1. Introduction
Lead exposure is a serious health risk for children because of its adverse effects such as damage to the brain and nervous system, slowed growth and development, or learning and behavior problems [
1,
2,
3,
4,
5,
6]. These adverse effects of lead exposure at early ages can bring long-term consequences later in life such as encounters with the juvenile justice system, antisocial behaviors, or impacts on socioeconomic status [
7,
8,
9,
10]. The US has a long history of policies and efforts addressing lead poisoning dating back to 1971’s Lead-Based Paint Poisoning Prevention Act and 1978’s residential lead-based paint ban as the country saw a sharp increase in children’s blood lead levels caused by the widespread lead contamination in the early 1970s [
11]. In 1992, Congress passed the Residential Lead-Based Paint Hazard Reduction Act of 1992, also known as Title X of the Housing and Community Development Act. This law directed US Department of Housing and Urban Development and US Environmental Protection Agency to require the disclose of known information on lead-based paint and lead-based paint hazards before the sale or lease of most housing built before 1978 [
12]. By 2009, the Surgeon General of the US Public Health Service issued
“The Surgeon General’s Call to Action to Promote Healthy Homes” to provide an overview of issues contributing to the nation’s unhealthy housing situation and to draw attention to the public health impact of housing hazards [
13]. Decades of these efforts are considered a major public success as it resulted in a 93.6% decline in geometric mean blood lead level of the US population from 12.8 to 0.92 µg/dL between 1976 and 1980 to 2015 and 2016 [
12]. Contrary to a contemporary misconception that lead exposure is no longer a problem, the Centers for Disease Control and Prevention estimates that approximately 530,000 US children aged 1–5 years or 2.6% of children in this age group had ≥5 µg/dL from the periods 1999–2002 to 2007–2010 [
14]. Despite these improvements, previous research stresses that there is no safe blood lead level in children and even very low level of lead exposure can cause health impairment [
1,
2,
3,
4,
10].
Children get exposed to lead from multiple sources including air, bare soil, food, drinking water, and/or consumer goods. However, the primary source of lead exposure in children is deteriorating lead-based paint found in older homes and buildings as well as contaminated dust and soil, which accounts for up to 70% of elevated blood lead levels in children in the US [
15]. The Centers for Disease Control and Prevention states that lead poisoning is 100% preventable and identifies four strategies to address this public health concern: (1) getting a blood lead test of your child, (2) testing paint and dust in your home for lead, (3) renovating your home, and (4) removing lead-containing products from your households [
16]. However, lead-based paint hazards remain to be a critical environmental hazard in many homes of children across the United States. The results of the American Healthy Homes Survey, conducted between June 2005 and March 2006, estimated that over 23 million homes or 22% of the nation’s housing still had significant lead-based paint hazards. It was also reported that 3.6 million of the homes belonged to households with one or more children younger than six years of age [
17]. This number could have been lowered with recent lead poisoning prevention efforts, but as of 2010, homes of 530,000 children with elevated blood levels could potentially have lead-based paint hazards in them [
14]. Additionally, the risk of lead exposure is not evenly distributed across the US population, with greater risks for communities of color and residents in urban and low-income areas where older, lead-contaminated homes are located. Studies reported consistent and significant racial disparity in lead exposure across the nation with higher blood lead levels for non-Hispanic Black children compared to non-Hispanic whites even after correcting for other housing or socioeconomic risk factors [
14,
18,
19,
20,
21]. Therefore, additional strategies need to be deployed to remedy these racial disparities in lead exposure.
Federal, state, and local lead policies to date have been mostly passive and reactive, concentrating its efforts on mitigation or remediation of lead exposure after-the-fact using children’s elevated blood lead level as an indicator to act upon. In addition, persistence of inequities in lead exposure to this date reveals the limitations of lead policies in lacking their focus on health equity [
14,
18,
22]. Future approaches to lead exposure interventions need to be proactive and prevention-oriented and should be multidisciplinary and well-coordinated among multiple parties involved. Most importantly, these new approaches must focus on eliminating health inequities related to lead [
18,
22].
The first critical step in establishing effective approaches to lead exposure prevention for children is to accurately identify target intervention areas. This allows public health practitioners to better pinpoint their efforts by locating neighborhoods where higher level of lead hazard is suspected and also more children of younger ages spend most of their time. In this study, we present a methodology for the measurement of child-focused lead-based paint hazard using geospatial analyses that will facilitate effective targeting of lead hazard areas at neighborhood level. This entails examining concentration of children aged 0–5 and conditions of two major built environments where younger children live, learn, and play—homes and childcare settings [
19].
Incorporating community-level data for effective identification and mitigation of health risks around one’s neighborhood is important [
23]. One’s health is largely determined by social determinants of health, defined as “the circumstances in which people live, work and grow; largely shaped by the distribution of resources and power” [
24]. The distribution of such resources is uneven across different neighborhoods, resulting in the concentration of disadvantage in certain areas and health disparity that is very much place-based. With the use of community-based data on neighborhood housing, childcare centers, and distribution of children by race and ethnicity, this study exemplifies the merits of a place-based approach and the use of Geographic Information System in healthcare and health intervention [
23,
25,
26]. The lead paint hazard calculated at census block group in this study will help better facilitate lead poisoning prevention efforts by identifying areas where more buildings require renovation, and more children require blood lead tests. This will also promote cross-sector collaboration among multiple parties from public health, local housing, and pediatric clinicians. More importantly, analyses of distribution of children of different race and ethnicity in relation to lead paint hazard will address racial health disparity in lead exposure and specifically identify areas to target interventions to address those disparities.
4. Conclusions
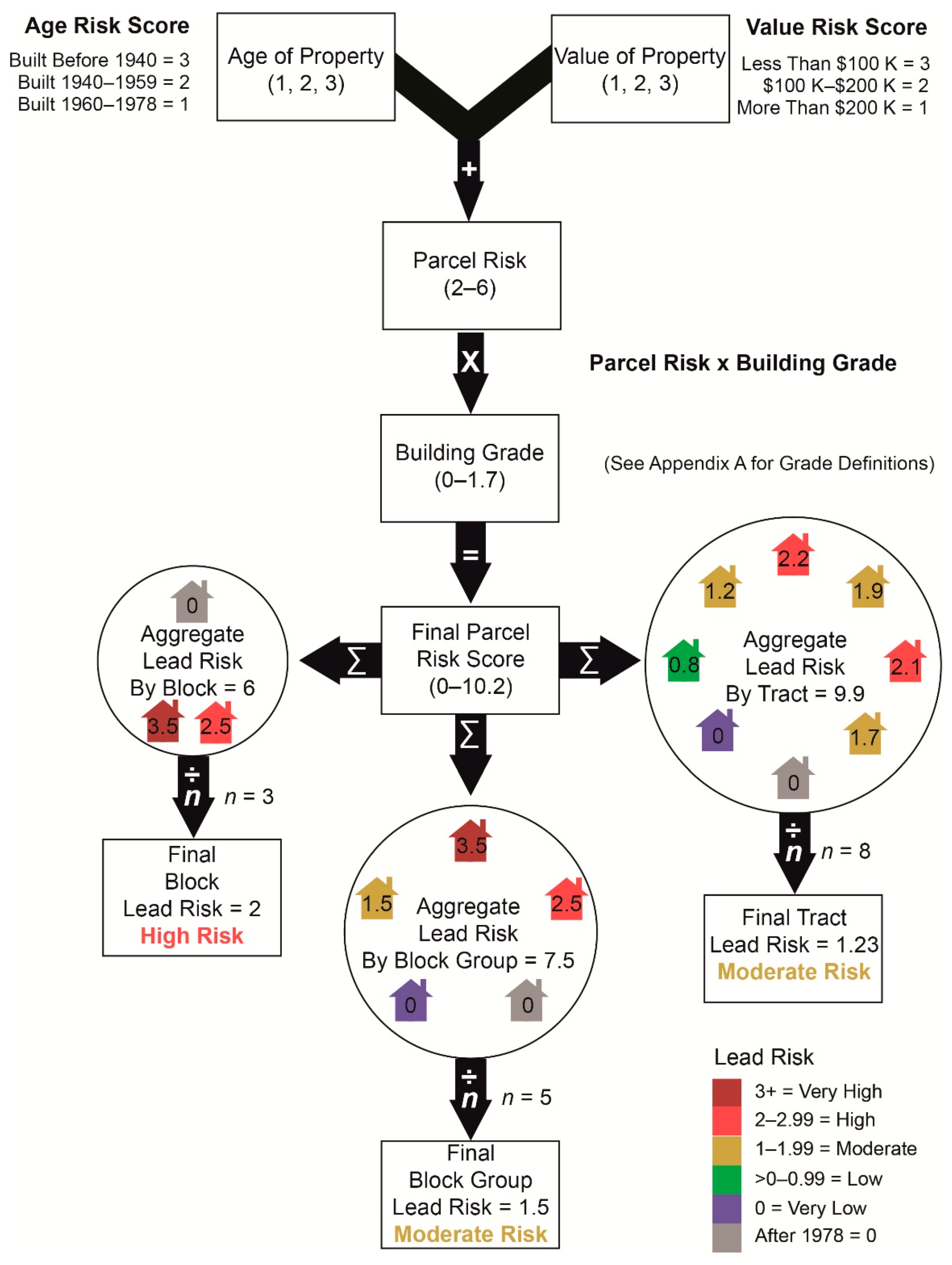
The quality of environment where children grow up makes critical and long-lasting imprints on the quality of their lives in various aspects including their physical and emotional health, intellectual development and academic accomplishment, and economic and social wellbeing. Among various sources of health risks found in environments for children, this study focuses on lead paint hazard which poses severe health risks for children. Noting the primary source of lead hazards is lead-based paints used in buildings constructed prior to 1978, this study answers an important call for child-friendly planning to improve public health by influencing the environment where children live and play. Using parcel-level data of all residential units in Franklin County Ohio, this study measures lead risk at neighborhood level by accounting for age, value, and quality of properties.
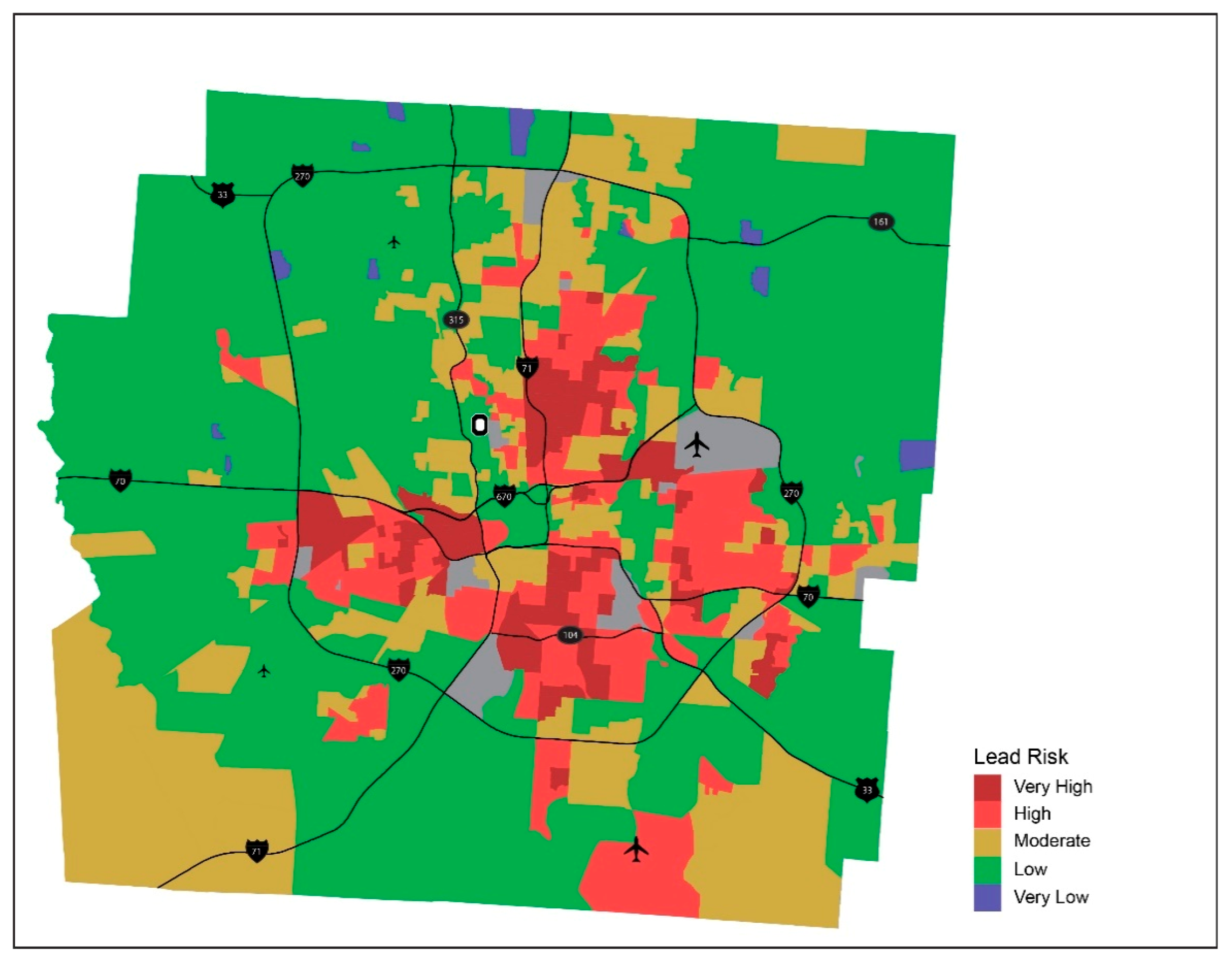
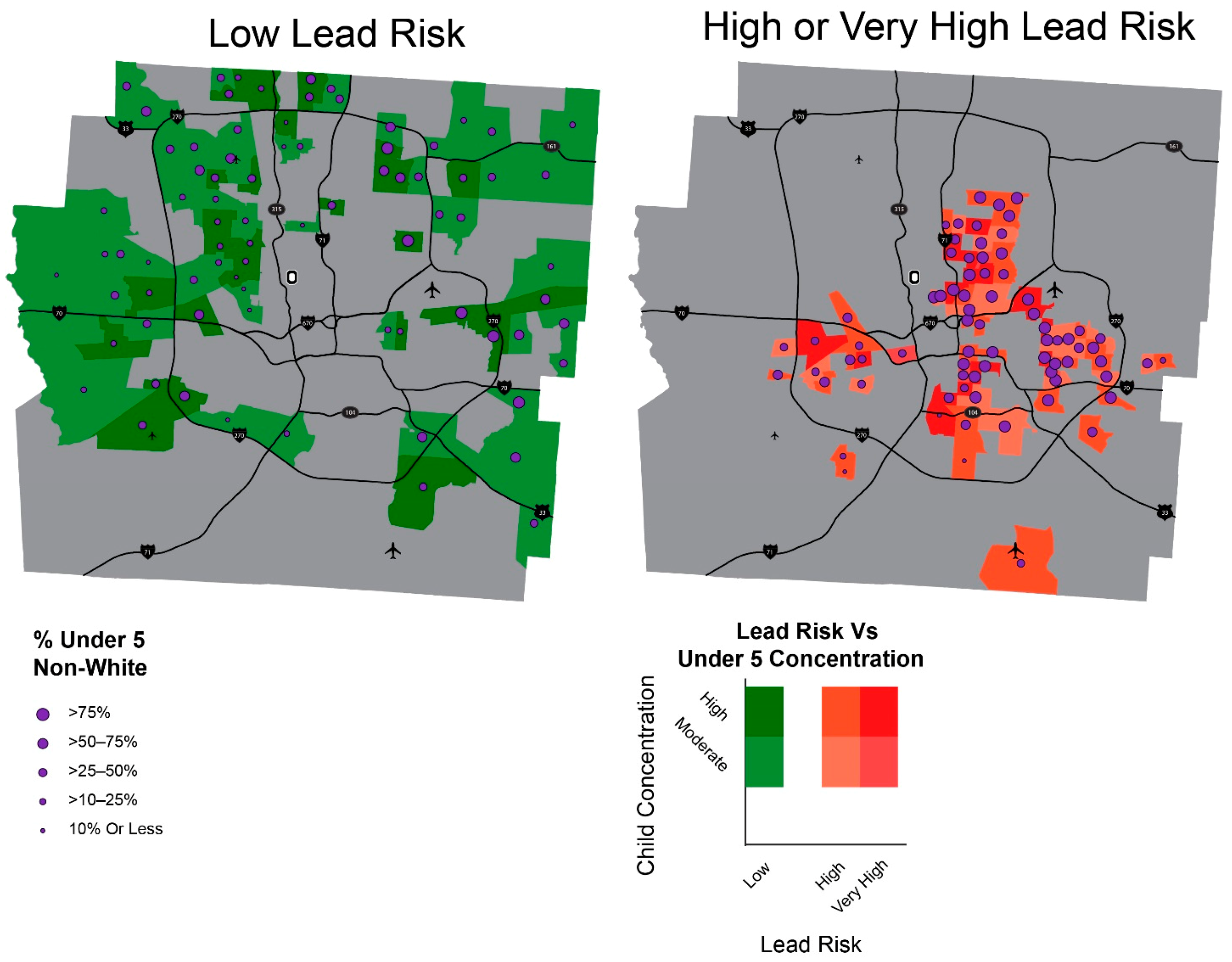
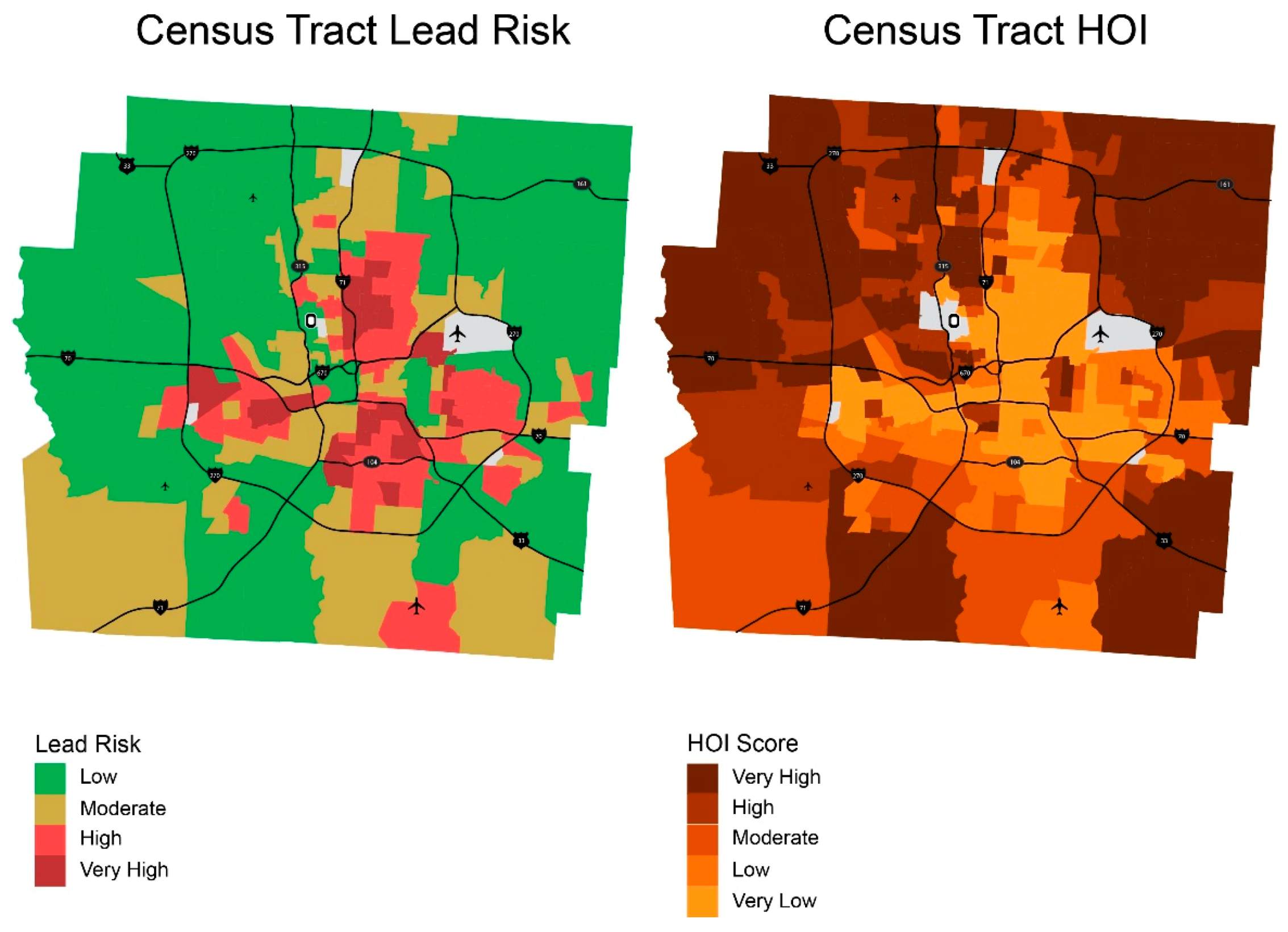
The result of the measurement and visualization of it shows a potential for assisting more targeted and proactive intervention to prevent lead poisoning in the county by identifying target areas at neighborhood level (census block or census block group). A cross-examination of areas with different lead risk and concentration of children revealed that more than a quarter of children under 5 in the county reside in areas with high or very high lead risk, which is close to 25,000 children. This analysis also suggests cross-sector collaboration among parties in healthcare and housing for multidimensional and comprehensive lead hazard intervention efforts through blood lead testing and home remediation.
Further analysis found racial disparity in lead risk in the county with 45% of Black children under 5 live in higher lead risk neighborhoods, compared to 18% of white children. This suggests an urgent need to address racial disparity in lead risk in order to improve public health in the county. To make our community healthier for our children, we need to ensure that the environment is healthy for all children, regardless of their racial or socioeconomic backgrounds because an environment that is unhealthy for some children is unhealthy for all children and adults in the entire community.
Lastly, it is also important to note that the methodology for estimating lead risk presented in this study is replicable and expandable to other parts of the country if parcel level data (age, value, and quality of residential parcels) are available. The year in which homes are built and the property value are often made public by county or state housing agencies. Additionally, the building quality grade categories used by Franklin County (see
Table A1 in
Appendix A), which ultimately was used in this study, are one of the standards commonly used across the country. Provided that this data can be obtained, lead risk can be estimated at the parcel level, which can subsequently be aggregated to neighborhood level such as census block or tract. This methodology therefore has great potential for improving targeted and proactive lead poisoning prevention efforts for children beyond the county level such as metropolitan area, state, or even at the national level.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}











