
The Immediate and Long-Term Impact of Military Aircraft Noise on Hearing: A Cross-Sectional Comparison of Fighter Pilots and Ground Staff

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Recruitment of Participants
2.2. Ethical Considerations
2.3. Conventional Pure-Tone and Extended High-Frequency Audiometry
2.4. Otoacoustic Emissions
2.5. Noise Measurement and Analysis
2.6. Data Analysis
3. Results
3.1. Characteristics of Participants
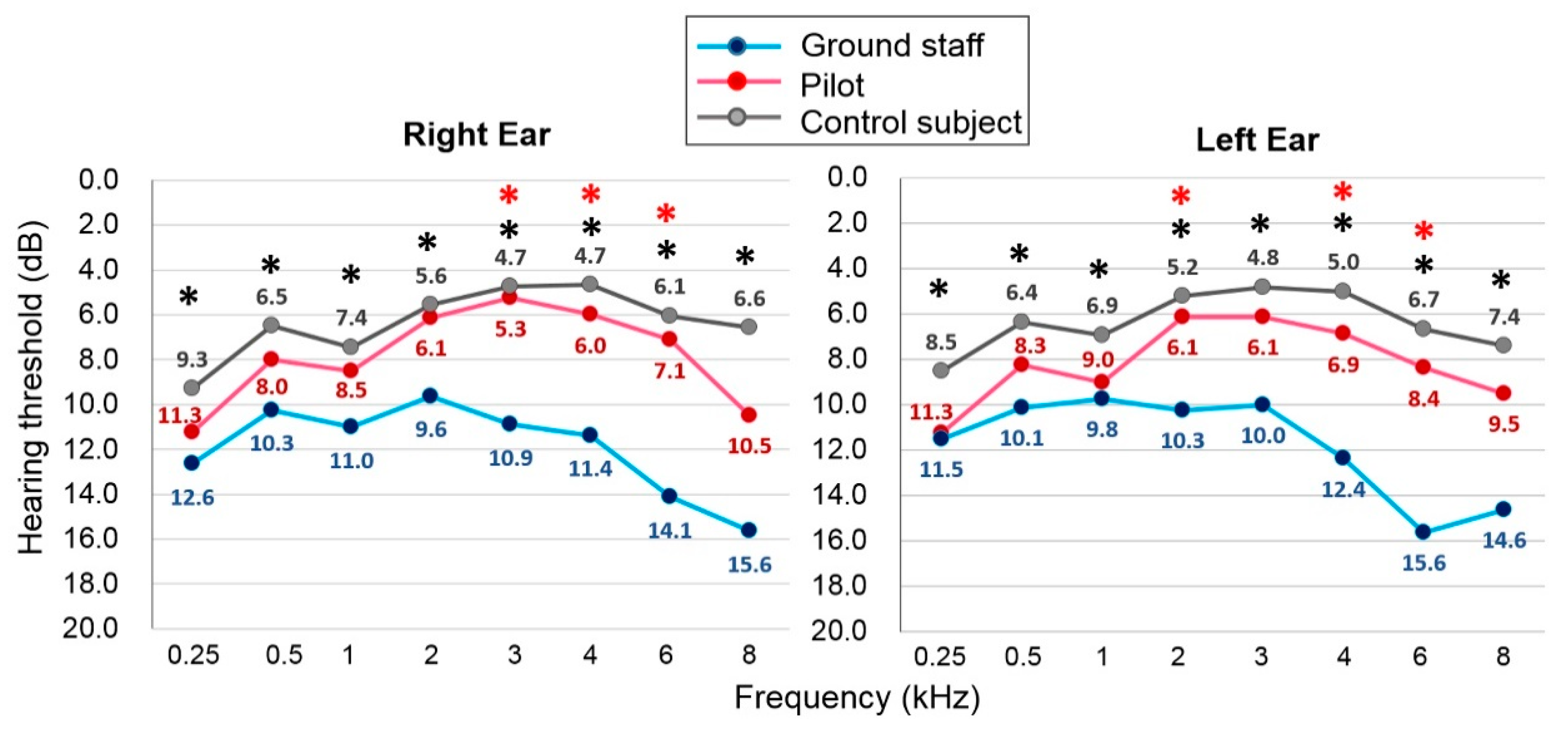
3.2. The Recent Hearing Thresholds Were Significantly Higher for Ground Staff Than for Fighter Pilots
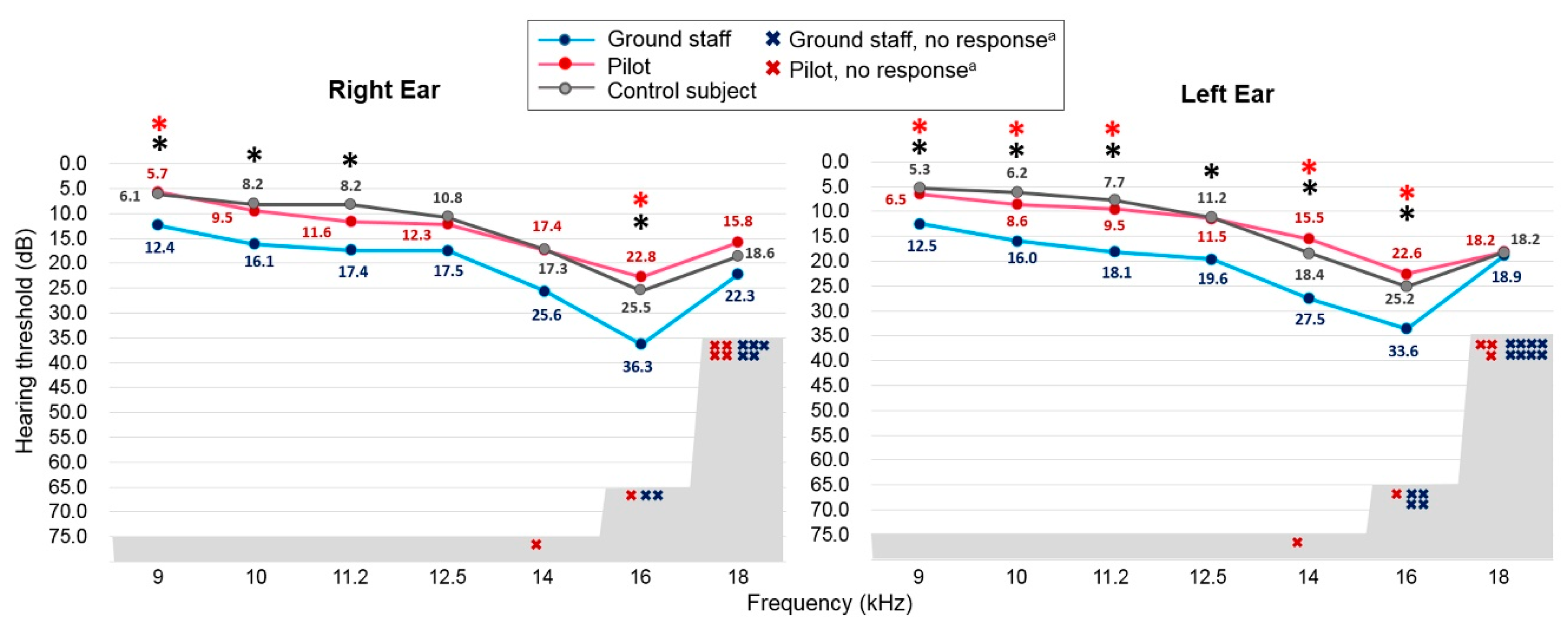
3.3. The EHF Audiometry Metric Showed a Statistically Significant Group Difference
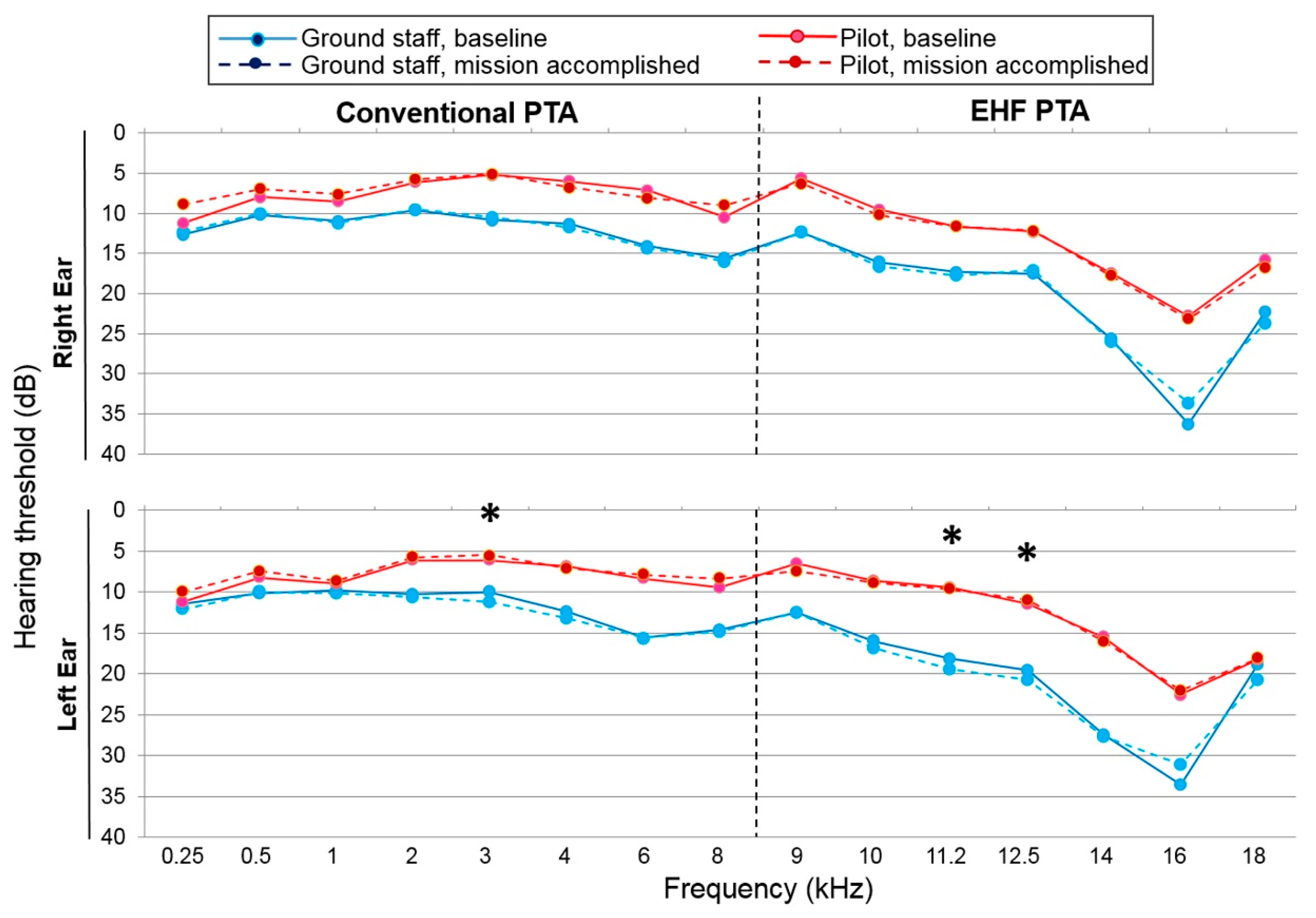
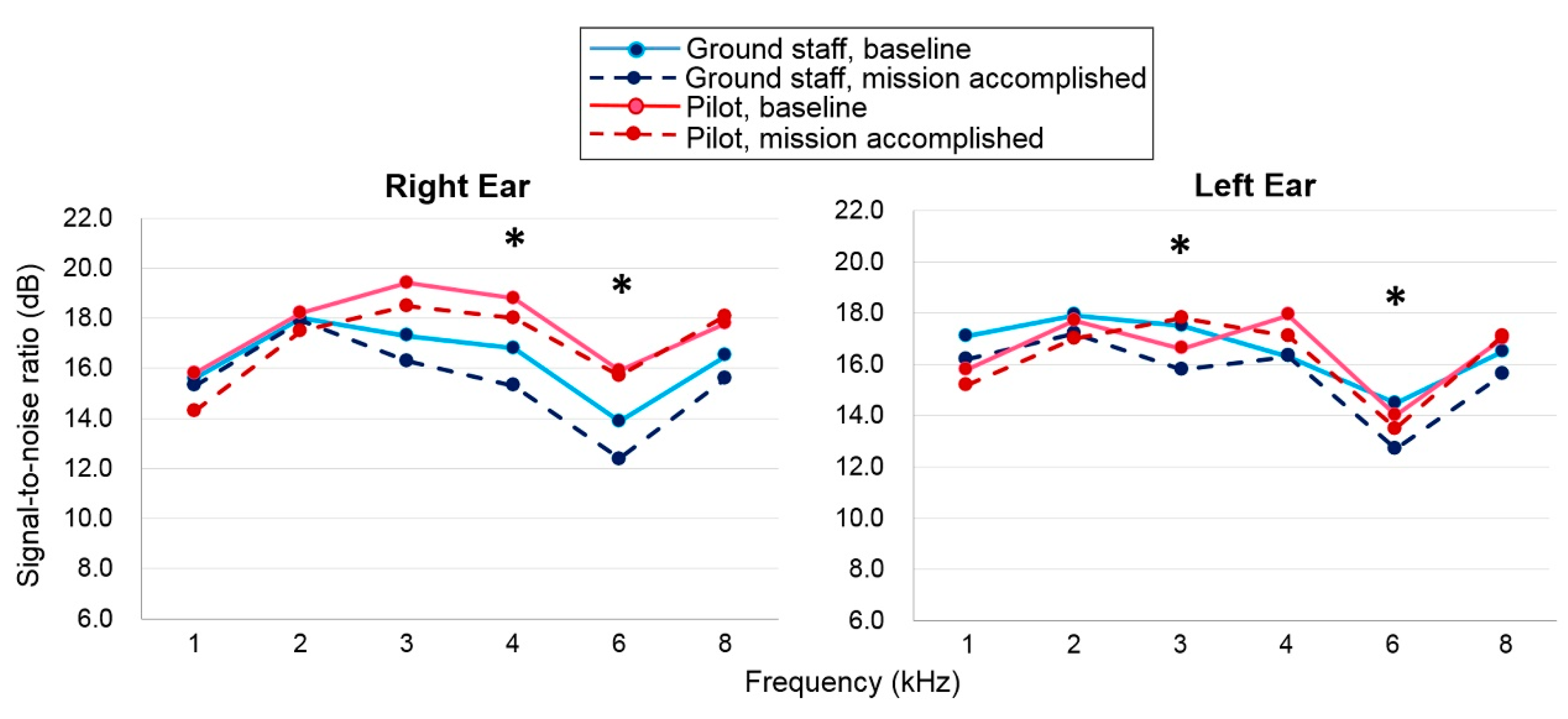
3.4. Immediate Noise Impact on Hearing after Accomplishing One Flight Mission
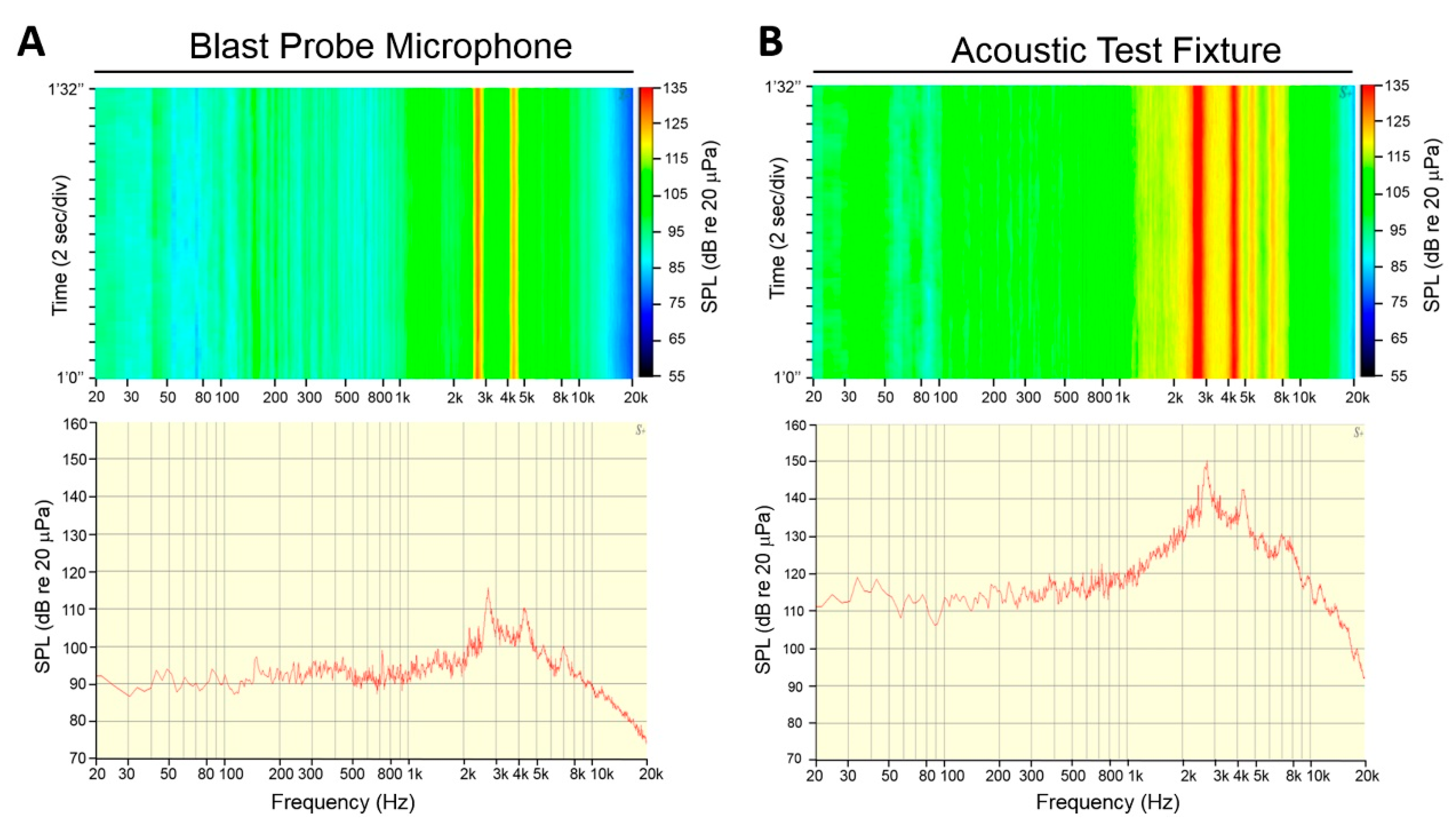
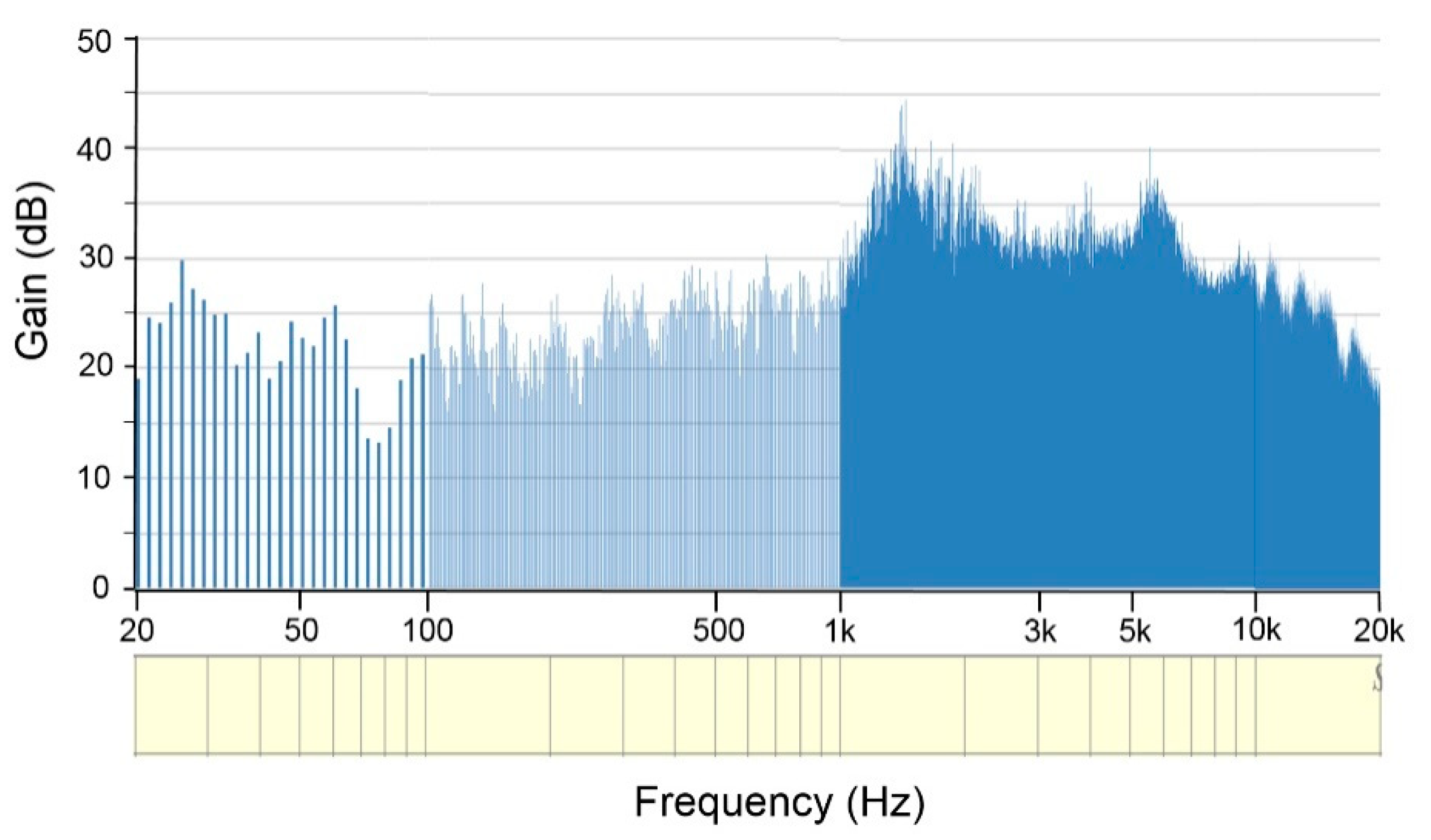
3.5. Analysis of the Noise Level in in the Hardened Aircraft Shelter
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yankaskas, K. Prelude: Noise-induced tinnitus and hearing loss in the military. Hear. Res. 2013, 295, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.S.; Griest, S.E.; Thielman, E.J.; Carlson, K.F.; Helt, W.J.; Lewis, M.S.; Blankenship, C.; Austin, D.; Theodoroff, S.M.; Henry, J.A. Audiologic characteristics in a sample of recently-separated military Veterans: The Noise Outcomes in Servicemembers Epidemiology Study (NOISE Study). Hear. Res. 2017, 349, 21–30. [Google Scholar] [CrossRef]
- Pourbakht, A.; Yamasoba, T. Cochlear damage caused by continuous and intermittent noise exposure. Hear. Res. 2003, 178, 70–78. [Google Scholar] [CrossRef]
- Dunn, D.E.; Davis, R.R.; Merry, C.J.; Franks, J.R. Hearing loss in the chinchilla from impact and continuous noise exposure. J. Acoust. Soc. Am. 1991, 90, 1979–1985. [Google Scholar] [CrossRef] [PubMed]
- Kemp, D.T. Stimulated acoustic emissions from within the human auditory system. J. Acoust. Soc. Am. 1978, 64, 1386–1391. [Google Scholar] [CrossRef]
- Kemp, D.T. Otoacoustic emissions, their origin in cochlear function, and use. Br. Med. Bull. 2002, 63, 223–241. [Google Scholar] [CrossRef]
- Kemp, D.T. Evidence of Mechanical Nonlinearity and frequency selective wave amplification in the cochlea. Arch. Otorhinolaryngol. 1979, 224, 37–45. [Google Scholar] [CrossRef]
- McGill, T.J.I.; Schuknecht, H.F. Human cochlear changes in noise induced hearing loss. Laryngoscope 1976, 86, 1293–1302. [Google Scholar] [CrossRef]
- Kapoor, N.; Mani, K.V.; Shukla, M. Distortion product oto-acoustic emission: A superior tool for hearing assessment than pure tone audiometry. Noise Health 2019, 21, 164–168. [Google Scholar]
- Sliwinska-Kowalska, M.; Kotylo, P. Otoacoustic emissions in industrial hearing loss assessment. Noise Health 2001, 3, 75–84. [Google Scholar]
- Baradarnfar, M.H.; Karamifar, K.; Mehrparvar, A.H.; Mollasadeghi, A.; Gharavi, M.; Karimi, G.; Vahidy, M.R.; Baradarnfar, A.; Mostaghaci, M. Amplitude changes in otoacoustic emissions after exposure to industrial noise. Noise Health 2012, 14, 28–31. [Google Scholar]
- Hofstetter, P.; Ding, D.; Powers, N.; Salvi, R.J. Quantitative relationship of carboplatin dose to magnitude of inner and outer hair cell loss and the reduction in distortion product otoacoustic emission amplitude in chinchillas. Hear. Res. 1997, 112, 199–215. [Google Scholar] [CrossRef]
- Job, A.; Raynal, M.; Kossowski, M.; Studler, M.; Ghernaouti, C.; Baffioni-Venturi, A.; Roux, A.; Darolles, C.; Guelorget, A. Otoacoustic detection of risk of early hearing loss in ears with normal audiograms: A 3-year follow-up study. Hear. Res. 2009, 251, 10–16. [Google Scholar] [CrossRef]
- Lapsley Miller, J.A.; Marshall, L.; Heller, L.M.; Hughes, L.M. Low-level otoacoustic emissions may predict susceptibility to noise-induced hearing loss. J. Acoust. Soc. Am. 2006, 120, 280–296. [Google Scholar] [CrossRef]
- Korres, G.S.; Balatsouras, D.G.; Tzagaroulakis, A.; Kandiloros, D.; Ferekidis, E. Extended high-frequency audiometry in subjects exposed to occupational noise. B-ENT 2008, 4, 147–155. [Google Scholar]
- Valiente, A.R.; Fidalgo, A.R.; Villarreal, I.M.; Berrocal, J.G. Extended high-frequency audiometry (9000-20000 Hz). Usefulness in audiological diagnosis. Acta Otorrhinolaryngol. Esp. 2016, 67, 40–44. [Google Scholar]
- Prendergast, G.; Hymers, M.; Lee, A. A quick and reliable estimate of extended high frequency hearing. Int. J. Audiol. 2020, 59, 823–827. [Google Scholar] [CrossRef]
- Somma, G.; Pietroiusti, A.; Magrini, A.; Coppeta, L.; Ancona, C.; Gardi, S.; Messina, M.; Bergamaschi, A. Extended high-frequency audiometry and noise induced hearing loss in cement workers. Am. J. Ind. Med. 2008, 51, 452–462. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, T.S.; Prieve, B.A. Detection of hearing loss using 2f2-f1 and 2f1-f2 distortion-product otoacoustic emissions. J. Speech Lang. Hear. Res. 2005, 48, 1165–1186. [Google Scholar] [CrossRef]
- Gorga, M.P.; Neely, S.T.; Ohlrich, B.; Hoover, B.; Redner, J.; Peters, J. From laboratory to clinic: A large scale study of distortion product otoacoustic emissions in ears with normal hearing and ears with hearing loss. Ear Hear. 1997, 18, 440–455. [Google Scholar] [CrossRef]
- Kampel-Furman, L.; Joachims, Z.; Bar-Cohen, H.; Grossman, A.; Frenkel-Nir, Y.; Shapira, Y.; Alon, E.; Carmon, E.; Gordon, B. Hearing threshold shifts among military pilots of the Israeli Air Force. J. R. Army Med. Corps 2018, 164, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Greenwell, B.M.; Tvaryanas, A.P.; Maupin, G.M. Risk Factors for Hearing Decrement Among U.S. Air Force Aviation-Related Personnel. Aerosp. Med. Hum. Perform. 2018, 89, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Cason, E.M. Air Force Hearing Conservation Program data 1998-2008: A cross-sectional analysis of positive threshold shifts. Mil. Med. 2012, 177, 589–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Prell, C.G.; Spankovich, C.; Lobariñas, E.; Griffiths, S.K. Extended high-frequency thresholds in college students: Effects of music player use and other recreational noise. J. Am. Acad. Audiol. 2013, 24, 725–739. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.O.; Dennis, J.H.; Badran, O.; Ismail, M.; Ballal, S.G.; Ashoor, A.; Jerwood, D. High-frequency (10–18 kHz) hearing thresholds: Reliability, and effects of age and occupational noise exposure. Occup. Med. 2001, 51, 245–258. [Google Scholar] [CrossRef] [Green Version]
- Marshall, L.; Miller, J.A.L.; Heller, L.M.; Wolgemuth, K.S.; Hughes, L.M.; Smith, S.D.; Kopke, R.D. Detecting incipient inner-ear damage from impulse noise with otoacoustic emissions. J. Acoust. Soc. Am. 2008, 125, 995–1013. [Google Scholar] [CrossRef] [Green Version]
- Konopka, W.; Pawlaczyk-Luszczynska, M.; Sliwinska-Kowalska, M.; Grzanka, A.; Zalewski, P. Effects of impulse noise on transiently evoked. Int. J. Audiol. 2005, 44, 3–7. [Google Scholar] [CrossRef]
- Mehrparvar, A.H.; Mirmohammadi, S.J.; Davari, M.H.; Mostaghaci, M.; Mollasadeghi, A.; Bahaloo, M.; Hashemi, S.H. Conventional Audiometry, Extended High-Frequency Audiometry, and DPOAE for Early Diagnosis of NIHL. Iran. Red Crescent Med. J. 2014, 16, e9628. [Google Scholar] [CrossRef]
- Anino, J.O.; Afullo, A.; Otieno, F. Occupational noise-induced hearing loss among workers at Jomo Kenyatta Internation airport, Nairobi. East Afr. Med. J. 2010, 87, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Mostafaee, M.; Nassiri, P.; Behzadi, M.H. Investigation of noise pollution in ground safety section of Mehrabad airport and its relation with employees hearing loss. Saf. Health Work 2015, 5, 23–34. [Google Scholar]
- Jaruchinda, P.; Thongdeetae, T.; Panichkul, S.; Hanchumpol, P. Prevalence and an analysis of noise--induced hearing loss in army helicopter pilots and aircraft mechanics. J. Med. Assoc. Thai. 2005, 88 (Suppl. 3), S232–S239. [Google Scholar] [PubMed]
- Rovig, G.W.; Bohnker, B.K.; Page, J.C. Hearing health risk in a population of aircraft carrier flight deck personnel. Mil. Med. 2004, 169, 429–432. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Rong, X.; Wang, Z.; Lin, A. Association between Smoking and Noise-Induced Hearing Loss: A Meta-Analysis of Observational Studies. Int. J. Environ. Res. Public Health 2020, 17, 1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Shi, Z.; Zhou, L.; Hu, Y.; Zhang, M. Occupational noise-induced hearing loss in China: A systematic review and meta-analysis. BMJ Open 2020, 10, e039576. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.R.; Lilly, D.J. Hearing loss from acute carbon monoxide intoxication. Ann. Otol. Rhinol. Laryngol. 1977, 86, 323–328. [Google Scholar] [CrossRef]
- Shahbaz Hassan, M.; Ray, J.; Wilson, F. Carbon monoxide poisoning and sensorineural hearing loss. J. Laryngol. Otol. 2003, 117, 134–137. [Google Scholar] [CrossRef]
- Shupak, A.; Tal, D.; Sharoni, Z.; Oren, M.; Ravid, A.; Pratt, H. Otoacoustic emissions in early noise-induced hearing loss. Otol. Neurotol. 2007, 28, 745–752. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Subject (n = 136) | Ground Staff (n = 40) | Fighter Pilot (n = 40) | p-Value | |
|---|---|---|---|---|
| Sex | <0.002 ** | |||
| Male (%) | 130 (95.6) | 31 (77.5) | 35 (87.5) | |
| Female (%) | 6 (4.4) | 9 (22.5) | 5 (12.5) | |
| Age (Mean ± SD) | 31.6 ± 5.2 | 31.5 ± 7.5 | 29.2 ± 4.6 | 0.051 |
| Wearing HPD | 0.806 a 0.675 b | |||
| Yes (%) | 125 (91.9) | 38 (95.0) | 36 (92.3) | |
| No (%) | 11 (8.1) | 2 (5.0) | 3 (7.7) |
| Grouped Frequencies (kHz) | Right Ear | Left Ear | ||||
|---|---|---|---|---|---|---|
| Ground Staff | Fighter Pilot | p-Value | Ground Staff | Fighter Pilot | p-Value | |
| Mean ± SEM | Mean ± SEM | Mean ± SEM | Mean ± SEM | |||
| 3FPTA (0.5, 1, 2) | 10.29 ± 1.30 | 7.54 ± 0.90 | 0.086 | 10.04 ± 2.38 | 7.96 ± 1.42 | 0.159 |
| 4FPTA (0.5, 1, 2, 4) | 10.56 ± 1.35 | 7.16 ± 0.89 | 0.038 * | 11.00 ± 1.47 | 7.25 ± 0.92 | 0.034 * |
| HFPTA (4, 6, 8) | 13.71 ± 2.25 | 7.88 ± 1.18 | 0.025 * | 14.21 ± 2.43 | 8.25 ± 1.06 | 0.029 * |
| OFPTA (0.5, 1, 2, 3, 4, 6, 8) | 11.94 ± 1.60 | 7.85 ± 0.93 | 0.030 * | 11.78 ± 1.64 | 8.19 ± 0.89 | 0.055 |
| EHFPTA (9, 10, 11.2, 12.5, 14, 16, 18) | 19.36 ± 2.73 | 12.95 ± 1.83 | 0.056 | 17.84 ± 2.61 | 12.47 ± 1.49 | 0.079 |
| Frequency (kHz) | Right Ear | Left Ear | ||||
|---|---|---|---|---|---|---|
| Ground Staff | Fighter Pilot | p-Value | Ground Staff | Fighter Pilot | p-Value | |
| n (%) | n (%) | n (%) | n (%) | |||
| 14 | 0 (0.0) | 1 (2.5) | 1.000 a | 0 (0.0) | 1 (2.5) | 1.000 a |
| 16 | 2 (5.0) | 1 (2.5) | 1.000 a | 4 (10.0) | 1 (2.5) | 0.359 a |
| 18 | 5 (12.5) | 4 (10.0) | 1.000 a | 8 (20.0) | 3 (7.5) | 0.105 |
| 9–18 | 5 (12.5) | 4 (10.0) | 1.000 a | 9 (22.5) | 3 (7.5) | 0.060 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, C.-Y.; Hung, C.-L.; Chen, H.-C.; Shih, C.-P.; Lu, R.-H.; Chen, C.-W.; Hung, L.-W.; Lin, Y.-C.; Chen, H.-K.; Chu, D.-M.; et al. The Immediate and Long-Term Impact of Military Aircraft Noise on Hearing: A Cross-Sectional Comparison of Fighter Pilots and Ground Staff. Int. J. Environ. Res. Public Health 2021, 18, 2982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062982
Kuo C-Y, Hung C-L, Chen H-C, Shih C-P, Lu R-H, Chen C-W, Hung L-W, Lin Y-C, Chen H-K, Chu D-M, et al. The Immediate and Long-Term Impact of Military Aircraft Noise on Hearing: A Cross-Sectional Comparison of Fighter Pilots and Ground Staff. International Journal of Environmental Research and Public Health. 2021; 18(6):2982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062982
Chicago/Turabian StyleKuo, Chao-Yin, Chia-Lien Hung, Hsin-Chien Chen, Cheng-Ping Shih, Rou-Huei Lu, Chen-Wai Chen, Li-Wen Hung, Yi-Chun Lin, Hang-Kang Chen, Da-Ming Chu, and et al. 2021. "The Immediate and Long-Term Impact of Military Aircraft Noise on Hearing: A Cross-Sectional Comparison of Fighter Pilots and Ground Staff" International Journal of Environmental Research and Public Health 18, no. 6: 2982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062982