
Different Responses to Stress, Health Practices, and Self-Care during COVID-19 Lockdown: A Stratified Analysis

 ,
,  ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Measures
2.2.1. Perceived Stress
2.2.2. COVID-19 Health Practices
2.2.3. Self-Care Activities
2.3. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics
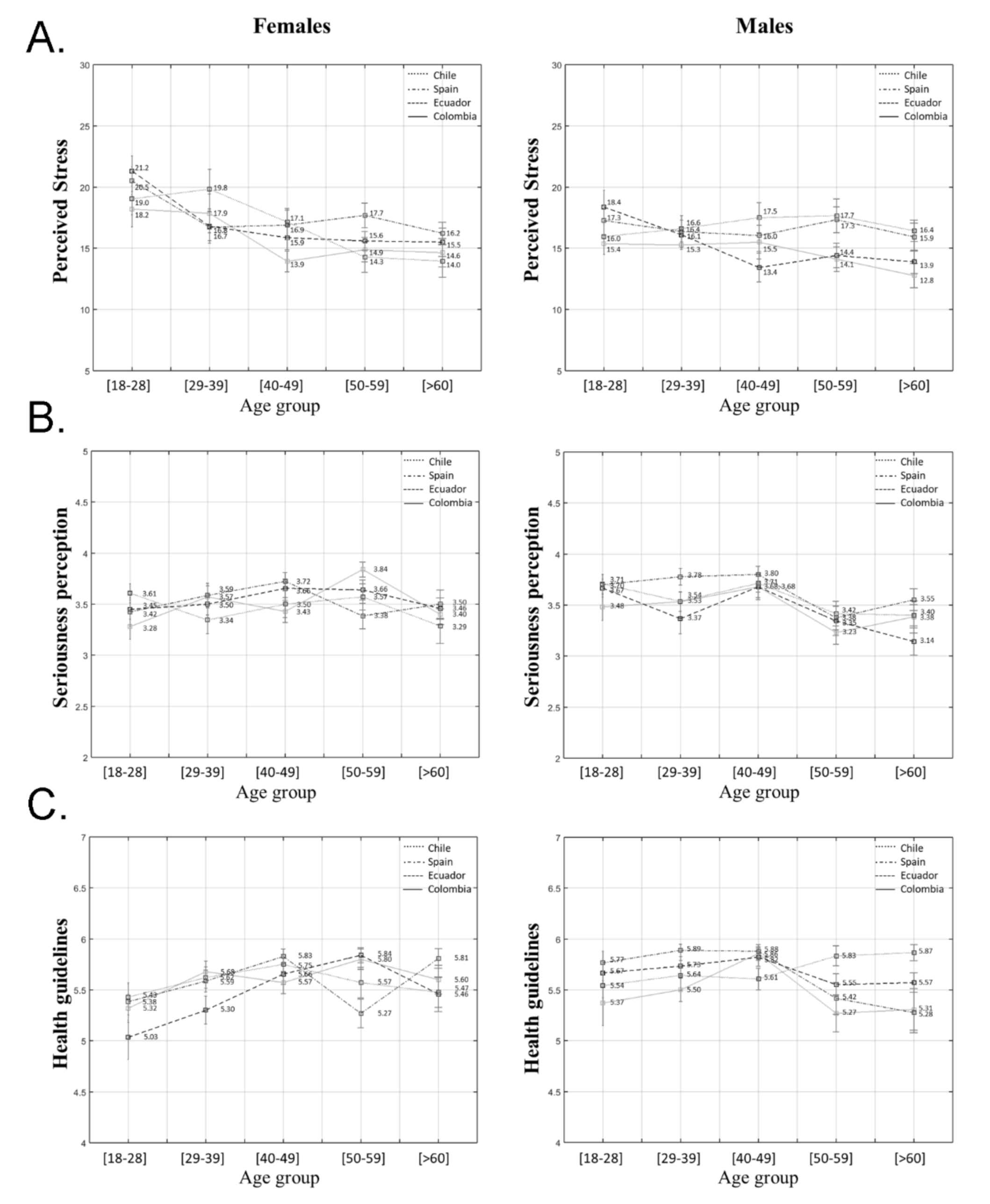
3.2. Perceived Stress
3.3. COVID-19 Health Practices
3.3.1. COVID-19 Seriousness Perception
3.3.2. Adherence to Public Health Guidelines
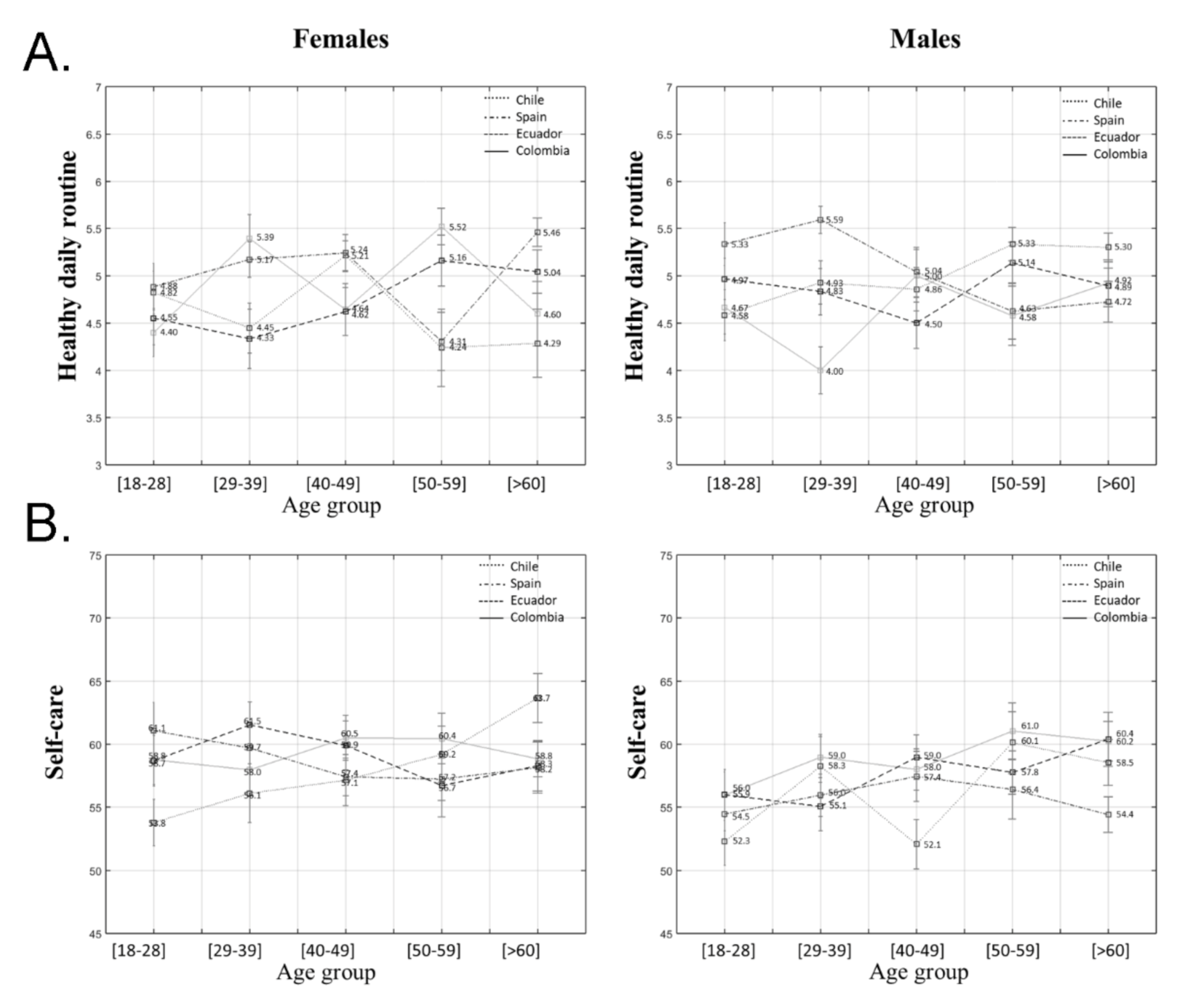
3.3.3. Healthy Daily Routines
3.4. Self-Care Activities
Health Consciousness
4. Discussion
Limitations
5. Conclusions
5.1. A More Integrative Health Promotion Approach
5.2. A Gender-Based Approach
5.3. Intersectionality and Community Action
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time [published correction appears in Lancet Infect Dis. 2020 September 2020, (9):e215]. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Chew, N.; Lee, G.; Tan, B.; Jing, M.; Goh, Y.; Ngiam, N.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, Z.F. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 7, 2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galea, S.; Merchant, R.M.; Lurie, N. The mental health consequences of COVID-19 and physical distancing: The need for prevention and early intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittelmark, M.B.; Sagy, S.; Eriksson, M.; Bauer, G.F.; Pelikan, J.M.; Lindström, B.; Espnes, G.A. Part IV: The Application of Salutogenesis in Everyday Settings. In The Handbook of Salutogenesis, 1st ed.; Springer Nature: London, UK, 2017; Volume 3, pp. 152–257. [Google Scholar]
- Mittelmark, M.B.; Bull, T.; Bouwman, L. Emerging ideas relevant to the salutogenic model of health. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Arild Espnes, G., Eds.; Springer Nature: Cham, Switzerland, 2017; pp. 45–56. [Google Scholar]
- Morgan, A.; Ziglio, E. Revitalising the evidence base for public health: An assets model. Promot. Educ. 2007, 2, 17–22. [Google Scholar] [CrossRef]
- Narasimhan, M.; Allotey, P.; Hardon, A. Self-care interventions to advance health and wellbeing: A conceptual framework to inform normative guidance. BMJ 2019, 365, l688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulia, K.K.; Kumar, V.M. Reverse quarantine: Management of COVID-19 by Kerala with its higher number of aged population. Psychogeriatrics 2020, 20, 794–795. [Google Scholar] [CrossRef]
- Hamer, M.; Kivimäki, M.; Gale, C.R.; Batty, G.D. Lifestyle risk factors, inflammatory mechanisms, and COVID-19 hospitalization: A community-based cohort study of 387,109 adults in UK. Brain Behav. Immun. 2020, 87, 184–187. [Google Scholar] [CrossRef]
- Martinez, E.Z.; Silva, F.M.; Morigi, T.Z.; Zucoloto, M.L.; Silva, T.L.; Joaquim, A.G.; Agnol, G.D.; Martinez, M.O.Z.; Silva, W.R. Physical activity in periods of social distancing due to COVID-19: A cross-sectional survey. Ciênc. Saúde Coletiva 2020, 25, 4157–4168. [Google Scholar] [CrossRef]
- Ruiz, M.C.; Devonport, T.; Chen-Wilson, C.H.; Nicholls, W.; Cagas, J.; Fernandez-Montalvo, J.; Choi, Y.; Robazza, C. A Cross-Cultural Exploratory Study of Health Behaviors and Wellbeing during COVID-19. Front. Psychol. 2021, 11, 3897. [Google Scholar] [CrossRef] [PubMed]
- Bann, D.; Villadsen, A.; Maddock, J.; Hughes, A.; Ploubidis, G.B.; Silverwood, R.J.; Patalay, P. Changes in the behavioural determinants of health during the coronavirus (COVID-19) pandemic: Gender, socioeconomic and ethnic inequalities in 5 British cohort studies. medRxiv 2020. [Google Scholar] [CrossRef]
- Alzueta, E.; Perrin, P.; Baker, F.C.; Caffarra, S.; Ramos-Usuga, D.; Yuksel, D.; Arango-Lasprilla, J.C. How the COVID-19 pandemic has changed our lives: A study of psychological correlates across 59 countries. J. Clin. Psychol. 2020, 1–15. [Google Scholar] [CrossRef]
- Perera, M.J.; Brintz, C.E.; Birnbaum-Weitzman, O.; Penedo, F.J.; Gallo, L.C.; Gonzalez, P.; Gouskova, N.; Isasi, C.R.; Navas-Nacher, E.L.; Perreira, K.M.; et al. Factor structure of the Perceived Stress Scale-10 (PSS) across English and Spanish language responders in the HCHS/SOL Sociocultural Ancillary Study. Psychol. Assess. 2017, 29, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedrozo-Pupo, J.C.; Pedrozo-Cortés, M.J.; Campo-Arias, A. Perceived stress associated with COVID-19 epidemic in Colombia: An online survey. Cad Saude Publica 2020, 36, e00090520. [Google Scholar] [CrossRef] [PubMed]
- Campo-Arias, A.; Pedrozo-Cortés, M.J.; Pedrozo-Pupo, J.C. Pandemic-Related Perceived Stress Scale of COVID-19: An exploration of online psychometric performance. Rev. Colomb. Psiquiatr. 2020, 49, 229–230. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Li, Q.X.; Zhang, H.; Zhu, J.Y.; Yang, X.; Wu, Y.H.; Xiong, J.; Li, F.; Wang, H.; Chen, Z. The psychological impact of COVID-19 outbreak on medical staff and the general public. Curr. Psychol. 2020, 7, 1–9. [Google Scholar] [CrossRef]
- Martínez, M.; Luis, E.O.; Oliveros, E.Y.; Fernández-Berrocal, P.; Sarrionandia, A.; Bermejo-Martins, E. Validity and reliability of the Self-Care Activities Screening Scale (SASS-14) during COVID-19. Health Qual. Life Outcomes 2021, 19, 1–12. [Google Scholar] [CrossRef]
- Płomecka, M.B.; Gobbi, S.; Neckels, R.; Radziński, P.; Skórko, B.; Lazzeri, S.; Dedic, A.; Bakalovic, A.; Hrustic, L.; Alp, A.B.; et al. Mental health impact of COVID-19: A global study of risk and resilience factors. medRxiv 2020. [Google Scholar] [CrossRef]
- Rodríguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological impact and associated factors during the initial stage of the coronavirus (COVID-19) pandemic among the general population in Spain. Front. Psychol. 2020, 11, 1540. [Google Scholar] [CrossRef]
- Bruine de Bruin, W.; Bennett, D. Relationships between initial COVID-19 risk perceptions and protective health behaviors: A national survey. Am. J. Prev. Med. 2020, 59, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Soffer, M. The role of stress in the relationships between gender and health-promoting behaviours. Scand. J. Caring Sci. 2010, 24, 572–580. [Google Scholar] [CrossRef]
- Kim, S.; Kim, J.H.; Park, Y.; Kim, S.; Kim, C.Y. Gender Analysis of COVID-19 Outbreak in South Korea: A Common Challenge and Call for Action. Health Educ. Behav. 2020, 47, 525–530. [Google Scholar] [CrossRef]
- Mahalik, J.R.; Burns, S.M.; Syzdek, M. Masculinity and perceived normative health behaviors as predictors of men’s health behaviors. Soc. Sci. Med. 2007, 64, 2201–2209. [Google Scholar] [CrossRef] [PubMed]
- Verbrugge, L.M.; Wingard, D.L. Sex differentials in health and mortality. Women Health 1987, 12, 103–145. [Google Scholar] [CrossRef] [PubMed]
- García-Tascón, M.; Sahelices-Pinto, C.; Mendaña-Cuervo, C.; Magaz-González, A.M. The Impact of the COVID-19 Confinement on the Habits of PA Practice According to Gender (Male/Female): Spanish Case. Int. J. Environ. Res. Public Health. 2020, 17, 6961. [Google Scholar] [CrossRef]
- Grzywacz, J.G.; Stoller, E.P.; Brewer-Lowry, A.N.; Bell, R.A.; Quandt, S.A.; Arcury, T.A. Gender and health lifestyle: An in-depth exploration of self-care activities in later life. Health Educ. Behav. 2012, 39, 332–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, C.; Quintus, M.; Egloff, B.; Luong, G.; Riediger, M.; Wrzus, C. Same old, same old? Age differences in the diversity of daily life. Psychol. Aging 2020, 353, 434–448. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, A.; Kadić-Maglajlić, S. The mediating role of health consciousness in the relation between emotional intelligence and health behaviors. Front. Psychol. 2018, 9, 2161. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.M.; Arnold, W. Health promoting behaviors of older Americans versus young and middle-aged adults. Educ. Gerontol. 2004, 30, 835–844. [Google Scholar] [CrossRef]
- Stapley, E.; Demkowicz, O.; Eisenstadt, M.; Wolpert, M.; Deighton, J. Coping with the stresses of daily life in England: A qualitative study of self-care strategies and social and professional support in early adolescence. J. Early Adolesc. 2020, 40, 605–632. [Google Scholar] [CrossRef]
- Chesser, A.; Drassen Ham, A.; Keene Woods, N. Assessment of COVID-19 Knowledge Among University Students: Implications for Future Risk Communication Strategies. Health Educ. Behav. 2020, 47, 540–543. [Google Scholar] [CrossRef]
- Abrams, D.; Wetherell, M.; Cochrane, S.; Hogg, M.A.; Turner, J.C. Knowing what to think by knowing who you are: Self-categorization and the nature of norm formation, conformity and group polarization. Br. J. Soc. Psychol. 1990, 29, 97–119. [Google Scholar] [CrossRef]
- Stolow, J.A.; Moses, L.M.; Lederer, A.M.; Carter, R. How fear appeal approaches in COVID-19 health communication may be harming the global community. Health Educ. Behav. 2020, 47, 531–535. [Google Scholar] [CrossRef]
- Schultz, P.W.; Nolan, J.M.; Cialdini, R.B.; Goldstein, N.J.; Griskevicius, V. The constructive, destructive, and reconstructive power of social norms. Psychol. Sci. 2007, 18, 429–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibley, C.G.; Greaves, L.M.; Satherley, N.; Wilson, M.S.; Overall, N.C.; Lee, C.H.J.; Milojev, P.; Bulbulia, J.; Osborne, D.; Milfont, T.L.; et al. Effects of the COVID-19 pandemic and nationwide lockdown on trust, attitudes toward government, and well-being. Am. Psychol. 2020, 75, 618–630. [Google Scholar] [CrossRef]
- Van den Broucke, S. Why health promotion matters to the COVID-19 pandemic, and vice versa. Health Promot. Int. 2020, 35, 181–186. [Google Scholar] [CrossRef] [Green Version]
- Shim, R.S.; Compton, M.T. The Social Determinants of Mental Health: Psychiatrists’ Roles in Addressing Discrimination and Food Insecurity. Am. Psychiatr. Publ. 2020, 18, 25–30. [Google Scholar] [CrossRef]
- Arora, T.; Grey, I. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. J. Health Psychol. 2020, 25, 1155–1163. [Google Scholar] [CrossRef]
- Brownson, R.C.; Seiler, R.; Eyler, A.A. Measuring the impact of public health policy. Prev. Chronic Dis. 2010, 7, A77. [Google Scholar] [PubMed]
- Jacques-Aviñó, C.; López-Jiménez, T.; Medina-Perucha, L.; de Bont, J.; Gonçalves, A.Q.; Duarte-Salles, T.; Berenguera, A. Gender-based approach on the social impact and mental health in Spain during COVID-19 lockdown: A cross-sectional study. BMJ Open. 2020, 10, e044617. [Google Scholar] [CrossRef] [PubMed]
- Ryan, N.E.; El Ayadi, A.M. A call for a gender-responsive, intersectional approach to address COVID-19. Glob. Public Health. 2020, 15, 1404–1412. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health Promotion Glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Spain | Chile | Colombia | Ecuador | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18–28 | 29–39 | 40–49 | 50–59 | <60 | 18–28 | 29–39 | 40–49 | 50–59 | <60 | 18–28 | 29–39 | 40–49 | 50–59 | <60 | 18–28 | 29–39 | 40–49 | 50–59 | <60 | ||
| 57(21) | 55(20) | 54(20) | 50(18) | 55(20) | 56(21.5) | 53(20.3) | 56(21.5) | 45(17) | 51(19.5) | 56(21) | 54(20) | 56(21) | 51(19) | 51(19) | 64(23) | 55(19.5) | 57(20) | 54(19.1) | 52(18) | ||
| Spain | Chile | Colombia | Ecuador | ||||||||||||||||||
| Female | Male | Total | Female | Male | Total | Female | Male | Total | Female | Male | Total | Full Sample | |||||||||
| N (%) | 136(50.2) | 135(49.8) | 271 | 127(48.7) | 134(51.4) | 261 | 131(48.9) | 147(51.1) | 268 | 137(48.6) | 145(51.4) | 282 | 1082 | ||||||||
| Income n (%) | |||||||||||||||||||||
| No salary | 22(16.2) | 23(17) | 45(16.6) | 19(15.0) | 8(6.0) | 27(10.3) | 21(16) | 22(16.1) | 43(16.0) | 23(16.8) | 20(13.8) | 43(15.2) | 158(14.6) | ||||||||
| One mw | 4(2.9) | 5(3.7) | 9(3.3) | 13(10.2) | 9(6.7) | 22(8.4) | 21(16) | 16(11.7) | 37(13.8) | 12(8.8) | 7(4.8) | 19(6.7) | 87(8) | ||||||||
| Two mw | 20(14.7) | 10(7.4) | 30(11) | 21(16.5) | 15(11.2) | 36(13.8) | 19(14.5) | 18(13.1) | 37(13.8) | 26(19.0) | 16(11.0) | 42(15) | 145(13.4) | ||||||||
| Three mw | 28(20.7) | 22(16.3) | 50(18.5) | 14(11.0) | 21(15.7) | 35(13.4) | 34(26.0) | 34(24.8) | 68(25.3) | 26(19.0) | 10(6.9) | 36(12.7) | 189(17.5) | ||||||||
| Four mw | 30(22.1) | 29(21.6) | 59(21.7) | 15(11.8) | 19(14.2) | 34(13) | 14(10.7) | 16(11.7) | 30(12.0) | 26(19.0) | 26(17.9) | 52(18.4) | 175(16.2) | ||||||||
| Five mw | 32(23.5) | 46(34.1) | 78(28.8) | 45(35.4) | 62(46.3) | 107(41) | 22(16.8) | 31(22.6) | 53(19.7) | 24(17.5) | 66(45.6) | 90(32) | 328(30.3) | ||||||||
| Educational Level n (%) | |||||||||||||||||||||
| Elementary | 1(0.7) | 3(2.2) | 4(1.48) | 2(1.6) | 2(1.5) | 4(1.53) | 0(0.0) | 1(0.7) | 1(0.4) | 2(1.5) | 0(0) | 2(0.7) | 11(1) | ||||||||
| High School | 20(14.7) | 22(16.3) | 42(15.5) | 12(9.4) | 16(11.9) | 28(7.0) | 14(10.7) | 21(15.3) | 35(13.5) | 20(14.6) | 28(19.3) | 48(17.0) | 153(14.1) | ||||||||
| Technical | 18(13.2) | 19(14.1) | 37(13.7) | 18(14.2) | 15(11.2) | 33(12.7) | 16(12.2) | 24(17.5) | 40(15.3) | 7(5.1) | 5(3.4) | 12(4.3) | 122(11.3) | ||||||||
| University | 97(71.3) | 91(67.4) | 188(69.3) | 95(74.8) | 101(75.4) | 196(75.1) | 101(77.1) | 91(66.4) | 192(74.5) | 108(78.8) | 112(77.2) | 220(78.0) | 796(73.6) | ||||||||
| COVID-19 variables n (%) | |||||||||||||||||||||
| Frontline workers (yes) | 34(25) | 46(34.1) | 80(29.5) | 36(28.3) | 44(32.8) | 80(30.7) | 70(53.4) | 61(44.5) | 131(48.9) | 35(25.5) | 41(28.3) | 76(27) | 367(33.9) | ||||||||
| Health risk factors (yes) | 39(28.7) | 50(37) | 89(32.8) | 33(26) | 51(38.1) | 84(32.2) | 44(33.6) | 33(24.1) | 77(28.7) | 31(22.6) | 56(38.6) | 87(30.9) | 337(31.1) | ||||||||
| Employment changes (yes) | 21(15.4) | 25(18.5) | 46(17) | 32(25.2) | 19(14.2) | 51(19.5) | 41(31.3) | 46(33.6) | 87(32.4) | 41(30) | 46(31.7) | 87(31) | 271(25) | ||||||||
| Accompanied during lockdown (yes) | 114(83.8) | 117(86.7) | 231(85.2) | 117(92.1) | 120(89) | 237(91) | 130(95) | 136(94) | 266(99.2) | 121(92.4) | 127(92.7) | 248(88) | 982(90.8) | ||||||||
| Community resources (yes) | 120(88.2) | 125(92.6) | 245(90.4) | 102(80.3) | 113(84.3) | 233(89.2) | 109(83.2) | 116(85) | 225(84) | 118(86.1) | 133(91.7) | 251(89) | 936(85.5) | ||||||||
| Children in charge (yes) | 32(23.5) | 31(23) | 63(23.2) | 48(37.8) | 38(28.4) | 86(33) | 37(28.2) | 56(41) | 93(34.7) | 47(34.3) | 48(33.1) | 95(33.6) | 337(31.1) | ||||||||
| Older people in charge (yes) | 15(11) | 14(10.4) | 29(10.7) | 37(30) | 20(15) | 57(22) | 53(40.5) | 53(38.7) | 106(39.5) | 47(34.3) | 48(33.1) | 95(33.6) | 287(26.5) | ||||||||
| Confinement days M (SD) | 21(4.6) | 17.5(6.5) | 17(4.0) | 25(0.6) | |||||||||||||||||
| Variable (Likert Scale) | ANOVA | Mean Comparison | Dif Mean | Error | p Value | 95% CI | |
|---|---|---|---|---|---|---|---|
| Perceived stress (1–6) | Inter-gender by age, F(4) = 2.88, p = 0.02 | Female 18–28 vs. male | 20.96 | 0.92 | 0.002 | 10.34 | 40.78 |
| F(4) = 6.71, p < 0.001 | Female 18–28 vs. 40–49 | 30.12 | 0.89 | 0.005 | 0.62 | 50.62 | |
| Female 18–28 vs. 50–59 | 30.47 | 0.91 | 0.002 | 0.91 | 60.04 | ||
| Female 18–28 vs. <60 | 30.96 | 0.92 | 0.000 | 10.37 | 60.56 | ||
| Female 29–39 vs. <60 | 20.62 | 0.86 | 0.024 | 0.19 | 50.04 | ||
| F(4) = 6.83, p < 0.001 | Colombia vs. Chile | −20.03 | 0.55 | 0.001 | −30.47 | −0.59 | |
| Colombia vs. Spain | −20.17 | 0.54 | 0.000 | −30.59 | −0.76 | ||
| Seriousness perception of COVID-19 pandemic (1–4) | Age x gender F(4) = 8.14, p < 0.001 | Males 18–28 vs. 50–59 | 0.29 | 0.81 | 0.003 | 0.07 | 0.53 |
| Males 18–28 vs. >60 | 0.28 | 0.004 | 0.009 | 0.04 | 0.49 | ||
| Males 40–49 vs. 50–59 | 0.37 | 0.08 | <0.001 | 0.14 | 0.61 | ||
| Male 40–49 vs. >60 | 0.34 | 0.08 | <0.001 | 0.12 | 0.57 | ||
| F(1) = 6.44, p = 0.01 | Female 18–28 vs. Male | −0.20 | 0.07 | 0.012 | −0.34 | −0.04 | |
| F(1) = 10.15, p = 0.002 | Female 50–59 vs. Male | 0.27 | 0.08 | 0.002 | 0.10 | 0.43 | |
| Public health guidelines (1–6) | Inter-gender by age and country F(4) = 6.48, p = 0.01 | 40–49 Colombian females vs. males | −0.29 | 0.13 | 0.029 | −0.54 | −0.03 |
| 50–59 Colombian females vs. males | 0.53 | 0.21 | 0.014 | 0.11 | 0.95 | ||
| F(4) = 7.05, p = 0.01 | 18–28 Ecuadorian females vs. males | −0.63 | 0.24 | 0.010 | −10.11 | −0.16 | |
| 29–39 Ecuadorian females vs. males | −0.43 | 0.17 | 0.012 | −0.77 | −0.10 | ||
| 50–59 Ecuadorian females vs. males | 0.29 | 0.13 | 0.036 | 0.02 | 0.56 | ||
| F(4) = 6.27, p = 0.01 | >60 Chilean females vs. males | −0.39 | 0.16 | 0.016 | −0.70 | −0.08 | |
| F(4) = 5.90, p = 0.01 | 29–39 Spanish females vs. males | −0.30 | 0.12 | 0.018 | −0.55 | −0.05 | |
| F(4) = 5.43, p = 0.24 | >60 Spanish females vs. males | 0.53 | 0.23 | 0.024 | 0.07 | 0.09 | |
| Inter-age by gender and country F(4) = 4.24, p = 0.003 | Ecuadorian females de 18–28 vs. 40–49 | −0.62 | 0.21 | 0.035 | −10.22 | −0.03 | |
| Ecuadorian females de 18–28 vs. 50–59 | −0.81 | 0.22 | 0.003 | −10.42 | −0.19 | ||
| F(4) = 3.98, p = 0.004 | Spanish females 40–49 females 50–59 | −0.56 | 0.17 | 0.017 | −10.06 | −0.06 | |
| Spanish females 40–49 females 50–59 | −0.54 | 0.18 | 0.031 | −10.05 | −0.03 | ||
| F(4) = 4.50, p = 0.002 | Spanish males 29–39 vs. males >60 | 0.61 | 0.19 | 0.012 | 0.08 | 10.14 | |
| Spanish males 40–49 vs. males >60 | 0.60 | 0.19 | 0.017 | 0.06 | 10.14 | ||
| Inter-country by gender and age F(4) = 5.17, p = 0.002 | 50–59 Ecuadorian female vs. Spanish | 0.57 | 0.16 | 0.004 | 0.13 | 10.01 | |
| 50–59 Chilean males vs. Colombian | 0.56 | 0.20 | 0.035 | 0.03 | 10.10 | ||
| >60 Chilean males vs. Spanish | 0.59 | 0.21 | 0.036 | 0.02 | 10.16 | ||
| Healthy daily routines (1–6) | Inter-gender by age and country F(1) = 15.32, p < 0.001 | 29–39 Colombian females vs. males | 10.39 | 0.36 | <0.001 | 0.68 | 20.11 |
| F(1) = 6.42, p = 0.02 | 50–59 Colombian females vs. males | 0.94 | 0.37 | 0.015 | 0.20 | 10.69 | |
| F(1) = 6.63, p = 0.01 | 50–59 Chilean females vs. males | −10.10 | 0.43 | 0.014 | −10.95 | −0.24 | |
| F(1) = 8.35, p = 0.006 | >60 Chilean females vs. males | −10.01 | 0.35 | 0.006 | −10.72 | −0.31 | |
| F(1) = 7.56, p = 0.008 | >60 Spanish females vs. males | 0.74 | 0.27 | 0.008 | 0.20 | 10.28 | |
| Inter-age by gender a country, F(4) = 6.42, p = 0.02 | Colombian females 18–28 vs. 50–59 | −10.12 | 0.39 | 0.046 | −20.23 | −0.01 | |
| F(4) = 3.92, p = 0.005 | Spanish females 40–49 vs. 50–59 | 0.93 | 0.31 | 0.032 | 0.05 | 10.82 | |
| Spanish females 50–59 vs. >60 | −10.15 | 0.32 | 0.004 | −20.07 | −0.24 | ||
| F(4) = 3.09, p = 0.02 | Spanish males 29–39 vs. 50–59 | 0.97 | 0.34 | 0.046 | 0.01 | 10.93 | |
| Inter-country by age and gender F(1) = 4.08, p = 0.009 | 29–39 Colombian females vs. Ecuadorian | 10.06 | 0.37 | 0.028 | 0.07 | 20.05 | |
| F(4) = 4.57, p = 0.005 | 50–59 Colombian females vs. Spanish | 10.21 | 0.41 | 0.022 | 0.11 | 20.31 | |
| 50–59 Colombian females vs. Chilean | 10.28 | 0.43 | 0.022 | 0.12 | 20.44 | ||
| F(3) = 3.44, p = 0.02 | Spanish females >60 vs. Chilean | 10.18 | 0.40 | 0.023 | 0.11 | 20.24 | |
| F(3) = 8.44, p < 0.001 | Colombian males 29–39 vs. Chilean | −0.93 | 0.32 | 0.024 | −10.78 | −0.08 | |
| Colombian males 29–39 vs. Spanish | −10.59 | 0.32 | 0.000 | −20.45 | −0.74 | ||
| Health consciousness (1–6) | Inter-gender by country, F(1) = 7.36, p = 0.007 | Colombian females vs. Colombian | −10.60 | 0.59 | 0.007 | −20.76 | −0.44 |
| F(1) = 13.80, p < 0.001 | Ecuadorian females vs. males | −20.11 | 0.57 | 0.000 | −30.23 | −0.99 | |
| Intra-gender by age F(4) = 6.57, p < 0.001 | Female 18–28 vs. female 50–59 | −10.91 | 0.67 | 0.047 | −30.80 | −0.02 | |
| Female 18–28 vs. female >60 | −30.44 | 0.67 | <0.001 | −50.33 | −10.54 | ||
| F(4) = 4.09, p < 0.001 | Males 18–28 vs. males 29–39 | −10.75 | 0.62 | 0.050 | −30.49 | 0.00 | |
| Males 18–28 vs. males 40–49 | −20.32 | 0.63 | 0.002 | −40.09 | −0.55 | ||
| Males 18–28 vs. males 50–59 | −10.89 | 0.64 | 0.031 | −30.69 | −0.10 | ||
| Inter-gender by age, F(1) = 4.69, p = 0.03 | Females 18–28 vs. males 18–28 | −10.35 | 0.62 | 0.031 | −20.58 | −0.12 | |
| F(1) = 5.58, p = 0.02 | Females 29–39 vs. males 29–39 | −10.42 | 0.60 | 0.019 | −20.61 | −0.24 | |
| F(1) = 9.18, p = 0.003 | Females 40–49 vs. males 40–49 | −10.87 | 0.62 | 0.003 | −30.09 | −0.66 | |
| F(1) = 3.96, p = 0.05 | Females 50–59 vs. males 50–59 | −10.34 | 0.67 | 0.048 | −20.66 | −0.01 | |
| Nutrition and physical activity (1–6) | Age main effect F(4) = 4.66, p = 0.001 | 18–28 vs. 29–39 | 10.21 | 0.41 | 0.029 | −20.35 | −0.07 |
| 18–28 vs. >60 | 10.39 | 0.42 | 0.009 | 0.21 | 20.56 | ||
| 40–49 vs. >60 | 10.19 | 0.42 | 0.041 | 0.03 | 20.37 | ||
| Country main effect, F(3) = 4.16, p = 0.006 | Ecuador vs. Spain | −10.24 | 0.37 | 0.005 | −20.21 | −0.27 | |
| Sleep (1–6) | Inter-age by country F(4) = 3.55, p = 0.008 | Chilean 29–39 vs. 40–49 | −10.35 | 0.45 | 0.031 | −20.63 | −0.70 |
| Chilean 29–39 vs. >60 | −10.41 | 0.46 | 0.025 | −20.72 | −0.10 | ||
| F(4) = 2.99, p = 0.02 | Ecuadorian 18–28 vs. 29–39 | 10.33 | 0.43 | 0.021 | 0.12 | 20.54 | |
| Inter-country by age F(3) = 4.66, p = 0.003 | Ecuadorian 29–39 vs. Spain 29–39 | −10.53 | 0.50 | 0.005 | −30.01 | −0.36 | |
| Chilean 29–39 vs. Spain 29–39 | −10.53 | 0.50 | 0.016 | −20.87 | −0.18 | ||
| Intra and interpersonal coping skills (1–6) | Intra-gender by age, F(4) = 3.23, p = 0.01 | Female 40–49 vs. >60 | −10.57 | 0.47 | 0.008 | −20.88 | −0.25 |
| F(4) = 2.41, p = 0.05 | Male 18–28 vs. >60 | 10.40 | 0.48 | 0.034 | 0.06 | 20.74 | |
| Inter-gender by age, F(1) = 10.94, p = 0.001 | >60 Female vs. male | 10.62 | 0.49 | 0.001 | −0.65 | 20.58 | |
| Country main effect, F(3) = 2.98, p = 0.03 | Ecuador vs. Spain | −10.24 | 0.37 | 0.005 | −20.21 | −0.27 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bermejo-Martins, E.; Luis, E.O.; Sarrionandia, A.; Martínez, M.; Garcés, M.S.; Oliveros, E.Y.; Cortés-Rivera, C.; Belintxon, M.; Fernández-Berrocal, P. Different Responses to Stress, Health Practices, and Self-Care during COVID-19 Lockdown: A Stratified Analysis. Int. J. Environ. Res. Public Health 2021, 18, 2253. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052253
Bermejo-Martins E, Luis EO, Sarrionandia A, Martínez M, Garcés MS, Oliveros EY, Cortés-Rivera C, Belintxon M, Fernández-Berrocal P. Different Responses to Stress, Health Practices, and Self-Care during COVID-19 Lockdown: A Stratified Analysis. International Journal of Environmental Research and Public Health. 2021; 18(5):2253. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052253
Chicago/Turabian StyleBermejo-Martins, Elena, Elkin O. Luis, Ainize Sarrionandia, Martín Martínez, María Sol Garcés, Edwin Y. Oliveros, Cristian Cortés-Rivera, Maider Belintxon, and Pablo Fernández-Berrocal. 2021. "Different Responses to Stress, Health Practices, and Self-Care during COVID-19 Lockdown: A Stratified Analysis" International Journal of Environmental Research and Public Health 18, no. 5: 2253. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052253