
A Meta-Analysis of the Efficacy of Hyaluronic Acid Eye Drops for the Treatment of Dry Eye Syndrome


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
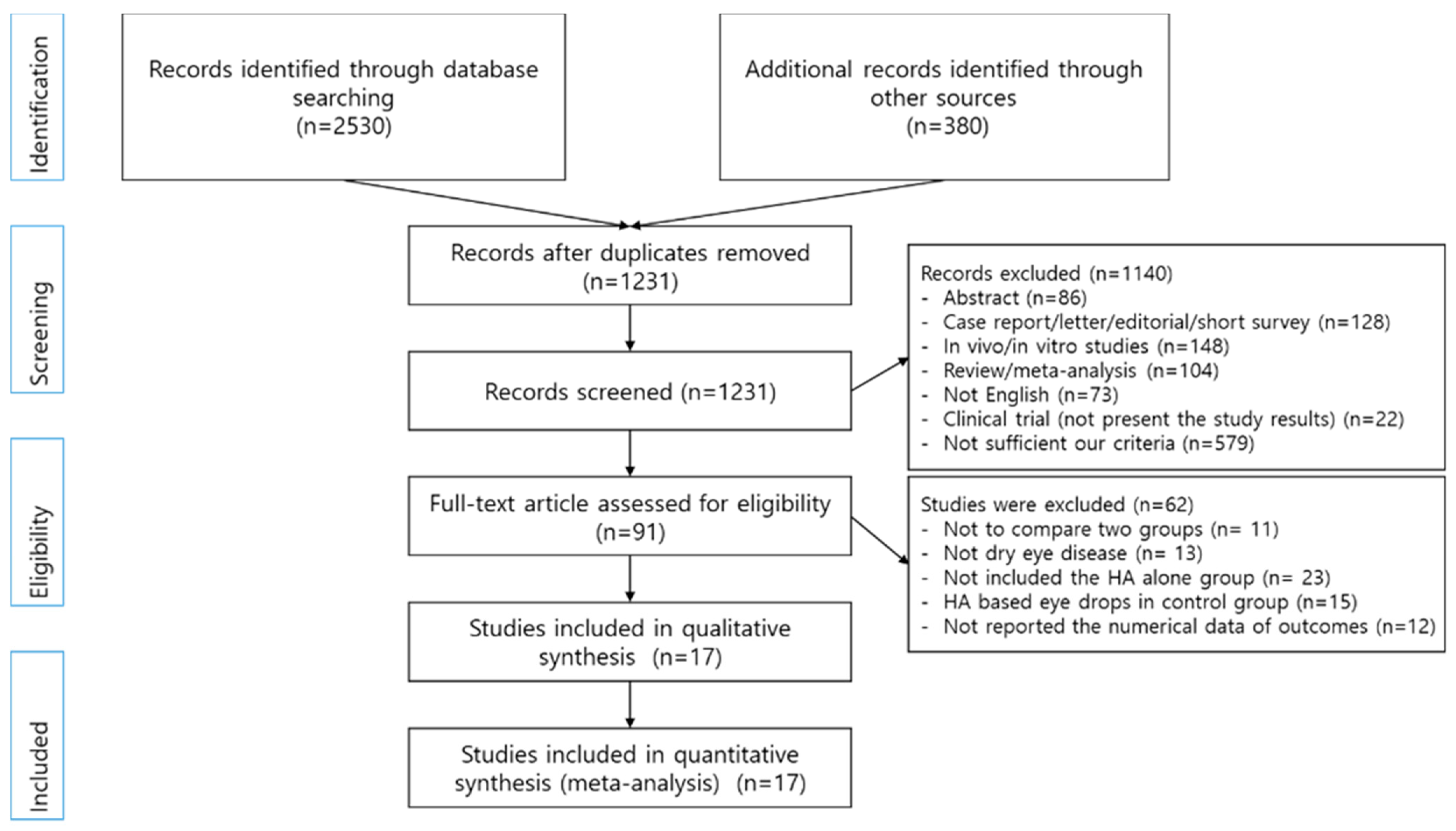
3.1. Literature Retrieval Results
3.2. Study Characteristics
3.3. Methodological Quality Assessment
3.4. Quantitative Analysis
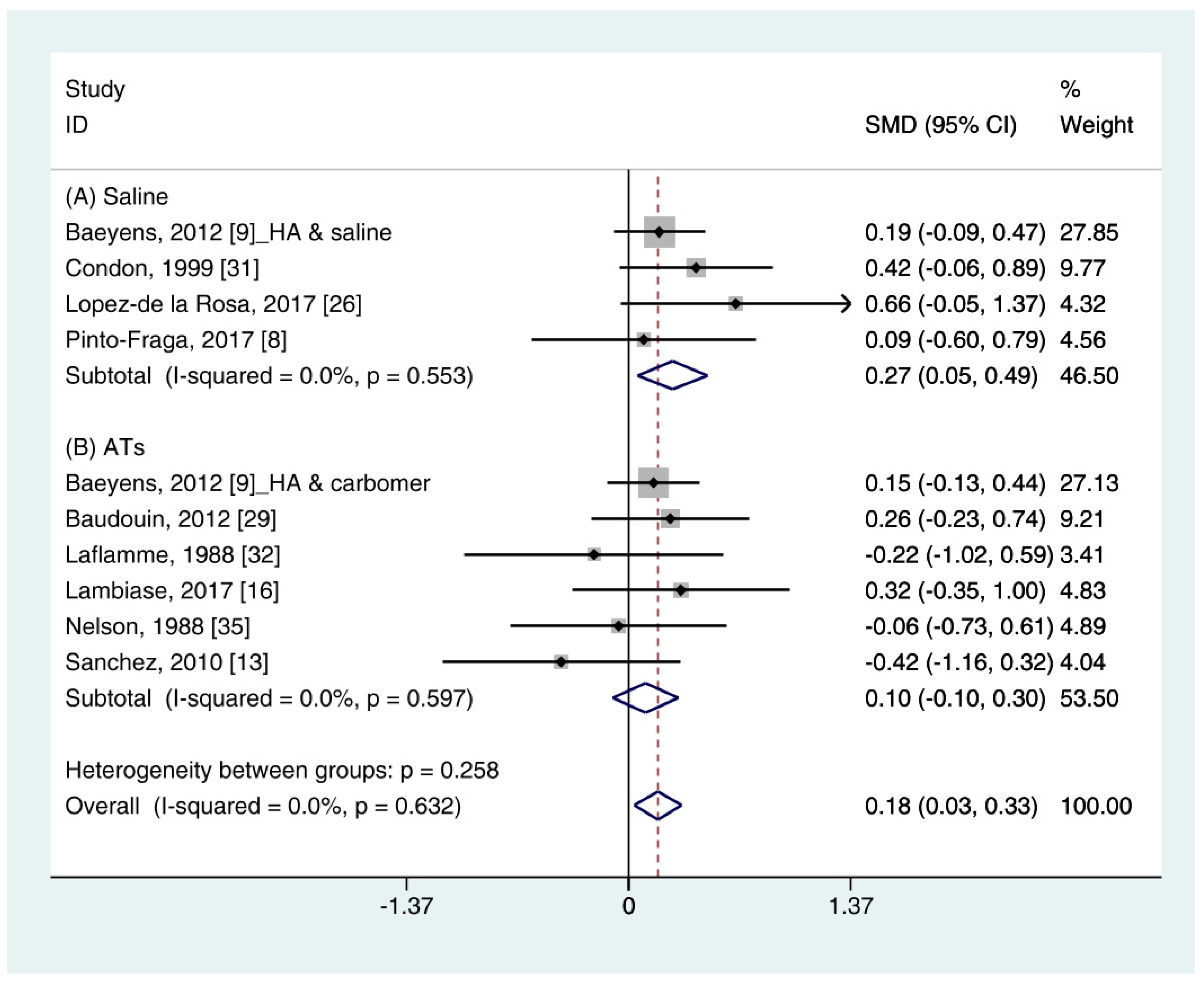
3.4.1. Schirmer’s (SH) Test
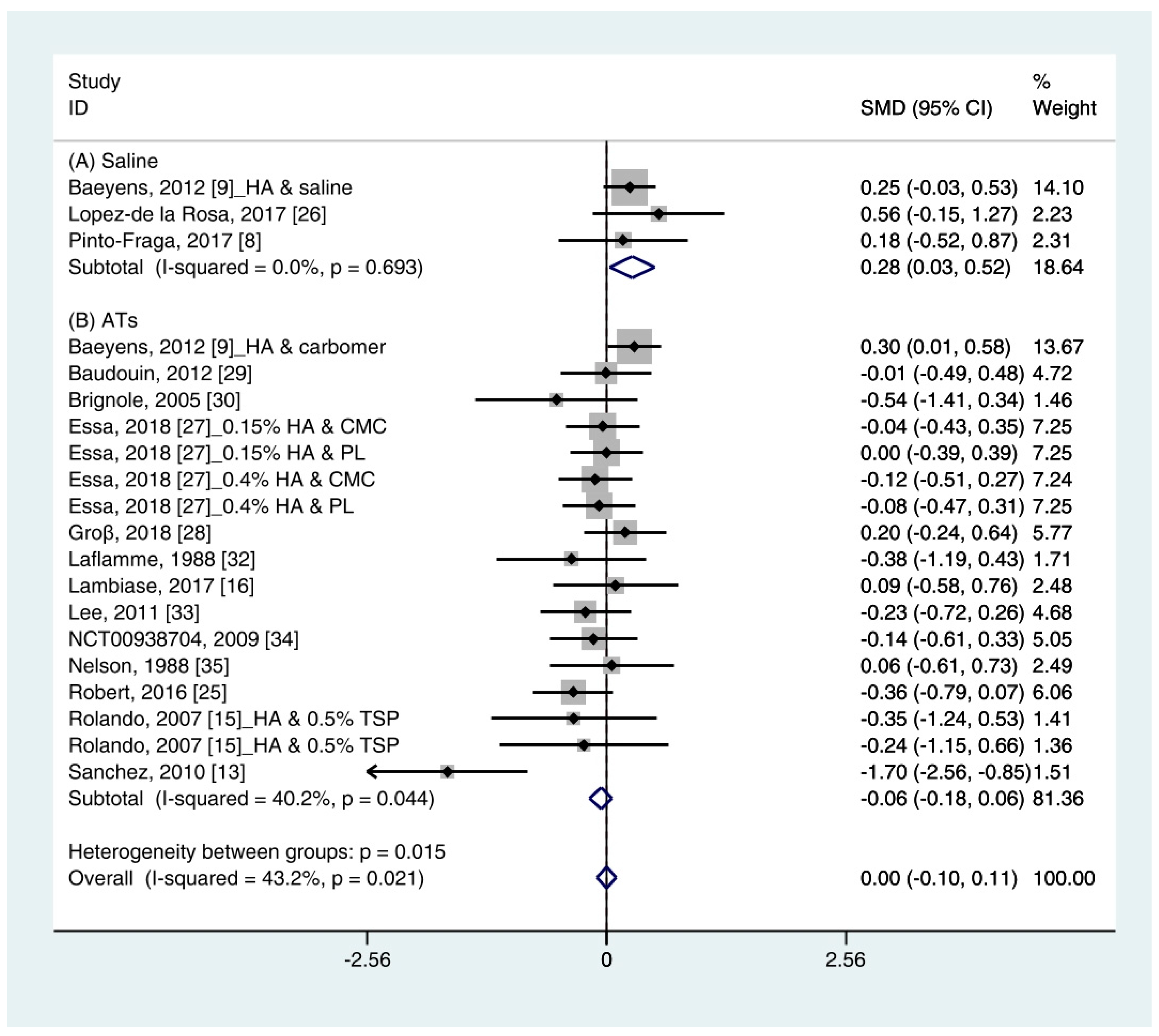
3.4.2. Tear Break-Up Time (TBUT)
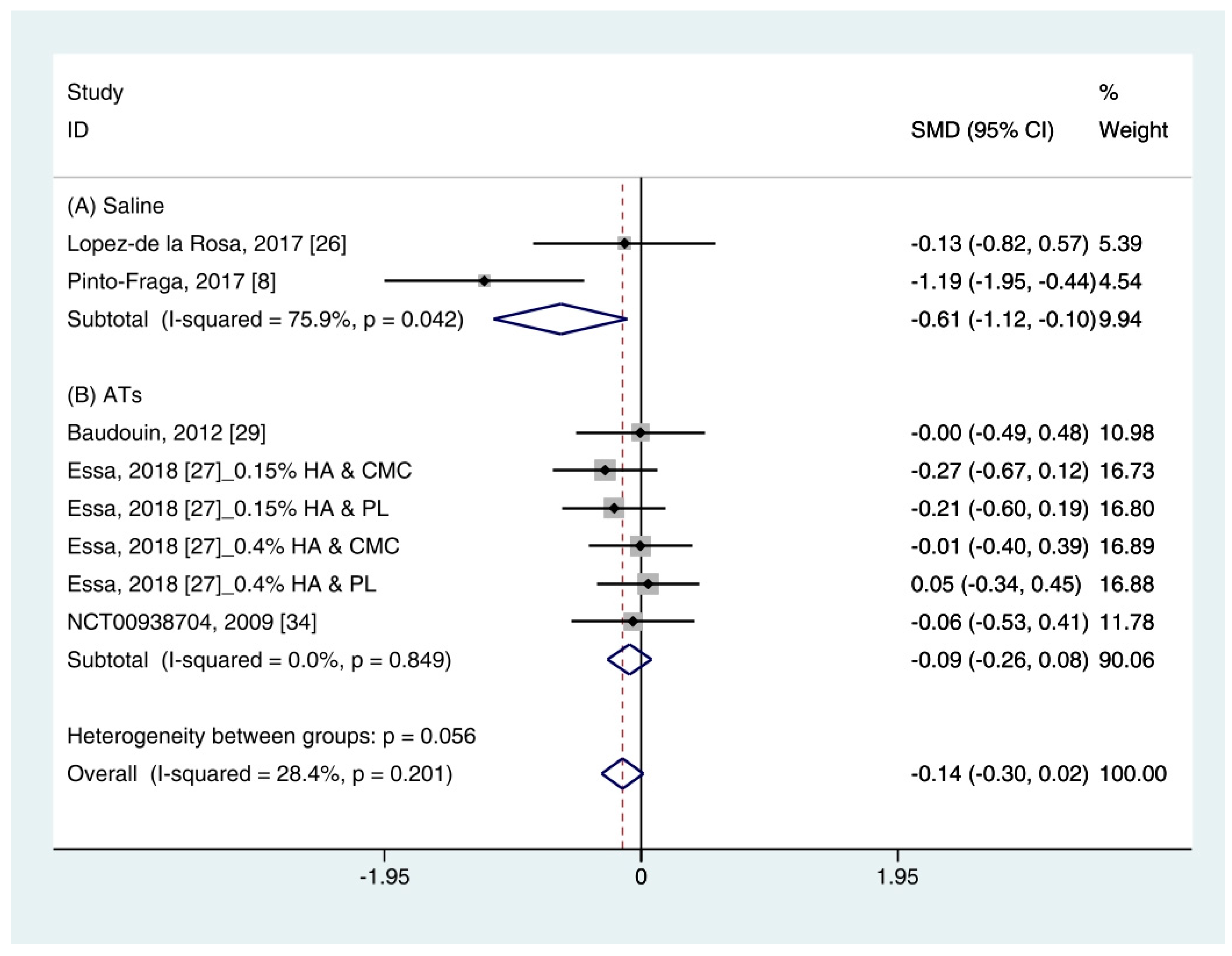
3.4.3. Corneal Fluorescein Staining Score
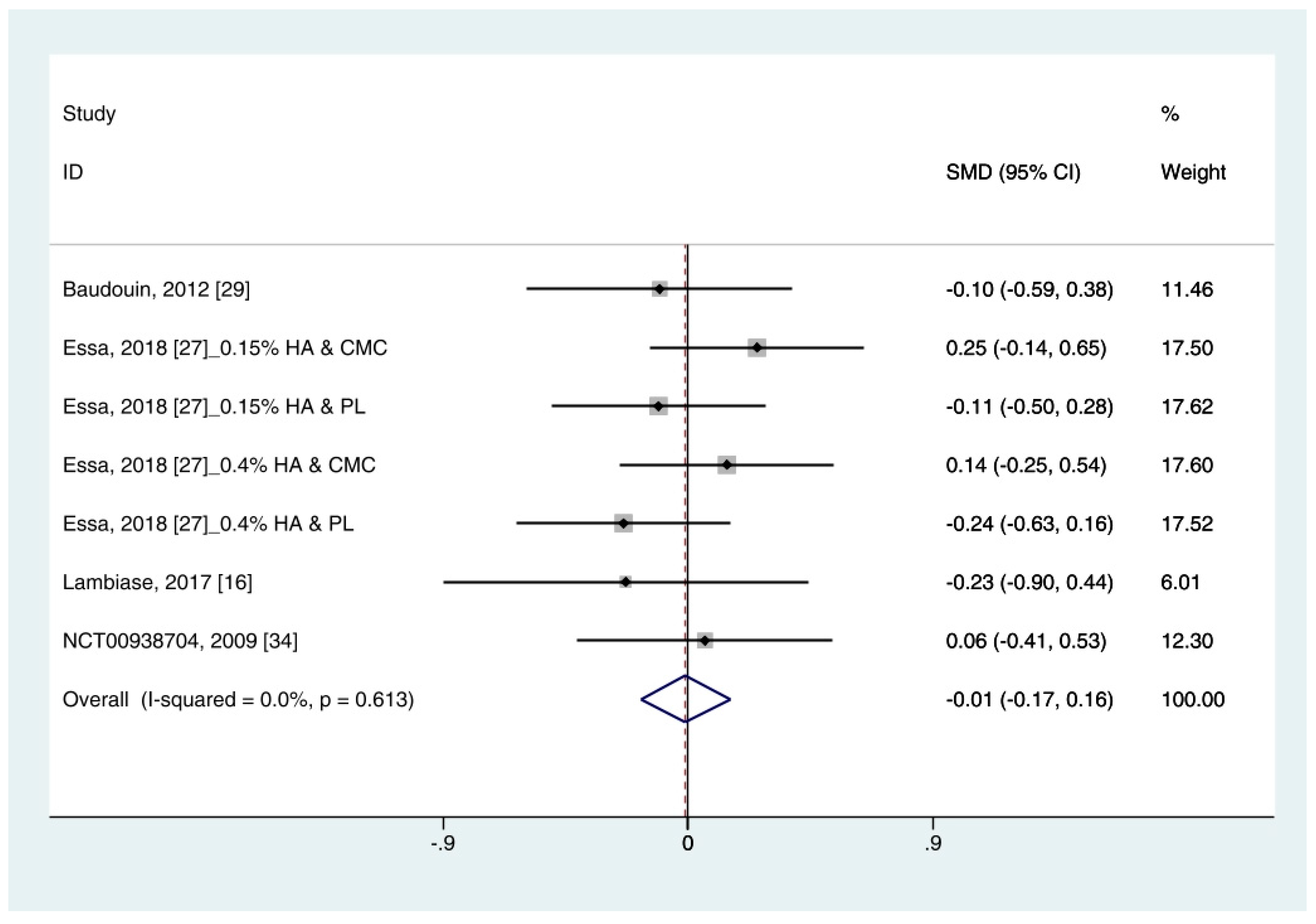
3.4.4. Ocular Surface Disease Index (OSDI)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- DEWS. The definition and classification of dry eye disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 75–92. [Google Scholar] [CrossRef]
- International Dry Eye WorkShop Study Group. The epidemiology of dry eye disease: Report of the Epidemiology Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 93–107. [Google Scholar] [CrossRef]
- Johnson, M.E.; Murphy, P.J. Changes in the tear film and ocular surface from dry eye syndrome. Prog. Retin. Eye Res. 2004, 23, 449–474. [Google Scholar] [CrossRef]
- Messmer, E.M. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch. Arztebl. Int. 2015, 112, 71–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.; Nichols, K.K.; Baldwin, E.K. Current patterns in the use of diagnostic tests in dry eye evaluation. Cornea 2008, 27, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-Del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. TFOS DEWS II Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef] [PubMed]
- Dogru, M.; Tsubota, K. Pharmacotherapy of dry eye. Expert Opin. Pharmacother. 2011, 12, 325–334. [Google Scholar] [CrossRef]
- DEWS. Management and therapy of dry eye disease: Report of the Management and Therapy Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 163–178. [Google Scholar] [CrossRef]
- Meyer, K. Chemical structure of hyaluronic acid. Fed. Proc. 1958, 17, 1075–1077. [Google Scholar]
- Shimmura, S.; Ono, M.; Shinozaki, K.; Toda, I.; Takamura, E.; Mashima, Y.; Tsubota, K. Sodium hyaluronate eyedrops in the treatment of dry eyes. Br. J. Ophthalmol. 1995, 79, 1007–1011. [Google Scholar] [CrossRef] [Green Version]
- Pinto-Fraga, J.; Lopez-de la Rosa, A.; Blazquez Arauzo, F.; Urbano Rodriguez, R.; Gonzalez-Garcia, M.J. Efficacy and Safety of 0.2% Hyaluronic Acid in the Management of Dry Eye Disease. Eye Contact Lens 2017, 43, 57–63. [Google Scholar] [CrossRef]
- Baeyens, V.; Bron, A.; Baudouin, C.; Vismed/Hylovis Study Group. Efficacy of 0.18% hypotonic sodium hyaluronate ophthalmic solution in the treatment of signs and symptoms of dry eye disease. J. Fr. Ophtalmol. 2012, 35, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Vogel, R.; Crockett, R.S.; Oden, N.; Laliberte, T.W.; Molina, L.; Sodium Hyaluronate Ophthalmic Solution Study Group. Demonstration of efficacy in the treatment of dry eye disease with 0.18% sodium hyaluronate ophthalmic solution (vismed, rejena). Am. J. Ophthalmol. 2010, 149, 594–601. [Google Scholar] [CrossRef]
- Troiano, P.; Monaco, G. Effect of hypotonic 0.4% hyaluronic acid drops in dry eye patients: A cross-over study. Cornea 2008, 27, 1126–1130. [Google Scholar] [CrossRef] [PubMed]
- You, I.C.; Li, Y.; Jin, R.; Ahn, M.; Choi, W.; Yoon, K.C. Comparison of 0.1%, 0.18% and 0.3% Hyaluronic Acid Eye Drops in the Treatment of Experimental Dry Eye. J. Ocul. Pharmacol. Ther. 2018, 34, 557–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, M.A.; Torralbo-Jimenez, P.; Giron, N.; de la Heras, B.; Herrero Vanrell, R.; Arriola-Villalobos, P.; Diaz-Valle, D.; Alvarez-Barrientos, A.; Benitez-Del-Castillo, J.M. Comparative analysis of carmellose 0.5% versus hyaluronate 0.15% in dry eye: A flow cytometric study. Cornea 2010, 29, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Mihaltz, K.; Faschinger, E.M.; Vecsei-Marlovits, P.V. Effects of Lipid-Versus Sodium Hyaluronate-Containing Eye Drops on Optical Quality and Ocular Surface Parameters as a Function of the Meibomian Gland Dropout Rate. Cornea 2018, 37, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Rolando, M.; Valente, C. Establishing the tolerability and performance of tamarind seed polysaccharide (TSP) in treating dry eye syndrome: Results of a clinical study. BMC Ophthalmol. 2007, 7, 5. [Google Scholar] [CrossRef] [Green Version]
- Lambiase, A.; Sullivan, B.D.; Schmidt, T.A.; Sullivan, D.A.; Jay, G.D.; Truitt, E.R., 3rd; Bruscolini, A.; Sacchetti, M.; Mantelli, F. A Two-Week, Randomized, Double-masked Study to Evaluate Safety and Efficacy of Lubricin (150 mug/mL) Eye Drops Versus Sodium Hyaluronate (HA) 0.18% Eye Drops (Vismed(R)) in Patients with Moderate Dry Eye Disease. Ocul. Surf. 2017, 15, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, S.; Oshiden, K.; Awamura, S.; Suzuki, H.; Nakamichi, N.; Yokoi, N. A randomized, multicenter phase 3 study comparing 2% rebamipide (OPC-12759) with 0.1% sodium hyaluronate in the treatment of dry eye. Ophthalmology 2013, 120, 1158–1165. [Google Scholar] [CrossRef]
- Ang, B.C.H.; Sng, J.J.; Wang, P.X.H.; Htoon, H.M.; Tong, L.H.T. Sodium Hyaluronate in the Treatment of Dry Eye Syndrome: A Systematic Review and Meta-Analysis. Sci. Rep. 2017, 7, 9013. [Google Scholar] [CrossRef] [Green Version]
- Kong, X.; Yan, C.; Ma, W.; Li, Y.; Xing, B.; Yang, Y.; Wang, R. Sodium hyaluronate’s effect on xerophthalmia: A meta-analysis of randomized controlled trials. Curr. Med. Res. Opin. 2016, 32, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Song, J.K.; Lee, K.; Park, H.Y.; Hyon, J.Y.; Oh, S.W.; Bae, W.K.; Han, J.S.; Jung, S.Y.; Um, Y.J.; Lee, G.H.; et al. Efficacy of Carboxymethylcellulose and Hyaluronate in Dry Eye Disease: A Systematic Review and Meta-Analysis. Korean J. Fam. Med. 2017, 38, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook/current (accessed on 5 May 2020).
- Robert, P.Y.; Cochener, B.; Amrane, M.; Ismail, D.; Garrigue, J.S.; Pisella, P.J.; Baudouin, C. Efficacy and safety of a cationic emulsion in the treatment of moderate to severe dry eye disease: A randomized controlled study. Eur. J. Ophthalmol. 2016, 26, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Lopez-de la Rosa, A.; Pinto-Fraga, J.; Blazquez Arauzo, F.; Urbano Rodriguez, R.; Gonzalez-Garcia, M.J. Safety and Efficacy of an Artificial Tear Containing 0.3% Hyaluronic Acid in the Management of Moderate-to-Severe Dry Eye Disease. Eye Contact Lens 2017, 43, 383–388. [Google Scholar] [CrossRef]
- Essa, L.; Laughton, D.; Wolffsohn, J.S. Can the optimum artificial tear treatment for dry eye disease be predicted from presenting signs and symptoms? Contact Lens Anterior Eye 2018, 41, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Gross, D.; Childs, M.; Piaton, J.M. Comparative study of 0.1% hyaluronic acid versus 0.5% carboxymethylcellulose in patients with dry eye associated with moderate keratitis or keratoconjunctivitis. Clin. Ophthalmol. 2018, 12, 1081–1088. [Google Scholar] [CrossRef] [Green Version]
- Baudouin, C.; Cochener, B.; Pisella, P.J.; Girard, B.; Pouliquen, P.; Cooper, H.; Creuzot-Garcher, C. Randomized, phase III study comparing osmoprotective carboxymethylcellulose with sodium hyaluronate in dry eye disease. Eur. J. Ophthalmol. 2012, 22, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Brignole, F.; Pisella, P.J.; Dupas, B.; Baeyens, V.; Baudouin, C. Efficacy and safety of 0.18% sodium hyaluronate in patients with moderate dry eye syndrome and superficial keratitis. Graefe’s Arch. Clin. Exp. Ophthalmol. 2005, 243, 531–538. [Google Scholar] [CrossRef]
- Condon, P.I.; McEwen, C.G.; Wright, M.; Mackintosh, G.; Prescott, R.J.; McDonald, C. Double blind, randomised, placebo controlled, crossover, multicentre study to determine the efficacy of a 0.1% (w/v) sodium hyaluronate solution (Fermavisc) in the treatment of dry eye syndrome. Br. J. Ophthalmol. 1999, 83, 1121–1124. [Google Scholar] [CrossRef] [Green Version]
- Laflamme, M.Y.; Swieca, R. A comparative study of two preservative-free tear substitutes in the management of severe dry eye. Can. J. Ophthalmol. 1988, 23, 174–176. [Google Scholar]
- Lee, J.H.; Ahn, H.S.; Kim, E.K.; Kim, T.I. Efficacy of sodium hyaluronate and carboxymethylcellulose in treating mild to moderate dry eye disease. Cornea 2011, 30, 175–179. [Google Scholar] [CrossRef]
- NCT. Study to Compare the Efficacy and Safety of Two Non-Preserved Artificial Tears for the Treatment of Dry Eye Signs and Symptoms. 2009. Available online: https://clinicaltrials.gov/show/NCT00938704 (accessed on 11 September 2020).
- Nelson, J.D.; Farris, R.L. Sodium hyaluronate and polyvinyl alcohol artificial tear preparations. A comparison in patients with keratoconjunctivitis sicca. Arch. Ophthalmol. 1988, 106, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef] [PubMed]
- Cho, P.; Yap, M. Schirmer test. I. A review. Optom. Vis. Sci. 1993, 70, 152–156. [Google Scholar] [CrossRef]
- Benelli, U.; Nardi, M.; Posarelli, C.; Albert, T.G. Tear osmolarity measurement using the TearLab™ Osmolarity System in the assessment of dry eye treatment effectiveness. Contact Lens Anterior Eye 2010, 33, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Iester, M.; Orsoni, G.J.; Gamba, G.; Taffara, M.; Mangiafico, P.; Giuffrida, S.; Rolando, M. Improvement of the ocular surface using hypotonic 0.4% hyaluronic acid drops in keratoconjunctivitis sicca. Eye (Lond.) 2000, 14, 892–898. [Google Scholar] [CrossRef] [Green Version]
- Methodologies to diagnose and monitor dry eye disease: Report of the Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 108–152. [CrossRef]
- Sullivan, B.D.; Whitmer, D.; Nichols, K.K.; Tomlinson, A.; Foulks, G.N.; Geerling, G.; Pepose, J.S.; Kosheleff, V.; Porreco, A.; Lemp, M.A. An objective approach to dry eye disease severity. Investig. Ophthalmol. Vis. Sci. 2010, 51, 6125–6130. [Google Scholar] [CrossRef] [Green Version]
- Nichols, K.K. Patient-reported symptoms in dry dye disease. Ocul. Surf. 2006, 4, 137–145. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Location | Publication Type | Study Design | Masking | Patients | Follow Up Duration (Days) | Sample Size (N) | Mean Age (Years) | Sex Ratio (M:W) | HA Conc. (%) | Type of Non-HA Eye Drops | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HA | Non-HA | |||||||||||
| Groβ [28] | France | Journal article | RCT (Parallel) | Single | Dry eye disease (Moderate) | 84 | 41 | 39 | 55.8 | 24:56 | 0.1 | 0.5% CMC |
| Essa [27] | United Kingdom | Journal article | RCT (Crossover) | Single | Dry eye disease | 28 | 50 | 50 | 60.8 | 35:15 | 0.15, 0.4 | Pospholipid liposome |
| 0.25% CMC | ||||||||||||
| Pinto-Fraga [11] | Spain | Journal article | RCT (Crossover) | Double | Dry eye patients (Mild) | 30 | 16 | 16 | 58.0 | 8:8 | 0.2 | 0.9% Saline |
| Lopez-de la Rosa [26] | Spain | Journal article | RCT (Crossover) | Double | Dry eye disease (Moderate to severe) | 30 | 16 | 16 | 57.5 | 4:12 | 0.3 | 0.9% Saline |
| Lambiase [19] | Italia | Journal article | RCT (Parallel) | Double | Dry eye patients | 14 | 20 | 15 | 56.9 | 3:36 | 0.18 | Lubricin |
| Robert [25] | France | Journal article | RCT (Parallel) | Single (Investigator) | Dry eye patients (Moderate to severe) | 90 | 41 | 44 | 62.6 | 16:69 | 0.18 | Hypotonic CE |
| Kinoshita [20] | Japan | Journal article | RCT (Parallel) | Quadruple | Dry eye patients | 28 | 95 | 93 | 55.6 | 25:163 | 0.1 | 2% Rebamipide |
| Baudouin [29] | France | Journal article | RCT (Parallel) | Single (Investigator) | Dry eye patients | 35 | 29 | 37 | 56.8 | 8:69 | 0.18 | 0.5% CMC |
| Baeyens [12] | France | Journal article | RCT (Parallel) | Double | Dry eye patients (Moderate) | 84 | 100 | 96 | 59.3 | 41:245 | 0.18 | Saline |
| 91 | 0.3% Carbomer | |||||||||||
| Lee [33] | Korea | Journal article | RCT (Parallel) | Single (Observer) | Dry eye patients (Mild to moderate) | 56 | 32 | 33 | 38 | 6:59 | 0.1 | 0.5% CMC |
| Sanchez [16] | Spain | Journal article | RCT (Parallel) | Single (Observer) | Dry eye syndrome or Sjogren’s syndrome | 30 | 15 * | 14 * | 71.8 | All female | 0.15 | 0.5% Carmellose |
| NCT00938704 [34] | German | Clinical trial | RCT (Parallel) | Double | Dry eye patients | 14 | 37 | 33 | 51.5 † | 19:51 | 0.18 | 0.5% CMC |
| Rolando [18] | Italia | Journal article | RCT (Parallel) | Open label | Dry eye syndrome | 90 | 9 | 11 | 60.3 | 10:20 | 0.2 | 0.5% TSP |
| 10 | 1% TSP | |||||||||||
| Brignole [30] | France | Journal article | RCT (Parallel) | Single (Observer) | Dry eye syndrome (Moderate) | 56 | 10 | 11 | 63 | 1:20 | 0.18 | 1% CMC |
| Condon [31] | United Kingdom | Journal article | RCT (Crossover) | Double | Dry eye syndrome (Severe) | 28 | 34 | 36 | 61 | 12:58 | 0.1 | 0.9% Saline |
| Nelson [35] | United States of America | Journal article | RCT (Parallel) | Double | Dry eye syndrome (Moderately severe) | 56 | 20 | 15 | 58.55 | 4:31 | 0.1 | 1.4% PVA |
| Laflamme [32] | Canada | Journal article | RCT (Crossover) | No comment | Dry eye patients (Severe) | 56 | 12 | 12 | 58 | Not reported | 0.1 | 1.4% PVA |
| First Author | Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias |
|---|---|---|---|---|---|---|---|
| Groβ [28] | ? | ? | ● | ? | ● | ● | ● |
| Essa [27] | ? | ? | ● | ● | ● | ● | ● |
| Pinto-Fraga [11] | ? | ? | ● | ● | ● | ● | ● |
| Lopez-de la Rosa [26] | ? | ? | ● | ● | ● | ● | ● |
| Lambiase [19] | ● | ? | ● | ● | ● | ● | ● |
| Robert [25] | ● | ● | ● | ● | ● | ● | ● |
| Kinoshita [20] | ● | ● | ○ | ● | ● | ● | ● |
| Baudouin [29] | ● | ? | ○ | ● | ● | ● | ● |
| Baeyens [12] | ? | ? | ● | ● | ● | ● | ● |
| Lee [33] | ? | ? | ○ | ● | ● | ● | ● |
| Sanchez [16] | ● | ? | ○ | ● | ● | ● | ? |
| NCT00938704 [34] | ? | ? | ● | ● | ● | ● | ● |
| Rolando [18] | ? | ? | ○ | ○ | ● | ● | ● |
| Brignole [30] | ● | ? | ○ | ● | ● | ● | ● |
| Condon [31] | ● | ● | ● | ● | ● | ● | ● |
| Nelson [35] | ? | ? | ● | ● | ● | ● | ? |
| Laflamme [32] | ? | ? | ? | ? | ● | ● | ● |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.-J.; Lee, W.-Y.; Kim, Y.-j.; Hong, Y.-p. A Meta-Analysis of the Efficacy of Hyaluronic Acid Eye Drops for the Treatment of Dry Eye Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 2383. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052383
Yang Y-J, Lee W-Y, Kim Y-j, Hong Y-p. A Meta-Analysis of the Efficacy of Hyaluronic Acid Eye Drops for the Treatment of Dry Eye Syndrome. International Journal of Environmental Research and Public Health. 2021; 18(5):2383. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052383
Chicago/Turabian StyleYang, Yun-Jung, Won-Young Lee, Young-jin Kim, and Yeon-pyo Hong. 2021. "A Meta-Analysis of the Efficacy of Hyaluronic Acid Eye Drops for the Treatment of Dry Eye Syndrome" International Journal of Environmental Research and Public Health 18, no. 5: 2383. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052383