physical capital (Schultz, 1961 [
31]), and its rate of return is also higher than physical capital. As an important part of capital accumulation, health investment can improve not only the productivity of individuals but also the productivity of the whole society (Lucas, 1989 [
32]). Health investment could promote economic growth through the following two main ways: The first is that health investment could promote economic growth by improving labor force participation rate and production efficiency; health investment could improve individuals’ health status and individuals can work longer with better health and increased life expectancy (Bloom et al., 2009 [
33]). The second is that health investment is conducive to human capital accumulation such as education and improves economic development efficiency by improving individual learning ability and returns to education (Fuchs, 1982 [
34]). Others think that health investment blocks the economic growth because it will squeeze out physical investment, which is still the main contributing factor to economic growth. By analyzing the relationship between the composition of public expenditure and economic growth, Devarajan et al. (1996) found that health expenditure has a slightly negative impact on economic growth [
35].
As discussed above, because of the decrease of working-age population caused by population aging, the first demographic dividend is wearing off. Given this, some thinks population aging will undermine economic development. On the contrary, other scholars believe that population aging can bring a second demographic dividend. Mason and Lee (2004) pointed out that low fertility and mortality will increase the capital–labor ratio (capital intensity) and output per capita [
36]. The impact on economic growth from population aging is determined by the relative importance of capital over labor in production (Curtis and Lugauer, 2019 [
37]). Lee and Mason (2006) believed that longer life expectancy will increase the consumption demand in old age, which will enhance people’s savings motive. In the perspective of the whole society, it will increase the accumulation of total social capital and promote economic growth [
38]. Lee and Mason (2010) found out that population aging leads to a tremendous increase in education levels of the population. They thought human capital investment is a potentially important generation mechanism of a second demographic dividend [
22]. Bairoliya et al. (2017) suggested that aging economies with high human capital may benefit from the increase of fertility [
39].
Saving is an important mechanism by which population aging affects economic growth. It is necessary to discuss the impact on saving from changes in demographics. Some recent papers focus on the channels through which demographics affect saving. In general, there are four channels. First, as mentioned above, total savings increases with the proportion of working-age population. Second, as the life expectancy increases, people will save for more consumption after retiring (Bloom et al., 2007 [
40]). Third, as the number of children declines, which leads to inadequate family insurance, people will increase precautionary savings. Fourth, as fertility decreases, some people who expect less retirement support from the next generation with smaller population will save more. Leff (1969) believed that there is a negative correlation between dependency ratio (including juvenile dependency ratio and old-age dependency ratio) and the household savings rate [
41]. Curtis et al. (2017) thought that different demographic profiles could affect savings differently. In China and India, with relative younger population, the increase of household savings rate is mostly due to the rapid decline in the number of children. In Japan, the most elderly country in the word, the decrease of savings rate is partially caused by the growing number of retirees [
42]. Imrohoroglu and Zhao (2018) suggested that the decline of family insurance caused by one-child policy in China increases savings rate [
43].
2.2. The Model
We assume an agent’s utility depends on his consumption level and health level (Grossman, 1972 [
30]). The level of health depends on the health investment in the adult life of representative individuals. The expected utility function of an agent is assumed as follows:
with
where
denotes consumption in period
,
denotes health level in period
, and
is the rate of time preference, which measures the weight in utility attached to the health level.
The analysis is based on an extended Mankiw–Romer–Weil model with two kinds of human capital (Knowles and Owen, 1995 [
44]). Output
Y is produced as a function of total factor productivity
A, physical capital
K, labor input
L, human education capital
E, and human health capital
H. At the same time, considering that population aging
will affect labor supply, the production function is assumed to be:
Subscripts
i and
t denote countries and years, respectively. Dividing by the labor force
Lit, the per capita production function can be written as follows:
with
being capital per effective unit of labor,
human education capital per effective unit of labor, and
human health capital per effective unit of labor. We assume population and technology grow with fixed rates
and
, respectively. Then, the accumulation equations of the three kinds of capital are as follows:
where
,
, and
denote the accumulation rate of physical capital, human education capital, and human health capital respectively, and
,
, and
denote their respective depreciation rates.
Each agent maximizes his own utility by selecting consumption and the levels of the accumulation of physical capital, human education capital, and human health capital. Therefore, the optimization problem can be written as follows:
Then, we assume the existence of a steady state (with
). To simplify the analysis, we assume
is the common depreciation rate. The Hamiltonian function is as follows:
According to the dynamic equilibrium condition (
), we can get steady-state values, which are denoted by asterisks:
and
According to Equations (4)–(7), and taking the natural logs. Then, we can get following equation:
2.3. Data and Methodology
Based on the theoretical model above, we set the basic econometric model as follows:
where subscripts
i and
t denote countries and years, respectively. g refers to economic growth measured by logarithmic form of GDP per capita, health capital H is measured by the ratio of total health expenditure to GDP, A refers to population aging measured by proportion of population aged 65 and over, educational capital E is measured by primary student-to-teacher ratio, K refers to accumulation rate of physical capital measured by ratio of gross domestic fixed capital formation to GDP, n refers to population growth rate, and ε is the stochastic disturbance term.
To further study the interaction between population aging and health investment on economic growth, this paper introduces the interaction term between population aging and health investment (HEAA) into the basic regression model, as shown in Equation (13):
To examine the impact on economic growth from health investment structure and financial expenditure structure, the two variables are added in the model (Equation (14)):
HS refers to health investment structure measured by the proportion of government health investment to total health investment and FS refers to financial expenditure structure measured by the proportion of government health investment to total government spending.
Using panel data from 186 countries and regions from 2000 to 2016, this paper empirically investigates the impact on economic growth of health investment and population aging.
The data for empirical analysis were obtained from a variety of sources. The per capita GDP and ratio of gross domestic fixed capital formation to GDP were obtained from the World Bank’s national accounts database, the OECD national accounts database, and WDI world bank development indicators database. World Health Organization (WHO) (World Health Organization 2005 [
1]) statistics were the source for population growth, the total population, the number people over 65 years old, and old-age dependency ratio. Primary student-to-teacher ratio was obtained from UNESCO Institute of Statistics. The ratio of health expenditure to GDP was derived from WHO Global Health Expenditure database. The ratio of people over 65 years old was calculated by dividing the number of people over 65 years old by the total population.
Summary statistics of the sample data are presented in
Table 1.
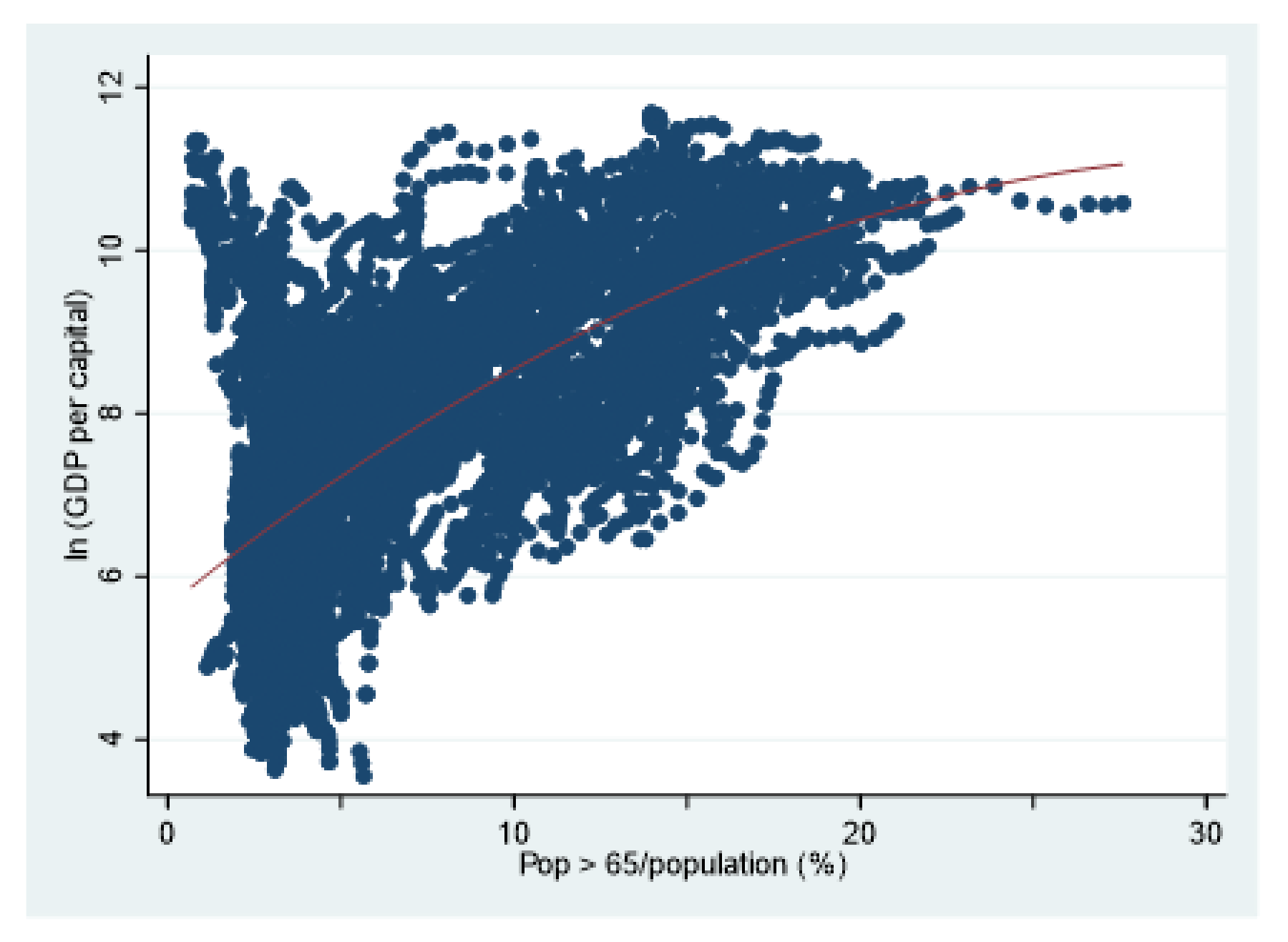
Table 2 presents pairwise correlation. Health investment and economic growth are positively correlated, which is consistent with the traditional human capital theory. Population aging and economic growth also present a positive relationship. Following Liu (2013) [
26], this paper uses a scatter plot to observe the relationship between population aging and economic growth. Through the scatter plot, the relationship between population aging and economic growth can be intuitively seen.
Figure 1 shows that aging population and economic growth present a tendency of positive correlation, but the positive relationship is gradually weakened. This is probably because, in the initial stage, the acceleration of physical capital accumulation and the extension of demographic dividend brought by population aging are conducive to economic growth, but, with the deepening of population aging, the positive relationship between population aging and economic growth gradually weakens and may even change.





{kind=link}