
Enablers of Patient Knowledge Empowerment for Self-Management of Chronic Disease: An Integrative Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Knowledge Enablers: Theoretical Background
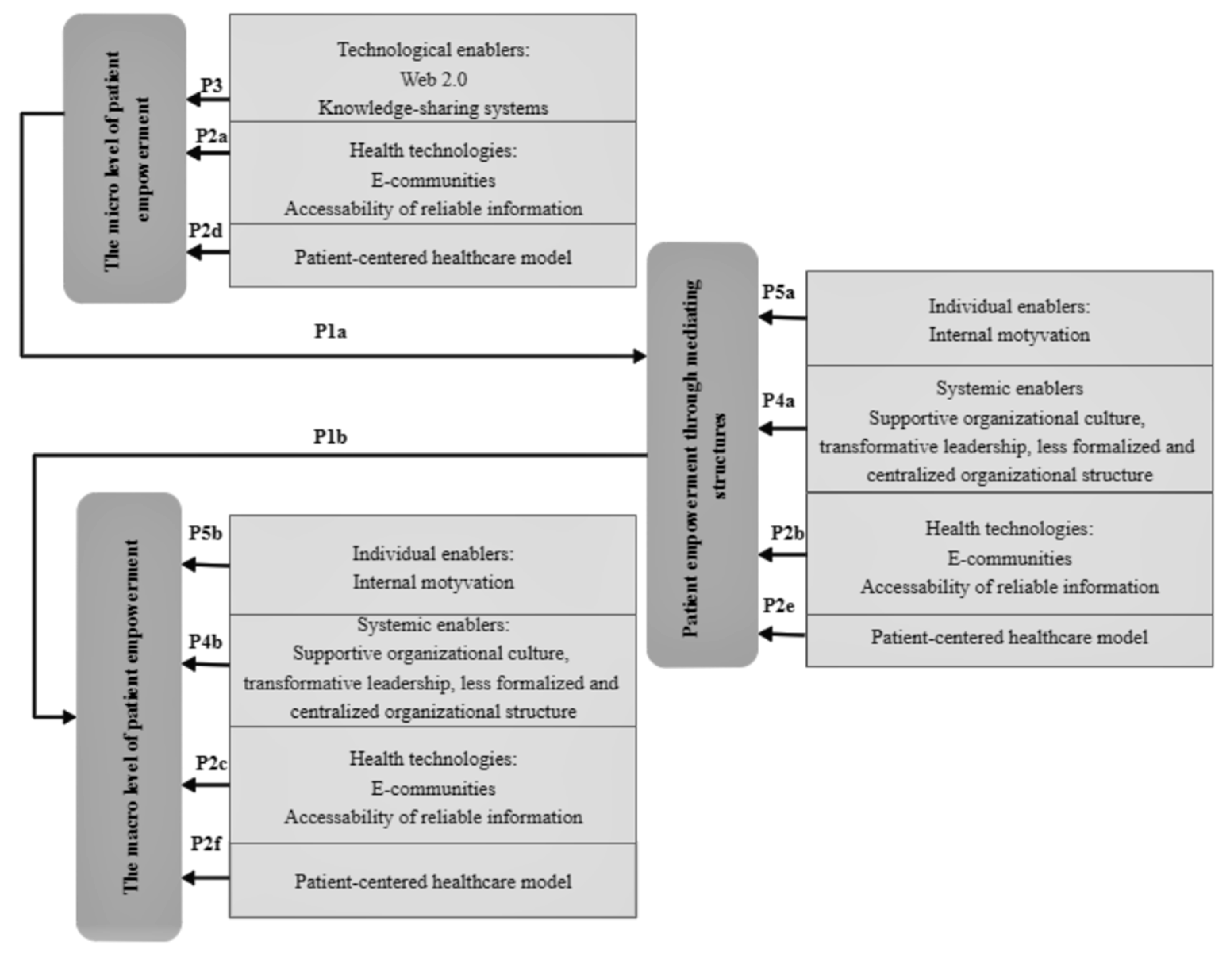
2.1.1. Patient Empowerment and Its Levels
- Empowerment is both theory and practice that deals with aspects of power, powerlessness, and oppression and how they contribute to the problems of individuals, families, or communities and affect helping relationships.
- Empowerment aims to increase personal, interpersonal, or political power in such a way that individuals, families, or communities can take action to improve their situation.
- Empowerment is a process that takes place at the individual, interpersonal, and/or community levels and includes subprocesses such as developing group awareness, reducing self-blame, accepting personal responsibility for change, and improving self-efficacy.
- Empowerment occurs through intervention methods, basing help relationships on cooperation, trust and shared power, awareness raising, individual involvement in the process of change, training in special skills, and mobilization of resources.
- A microcomponent covering such intrapersonal aspects as patient self-esteem and self-efficacy;
- Mediating structures characterized by mechanisms specific to groups of individuals and active participation of group members in sharing knowledge and growing their critical consciousness.
- A macrocomponent that encompasses social and political activities as mediating structures become community organizations capable of changing or creating new social conditions.
2.1.2. Patient Knowledge Formation for Patient Empowerment
- Promoting Action on Research Implementation in Health Services (PARIHS);
- Consolidated Framework for Implementation Research (CFIR);
- Knowledge to Action Framework (KTA).
2.1.3. Patient Knowledge Enablers: The Importance of Integrating Public Health Management and Knowledge Management Theories
- The knowledge protection process that manifests itself through knowledge storage activities [42].
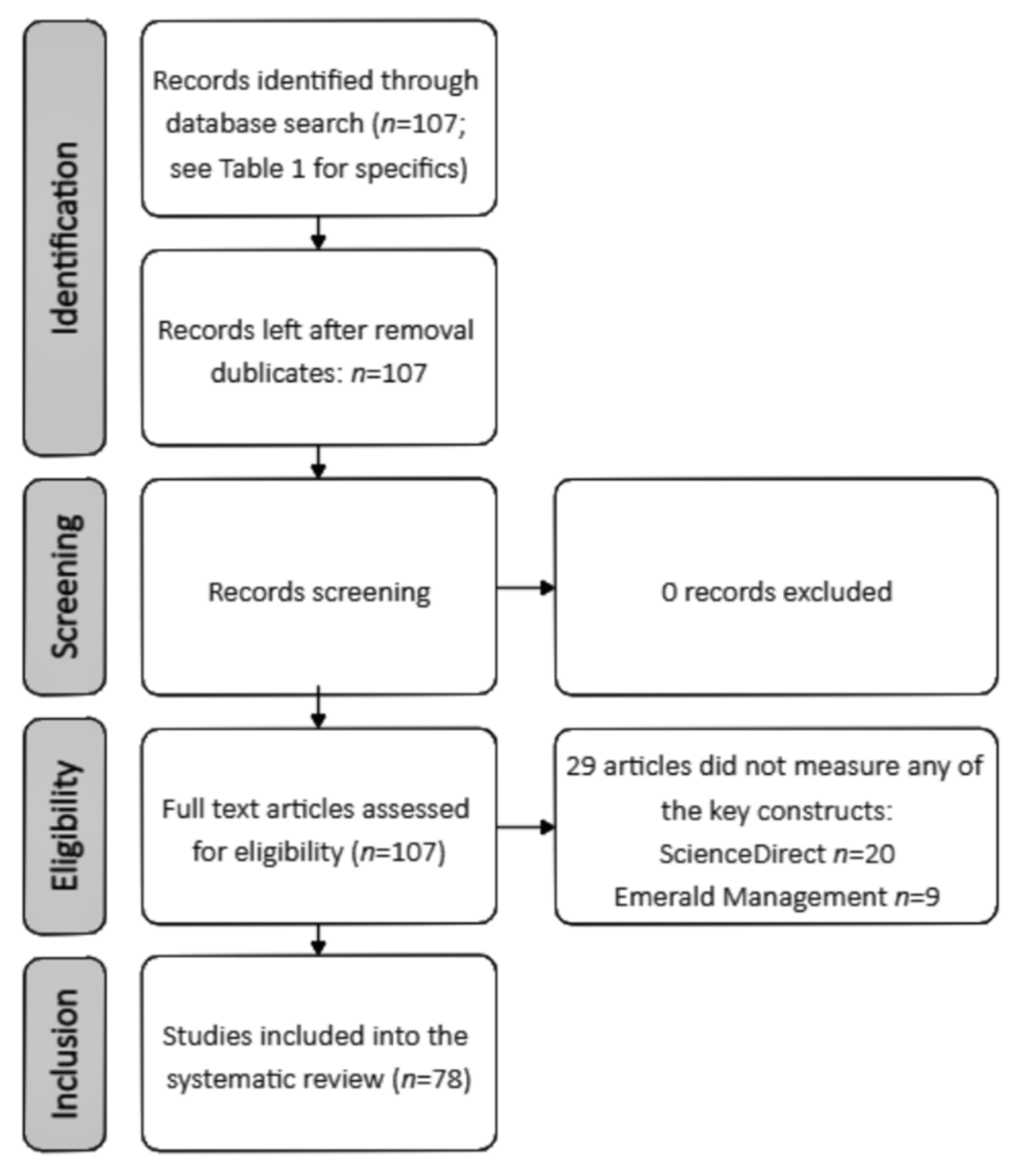
2.2. Methodology of Literature Review
2.2.1. Choice of Synthesis Vehicle
2.2.2. Literature Review
- ScienceDirect database search string: “patient empowerment” AND “knowledge” AND “enablers”.
- Emerald Management database search string: “knowledge management enablers” AND “empowerment”.
- As the aim of the study was to find a new approach that integrates two different research traditions, to reveal the holistic approach and ensure the completeness criterion, it was important to find a wide range of knowledge enablers; therefore, the research that conceptually and/or empirically develops the above keywords from various perspectives were considered suitable;
- The Emerald Management database does not detail search results and only provides research papers. In order to ensure a balance between the two disciplines when analyzing only scientific publications, the types of publications such as conference abstracts, mini reviews, short communications, and Encyclopedia were not included in the data analysis from the results obtained in the ScienceDirect database. From both databases, the research included in the integrative review met the peer-review and open access criteria. The application of the peer review filter in the search of both databases resulted in the entry of valid research papers into the integrative review.
2.2.3. Thematic Synthesis
3. Results
3.1. Overview of Identified Themes
3.2. Patient Knowledge Enablers: A Public Health Management Perspective
3.2.1. Individual Patient Knowledge Enablers
3.2.2. Health Technologies
3.2.3. Patient-Centered Healthcare Model
3.2.4. Disease Management Programs
3.2.5. Learning Health System
3.3. Patient Knowledge Enablers: A Knowledge Management Perspective
3.3.1. Technological Knowledge Sharing Enablers
3.3.2. Systematic Knowledge Sharing Enablers
3.3.3. Individual Enablers
3.4. Integration
3.5. Limitations
- Given the time and physical resources of the researchers, a relatively limited number of databases for the identification of potentially eligible studies were used.
- The choice to analyze only open access publications due to limited financial resources may have led to insufficient identification of themes of knowledge enablers for chronic patients from public health management and knowledge management perspectives and thus may have affected the results of the integration of these two perspectives.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holmström, I.; Röing, M. The relation between patient-centeredness and patient empowerment: A discussion on concepts. Patient Educ. Couns. 2010, 79, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Small, N.; Bower, P.; Chew-Graham, C.A.; Whalley, D.; Protheroe, J. Patient empowerment in long-term conditions: Development and preliminary testing of a new measure. BMC Health Serv. Res. 2013, 13, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, P.J.; Nakamoto, K. Patient behavior and the benefits of artificial intelligence: The perils of “dangerous” literacy and illusory patient empowerment. Patient Educ. Couns. 2013, 92, 223–228. [Google Scholar] [CrossRef]
- Anderson, R.M.; Funnell, M.M. Patient empowerment: Myths and misconceptions. Patient Educ. Couns. 2010, 79, 277–282. [Google Scholar] [CrossRef] [Green Version]
- Asimakopoulou, K.; Gilbert, D.; Newton, P.; Scambler, S. Back to basics: Re-examining the role of patient empowerment in diabetes. Patient Educ. Couns. 2012, 86, 281–283. [Google Scholar] [CrossRef]
- Wakefield, D.; Bayly, J.; Selman, L.E.; Firth, A.M.; Higginson, I.J.; Murtagh, F.E. Patient empowerment, what does it mean for adults in the advanced stages of a life-limiting illness: A systematic review using critical interpretive synthesis. Palliat. Med. 2018, 32, 1288–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snyder, H. Literature review as a research methodology: An overview and guidelines. J. Bus. Res. 2019, 104, 333–339. [Google Scholar] [CrossRef]
- Köhler, A.K.; Tingström, P.; Jaarsma, T.; Nilsson, S. Patient empowerment and general self-efficacy in patients with coronary heart disease: A cross-sectional study. BMC Fam. Pr. 2018, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Martos-Méndez, M.J. Self-efficacy and adherence to treatment: The mediating effects of social support. J. Behav. Health Soc. Issues 2015, 7, 19–29. [Google Scholar] [CrossRef]
- Aujoulat, I.; D’Hoore, W.; Deccache, A. Patient empowerment in theory and practice: Polysemy or cacophony? Patient Educ. Couns. 2007, 66, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Piper, S. Patient empowerment: Emancipatory or technological practice? Patient Educ. Couns. 2010, 79, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Johnston, A.C.; Worrell, J.L.; Di Gangi, P.M.; Wasko, M. Online health communities. Inf. Technol. People 2013, 26, 213–235. [Google Scholar] [CrossRef]
- Ippolito, A.; Smaldone, F.; Ruberto, M. Exploring patient empowerment. TQM J. 2019, 32, 92–109. [Google Scholar] [CrossRef]
- Doherty, K.; Barry, M.; Belisario, J.M.; Morrison, C.; Car, J.; Doherty, G. Personal information and public health: Design tensions in sharing and monitoring wellbeing in pregnancy. Int. J. Hum. Comput. Stud. 2020, 135, 102373. [Google Scholar] [CrossRef] [PubMed]
- Christie, H.L.; Martin, J.L.; Connor, J.; Tange, H.J.; Verhey, F.R.; De Vugt, M.E.; Orrell, M. eHealth interventions to support caregivers of people with dementia may be proven effective, but are they implementation-ready? Internet Interv. 2019, 18, 100260. [Google Scholar] [CrossRef] [PubMed]
- Adeinat, I.M.; Abdulfatah, F.H. Organizational culture and knowledge management processes: Case study in a public university. VINE J. Infect. Knowl. Manag. Syst. 2019, 49, 35–53. [Google Scholar] [CrossRef]
- Arif, M.; Mohammed, A.-Z.; Gupta, A.D. Understanding knowledge sharing in the Jordanian construction industry. Constr. Innov. 2015, 15, 333–354. [Google Scholar] [CrossRef]
- Curado, C.; Vieira, S. Trust, knowledge sharing and organizational commitment in SMEs. Pers. Rev. 2019, 48, 1449–1468. [Google Scholar] [CrossRef]
- Yao, J.; Crupi, A.; Di Minin, A.; Zhang, X. Knowledge sharing and technological innovation capabilities of Chinese software SMEs. J. Knowl. Manag. 2020, 24, 607–634. [Google Scholar] [CrossRef]
- Scharf, D. A New View of Patient Education: How Information and Knowledge Management Can Contribute to Pa-tient-centered Health Care. In Knowledge Work; The Knowledge Institute. Rutgers University: New Brunswick, NJ, USA, 2010; pp. 139–158. [Google Scholar]
- Menear, M.; Blanchette, M.-A.; Demers-Payette, O.; Roy, D. A framework for value-creating learning health systems. Health Res. Policy Syst. 2019, 17, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Friedman, C.P.; Wong, A.K.; Blumenthal, D. Achieving a Nationwide Learning Health System. Sci. Transl. Med. 2010, 2, 8–10. [Google Scholar] [CrossRef] [Green Version]
- Rubin, J.C. Patient empowerment and the Learning Health System. Learn. Health Syst. 2017, 1, e10030. [Google Scholar] [CrossRef] [PubMed]
- Flynn, A.J.; Friedman, C.P.; Boisvert, P.; Landis-Lewis, Z.; Lagoze, C. The Knowledge Object Reference Ontology (KORO): A formalism to support management and sharing of computable biomedical knowledge for learning health systems. Learn. Health Syst. 2018, 2, e10054. [Google Scholar] [CrossRef] [Green Version]
- Nonaka, I.; Von Krogh, G. Perspective—Tacit Knowledge and Knowledge Conversion: Controversy and Advancement in Organizational Knowledge Creation Theory. Organ. Sci. 2009, 20, 635–652. [Google Scholar] [CrossRef] [Green Version]
- Hussein, A.T.T.; Singh, S.K.; Farouk, S.; Sohal, A.S. Knowledge sharing enablers, processes and firm innovation capability. J. WorkLearn. 2016, 28, 484–495. [Google Scholar] [CrossRef]
- Kale, S.; Karaman, E.A. Evaluating the Knowledge Management Practices of Construction Firms by Using Importance–Comparative Performance Analysis Maps. J. Constr. Eng. Manag. 2011, 137, 1142–1152. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez, L.M.; Delois, K.A.; GlenMaye, L. Understanding Empowerment Practice: Building on Practitioner-Based Knowledge. Fam. Soc. J. Contemp. Soc. Serv. 1995, 76, 534–542. [Google Scholar] [CrossRef]
- Peterson, N.A. Empowerment Theory: Clarifying the Nature of Higher-Order Multidimensional Constructs. Am. J. Community Psychol. 2014, 53, 96–108. [Google Scholar] [CrossRef] [PubMed]
- European Patient Forum, Toolkit for Patient Organizations on Patient Empowerment. Available online: https://www.eu-patient.eu/library/toolkits/ (accessed on 15 September 2020).
- Bate, P.; Robert, G. Experience-based design: From redesigning the system around the patient to co-designing services with the patient. Qual. Saf. Health Care 2006, 15, 307–310. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.; Khadka, A. Role of empowerment and sense of community on online social health support group. Infect. Technol. People 2019, 32, 1564–1590. [Google Scholar] [CrossRef]
- Rutten, L.J.F.; Hesse, B.W.; Sauver, J.L.S.; Wilson, P.; Chawla, N.; Hartigan, D.B.; Moser, R.P.; Taplin, S.; Glasgow, R.; Arora, N.K. Health Self-Efficacy Among Populations with Multiple Chronic Conditions: The Value of Patient-Centered Communication. Adv. Ther. 2016, 33, 1440–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagstaff, B. Impact of antibiotic restrictions: The patient’s perspective. Clin. Microbiol. Infect. 2006, 12, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora, M.A.; Saarijärvi, M.; Sparud-Lundin, C.; Moons, P.; Bratt, E.-L. Empowering Young Persons with Congenital Heart Disease: Using Intervention Mapping to Develop a Transition Program—The Stepstones Project. J. Pediatr. Nurs. 2020, 50, e8–e17. [Google Scholar] [CrossRef]
- Rissel, C. Empowerment: The holy grail of health promotion? Health Promot. Int. 1994, 9, 39–47. [Google Scholar] [CrossRef]
- Hatch, M.J.; Cunliffe, A.L. Organization Theory: Modern, Symbolic, and Postmodern Perspectives, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Dizon, J.T. Theoretical Concepts and Practice of Community Organizing. J. Public Aff. Dev. 2012, 1, 89–123. [Google Scholar]
- Field, B.; Booth, A.; Ilott, I.; Gerrish, K. Using the Knowledge to Action Framework in practice: A citation analysis and systematic review. Implement. Sci. 2014, 9, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milat, A.J.; Li, B. Narrative review of frameworks for translating research evidence into policy and practice. Public Health Res. Pr. 2017, 27, 1–13. [Google Scholar] [CrossRef]
- Brathwaite, R.; Hutchinson, E.; McKee, M.; Palafox, B.; Balabanova, D. The Long and Winding Road: A Systematic Literature Review Conceptualising Pathways for Hypertension Care and Control in Low- and Middle-Income Countries. Int. J. Health Policy Manag. 2020, x(x), 1–12. [Google Scholar] [CrossRef]
- Gold, A.H.; Malhotra, A.; Segars, A.H. Knowledge Management: An Organizational Capabilities Perspective. J. Manag. Inf. Syst. 2001, 18, 185–214. [Google Scholar] [CrossRef]
- Song, J.H.; Yoon, S.W.; Yoon, H.J. Identifying organizational knowledge creation enablers through content analysis: The voice from the industry. Perform. Improv. Q. 2011, 24, 71–88. [Google Scholar] [CrossRef]
- Lee, H.; Choi, B. Journal of Management Information Systems, Informa-tion and Management. J. Organ. Comput. Electron. Commer. 2003, 20, 179–228. [Google Scholar]
- Al-Gharibeh, K. The Knowledge Enablers of Knowledge Transfer: An Empirical Study in Telecommunications Companies. IBIMA Bus. Rev. 2011, 2011, 1–13. [Google Scholar] [CrossRef]
- Owusu-Manu, D.-G.; Edwards, D.J.; Pärn, E.A.; Antwi-Afari, M.F.; Aigbavboa, C. The knowledge enablers of knowledge transfer: A study in the construction industries in Ghana. J. Eng. Des. Technol. 2018, 16, 194–210. [Google Scholar] [CrossRef]
- Lilleoere, A.; Hansen, E.H. Knowledge-sharing enablers and barriers in pharmaceutical research and development. J. Knowl. Manag. 2011, 15, 53–70. [Google Scholar] [CrossRef]
- Karamat, J.; Shurong, T.; Ahmad, N.; Waheed, A.; Mahmood, K. Enablers Supporting the Implementation of Knowledge Management in the Healthcare of Pakistan. Int. J. Environ. Res. Public Health 2018, 15, 2816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, R.V.D.; Melo, T.M. Linkage between dynamics capability and knowledge management factors. Manag. Decis. 2017, 55, 2256–2276. [Google Scholar] [CrossRef] [Green Version]
- Donate, M.J.; Guadamillas, F. Organizational factors to support knowledge management and innovation. J. Knowl. Manag. 2011, 15, 890–914. [Google Scholar] [CrossRef]
- Ali, A.A.; Selvam, D.D.D.P.; Paris, L.; Gunasekaran, A. Key factors influencing knowledge sharing practices and its relationship with organizational performance within the oil and gas industry. J. Knowl. Manag. 2019, 23, 1806–1837. [Google Scholar] [CrossRef]
- Cronin, M.A.; George, E. The Why and How of the Integrative Review. Organ. Res. Methods 2020, 1–25. [Google Scholar] [CrossRef]
- Lewins, A.; Silver, C. Using Software in Qualitative Research: A Step-by-Step Guide; Sage: London, UK, 2014. [Google Scholar]
- Seidel, J.V. QDA: A Model of the Process Noticing, Collecting, Thinking about Things. Available online: http://eer.engin.umich.edu/wp-content/uploads/sites/443/2019/08/Seidel-Qualitative-Data-Analysis.pdf (accessed on 4 September 2020).
- Meslin, E.M.; Alpert, S.A.; Carroll, A.E.; Odell, J.D.; Tierney, W.M.; Schwartz, P.H. Giving patients granular control of personal health information: Using an ethics ‘Points to Consider’ to inform informatics system designers. Int. J. Med. Inform. 2013, 82, 1136–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meis, J.J.; Bosma, C.B.; Spruit, M.A.; Franssen, F.M.; Janssen, D.J.; Teixeira, P.J.; Augustin, I.M.; Wouters, E.F.; De Vries, N.K.; Schols, A.M.; et al. A qualitative assessment of COPD patients’ experiences of pulmonary rehabilitation and guidance by healthcare professionals. Respir. Med. 2014, 108, 500–510. [Google Scholar] [CrossRef] [Green Version]
- Steinmetz, M.; Rammos, C.; Rassaf, T.; Lortz, J. Digital interventions in the treatment of cardiovascular risk factors and atherosclerotic vascular disease. IJC Hear. Vasc. 2020, 26, 100470. [Google Scholar] [CrossRef]
- Kraus, S.; Schiavone, F.; Pluzhnikova, A.; Invernizzi, A.C. Digital transformation in healthcare: Analyzing the current state-of-research. J. Bus. Res. 2021, 123, 557–567. [Google Scholar] [CrossRef]
- Menon, M.; George, B. Social media use for patient empowerment in the Gulf Cooperation Council region. Clin. eHealth 2018, 1, 21–27. [Google Scholar] [CrossRef]
- Kouroubali, A.; Katehakis, D.G. The new European interoperability framework as a facilitator of digital transformation for citizen empowerment. J. Biomed. Inform. 2019, 94, 103166. [Google Scholar] [CrossRef]
- Verbraecken, J. Telemedicine Applications in Sleep Disordered Breathing. Sleep Med. Clin. 2016, 11, 445–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marco-Ruiz, L.; Bønes, E.; De La Asunción, E.; Gabarron, E.; Aviles-Solis, J.C.; Lee, E.; Traver, V.; Sato, K.; Bellika, J.G. Combining multivariate statistics and the think-aloud protocol to assess Human-Computer Interaction barriers in symptom checkers. J. Biomed. Inform. 2017, 74, 104–122. [Google Scholar] [CrossRef] [PubMed]
- Hatton, J.D.; Schmidt, T.M.; Jelen, J. Adoption of Electronic Health Care Records: Physician Heuristics and Hesitancy. Procedia Technol. 2012, 5, 706–715. [Google Scholar] [CrossRef] [Green Version]
- Van Gorp, P.; Comuzzi, M.; Jahnen, A.; Kaymak, U.; Middleton, B. An open platform for personal health record apps with platform-level privacy protection. Comput. Biol. Med. 2014, 51, 14–23. [Google Scholar] [CrossRef]
- Kopanitsa, G.; Veseli, H.; Yampolsky, V. Development, implementation and evaluation of an information model for archetype based user responsive medical data visualization. J. Biomed. Inform. 2015, 55, 196–205. [Google Scholar] [CrossRef] [Green Version]
- Genitsaridi, I.; Kondylakis, H.; Koumakis, L.; Marias, K.; Tsiknakis, M. Towards Intelligent Personal Health Record Systems: Review, Criteria and Extensions. Procedia Comput. Sci. 2013, 21, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Fiske, A.; Buyx, A.; Prainsack, B. The double-edged sword of digital self-care: Physician perspectives from Northern Germany. Soc. Sci. Med. 2020, 260, 113174. [Google Scholar] [CrossRef]
- Wicks, P.; Keininger, D.L.; Massagli, M.P.; De La Loge, C.; Brownstein, C.; Isojärvi, J.; Heywood, J. Perceived benefits of sharing health data between people with epilepsy on an online platform. Epilepsy Behav. 2012, 23, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Van Der Heide, I.; Snoeijs, S.; Quattrini, S.; Struckmann, V.; Hujala, A.; Schellevis, F.; Rijken, M. Patient-centeredness of integrated care programs for people with multimorbidity. Results from the European ICARE4EU project. Health Policy 2018, 122, 36–43. [Google Scholar] [CrossRef]
- Pimouguet, C.; Le Goff, M.; Thiébaut, R.; Dartiques, J.F.; Helmer, C. Effectiveness of disease-management programs for improving diabetes care: A meta-analysis. CMAJ. 2011, 183, E115–E127. [Google Scholar] [CrossRef] [Green Version]
- CN, B.M.; Alberts, M.J.; Balady, G.J.; Ballantyne, C.M.; Berra, K.; Black, H.R.; Underberg, J.A. ACCF/AHA/ACP 2009 Competence and Training Statement: A Curriculum on Prevention of Cardiovascular Disease. J. Am. Coll. Cardiol. 2009, 54, 1336–1363. [Google Scholar] [CrossRef] [Green Version]
- Holt, D.; Bouder, F.; Elemuwa, C.; Gaedicke, G.; Khamesipour, A.; Kisler, B.; Kochhar, S.; Kutalek, R.; Maurer, W.; Obermeier, P.; et al. The importance of the patient voice in vaccination and vaccine safety—are we listening? Clin. Microbiol. Infect. 2016, 22, S146–S153. [Google Scholar] [CrossRef] [Green Version]
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V.; et al. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. Lancet Glob. Health 2018, 6, e1196–e1252. [Google Scholar] [CrossRef] [Green Version]
- Al Saifi, S.A. Positioning organisational culture in knowledge management research. J. Knowl. Manag. 2015, 19, 164–189. [Google Scholar] [CrossRef]
- Malik, M.S.; Kanwal, M. Impacts of organizational knowledge sharing practices on employees’ job satisfaction. J. Work. Learn. 2018, 30, 2–17. [Google Scholar] [CrossRef]
- Qandah, R.; Suifan, T.S.; Masa’Deh, R.; Obeidat, B.Y. The impact of knowledge management capabilities on innovation in entrepreneurial companies in Jordan. Int. J. Organ. Anal. 2020. [Google Scholar] [CrossRef]
- Yeh, Y.; Lai, S.; Ho, C. Knowledge management enablers: A case study. Ind. Manag. Data Syst. 2006, 106, 793–810. [Google Scholar] [CrossRef]
- Han, S.-H. The antecedents and dimensionality of knowledge-sharing intention. Eur. J. Train. Dev. 2018, 42, 125–142. [Google Scholar] [CrossRef]
- Ehrhart, M.G.; Schneider, B. Organizational Climate and Culture. Annu. Rev. Psychol. 2013, 64, 361–388. [Google Scholar]
- Pellegrini, M.M.; Ciampi, F.; Marzi, G.; Orlando, B. The relationship between knowledge management and leadership: Mapping the field and providing future research avenues. J. Knowl. Manag. 2020, 24, 1445–1492. [Google Scholar] [CrossRef]
- De Angelis, C.T. The impact of national culture and knowledge management on governmental intelligence. J. Model. Manag. 2016, 11, 240–268. [Google Scholar] [CrossRef]
- Mutonyi, B.R.; Slåtten, T.; Lien, G. Organizational climate and creative performance in the public sector. Eur. Bus. Rev. 2020, 32, 615–631. [Google Scholar] [CrossRef]
- Joshi, H.; Chawla, D.; Farooquie, J.A. Segmenting knowledge management (KM) practitioners and its relationship to performance variation-some empirical evidence. J. Knowl. Manag. 2014, 18, 469–493. [Google Scholar] [CrossRef]
- Gürlek, M.; Çemberci, M. Understanding the relationships among knowledge-oriented leadership, knowledge management capacity, innovation performance and organizational performance. Kybernetes 2020, 49, 2819–2846. [Google Scholar] [CrossRef]
- Xiao, Y.; Zhang, X.; De Pablos, P.O. How does individuals’ exchange orientation moderate the relationship between transformational leadership and knowledge sharing? J. Knowl. Manag. 2017, 21, 1622–1639. [Google Scholar] [CrossRef]
- Latif, K.F.; Afzal, O.; Saqib, A.; Sahibzada, U.F.; Alam, W. Direct and configurational paths of knowledge-oriented leadership, entrepreneurial orientation, and knowledge management processes to project success. J. Intellect. Cap. 2020, 22, 149–170. [Google Scholar] [CrossRef]
- Rohim, A.; Budhiasa, I.G.S. Organizational culture as moderator in the relationship between organizational reward on knowledge sharing and employee performance. J. Manag. Dev. 2019, 38, 538–560. [Google Scholar] [CrossRef]
- Wong, K.Y.; Aspinwall, E. An empirical study of the important factors for knowledge-management adoption in the SME sector. J. Knowl. Manag. 2005, 9, 64–82. [Google Scholar] [CrossRef] [Green Version]
- Thani, F.N.; Mirkamali, S.M. Factors that enable knowledge creation in higher education: A structural model. Data Technol. Appl. 2018, 52, 424–444. [Google Scholar] [CrossRef]
- Ramachandran, S.D.; Chong, S.; Wong, K. Knowledge management practices and enablers in public universities: A gap analysis. Campus-Wide Infect. Syst. 2013, 30, 76–94. [Google Scholar] [CrossRef]
- Huang, Y.-C.; Chin, Y.-C. Transforming collective knowledge into team intelligence: The role of collective teaching. J. Knowl. Manag. 2018, 22, 1243–1263. [Google Scholar] [CrossRef]
- Paduch, A.; Kuske, S.; Schiereck, T.; Droste, S.; Loerbroks, A.; Sørensen, M.; Maggini, M.; Icks, A. Psychosocial barriers to healthcare use among individuals with diabetes mellitus: A systematic review. Prim. Care Diabetes 2017, 11, 495–514. [Google Scholar] [CrossRef] [Green Version]
- Akbari, N.; Ghaffari, A. Verifying relationship of knowledge management initiatives and the empowerment of human resources. J. Knowl. Manag. 2017, 21, 1120–1141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Databases | Number of Articles Found | Article Type | Subject Areas | Access Type, Review Type |
|---|---|---|---|---|
| ScienceDirect | 51 | Review articles (14) Research articles (34) Discussion (2) Editorials (1) | Medicine and Dentistry (29) Computer Science (6) Nursing and Health Professionals (9) Biochemistry, Genetics and Molecular Biology (3) Immunology and Microbiology (2) Neuroscience (2) | Open Access, Peer-review |
| Emerald Management | 56 | Articles (56) | Social Sciences (56) | Open Access, Peer-review |
| Themes | Subthemes | Number of Citations |
|---|---|---|
| Individual enablers | Autonomy | 8 |
| Motivation | 3 | |
| Involvement in the search for a health-related decision | 4 | |
| Involvement of a partner | 3 | |
| Self-esteem | 2 | |
| Clear available information about the chronic disease | 2 | |
| Health technologies | Digital information | 11 |
| Digital self-care via empowering healthcare forms | 36 | |
| Accessibility of reliable information | 11 | |
| Creation of e-communities | 10 | |
| Patient-centeredness model | Characteristics of patient-centered model | 12 |
| Disease management programs | Multicomponentiality of disease management programs | 8 |
| Interaction between the patient and a healthcare professional | 4 | |
| Learning health system | Mission of learning health system | 9 |
| World Health Organization | 5 |
| Themes | Subthemes | Number of Citations |
|---|---|---|
| Technological enablers of knowledge sharing | Web 2.0 | 12 |
| Systems of knowledge sharing | 5 | |
| Systemic enablers of knowledge sharing | Supportive organizational culture | 38 |
| Transformative leadership | 15 | |
| Less formalized and centralized organizational structure | 7 | |
| Enablers of individual knowledge sharing | Openness to experience | 3 |
| Satisfaction arising from helping others | 3 | |
| Self-efficacy | 1 | |
| Attitudes, subjective norms and conscious self-control | 2 | |
| Internal motivation for knowledge sharing | 7 |
| Theme | Subthemes | Number of Citations: | |
|---|---|---|---|
| In Public Health Management Literature | In Knowledge Management Literature | ||
| Levels of patient empowerment | Microlevel | 11 | 6 |
| Empowerment through mediating structures | 15 | 23 | |
| Macrolevel | 9 | 19 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vainauskienė, V.; Vaitkienė, R. Enablers of Patient Knowledge Empowerment for Self-Management of Chronic Disease: An Integrative Review. Int. J. Environ. Res. Public Health 2021, 18, 2247. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052247
Vainauskienė V, Vaitkienė R. Enablers of Patient Knowledge Empowerment for Self-Management of Chronic Disease: An Integrative Review. International Journal of Environmental Research and Public Health. 2021; 18(5):2247. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052247
Chicago/Turabian StyleVainauskienė, Vestina, and Rimgailė Vaitkienė. 2021. "Enablers of Patient Knowledge Empowerment for Self-Management of Chronic Disease: An Integrative Review" International Journal of Environmental Research and Public Health 18, no. 5: 2247. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052247