Positive Externalities of Climate Change Mitigation and Adaptation for Human Health: A Review and Conceptual Framework for Public Health Research



Abstract
:1. Introduction
2. Climate Change Burden to Public Health
2.1. Climate Change and Global Health
2.2. Climate Change and Global Injustice: Examples from Africa
3. Climate Change Mitigation and Adaptation Strategies
3.1. Climate Change Mitigation Strategies
3.2. Climate Change Adaptation Strategies
3.3. Dual Purpose Strategies (Mitigation and Adaptation)
4. Positive Externalities of Mitigation and Adaptation: A Strategic Conceptual Framework
4.1. Methods
4.2. The New Conceptual Framework
4.3. The Links between Public Health and Other Sectors in the New Conceptual Framework
4.3.1. Urban Development and Green Infrastructure
4.3.2. Housing, Transportation and Agriculture
4.3.3. Health Outcomes, Health Systems and Health Care Expenditures
5. Final Recommendations for Stakeholders
- Health should be incorporated into all policy creation and implementation with public health scientists and health care professionals engaged at each stage of policy development. “Health in all policies” or “health outcomes in all interventions” should be considered a gold standard moving forward.
- Government leaders should prioritize climate action within their cities, states, nations, and across borders focused on environmental justice and advancing the health of vulnerable populations.
- Climate education should be incorporated into schools and graduate studies to ensure a basic foundation of science across sectors and critical thinking skills are built. Application of the topic is encouraged for those interested in dual degrees in health professional studies.
- Research funding should incentivize climate smart initiatives, including green and climate resilient infrastructure, climate resilient agriculture and food systems, climate resilient transportation systems, climate resilient healthcare systems, and healthy environments in low, middle, and high-income settings with emphasis on developing tools, technologies, and models that accurately categorize risk and quantify health impacts from EWE.
- Rapid identification and implementation of solutions that reduce GHGE on a global scale and adapt and build resilient communities locally should guide those in positions of leadership and power.
- Collaboration across multiple sectors under this new framework should alleviate any duplication of efforts and ensure efficiency as we strive for an evidence-based and impact driven decision-making process to reduce health disparities and promote intergenerational equity.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
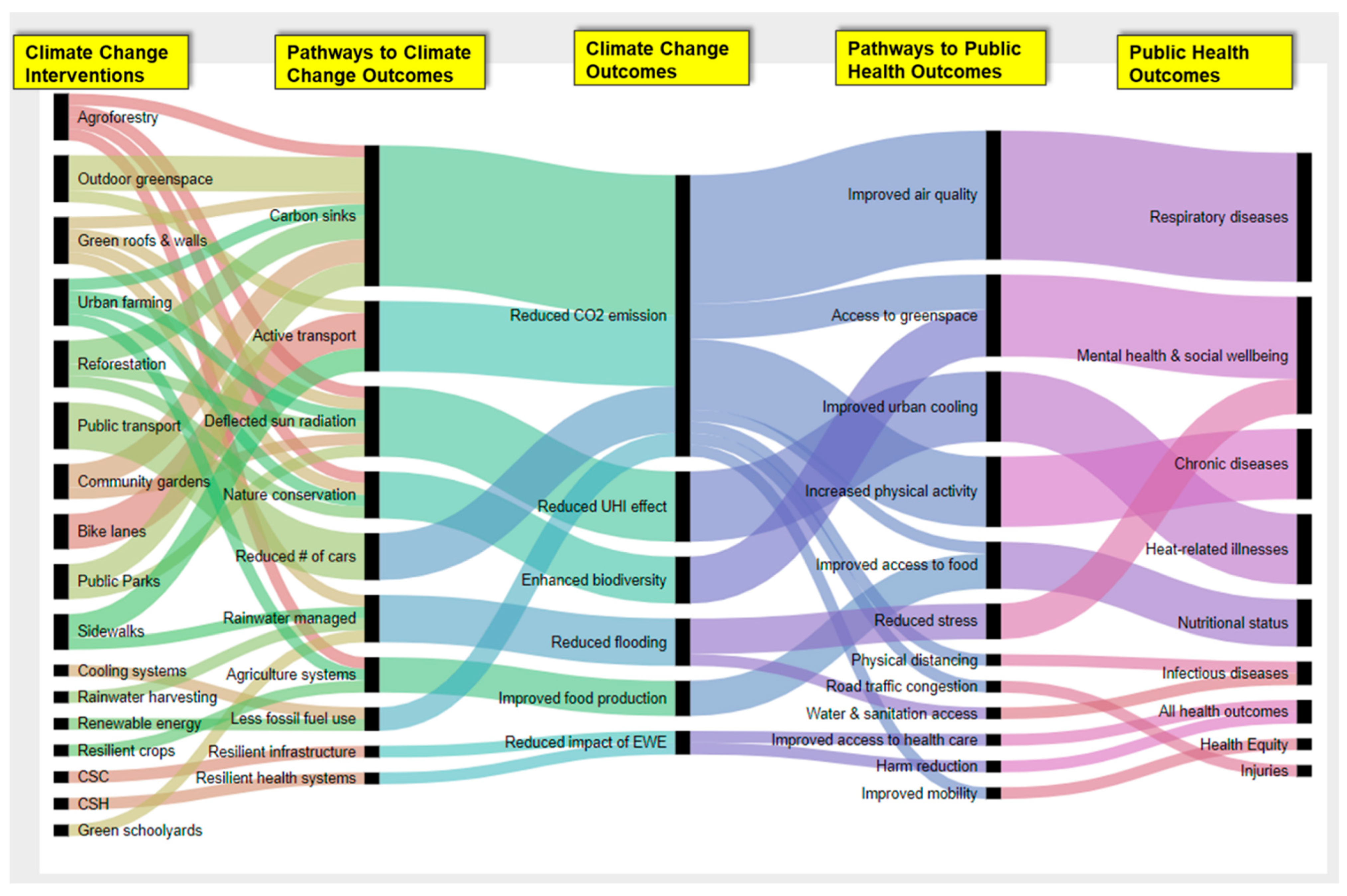
| Mitigation or Adaptation Strategies | Pathways to Anticipated Climate Change Outcomes | Climate Change Outcome | Pathways to Positive Health Outcomes | Improved Health Outcome in any of the Domains Presented Here |
|---|---|---|---|---|
| Public transport | Reduced # of cars | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Public transport | Reduced # of cars | Reduced CO2 emission | Road traffic congestion | Injuries |
| Public transport | Reduced # of cars | Reduced CO2 emission | Increased physical activity | Chronic diseases |
| Public transport | Reduced # of cars | Reduced CO2 emission | Improved mobility | Health Equity |
| Reforestation | Carbon sinks | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Reforestation | Carbon sinks | Reduced CO2 emission | Access to greenspace | Mental health & social wellbeing |
| Reforestation | Nature conservation | Enhanced biodiversity | Access to greenspace | Mental health & social wellbeing |
| Reforestation | Deflected sun radiation | Reduced UHI effect | Improved urban cooling | Heat-related illnesses |
| Public Parks | Carbon sinks | Reduced CO2 emission | Access to greenspace | Mental health & social wellbeing |
| Public Parks | Carbon sinks | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Public Parks | Deflected sun radiation | Reduced UHI effect | Improved urban cooling | Heat-related illnesses |
| Sidewalks | Rainwater managed | Reduced flooding | Reduced stress | Mental health & social wellbeing |
| Sidewalks | Active transport | Reduced CO2 emission | Increased physical activity | Chronic diseases |
| Sidewalks | Active transport | Reduced CO2 emission | Increased physical activity | Chronic diseases |
| Community gardens | Carbon sinks | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Community gardens | Carbon sinks | Reduced CO2 emission | Improved access to food | Nutritional status |
| Community gardens | Deflected sun radiation | Reduced UHI effect | Improved urban cooling | Heat-related illnesses |
| Bike lanes | Active transport | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Bike lanes | Active transport | Reduced CO2 emission | Increased physical activity | Chronic diseases |
| Bike lanes | Active transport | Reduced CO2 emission | Increased physical activity | Chronic diseases |
| Green schoolyards | Rainwater managed | Reduced flooding | Reduced stress | Mental health & social wellbeing |
| Resilient crops | Agriculture systems | Improved food production | Improved access to food | Nutritional status |
| Agroforestry | Agriculture systems | Improved food production | Improved access to food | Nutritional status |
| Agroforestry | Carbon sinks | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Agroforestry | Deflected sun radiation | Reduced UHI effect | Improved urban cooling | Heat-related illnesses |
| Agroforestry | Nature conservation | Enhanced biodiversity | Access to greenspace | Mental health & social wellbeing |
| Urban farming | Agriculture systems | Improved food production | Improved access to food | Nutritional status |
| Urban farming | Nature conservation | Enhanced biodiversity | Access to greenspace | Mental health & social wellbeing |
| Urban farming | Deflected sun radiation | Reduced UHI effect | Improved urban cooling | Heat-related illnesses |
| Urban farming | Carbon sinks | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Green roofs & walls | Deflected sun radiation | Reduced UHI effect | Improved urban cooling | Heat-related illnesses |
| Green roofs & walls | Rainwater managed | Reduced flooding | Reduced stress | Mental health & social wellbeing |
| Green roofs & walls | Carbon sinks | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Green roofs & walls | Nature conservation | Enhanced biodiversity | Access to greenspace | Mental health & social wellbeing |
| Rainwater harvesting | Rainwater managed | Reduced flooding | Water & sanitation access | Infectious diseases |
| Renewable energy | Less fossil fuel use | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Cooling systems | Less fossil fuel use | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Outdoor greenspace | Carbon sinks | Reduced CO2 emission | Physical distancing | Infectious diseases |
| Outdoor greenspace | Carbon sinks | Reduced CO2 emission | Improved air quality | Respiratory diseases |
| Outdoor greenspace | Carbon sinks | Reduced CO2 emission | Access to greenspace | Mental health & social wellbeing |
| Outdoor greenspace | Active transport | Reduced CO2 emission | Increased physical activity | Chronic diseases |
| CSH | Resilient health systems | Reduced impact of EWE | Improved access to health care | All health outcomes |
| CSC | Resilient infrastructure | Reduced impact of EWE | Harm reduction | All health outcomes |
References
- Landrigan, P.; Fuller, R.; Haines, A.; Watts, N.; McCarthy, G. Pollution prevention and climate change mitigation: Measuring the health benefits of comprehensive interventions. Lancet Planet. Heal. 2018, 2, e515–e516. [Google Scholar] [CrossRef] [Green Version]
- Council, N.R. America’s Climate Choices; National Academies Press: Washington, DC, USA, 2011; ISBN 0309305535. [Google Scholar]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef] [Green Version]
- Haines, A.; Kovats, R.S.; Campbell-Lendrum, D.; Corvalan, C. Climate change and human health: Impacts, vulnerability, and mitigation. Lancet 2006, 367, 2101–2109. [Google Scholar] [CrossRef]
- OECD Emissions, Reducing Transport Greenhouse Gas: Trends & Data 2010. In Proceedings of the International Transport Forum, Organisation for Economic Cooperation and Development, Leipzig, Germany, 26–28 May 2010; Available online: http://www.indiaenvironmentportal.org.in/files/10GHGTrends.pdf (accessed on 2 March 2021).
- Kwan, S.C.; Hashim, J.H. A review on co-benefits of mass public transportation in climate change mitigation. Sustain. Cities Soc. 2016, 22, 11–18. [Google Scholar] [CrossRef]
- Assad, S.W. The rise of consumerism in Saudi Arabian society. Int. J. Commer. Manag. 2007, 17, 73–104. [Google Scholar] [CrossRef]
- The Holy Father Pope Francis Encyclical Letter Laudato Si’ of the Holy Father Francis on Care for Our Common Home. Available online: http://www.vatican.va/content/francesco/en/encyclicals/documents/papa-francesco_20150524_enciclica-laudato-si.html (accessed on 19 December 2020).
- Mayell, H. As consumerism spreads, Earth suffers, study says: National Geographic News. 2004. Available online: http://www.mercymidatlantic.org/PDF/NatGeo_As_Consumerism_Spreads_01122004.pdf (accessed on 2 March 2021).
- Parikh, J.; Shukla, V. Urbanization, energy use and greenhouse effects in economic development: Results from a cross-national study of developing countries. Glob. Environ. Chang. 1995, 5, 87–103. [Google Scholar] [CrossRef]
- Ala-Mantila, S.; Heinonen, J.; Junnila, S. Relationship between urbanization, direct and indirect greenhouse gas emissions, and expenditures: A multivariate analysis. Ecol. Econ. 2014, 104, 129–139. [Google Scholar] [CrossRef]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Kjellstrom, T.; Weaver, H.J. Climate change and health: Impacts, vulnerability, adaptation and mitigation. N. S. W. Public Health Bull. 2009, 20, 5–9. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.; Dilkina, B.; Moreno-Cruz, J. Modeling migration patterns in the USA under sea level rise. PLoS ONE 2020, 15, e0227436. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Cardona, O.-D.; van Aalst, M.K.; Birkmann, J.; Fordham, M.; McGregor, G.; Perez, R.; Pulwarty, R.S.; Lisa Schipper, E.F.; Tan Sinh, B.; Décamps, H.; et al. Determinants of Risk: Exposure and Vulnerabilit: Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation 2 Determinants of Risk: Exposure and Vulnerability; Intergovernmental Panel on Climate Change: Melbourne, Australia, 2012. [Google Scholar]
- Thomas, K.; Hardy, R.D.; Lazrus, H.; Mendez, M.; Orlove, B.; Rivera-Collazo, I.; Roberts, J.T.; Rockman, M.; Warner, B.P.; Winthrop, R. Explaining differential vulnerability to climate change: A social science review. Wiley Interdiscip. Rev. Clim. Chang. 2019, 10, e565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMichael, A.J. Globalization, Climate Change, and Human Health. N. Engl. J. Med. 2013, 368, 1335–1343. [Google Scholar] [CrossRef] [Green Version]
- The United Nations Framework Convention on Climate Change the Paris Agreement | UNFCCC. Available online: https://unfccc.int/process-and-meetings/the-paris-agreement/the-paris-agreement (accessed on 31 May 2020).
- UN What is the Paris Agreement? | UNFCCC. Available online: https://unfccc.int/process-and-meetings/the-paris-agreement/what-is-the-paris-agreement (accessed on 2 January 2020).
- Bustamante, M.M.C.; Silva, J.S.; Scariot, A.; Sampaio, A.B.; Mascia, D.L.; Garcia, E.; Sano, E.; Fernandes, G.W.; Durigan, G.; Roitman, I.; et al. Ecological restoration as a strategy for mitigating and adapting to climate change: Lessons and challenges from Brazil. Mitig. Adapt. Strateg. Glob. Chang. 2019, 24, 1249–1270. [Google Scholar] [CrossRef]
- Ramesh, R.; Banerjee, K.; Paneerselvam, A.; Raghuraman, R.; Purvaja, R.; Lakshmi, A. Importance of Seagrass Management for Effective Mitigation of Climate Change; Elsevier Inc.: Amsterdan, The Netherlands, 2019; ISBN 9780128104736. [Google Scholar]
- Organisation for Economic Cooperation and Development: Handbook on the OECD-DAC Climate Markers. Available online: http://www.oecd.org/dac/stats/48785310.pdf. (accessed on 2 January 2020).
- World Health Organization (WHO) WHO Guidance for Climate Resilient and Environmentally Sustainable Health Care Facilities. Available online: https://www.who.int/publications/i/item/climate-resilient-and-environmentally-sustainable-health-care-facilities (accessed on 25 January 2021).
- Lempert, R.J.; Arnold, J.R.; Pulwarty, R.S.; Gordon, K.; Greig, K.; Hawkins-Hoffman, C.; Sands, D.; Werrell, C. Chapter 28: Adaptation Response. Impacts, Risks, and Adaptation in the United States: The Fourth National Climate Assessment, Volume II; Intergovermental Panel on Climate Change: Washington, DC, USA, 2018. [Google Scholar]
- Deb, A.; Kanungo, S.; Deb, M.; Nair, G. Impact of climate change on health and strategies for mitigation and adaptation. WHO South-East Asia J. Public Heal. 2012, 1, 8. [Google Scholar] [CrossRef] [PubMed]
- Harlan, S.L.; Ruddell, D.M. Climate change and health in cities: Impacts of heat and air pollution and potential co-benefits from mitigation and adaptation. Curr. Opin. Environ. Sustain. 2011, 3, 126–134. [Google Scholar] [CrossRef]
- Kim, E.J. The impacts of climate change on human health in the United States: A scientific assessment, by us global change research program. J. Am. Plan. Assoc. 2016, 82, 418–419. [Google Scholar] [CrossRef]
- The Center for Disease Control and Prevention Climate Change and Public Health—Climate Effects on Health. Available online: https://www.cdc.gov/climateandhealth/effects/default.htm (accessed on 24 January 2021).
- Hauer, M.E.; Evans, J.M.; Mishra, D.R. Millions projected to be at risk from sea-level rise in the continental United States. Nat. Clim. Chang. 2016, 6, 691–695. [Google Scholar] [CrossRef]
- Prüss-Ustün, A.; van Deventer, E.; Mudu, P.; Campbell-Lendrum, D.; Vickers, C.; Ivanov, I.; Forastiere, F.; Gumy, S.; Dora, C.; Adair-Rohani, H. Environmental risks and non-communicable diseases. Bmj 2019, 364, 1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjellstrom, T.; Butler, A.J.; Lucas, R.M.; Bonita, R. Public health impact of global heating due to climate change: Potential effects on chronic non-communicable diseases. Int. J. Public Health 2010, 55, 97–103. [Google Scholar] [CrossRef]
- Shuman, E.K. Global climate change and infectious diseases. N. Engl. J. Med. 2010, 362, 1061–1063. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Lu, Y.; Zhou, S.; Chen, L.; Xu, B. Impact of climate change on human infectious diseases: Empirical evidence and human adaptation. Environ. Int. 2016, 86, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Liang, L.; Gong, P. Climate change and human infectious diseases: A synthesis of research findings from global and spatio-temporal perspectives. Environ. Int. 2017, 103, 99–108. [Google Scholar] [CrossRef]
- Kishore, N.; Marqués, D.; Mahmud, A.; Kiang, M.V.; Rodriguez, I.; Fuller, A.; Ebner, P.; Sorensen, C.; Racy, F.; Lemery, J. Mortality in puerto rico after hurricane maria. N. Engl. J. Med. 2018, 379, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.R.; Woodward, A.; Campbell-Lendrum, D.; Chadee Trinidad, D.D.; Honda, Y.; Liu, Q.; Aranda, C.; Berry, H. Human Health: Impacts, Adaptation, and Co-Benefits. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK, 2014; pp. 709–754. [Google Scholar]
- Rice, M.B.; Thurston, G.D.; Balmes, J.R.; Pinkerton, K.E. Climate change. A global threat to cardiopulmonary health. Am. J. Respir. Crit. Care Med. 2014, 189, 512–519. [Google Scholar] [CrossRef] [Green Version]
- United States Global Change Research Program (USGCRP). Fourth National Climate Assessment, Volume II: Impacts, Risks, and Adaptation in the United States. Available online: https://nca2018.globalchange.gov/ (accessed on 24 January 2021).
- Pachauri, R.K.; Allen, M.R.; Barros, V.R.; Broome, J.; Cramer, W.; Christ, R.; Church, J.A.; Clarke, L.; Dahe, Q.; Dasgupta, P. Climate Change 2014: Synthesis Report. Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Intergovernmental Panel on Climate Change: Geneva, Switzerland, 2014; ISBN 9291691437. [Google Scholar]
- Allen, M.R.; Barros, V.R.; Broome, J.; Cramer, W.; Christ, R.; Church, J.A.; Clarke, L.; Dahe, Q.; Dasgupta, P.; Dubash, N.K. IPCC Fifth Assessment Synthesis Report-Climate Change 2014 Synthesis Report; Intergovernmental Panel on Climate Change: Geneva, Switzerland, 2014. [Google Scholar]
- Fouillet, A.; Rey, G.; Laurent, F.; Pavillon, G.; Bellec, S.; Guihenneuc-Jouyaux, C.; Clavel, J.; Jougla, E.; Hémon, D. Excess mortality related to the August 2003 heat wave in France. Int. Arch. Occup. Environ. Health 2006, 80, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and Mortality in 11 Cities of the Eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Beagley, J.; Belesova, K.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D. The 2020 report of The Lancet Countdown on health and climate change: Responding to converging crises. Lancet 2020. [Google Scholar]
- Le Houérou, H.N. Climate change, drought and desertification. J. Arid Environ. 1996, 34, 133–185. [Google Scholar] [CrossRef] [Green Version]
- Goudie, A.S.; Middleton, N.J. The changing frequency of dust storms through time. Clim. Chang. 1992, 20, 197–225. [Google Scholar] [CrossRef]
- Chan, C.-C.; Chuang, K.-J.; Chen, W.-J.; Chang, W.-T.; Lee, C.-T.; Peng, C.-M. Increasing cardiopulmonary emergency visits by long-range transported Asian dust storms in Taiwan. Environ. Res. 2008, 106, 393–400. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Chen, Y.-S.; Chiu, H.-F.; Goggins, W.B. Effects of Asian dust storm events on daily stroke admissions in Taipei, Taiwan. Environ. Res. 2005, 99, 79–84. [Google Scholar] [CrossRef]
- Rublee, C.S.; Sorensen, C.J.; Lemery, J.; Wade, T.J.; Sams, E.A.; Hilborn, E.D.; Crooks, J.L. Associations between dust storms and intensive care unit admissions in the United States, 2000–2015. GeoHealth 2020, 4, e2020GH000260. [Google Scholar] [CrossRef] [PubMed]
- Perez, L.; Tobías, A.; Querol, X.; Pey, J.; Alastuey, A.; Díaz, J.; Sunyer, J. Saharan dust, particulate matter and cause-specific mortality: A case–crossover study in Barcelona (Spain). Environ. Int. 2012, 48, 150–155. [Google Scholar] [CrossRef]
- Kanatani, K.T.; Ito, I.; Al-Delaimy, W.K.; Adachi, Y.; Mathews, W.C.; Ramsdell, J.W. Desert dust exposure is associated with increased risk of asthma hospitalization in children. Am. J. Respir. Crit. Care Med. 2010, 182, 1475–1481. [Google Scholar] [CrossRef] [Green Version]
- Cheng, M.-F.; Ho, S.-C.; Chiu, H.-F.; Wu, T.-N.; Chen, P.-S.; Yang, C.-Y. Consequences of exposure to Asian dust storm events on daily pneumonia hospital admissions in Taipei, Taiwan. J. Toxicol. Environ. Heal. Part A 2008, 71, 1295–1299. [Google Scholar] [CrossRef]
- World Health Organization Flooding and communicable diseases fact sheet. Wkly. Epidemiol. Rec. Relev. Epidemiol Hebd. 2005, 80, 21–28.
- Brown, L.; Murray, V. Examining the relationship between infectious diseases and flooding in Europe: A systematic literature review and summary of possible public health interventions. Disaster Heal. 2013, 1, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panic, M.; Ford, J.D. A review of national-level adaptation planning with regards to the risks posed by climate change on infectious diseases in 14 OECD nations. Int. J. Environ. Res. Public Health 2013, 10, 7083–7109. [Google Scholar] [CrossRef] [PubMed]
- Greer, A.; Ng, V.; Fisman, D. Climate change and infectious diseases in North America: The road ahead. CMAJ 2008, 178, 715–722. [Google Scholar]
- Deeb, R.; Tufford, D.; Scott, G.I.; Moore, J.G.; Dow, K. Impact of climate change on Vibrio vulnificus abundance and exposure risk. Estuaries Coasts 2018, 41, 2289–2303. [Google Scholar] [CrossRef]
- Brokamp, C.; Beck, A.F.; Muglia, L.; Ryan, P. Combined sewer overflow events and childhood emergency department visits: A case-crossover study. Sci. Total Environ. 2017, 607, 1180–1187. [Google Scholar] [CrossRef]
- Markwell, P.; Ratard, R. Deaths Directly Caused by Hurricane Katrina. Available online: https://ldh.la.gov/assets/oph/Center-PHCH/Center-CH/stepi/specialstudies/2014PopwellRatard_KatrinaDeath_PostedOnline.pdf (accessed on 2 January 2020).
- Henderson, S.B.; Johnston, F.H. Measures of forest fire smoke exposure and their associations with respiratory health outcomes. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Rappold, A.G.; Stone, S.L.; Cascio, W.E.; Neas, L.M.; Kilaru, V.J.; Carraway, M.S.; Szykman, J.J.; Ising, A.; Cleve, W.E.; Meredith, J.T. Peat bog wildfire smoke exposure in rural North Carolina is associated with cardiopulmonary emergency department visits assessed through syndromic surveillance. Environ. Health Perspect. 2011, 119, 1415–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rappold, A.G.; Cascio, W.E.; Kilaru, V.J.; Stone, S.L.; Neas, L.M.; Devlin, R.B.; Diaz-Sanchez, D. Cardio-respiratory outcomes associated with exposure to wildfire smoke are modified by measures of community health. Environ. Heal. 2012, 11, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hänninen, O.O.; Salonen, R.O.; Koistinen, K.; Lanki, T.; Barregard, L.; Jantunen, M. Population exposure to fine particles and estimated excess mortality in Finland from an East European wildfire episode. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 414–422. [Google Scholar] [CrossRef] [Green Version]
- Kovats, R.S.; Campbell-Lendrum, D.; Matthies, F. Climate change and human health: Estimating avoidable deaths and disease. Risk Anal. 2005, 25, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- Frankovic, I. The Impact of Climate Change on Health Expenditures; Institut für Stochastik und Wirtschaftsmathematik: TU Wien, Austria, 2017. [Google Scholar]
- Samet, J. Public Health: Adapting to Climate Change. Issues Brief. 2010. Available online: https://media.rff.org/documents/RFF-IB-10-06.pdf (accessed on 2 March 2021).
- McMichael, C. Human mobility, climate change, and health: Unpacking the connections. Lancet Planet. Heal. 2020, 4, e217–e218. [Google Scholar] [CrossRef]
- Salas, R.N.; Knappenberger, P.; Hess, J.J. Lancet Countdown on Health and Climate Change: Policy Brief for the United States of America. London, United Kingdom. 2020. Available online: http://www.lancetcountdownus.org/wp-content/uploads/2020/12/FINAL-2020_12_02_Lancet-Countdown-Policy-Document-USA-ENG.pdf?hsCtaTracking=3d902c23-c855-441f-ab5d-61f4f76a2ea1%7C6d90df30-4bf7-42f3-a282-f61d5292a03e (accessed on 2 March 2021).
- Gamble, J.L.; Balbus, J.; Berger, M.; Bouye, K.; Campbell, V.; Chief, K.; Conlon, K.; Crimmins, A.; Flanagan, B.; Gonzalez-Maddux, C. Ch. 9: Populations of Concern; US Global Change Research Program: Washington, DC, USA, 2016.
- Philipsborn, R.P.; Chan, K. Climate change and global child health. Pediatrics 2018, 141. [Google Scholar] [CrossRef] [Green Version]
- Patz, J.A.; Gibbs, H.K.; Foley, J.A.; Rogers, J.V.; Smith, K.R. Climate change and global health: Quantifying a growing ethical crisis. Ecohealth 2007, 4, 397–405. [Google Scholar] [CrossRef]
- Levy, B.S.; Patz, J.A. Climate change, human rights, and social justice. Ann. Glob. Heal. 2015, 81, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.S.; Shandas, V.; Pendleton, N. The effects of historical housing policies on resident exposure to intra-urban heat: A study of 108 US urban areas. Climate 2020, 8, 12. [Google Scholar] [CrossRef] [Green Version]
- Nardone, A.; Rudolph, K.E.; Morello-Frosch, R.; Casey, J.A. Redlines and Greenspace: The Relationship between Historical Redlining and 2010 Greenspace across the United States. Environ. Health Perspect. 2021, 129, 17006. [Google Scholar] [CrossRef] [PubMed]
- Fleischman, L.; Franklin, M. Fumes across the Fence-Line: The Health Impacts of air Pollution from Oil & Gas Facilities on African American Communities; Boston Branch NAACP: Roxbury, MA, USA, 2017. [Google Scholar]
- Browne, D. Strategies to Protect the Planet can Reduce Cancer, Too. J. Natl. Med. Assoc. 2018, 110, 2–3. [Google Scholar] [CrossRef]
- Maantay, J. Zoning, equity, and public health. Am. J. Public Health 2001, 91, 1033–1041. [Google Scholar] [CrossRef] [Green Version]
- Dugard, J.; Alcaro, A. Let’s work together: Environmental and socioeconomic rights in the courts. S. Afr. J. Hum. Rights 2013, 29, 14–31. [Google Scholar] [CrossRef]
- Thind, M.P.S.; Tessum, C.W.; Azevedo, I.L.; Marshall, J.D. Fine particulate air pollution from electricity generation in the US: Health impacts by race, income, and geography. Environ. Sci. Technol. 2019, 53, 14010–14019. [Google Scholar] [CrossRef]
- Ragavan, M.I.; Marcil, L.E.; Garg, A. Climate Change as a Social Determinant of Health. Pediatrics 2020, 145, e20193169. [Google Scholar] [CrossRef]
- Bekkar, B.; Pacheco, S.; Basu, R.; DeNicola, N. Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the US: A systematic review. JAMA Netw. open 2020, 3, e208243. [Google Scholar] [CrossRef]
- The Guardian Ella Kissi-Debrah: How a Mother’s Fight for Justice May help Prevent Other Air Pollution Deaths? Available online: https://www.theguardian.com/environment/2020/dec/16/ella-kissi-debrah-mother-fight-justice-air-pollution-death (accessed on 25 January 2021).
- Suglia, S.F.; Gryparis, A.; Schwartz, J.; Wright, R.J. Association between traffic-related black carbon exposure and lung function among urban women. Environ. Health Perspect. 2008, 116, 1333–1337. [Google Scholar] [CrossRef]
- Sekine, K.; Shima, M.; Nitta, Y.; Adachi, M. Long term effects of exposure to automobile exhaust on the pulmonary function of female adults in Tokyo, Japan. Occup. Environ. Med. 2004, 61, 350–357. [Google Scholar] [CrossRef] [Green Version]
- Kan, H.; Heiss, G.; Rose, K.M.; Whitsel, E.; Lurmann, F.; London, S.J. Traffic exposure and lung function in adults: The Atherosclerosis Risk in Communities study. Thorax 2007, 62, 873–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, W.Q.; FitzGerald, J.M.; Carlsten, C.; Sadatsafavi, M.; Brauer, M. Associations of ambient air pollution with chronic obstructive pulmonary disease hospitalization and mortality. Am. J. Respir. Crit. Care Med. 2013, 187, 721–727. [Google Scholar] [CrossRef]
- Nichols, J.L.; Owens, E.O.; Dutton, S.J.; Luben, T.J. Systematic review of the effects of black carbon on cardiovascular disease among individuals with pre-existing disease. Int. J. Public Health 2013, 58, 707–724. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.R.; Jerrett, M.; Anderson, H.R.; Burnett, R.T.; Stone, V.; Derwent, R.; Atkinson, R.W.; Cohen, A.; Shonkoff, S.B.; Krewski, D. Public health benefits of strategies to reduce greenhouse-gas emissions: Health implications of short-lived greenhouse pollutants. Lancet 2009, 374, 2091–2103. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Nethery, R.C.; Sabath, M.B.; Braun, D.; Dominici, F. Air pollution and COVID-19 mortality in the United States: Strengths and limitations of an ecological regression analysis. Sci. Adv. 2020, 6, eabd4049. [Google Scholar] [CrossRef]
- Limaye, V.S.; Max, W.; Constible, J.; Knowlton, K. Estimating the Health-Related Costs of 10 Climate-Sensitive U.S. Events During 2012. GeoHealth 2019, 3, 245–265. [Google Scholar] [CrossRef] [PubMed]
- Knowlton, K.; Rotkin-Ellman, M.; Geballe, L.; Max, W.; Solomon, G.M. Six climate change-related events in the United States accounted for about $14 billion in lost lives and health costs. Health Aff. 2011, 30, 2167–2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Centers for Environmental Information Billion-Dollar Weather and Climate Disasters: Overview. Available online: https://www.ncdc.noaa.gov/billions/ (accessed on 25 January 2021).
- International Federation of Red Cross and Red Crescent Societies. World Disasters Report 2020; International Federation of Red Cross and Red Crescent Societies: Geneva, Switzerland, 2020. [Google Scholar]
- World Meteorological Organization. The State of the Global Climate 2020. Available online: https://public.wmo.int/en/our-mandate/climate/wmo-statement-state-of-global-climate (accessed on 25 January 2021).
- Awumbila, M. Drivers of Migration and Urbanization in Africa: Key Trends and Issues; UN Expert Group Meeting on Sustainable Cities, Human Mobility and International Migration: New York, NY, USA, 2017. [Google Scholar]
- Blaine, T.; Ryan, S.; Zermoglio, F.; Quinn, C. Understanding and Responding to the Shifting Burden of Disease: Malaria Risks in Africa Under a Changing Climate. Available online: https://ui.adsabs.harvard.edu/abs/2018AGUFMGH21C1084B/abstract (accessed on 2 March 2021).
- Quinn, C.; Blaine, T.; Zermoglio, F.; Colborn, J.; Ebi, K. Integrating Climate Change and Variability into Infectious Disease Decision Making: Lessons from sub-Saharan. 2018, pp. 1–2. Available online: https://ui.adsabs.harvard.edu/abs/2018AGUFMGH23A..07Q/abstract (accessed on 2 March 2021).
- Nshimiyimana, L.; Onyambu, P.M.; Rutayisire, E. Diarrhoeal Diseases in Children Under Five Years Exhibited Space-Time Disparities and Priority Areas for Control Interventions in Rwanda CURRENT STATUS: UNDER REVIEW. Int. J. Health Geogr. 2019, 1–20. [Google Scholar]
- Korukire, N.; Bozzi, L.; Banamwana, G.; Birasa, L.; Ineza, M.C.; Rumagihwa, L.; Cishahayo, E.U.; Kayitesi, I.; Akanbi, M.O. Climate Change and Mental Health: New Model of Managing Mental Health Illness Resulting From Climate Change Events. Rwanda Perspective. Rwanda J. Med. Heal. Sci. 2019, 2, 62–65. [Google Scholar] [CrossRef]
- Kirby, M.; Nagel, C.; Uejio, C.; Okull, P.; Nsabimana, J.A.; Habyarimana, J.; Clasen, T. Effect of precipitation on clinic-diagnosed enteric infections in children in Rwanda: An observational study. Lancet Planet. Heal. 2018, 2, S14. [Google Scholar] [CrossRef]
- Kula, N.; Haines, A.; Fryatt, R. Reducing Vulnerability to Climate Change in Sub-Saharan Africa: The Need for Better Evidence. PLoS Med. 2013, 10. [Google Scholar] [CrossRef] [Green Version]
- Matinga, M.N.; Clancy, J.S.; Annegarn, H.J. Explaining the non-implementation of health-improving policies related to solid fuels use in South Africa. Energy Policy 2014, 68, 53–59. [Google Scholar] [CrossRef]
- Scorgie, Y.; Annegarn, H.; Burger, L. Study to Examine the Potential Socio-Economic Impact of Measures to Reduce Air Pollution from Combustion; University of Johannesburg: Johannesburg, South Africa, 2004. [Google Scholar]
- Norman, R.; Cairncross, E.; Witi, J.; Bradshaw, D.; Collaboration, S.A.C.R.A. Estimating the burden of disease attributable to urban outdoor air pollution in South Africa in 2000. S. Afr. Med. J. 2007, 97, 782–790. [Google Scholar]
- Shirinde, J.; Wichmann, J.; Voyi, K. Association between wheeze and selected air pollution sources in an air pollution priority area in South Africa: A cross-sectional study. Environ. Heal. 2014, 13, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikomeye, J.C. Knowledge and Practices towards Malnutrition AMONG caregivers of Under Five Children in Ngoma District, Rwanda. Ph.D. Thesis, Mount Kenya University, Thika, Kenya, 2017. [Google Scholar]
- Stanke, C.; Kerac, M.; Prudhomme, C.; Medlock, J.; Murray, V. Health effects of drought: A systematic review of the evidence. PLoS Curr. 2013, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell-Lendrum, D.H.; Corvalan, C.F.; Prüss Ustün, A. How much disease could climate change cause. Clim. Chang. Hum. Heal. Risks Responses. Geneva WHO 2003, 133–158. [Google Scholar]
- Cline, W.R. Global Warming and Agriculture: Impact Estimates by Country; Center for Global Development, Peterson Institute for International Economics: Washington DC, USA, 2007; ISBN 088132535X. [Google Scholar]
- Cooper, P.J.M.; Dimes, J.; Rao, K.P.C.; Shapiro, B.; Shiferaw, B.; Twomlow, S. Coping better with current climatic variability in the rain-fed farming systems of sub-Saharan Africa: An essential first step in adapting to future climate change? Agric. Ecosyst. Environ. 2008, 126, 24–35. [Google Scholar] [CrossRef] [Green Version]
- World Food Program. Rwanda Comprehensive Food Security and Vulnerability Analysis: World Food Program; World Food Program: Kigali, Rwanda, 2015. [Google Scholar]
- Grace, K.; Davenport, F.; Funk, C.; Lerner, A.M. Child malnutrition and climate in Sub-Saharan Africa: An analysis of recent trends in Kenya. Appl. Geogr. 2012, 35, 405–413. [Google Scholar] [CrossRef]
- United Nations Development Programme. Climate Change Adaptation in Africa: UNDP Synthesis of Experiences and Recommendations; United Nations Development Programme: Thailand, Bangkok, 2018. [Google Scholar]
- Thompson, H.E.; Berrang-Ford, L.; Ford, J.D. Climate change and food security in sub-Saharan Africa: A systematic literature review. Sustainability 2010, 2, 2719–2733. [Google Scholar] [CrossRef] [Green Version]
- Australian International Food Security Centre Food Security and Why It Matters. Available online: https://aifsc.aciar.gov.au/food-security-and-why-it-matters.html (accessed on 6 December 2020).
- USAID. Rwanda: Nutrition Profile. Available online: https://www.usaid.gov/sites/default/files/documents/1864/Rwanda-Nutrition-Profile-Mar2018-508.pdf (accessed on 2 March 2021).
- Paridaens, A.-M.; Jayasinghe, S. Rwanda 2018 Comprehensive Food Security and Vulnerability Analysis; National Institute of Statistics of Rwanda: Kigali, Rwanda, 2018.
- Twongyirwe, R.; Mfitumukiza, D.; Barasa, B.; Naggayi, B.R.; Odongo, H.; Nyakato, V.; Mutoni, G. Perceived effects of drought on household food security in South-western Uganda: Coping responses and determinants. Weather Clim. Extrem. 2019, 24, 100201. [Google Scholar] [CrossRef]
- Afifi, T.; Liwenga, E.; Kwezi, L. Rainfall-induced crop failure, food insecurity and out-migration in Same-Kilimanjaro, Tanzania. Clim. Dev. 2014, 6, 53–60. [Google Scholar] [CrossRef]
- Emaziye, P.O.; Okoh, R.N.; Ike, P.C. An Evaluation of Effect of Climate Change on Food Security of Rural Households in Cross River State, Nigeria. Asian J. Agric. Sci. 2013, 5, 56–61. [Google Scholar] [CrossRef]
- Burke, A.; Fishel, S. A coal elimination treaty 2030: Fast tracking climate change mitigation, global health and security. Earth Syst. Gov. 2020, 100046. [Google Scholar] [CrossRef]
- Meinshausen, M.; Meinshausen, N.; Hare, W.; Raper, S.C.B.; Frieler, K.; Knutti, R.; Frame, D.J.; Allen, M.R. Greenhouse-gas emission targets for limiting global warming to 2 C. Nature 2009, 458, 1158–1162. [Google Scholar] [CrossRef]
- Shindell, D.; Faluvegi, G.; Seltzer, K.; Shindell, C. Quantified, localized health benefits of accelerated carbon dioxide emissions reductions. Nat. Clim. Chang. 2018, 8, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Widder, L. Earth eco-building: Textile-reinforced earth block construction. Energy Procedia 2017, 122, 757–762. [Google Scholar] [CrossRef]
- Devi, K.S.; Lakshmi, V.V.; Alakanandana, A. Impacts of cement industry on environment-an overview. Asia Pac. J. Res 2017, 1, 156–161. [Google Scholar]
- Sugiyama, M. Climate change mitigation and electrification. Energy Policy 2012, 44, 464–468. [Google Scholar] [CrossRef]
- Frizen, K. Aggregate effect of the intended nationally determined contributions: An update. In Proceedings of the Conference of the Parties Twenty—Second Session, Marrakech, Morocco, 7–18 November 2016. [Google Scholar]
- Tambo, E.; Duo-quan, W.; Zhou, X.-N. Tackling air pollution and extreme climate changes in China: Implementing the Paris climate change agreement. Environ. Int. 2016, 95, 152–156. [Google Scholar] [CrossRef]
- Gallagher, K.S.; Zhang, F.; Orvis, R.; Rissman, J.; Liu, Q. Assessing the Policy gaps for achieving China’s climate targets in the Paris Agreement. Nat. Commun. 2019, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center for Climate and Energy Solutions. China’s Nationally Determined Contributions to the Paris Agreement; Center for Climate and Energy Solutions: Arlington, VA, USA, 2015. [Google Scholar]
- Vennemo, H.; Aunan, K.; Jinghua, F.; Holtedahl, P.; Tao, H.; Seip, H.M. Domestic environmental benefits of China’s energy-related CDM potential. Clim. Chang. 2006, 75, 215–239. [Google Scholar] [CrossRef]
- Klausbruckner, C.; Annegarn, H.; Henneman, L.R.F.; Rafaj, P. A policy review of synergies and trade-offs in South African climate change mitigation and air pollution control strategies. Environ. Sci. Policy 2016, 57, 70–78. [Google Scholar] [CrossRef]
- Department of Environmental Affairs. National Climate Change Response: White Paper; Department of Environmental Affairs: Pretoria, South Africa, 2012.
- Papafotiou, E.; Katsifarakis, K.L. Ecological Rainwater Management in Urban Areas. Preliminary Considerations for the City of Corinth, Greece. Agric. Agric. Sci. Procedia 2015, 4, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Chiang, Y.-C.; Sullivan, W.; Larsen, L. Measuring neighborhood walkable environments: A comparison of three approaches. Int. J. Environ. Res. Public Health 2017, 14, 593. [Google Scholar] [CrossRef] [Green Version]
- Kabisch, N.; Frantzeskaki, N.; Pauleit, S.; Naumann, S.; Davis, M.; Artmann, M.; Haase, D.; Knapp, S.; Korn, H.; Stadler, J. Nature-based solutions to climate change mitigation and adaptation in urban areas: Perspectives on indicators, knowledge gaps, barriers, and opportunities for action. Ecol. Soc. 2016, 21. [Google Scholar] [CrossRef] [Green Version]
- Eggermont, H.; Balian, E.; Azevedo, J.M.N.; Beumer, V.; Brodin, T.; Claudet, J.; Fady, B.; Grube, M.; Keune, H.; Lamarque, P. Nature-based solutions: New influence for environmental management and research in Europe. GAIA-Ecological Perspect. Sci. Soc. 2015, 24, 243–248. [Google Scholar] [CrossRef]
- Ziervogel, G.; New, M.; Archer van Garderen, E.; Midgley, G.; Taylor, A.; Hamann, R.; Stuart-Hill, S.; Myers, J.; Warburton, M. Climate change impacts and adaptation in South Africa. Wiley Interdiscip. Rev. Clim. Chang. 2014, 5, 605–620. [Google Scholar] [CrossRef]
- Alemayehu, F.R.; Bendevis, M.A.; Jacobsen, S.E. The Potential for Utilizing the Seed Crop Amaranth (Amaranthus spp.) in East Africa as an Alternative Crop to Support Food Security and Climate Change Mitigation. J. Agron. Crop Sci. 2015, 201, 321–329. [Google Scholar] [CrossRef]
- Elum, Z.A.; Modise, D.M.; Marr, A. Farmer’s perception of climate change and responsive strategies in three selected provinces of South Africa. Clim. Risk Manag. 2017, 16, 246–257. [Google Scholar] [CrossRef]
- Friel, S.; Dangour, A.D.; Garnett, T.; Lock, K.; Chalabi, Z.; Roberts, I.; Butler, A.; Butler, C.D.; Waage, J.; McMichael, A.J.; et al. Public health benefits of strategies to reduce greenhouse-gas emissions: Food and agriculture. Lancet 2009, 374, 2016–2025. [Google Scholar] [CrossRef]
- Hu, F.B.; Manson, J.E.; Willett, W.C. Types of dietary fat and risk of coronary heart disease: A critical review. J. Am. Coll. Nutr. 2001, 20, 5–19. [Google Scholar] [CrossRef]
- Stoeckli, R.; Keller, U. Nutritional fats and the risk of type 2 diabetes and cancer. Physiol. Behav. 2004, 83, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Craggs, G. Photosynthesis and its Role in Climate Change and Soil Regeneration. Available online: https://www.futuredirections.org.au/publication/photosynthesis-role-climate-change-soil-regeneration (accessed on 6 December 2020).
- Bowler, D.E.; Buyung-Ali, L.; Knight, T.M.; Pullin, A.S. Urban greening to cool towns and cities: A systematic review of the empirical evidence. Landsc. Urban Plan. 2010, 97, 147–155. [Google Scholar] [CrossRef]
- Nurse, J.; Basher, D.; Bone, A.; Bird, W. An ecological approach to promoting population mental health and well-being—A response to the challenge of climate change. Perspect. Public Health 2010, 130, 27–33. [Google Scholar] [CrossRef]
- Lipper, L.; Thornton, P.; Campbell, B.M.; Baedeker, T.; Braimoh, A.; Bwalya, M.; Caron, P.; Cattaneo, A.; Garrity, D.; Henry, K.; et al. Climate-smart agriculture for food security. Nat. Clim. Chang. 2014, 4, 1068–1072. [Google Scholar] [CrossRef]
- McCarthy, N.; Lipper, L.; Branca, G. Climate-smart agriculture: Smallholder adoption and implications for climate change adaptation and mitigation. Mitig. Clim. Chang. Agric. Work. Pap. 2011, 3, 1–37. [Google Scholar]
- FAO Overview | Climate-Smart Agriculture | Food and Agriculture Organization of the United Nations. Available online: http://www.fao.org/climate-smart-agriculture/overview/en/ (accessed on 31 July 2020).
- Khatri-Chhetri, A.; Aggarwal, P.K.; Joshi, P.K.; Vyas, S. Farmers’ prioritization of climate-smart agriculture (CSA) technologies. Agric. Syst. 2017, 151, 184–191. [Google Scholar] [CrossRef]
- Amy, C. A virtuous cycle of virtually no waste: Climate-smart agriculture featured at Food Security Forum—Forests, Trees and Agroforestry. Available online: https://www.foreststreesagroforestry.org/news-article/a-virtuous-cycle-of-virtually-no-waste-climate-smart-agriculture-featured-at-food-security-forum/ (accessed on 21 August 2020).
- Bayala, J.; Sanou, J.; Teklehaimanot, Z.; Kalinganire, A.; Ouédraogo, S.J. Parklands for buffering climate risk and sustaining agricultural production in the Sahel of West Africa. Curr. Opin. Environ. Sustain. 2014, 6, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Mbow, C.; Van Noordwijk, M.; Luedeling, E.; Neufeldt, H.; Minang, P.A.; Kowero, G. Agroforestry solutions to address food security and climate change challenges in Africa. Curr. Opin. Environ. Sustain. 2014, 6, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Ofori, D.A.; Gyau, A.; Dawson, I.K.; Asaah, E.; Tchoundjeu, Z.; Jamnadass, R. Developing more productive African agroforestry systems and improving food and nutritional security through tree domestication. Curr. Opin. Environ. Sustain. 2014, 6, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Lwasa, S.; Mugagga, F.; Wahab, B.; Simon, D.; Connors, J.; Griffit, C. Urban and peri-urban agriculture and forestry: Transcending poverty alleviation to climate change mitigation and adaptation. Urban Clim. 2014, 7, 92–106. [Google Scholar] [CrossRef]
- Alberti, M.; Marzluff, J.M. Ecological resilience in urban ecosystems: Linking urban patterns to human and ecological functions. Urban Ecosyst. 2004, 7, 241–265. [Google Scholar] [CrossRef]
- McDonnell, M.J.; Pickett, S.T.A.; Groffman, P.; Bohlen, P.; Pouyat, R.V.; Zipperer, W.C.; Parmelee, R.W.; Carreiro, M.M.; Medley, K. Ecosystem processes along an urban-to-rural gradient. In Urban Ecology; Springer: Boston, MA, USA, 2008; pp. 299–313. [Google Scholar]
- Pandey, S.S.; Cockfield, G.; Maraseni, T.N. Assessing the roles of community forestry in climate change mitigation and adaptation: A case study from Nepal. For. Ecol. Manag. 2016, 360, 400–407. [Google Scholar] [CrossRef]
- Karliner, J.; Slotterback, S.; Boyd, R.; Ashby, B.; Steele, K. Health Care’s Climate Footprint: How the Health Sector Contributes to the Global Climate Crisis and Opportunities for Action 2019. Available online: https://noharm-global.org/sites/default/files/documents-files/5961/HealthCaresClimateFootprint_092319.pdf (accessed on 2 March 2021).
- Balbus, J.; Berry, P.; Brettle, M.; Jagnarine-Azan, S.; Soares, A.; Ugarte, C.; Varangu, L.; Prats, E.V. Enhancing the sustainability and climate resiliency of health care facilities: A comparison of initiatives and toolkits. Rev. Panam. Salud Pública 2016, 40, 174–180. [Google Scholar] [PubMed]
- The World Bank Climate-Smart Healthcare: Low-Carbon and Resilience Strategies for the Health Sector—2017. Available online: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/322251495434571418/climate-smart-healthcare-low-carbon-and-resilience-strategies-for-the-health-sector (accessed on 25 January 2021).
- Hassan, S.; Nguyen, M.; Buchanan, M.; Grimshaw, A.; Adams, O.P.; Hassell, T.; Ragster, L.; Nunez-Smith, M. Management of Chronic Noncommunicable Diseases After Natural Disasters in the Caribbean: A Scoping Review: A scoping review of literature published between 1974 and 2020 examining the burden and management of chronic noncommunicable diseases after natural. Health Aff. 2020, 39, 2136–2143. [Google Scholar] [CrossRef]
- Boyer, C.J.; Bowen, K.; Murray, V.; Hadley, J.; Hilly, J.J.; Hess, J.J.; Ebi, K.L. Using Implementation Science For Health Adaptation: Opportunities For Pacific Island Countries. Health Aff. 2020, 39, 2160–2167. [Google Scholar] [CrossRef]
- National Health Service Delivering a “Net Zero” National Health Service. Available online: https://www.england.nhs.uk/greenernhs/wp-content/uploads/sites/51/2020/10/delivering-a-net-zero-national-health-service.pdf (accessed on 25 January 2021).
- Salas, R.N.; Jha, A.K. Climate change threatens the achievement of effective universal healthcare. BMJ 2019, 366, l5302. [Google Scholar] [CrossRef] [PubMed]
- Salas, R.N.; Maibach, E.; Pencheon, D.; Watts, N.; Frumkin, H. A pathway to net zero emissions for healthcare. BMJ 2020, 371, m3785. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Maldives Green CLIMATE-Smart Hospitals: Hospital Vulnerability Analysis and Report; World Health Organization (WHO): Geneva, Switzerland, 2018. [Google Scholar]
- The World Bank. Madagascar—Climate Change and Health Diagnostic: Risks and Opportunities for Climate-Smart Health and Nutrition Investment; The World Bank Group: Washington, DC, USA, 2018. [Google Scholar]
- UNFCCC National Adaptation Plans. Available online: https://www4.unfccc.int/sites/NAPC/News/Pages/national_adaptation_plans.aspx (accessed on 25 January 2021).
- World Health Organization (WHO). Bangladesh Health-National Adaptation Plan (HNAP); World Health Organization (WHO): Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization (WHO). Health and Climate Change Country Profiles. Available online: https://www.who.int/activities/monitoring-health-impacts-of-climate-change-and-national-progress (accessed on 25 January 2021).
- Shea, B.; Knowlton, K.; Shaman, J. Assessment of climate-health curricula at international health professions schools. JAMA Netw. Open 2020, 3, e206609. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, C.; Murray, V.; Lemery, J.; Balbus, J. Climate change and women’s health: Impacts and policy directions. PLoS Med. 2018, 15, e1002603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemery, J.; Balbus, J.; Sorensen, C.; Rublee, C.; Dresser, C.; Balsari, S.; Calvello Hynes, E. Training Clinical and Public Health Leaders In Climate And Health: Commentary explores training clinical and public health leaders in climate and health. Health Aff. 2020, 39, 2189–2196. [Google Scholar] [CrossRef]
- Patz, J.A. Solving the global climate crisis: The greatest health opportunity of our times? Public Health Rev. 2016, 37, 30. [Google Scholar] [CrossRef] [Green Version]
- Howard, C.; Huston, P. Climate change and infectious diseases: The solutions: The health effects of climate change: Know the risks and become part of the solutions. Canada Commun. Dis. Rep. 2019, 45, 114. [Google Scholar] [CrossRef] [PubMed]
- Kuo, F.E.; Sullivan, W.C. Aggression and violence in the inner city effects of environment via mental fatigue. Environ. Behav. 2001, 33, 543–571. [Google Scholar] [CrossRef]
- Kuo, F.E.; Sullivan, W.C. Environment and crime in the inner city does vegetation reduce crime? Environ. Behav. 2001, 33, 343–367. [Google Scholar] [CrossRef]
- Hamilton, K.; Brahmbhatt, M.; Liu, J. Multiple Benefits from Climate Change Mitigation: Assessing the Evidence. Available online: https://www.lse.ac.uk/granthaminstitute/wp-content/uploads/2017/11/Multiple-benefits-from-climate-action_Hamilton-et-al-1.pdf (accessed on 2 March 2021).
- RAWGraphs. Available online: https://app.rawgraphs.io/ (accessed on 25 January 2021).
- Jiang, L.; O’Neill, B.C. Global urbanization projections for the Shared Socioeconomic Pathways. Glob. Environ. Chang. 2017, 42, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.Y. The role of urban green infrastructure in offsetting carbon emissions in 35 major Chinese cities: A nationwide estimate. Cities 2015, 44, 112–120. [Google Scholar] [CrossRef]
- Nowak, D.J.; Greenfield, E.J.; Hoehn, R.E.; Lapoint, E. Carbon storage and sequestration by trees in urban and community areas of the United States. Environ. Pollut. 2013, 178, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Pauleit, S.; Ambrose-Oji, B.; Andersson, E.; Anton, B.; Buijs, A.; Haase, D.; Elands, B.; Hansen, R.; Kowarik, I.; Kronenberg, J. Advancing urban green infrastructure in Europe: Outcomes and reflections from the GREEN SURGE project. Urban For. Urban Green. 2019, 40, 4–16. [Google Scholar] [CrossRef]
- Younger, M.; Morrow-Almeida, H.R.; Vindigni, S.M.; Dannenberg, A.L. The built environment, climate change, and health: Opportunities for co-benefits. Am. J. Prev. Med. 2008, 35, 517–526. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health Benefits from Nature Experiences Depend on Dose. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Chun, B.; Guldmann, J.-M. Impact of greening on the urban heat island: Seasonal variations and mitigation strategies. Comput. Environ. Urban Syst. 2018, 71, 165–176. [Google Scholar] [CrossRef]
- US EPA What is Green Infrastructure? | Green Infrastructure | US EPA. Available online: https://www.epa.gov/green-infrastructure/what-green-infrastructure (accessed on 11 September 2020).
- World Health Organization Health in the Green Economy: Health Co-Benefits of Climate Change Mitigation—Transport Sector; World Health Organization: Geneva, Switzerland, 2012.
- Beyer, K.M.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.J.; Malecki, K.M. Exposure to neighborhood green space and mental health: Evidence from the survey of the health of Wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef] [Green Version]
- Mantler, A.; Logan, A.C. Natural environments and mental health. Adv. Integr. Med. 2015, 2, 5–12. [Google Scholar] [CrossRef]
- Thomas, F. The role of natural environments within women’s everyday health and wellbeing in Copenhagen, Denmark. Heal. Place 2015, 35, 187–195. [Google Scholar] [CrossRef] [PubMed]
- McCormick, R. Does Access to Green Space Impact the Mental Well-being of Children: A Systematic Review. J. Pediatr. Nurs. 2017, 37, 3–7. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would you be happier living in a greener urban area? A fixed-effects analysis of panel data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef]
- Cheng, J.J.; Berry, P. Health co-benefits and risks of public health adaptation strategies to climate change: A review of current literature. Int. J. Public Health 2013, 58, 305–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikomeye, J.; Balza, J.; Beyer, K. The Impact of Schoolyard Greening on Children’s Physical Activity and Socioemotional Health: A Systematic Review of Experimental Studies. Int. J. Environ. Res. Public Health 2021, 18, 535. [Google Scholar] [CrossRef]
- Kardan, O.; Gozdyra, P.; Misic, B.; Moola, F.; Palmer, L.J.; Paus, T.; Berman, M.G. Neighborhood greenspace and health in a large urban center. Sci. Rep. 2015, 5, 1_13. [Google Scholar] [CrossRef] [Green Version]
- Loukaitou-Sideris, A.; Levy-Storms, L.; Chen, L.; Brozen, M. Parks for an aging population: Needs and preferences of low-income seniors in Los Angeles. J. Am. Plan. Assoc. 2016, 82, 236–251. [Google Scholar] [CrossRef]
- Yang, B.-Y.; Markevych, I.; Bloom, M.S.; Heinrich, J.; Guo, Y.; Morawska, L.; Dharmage, S.C.; Knibbs, L.D.; Jalaludin, B.; Jalava, P.; et al. Community greenness, blood pressure, and hypertension in urban dwellers: The 33 Communities Chinese Health Study. Environ. Int. 2019, 126, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Beyer, K.M.M.; Szabo, A.; Hoormann, K.; Stolley, M. Time spent outdoors, activity levels, and chronic disease among American adults. J. Behav. Med. 2018, 41, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, M.J. Influence of urban and transport planning and the city environment on cardiovascular disease /692/4019 /692/499 review-article. Nat. Rev. Cardiol. 2018, 15, 432–438. [Google Scholar] [CrossRef]
- Yeager, R.; Riggs, D.W.; DeJarnett, N.; Tollerud, D.J.; Wilson, J.; Conklin, D.J.; O’Toole, T.E.; McCracken, J.; Lorkiewicz, P.; Xie, Z.; et al. Association between residential greenness and cardiovascular disease risk. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef]
- Yeager, R.A.; Smith, T.R.; Bhatnagar, A. Green environments and cardiovascular health. Trends Cardiovasc. Med. 2020, 30, 241–246. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Roe, J.J.; Thompson, C.W.; Aspinall, P.A.; Brewer, M.J.; Duff, E.I.; Miller, D.; Mitchell, R.; Clow, A. Green space and stress: Evidence from cortisol measures in deprived urban communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, C.W.; Roe, J.; Aspinall, P.; Mitchell, R.; Clow, A.; Miller, D. More green space is linked to less stress in deprived communities: Evidence from salivary cortisol patterns. Landsc. Urban Plan. 2012, 105, 221–229. [Google Scholar] [CrossRef] [Green Version]
- Bogar, S.; Beyer, K. Green Space, Violence, and Crime: A Systematic Review. Trauma. Violence Abuse 2015, 17. [Google Scholar] [CrossRef]
- Weed, M.; Foad, A. Rapid Scoping Review of Evidence of Outdoor Transmission of COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Shoari, N.; Ezzati, M.; Baumgartner, J.; Malacarne, D.; Fecht, D. Accessibility and allocation of public parks and gardens in England and Wales: A COVID-19 social distancing perspective. PLoS ONE 2020, 15, e0241102. [Google Scholar] [CrossRef] [PubMed]
- Courtemanche, C.; Garuccio, J.; Le, A.; Pinkston, J.; Yelowitz, A. Strong Social Distancing Measures in the United States Reduced The COVID-19 Growth Rate. Health Aff. 2020, 39, 1237–1246. [Google Scholar] [CrossRef] [PubMed]
- Freeman, S.; Eykelbosh, A. COVID-19 and outdoor safety: Considerations for use of outdoor recreational spaces. Available online: https://ncceh.ca/sites/default/files/COVID-19OutdoorSafety—April162020.pdf (accessed on 4 May 2020).
- Leclerc, Q.J.; Fuller, N.M.; Knight, L.E.; Funk, S.; Knight, G.M. What settings have been linked to SARS-CoV-2 transmission clusters? Wellcome Open Res. 2020, 5, 83. [Google Scholar] [CrossRef]
- Venter, Z.S.; Barton, D.N.; Gundersen, V.; Figari, H. Urban nature in a time of crisis: Recreational use of green space increases during the COVID-19 outbreak in Oslo, Norway. Environ. Res. Lett. 2020, 15, 104075. [Google Scholar] [CrossRef]
- Brink, L.A.; Nigg, C.R.; Lampe, S.M.R.; Kingston, B.A.; Mootz, A.L.; Van Vliet, W. Influence of schoolyard renovations on children’s physical activity: The learning landscapes program. Am. J. Public Health 2010, 100, 1672–1678. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Aggio, D.; Knock, G.; Kipps, C.; Shankar, A.; Smith, L. Effect of major school playground reconstruction on physical activity and sedentary behaviour: Camden active spaces. BMC Public Health 2017. [Google Scholar] [CrossRef] [Green Version]
- Wallner, P.; Kundi, M.; Arnberger, A.; Eder, R.; Allex, B.; Weitensfelder, L.; Hutter, H.P. Reloading pupils’ batteries: Impact of green spaces on cognition and wellbeing. Int. J. Environ. Res. Public Health 2018, 15, 1205. [Google Scholar] [CrossRef] [Green Version]
- Kelz, C.; Evans, G.W.; Röderer, K. The Restorative Effects of Redesigning the Schoolyard: A Multi-Methodological, Quasi-Experimental Study in Rural Austrian Middle Schools. Environ. Behav. 2015, 47, 119–139. [Google Scholar] [CrossRef] [Green Version]
- van Dijk-Wesselius, J.E.; Maas, J.; Hovinga, D.; van Vugt, M.; van den Berg, A.E. The impact of greening schoolyards on the appreciation, and physical, cognitive and social-emotional well-being of schoolchildren: A prospective intervention study. Landsc. Urban Plan. 2018, 180, 15–26. [Google Scholar] [CrossRef]
- Raney, M.A.; Hendry, C.F.; Yee, S.A. Physical Activity and Social Behaviors of Urban Children in Green Playgrounds. Am. J. Prev. Med. 2019, 56, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Floyd, M.F.; Rodríguez, D.A.; Saelens, B.E. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation 2012, 125, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Goran, M.I.; Ball, G.D.C.; Cruz, M.L. Obesity and risk of type 2 diabetes and cardiovascular disease in children and adolescents. J. Clin. Endocrinol. Metab. 2003, 88, 1417–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillaume, M.; Lapidus, L.; Björntorp, P.; Lambert, A. Physical activity, obesity, and cardiovascular risk factors in children. The Belgian Luxembourg Child Study II. Obes. Res. 1997, 5, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Goran, M.I.; Reynolds, K.D.; Lindquist, C.H. Role of physical activity in the prevention of obesity in children. Int. J. Obes. 1999, 23, S18–S33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hills, A.P.; Andersen, L.B.; Byrne, N.M. Physical activity and obesity in children. Br. J. Sports Med. 2011, 45, 866–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodney, J.P.; Maddock, J.E. HHS Public Access. Physiol. Behav. 2017, 176, 139–148. [Google Scholar] [CrossRef]
- World Health Organization Health in the Green Economy: Health Co-Benefits of Climate Change Mitigation-Housing Sector; World Health Organization: Geneva, Switzerland, 2011; ISBN 9241501715.
- Lak, A.; Asl, S.S.; Maher, A. Resilient urban form to pandemics: Lessons from COVID-19. Med. J. Islam. Repub. Iran 2020, 34, 71. [Google Scholar]
- Rosenzweig, C.; Tubiello, F.N. Adaptation and mitigation strategies in agriculture: An analysis of potential synergies. Mitig. Adapt. Strateg. Glob. Chang. 2007, 12, 855–873. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.; Kitchen, P. Sense of place and health in Hamilton, Ontario: A case study. Soc. Indic. Res. 2012, 108, 257–276. [Google Scholar] [CrossRef] [Green Version]
- Deligios, P.A.; Chergia, A.P.; Sanna, G.; Solinas, S.; Todde, G.; Narvarte, L.; Ledda, L. Climate change adaptation and water saving by innovative irrigation management applied on open field globe artichoke. Sci. Total Environ. 2019, 649, 461–472. [Google Scholar] [CrossRef]
- Moya, P.; Hong, L.; Dawe, D.; Chongde, C. The impact of on-farm water saving irrigation techniques on rice productivity and profitability in Zhanghe Irrigation System, Hubei, China. Paddy Water Environ. 2004, 2, 207–215. [Google Scholar] [CrossRef]
- Freeman, M.C.; Garn, J.V.; Sclar, G.D.; Boisson, S.; Medlicott, K.; Alexander, K.T.; Penakalapati, G.; Anderson, D.; Mahtani, A.G.; Grimes, J.E.T. The impact of sanitation on infectious disease and nutritional status: A systematic review and meta-analysis. Int. J. Hyg. Environ. Health 2017, 220, 928–949. [Google Scholar] [CrossRef]
- Eckelman, M.J.; Sherman, J. Environmental impacts of the US health care system and effects on public health. PLoS ONE 2016, 11, e0157014. [Google Scholar] [CrossRef] [Green Version]
- US Environmental Protection Agency. The Benefits and Costs of the Clean Air Act, 1970 to 1990; U.S. Environmental Protection Agency: Washington, DC, USA, 1997.
- Friel, S.; Bowen, K.; Campbell-Lendrum, D.; Frumkin, H.; McMichael, A.J.; Rasanathan, K. Climate change, noncommunicable diseases, and development: The relationships and common policy opportunities. Annu. Rev. Public Health 2011, 32, 133–147. [Google Scholar] [CrossRef] [Green Version]
- Hess, J.; Boodram, L.-L.G.; Paz, S.; Ibarra, A.M.S.; Wasserheit, J.N.; Lowe, R. Strengthening the global response to climate change and infectious disease threats. BMJ 2020, 371, m3081. [Google Scholar] [CrossRef]
- Khomenko, S.; Cirach, M.; Pereira-Barboza, E.; Mueller, N.; Barrera-Gómez, J.; Rojas-Rueda, D.; de Hoogh, K.; Hoek, G.; Nieuwenhuijsen, M. Premature mortality due to air pollution in European cities: A health impact assessment. Lancet Planet. Heal. 2021. [Google Scholar] [CrossRef]
- Chang, K.M.; Hess, J.J.; John, M.; Dean, A.; Green, D.; Partanen, A.; Estella, S.; Zhang, Y.; Smith, S.J.; Bowden, J.H.; et al. Co-benefits of global, domestic, and sectoral greenhouse gas mitigation for US air quality and human health in 2050. Environ. Res. Lett. 2017, 12, 114033. [Google Scholar] [CrossRef]
- Cifuentes, L.; Borja-Aburto, V.H.; Gouveia, N.; Thurston, G.; Davis, D.L. Assessing the health benefits of urban air pollution reductions associated with climate change mitigation (2000-2020): Santiago, São Paulo, México City, and New York City. Environ. Health Perspect. 2001, 109, 419–425. [Google Scholar]
- Patz, J.A.; Lois, A.N.; Clifford, S.; Brossard, D.; Maibach, E. Medical Alert! Climate Change is Harming our Health in Wisconsin; University of Wisconsin-Madison: Madison, WI, USA, 2020. [Google Scholar]
- Kakkad, K.; Barzaga, M.L.; Wallenstein, S.; Azhar, G.S.; Sheffield, P.E. Neonates in Ahmedabad, India, during the 2010 heat wave: A climate change adaptation study. J. Environ. Public Health 2014, 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, C.J.; Salas, R.N.; Rublee, C.; Hill, K.; Bartlett, E.S.; Charlton, P.; Dyamond, C.; Fockele, C.; Harper, R.; Barot, S. Clinical implications of climate change on US emergency medicine: Challenges and opportunities. Ann. Emerg. Med. 2020, 76, 168–178. [Google Scholar] [CrossRef]
- Health Care without Harm Safe Haven in the Storm: Protecting Lives and Margins with Climate-Smart Health Care. Available online: https://noharm-uscanada.org/documents/safe-haven-storm-protecting-lives-and-margins-climate-smart-health-care (accessed on 25 January 2021).
- Case Studies | U.S. Climate Resilience Toolkit. Available online: https://toolkit.climate.gov/case-studies (accessed on 25 January 2021).
- Seltenrich, N. Safe from the Storm: Creating Climate-Resilient Health Care Facilities. Environ. Health Perspect. 2018, 126, 102001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocanour, C.S.; Allen, S.J.; Mazabob, J.; Sparks, J.W.; Fischer, C.P.; Romans, J.; Lally, K.P. Lessons Learned from the Evacuation of an Urban Teaching Hospital. Arch. Surg. 2002, 137, 1141–1145. [Google Scholar] [CrossRef] [Green Version]
- Department of Disaster Management, B.V.I. PEEBLES HOSPITAL SCORES AN “A” ON HOSPITAL SAFETY INDEX. Available online: https://www.bviddm.com/peebles-hospital-scores-an-a-on-hospital-safety-index-2/ (accessed on 25 January 2021).
- Hess, J.J.; Ranadive, N.; Boyer, C.; Aleksandrowicz, L.; Anenberg, S.C.; Aunan, K.; Belesova, K.; Bell, M.L.; Bickersteth, S.; Bowen, K. Guidelines for modeling and reporting health effects of climate change mitigation actions. Environ. Health Perspect. 2020, 128, 115001. [Google Scholar] [CrossRef]
- Bell, M.L.; Davis, D.L.; Cifuentes, L.A.; Krupnick, A.J.; Morgenstern, R.D.; Thurston, G.D. Ancillary human health benefits of improved air quality resulting from climate change mitigation. Environ. Heal. 2008, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, B.C.; Kriegler, E.; Riahi, K.; Ebi, K.L.; Hallegatte, S.; Carter, T.R.; Mathur, R.; van Vuuren, D.P. A new scenario framework for climate change research: The concept of shared socioeconomic pathways. Clim. Chang. 2014, 122, 387–400. [Google Scholar] [CrossRef] [Green Version]
- Sellers, S.; Ebi, K.L. Climate change and health under the shared socioeconomic pathway framework. Int. J. Environ. Res. Public Health 2018, 15, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, M.; Zuidema, C.; Bauman, B.; Burke, T.; Sheehan, M. Integrating public health into climate change policy and planning: State of practice update. Int. J. Environ. Res. Public Health 2019, 16, 3232. [Google Scholar] [CrossRef] [Green Version]
- Hess, J.J.; Mcdowell, J.Z.; Luber, G. Integrating Climate Change Adaptation into Public Health Practice: Using Adaptive Management to Increase Adaptive Capacity and Build Resilience. Environ. Health Perspect. 2012, 120, 171–179. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bikomeye, J.C.; Rublee, C.S.; Beyer, K.M.M. Positive Externalities of Climate Change Mitigation and Adaptation for Human Health: A Review and Conceptual Framework for Public Health Research. Int. J. Environ. Res. Public Health 2021, 18, 2481. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052481
Bikomeye JC, Rublee CS, Beyer KMM. Positive Externalities of Climate Change Mitigation and Adaptation for Human Health: A Review and Conceptual Framework for Public Health Research. International Journal of Environmental Research and Public Health. 2021; 18(5):2481. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052481
Chicago/Turabian StyleBikomeye, Jean C., Caitlin S. Rublee, and Kirsten M. M. Beyer. 2021. "Positive Externalities of Climate Change Mitigation and Adaptation for Human Health: A Review and Conceptual Framework for Public Health Research" International Journal of Environmental Research and Public Health 18, no. 5: 2481. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052481