
Time in Nature Associated with Decreased Fatigue in UK Truck Drivers

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
1.1. Health Problems Associated with Long-Distance Driving
1.2. Health Benefits of Exposure to Nature
2. Materials and Methods
2.1. Study Design, Setting and Participants
2.2. Online Questionnaire
2.3. Baseline Measurements
2.4. Statistical Analysis
3. Results
3.1. Pre-Covid-19 Outbreak (February–July 2019)
3.2. During the Covid-19 Outbreak (May–July 2020)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guest, A.; Chen, Y.; Pearson, N.; King, J.; Paine, N.; Clemes, S. Cardiometabolic risk factors and mental health status among truck drivers: A systematic review. BMJ Open 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Fink, G. Stress: The Health Epidemic of the 21st Century. 2016. Available online: http://0-scitechconnect-elsevier-com.brum.beds.ac.uk/stress-health-epidemic-21st-century/ (accessed on 28 January 2021).
- Mental Health Foundation. Stress: Are We Coping? 2018. Available online: https://www.mentalhealth.org.uk/publications/stress-are-we-coping (accessed on 28 January 2021).
- Guterres, A. UN Leads Call to Protect Most Vulnerable from Mental Health Crisis during and after COVID-19. Available online: https://news.un.org/en/story/2020/05/1063882 (accessed on 28 January 2021).
- Ader, R.; Cohen, N.; Felten, D. Psychoneuroimmunology: Interactions between the nervous system and the immune system. Lancet 1995, 345, 99–103. [Google Scholar] [CrossRef]
- Cardinali, D. Autonomic Nervous System: Basic and Clinical Aspects; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Vinik, A.; Maser, R.; Ziegler, D. Autonomic imbalance: Prophet of doom or scope for hope? Diabet. Med. 2011, 28, 643–651. [Google Scholar] [CrossRef]
- American Psychological Association. Stress Effects on the Body. Available online: https://www.apa.org/topics/stress/body (accessed on 28 January 2021).
- Lucassen, P.; Pruessner, J.; Sousa, N.; Almeida, O.; Van Dam, A.M.; Rajkowska, G.; Swaab, D.; Czéh, B. Neuropathology of stress. Acta Neuropathol. 2014, 127, 109–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blix, E.; Perski, A.; Berglund, H.; Savic, I. Long-term occupational stress is associated with regional reductions in brain tissue volumes. PLoS ONE 2013, 8, e64065. [Google Scholar] [CrossRef] [Green Version]
- Laugsand, L.; Strand, L.; Platou, C.; Vatten, L.; Janszky, I. Insomnia and the risk of incident heart failure: A population study. Eur. Hear. J. 2014, 35, 1382–1393. [Google Scholar] [CrossRef] [Green Version]
- Vyas, M.; Garg, A.; Iansavichus, A.; Costella, J.; Donner, A.; Laugsand, L. Shift work and vascular events: Systematic review and meta-analysis. Br. Med. J. 2012, 345, e4800. [Google Scholar] [CrossRef] [Green Version]
- Rapsomaniki, E.; Timmis, A.; George, J.; Pujades-Rodriguez, M.; Shah, A.; Denaxas, S.; White, I.; Caulfield, M.; Deanfield, J.; Smeeth, L.; et al. Blood pressure and incidence of twelve cardiovascular diseases: Lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people. Lancet 2014, 383, 1899–1911. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Cai, X.; Zhang, J.; Mai, W.; Wang, S.; Hu, Y.; Ren, H.; Xu, D. Prehypertension and Incidence of ESRD: A systematic review and meta-analysis. Am. J. Kidney Dis. 2014, 63, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Resch, M. The psychological factors affecting athletic performance. Orv. Hetil. 2010, 151, 815–821. [Google Scholar] [CrossRef]
- Stults-Kolehmainen, M.; Bartholomew, J. Psychological stress impairs short-term muscular recovery from resistance exercise. Med. Sci. Sport. Exerc. 2012, 44, 2220–2227. [Google Scholar] [CrossRef] [PubMed]
- Rastgoo, M.; Nakisa, B.; Rakotonirainy, A.; Chandran, V.; Tjondronegoro, D. A critical review of proactive detection of driver stress levels based on multimodal measurements. ACM Comput. Surv. 2018, 51, 1–35. [Google Scholar] [CrossRef] [Green Version]
- Hege, A.; Lemke, M.; Apostolopoulos, Y.; Sönmez, S. Occupational health disparities among U.S. Long-haul truck drivers: The influence of work organization and sleep on cardiovascular and metabolic disease risk. PLoS ONE 2018, 13, e0207322. [Google Scholar] [CrossRef] [Green Version]
- Meijman, T.; Schaufeli, W. Psychishe vermoeidheid en arbeid: Ontwikkelingen in de A & O psychologie. Fatigue at work: Developments inI&O psychology. Psycholoog 1996, 31, 236–241. [Google Scholar]
- Thorsteinsson, E.; Brown, R. Mediators and moderators of the stressor–fatigue relationship in nonclinical samples. J. Psychosom. Res. 2009, 66, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Åkerstedt, T.; Axelsson, J.; Lekander, M.; Orsini, N.; Kecklund, G. Do sleep, stress, and illness explain daily variations in fatigue? A prospective study. J. Psychosom. Res. 2014, 76, 280–285. [Google Scholar] [CrossRef]
- Doerr, J.; Ditzen, B.; Strahler, J.; Linnemann, A.; Ziemek, J.; Skoluda, N.; Hoppmann, C.; Nater, U. Reciprocal relationship between acute stress and acute fatigue in everyday life in a sample of university students. Biol. Psychol. 2015, 110, 42–49. [Google Scholar] [CrossRef]
- Dinges, D.; Maislin, G. Truck Driver Fatigue Management Survey; Federal Motor Carrier Safety Administration, US Department of Transportation, Report No. FMCSA-RRR-06-008; 2006. Available online: https://www.fmcsa.dot.gov/sites/fmcsa.dot.gov/files/docs/Dinges_D_F_Maislin_G___Truck_Driver_Fatigue_Management_Survey__2006.pdf (accessed on 28 January 2021).
- Lemke, M.; Hege, A.; Apostolopoulos, Y.; Wideman, L.; Sönmez, S. Work and sleep among transport operators: Disparities and implications for safety. J. Transp. Health 2017, 7, 298–309. [Google Scholar] [CrossRef]
- Kaplan, S.; Prato, C. Associating crash avoidance maneuvers with driver attributes and accident characteristics: A mixed logit model approach. Traffic Inj. Prev. 2012, 13, 315–326. [Google Scholar] [CrossRef]
- Moore, B.; Brooks, C. Heavy vehicle driver fatigue: A policy advisers’ perspective. In Proceedings of the 4th International Conference on Fatigue and Transportation, Fremantle, Australia, 6 March 2000. [Google Scholar]
- Haworth, N. Fatigue and fatigue research: The Australian experience. Accid. Res. Centre Monash Univ. 1998, 1–13. Available online: http://158.132.155.107/posh97/private/research/papers/fatigue.pdf (accessed on 28 January 2021).
- Jones, I.; Stein, H. Effect of Driver Hours of Service on Tractor-Trailer Crash Involvement; Insurance Institute for Highway Safety: Washington, DC, USA, 1987. [Google Scholar]
- Jackson, P.; Hilditch, C.; Holmes, A.; Reed, N.; Merat, N.; Smith, L. Fatigue and Road Safety: A Critical Analysis of Recent Evidence; Department for Transport, Road Safety Web Publication; 2011; Volume 21. Available online: https://webarchive.nationalarchives.gov.uk/20121103213009/http://www.dft.gov.uk/publications/rsrr-theme3-fatigue-road-safety-analysis/ (accessed on 28 January 2021).
- Lock, A.; Bonetti, D.; Campbell, A. The psychological and physiological health effects of fatigue. Occup. Med. 2018, 68, 502–511. [Google Scholar] [CrossRef]
- Knutson, K. Sleep duration and cardiometabolic risk: A review of the epidemiologic evidence. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 731–743. [Google Scholar] [CrossRef] [Green Version]
- Black, P. The inflammatory response is an integral part of the stress response: Implications for atherosclerosis, insulin resistance, type II diabetes and metabolic syndrome X. Brain. Behav. Immun. 2003, 17, 350–364. [Google Scholar] [CrossRef]
- Ayas, N.; White, D.; Manson, J.; Stampfer, M.; Speizer, F.; Malhotra, A. A prospective study of sleep duration and coronary heart disease in women. Arch. Intern. Med. 2003, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ji, A.; Zhu, Y.; Liang, Z.; Wu, J.; Li, S. A meta- analysis including dose-response relationship between night shift work and the risk of colorectal cancer. Oncotarget 2015, 6, 25046–25060. [Google Scholar] [CrossRef] [Green Version]
- Cappuccio, F.; D’Elia, L.; Strazzullo, P.; Miller, M. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef]
- Garbarino, S.; Guglielmi, O.; Sannita, W.; Magnavita, N.; Lanteri, P. Sleep and mental health in truck drivers: Descriptive review of the current evidence and proposal of strategies for primary prevention. Int. J. Environ. Res. Public Health 2018, 15, 1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deale, A.; Wessely, S. Diagnosis of psychiatric disorder in clinical evaluation of chronic fatigue syndrome. J. R. Soc. Med. 2000, 93, 310–312. [Google Scholar] [CrossRef] [Green Version]
- Roy-Byrne, P.; Afari, N.; Ashton, S.; Fischer, M.; Goldberg, J.; Buchwald, D. Chronic fatigue and anxiety/depression: A twin study. Br. J. Psychiatry 2002, 180, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Manu, P.; Lane, T.; Matthews, D. The frequency of the chronic fatigue syndrome in patients with symptoms of persistent fatigue. Ann. Intern. Med. 1988, 109, 554–556. [Google Scholar] [CrossRef] [PubMed]
- Apostolopoulos, Y.; Sönmez, S.; Shattell, M.; Belzer, M. Worksite-induced morbidities among truck drivers in the United States. AAOHN J. Off. J. Am. Assoc. Occup. Health Nurses 2010, 58, 285–296. [Google Scholar]
- Sieber, W.; Robinson, C.; Birdsey, J.; Chen, G.; Hitchcock, E.; Lincoln, J.; Nakata, A.; Sweeney, M. Obesity and other risk factors: The National Survey of U.S. Long-Haul Truck Driver Health and Injury. Am. J. Ind. Med. 2014, 57, 615–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, B.; Church, T.; Bonnell, R.; Ben-Joseph, R.; Borgstadt, T. The impact of overweight and obesity on the direct medical costs of truck drivers. J. Occup. Environ. Med. 2009, 51, 180–184. [Google Scholar] [CrossRef]
- Bigert, C.; Gustavsson, P.; Hallqvist, J.; Hogstedt, C.; Lewné, M.; Plato, N.; Reuterwall, C.; Schéele, P. Myocardial infarction among professional drivers. Epidemiology 2003, 14, 333–339. [Google Scholar] [CrossRef]
- Craig, R.; Mindell, J.; Hirani, V. Health Survey for England—2013. Health and Social Care Information Centre. 2014. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/health-survey-for-england-2013 (accessed on 28 January 2021).
- Penninx, B.; Milaneschi, Y.; Lamers, F.; Vogelzangs, N. Understanding the somatic consequences of depression: Biological mechanisms and the role of depression symptom profile. BMC Med. 2013, 11, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Saltzman, G.; Belzer, M. Truck Driver Occupational Safety and Health. In Proceedings of the 2003 Conference Report and Selective Literature Review, Cincinnati, OH, USA, 8 February 2007; Available online: https://www.cdc.gov/niosh/docs/2007-120/pdfs/2007-120.pdf?id=10.26616/NIOSHPUB2007120 (accessed on 28 January 2021).
- Frumkin, H.; Bratman, G.; Breslow, S.; Cochran, B.; Kahn, P.; Lawler, J.; Levin, P.; Tandon, P.; Varanasi, U.; Wolf, K.; et al. Nature contact and human health: A research agenda. Environ. Health Perspect. 2017, 125, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, M.; Jones, R.; Tocchini, K. Shinrin-yoku (Forest bathing) and nature therapy: A state-of-the-art review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratman, G.; Anderson, C.; Berman, M.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.; Hartig, T.; et al. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, H.; Song, C.; Ikei, H.; Park, B.; Kagawa, T.; Miyazaki, Y. Combined Effect of Walking and Forest Environment on Salivary Cortisol Concentration. Front. Public Health 2019, 7, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Park, B.; Tsunetsugu, Y.; Lee, J.; Kagawa, T.; Miyazaki, Y. Effect of the forest environment on physiological relaxation-the results of field tests at 35 sites throughout Japan. In Forest Medicine; Li, Q., Ed.; Nova Science Publishers: New York, NY, USA, 2012; pp. 55–65. [Google Scholar]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid. Based Complement. Altern. Med. 2014, 2014. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Berto, R. Exposure to restorative environments helps restore attentional capacity. J. Environ. Psychol. 2005, 25, 249–259. [Google Scholar] [CrossRef]
- Joye, Y.; Dewitte, S. Nature’s broken path to restoration. A critical look at Attention Restoration Theory. J. Environ. Psychol. 2018, 59, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Berman, M.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef]
- Varela-Mato, V.; Caddick, N.; King, J.; Yates, T.; Stensel, D.; Nimmo, M.; Clemes, S. A Structured Health Intervention for Truckers (SHIFT). J. Occup. Environ. Med. 2018, 60, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clemes, S.; Mato, V.; Munir, F.; Chen, L.; Hamer, M.; Gray, L.; Edwardson, C.; Jaicim, N.; Richardson, G.; Johnson, V.; et al. Cluster randomised controlled trial to investigate the effectiveness and cost—Effectiveness of a Structured Health Intervention For Truckers (the SHIFT study): A study protocol. BMJ Open 2019, 9, E030175. [Google Scholar]
- Zigmond, A.; Snaith, R. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Bjelland, I.; Dahl, A.; Haug, T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Winwood, P.; Lushington, K.; Winefield, A. Further development and validation of the Occupational Fatigue Exhaustion Recovery (OFER) scale. J. Occup. Environ. Med. 2006, 48, 381–389. [Google Scholar] [CrossRef]
- Winwood, P.; Winefield, A.; Dawson, D.; Lushington, K. Development and validation of a scale to measure work-related fatigue and recovery: The Occupational Fatigue Exhaustion/Recovery Scale (OFER). J. Occup. Environ. Med. 2005, 47, 594–606. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Grant, P.; Tigbe, W.; Granat, M. The validity and reliability of a novel activity monitor as a measure of walking. Br. J. Sports Med. 2006, 40, 779–784. [Google Scholar] [CrossRef] [Green Version]
- Varela Mato, V.; Yates, T.; Stensel, D.; Biddle, S.; Clemes, S. Concurrent validity of actigraph-determined sedentary time against the activpal under free-living conditions in a sample of bus drivers. Meas. Phys. Educ. Exerc. Sci. 2017, 21, 212–222. [Google Scholar] [CrossRef]
- Winkler, E.; Bodicoat, D.; Healy, G.; Bakrania, K.; Yates, T.; Owen, N.; Dunstan, D.; Edwardson, C. Identifying adults’ valid waking wear time by automated estimation in activPAL data collected with a 24 h wear protocol. Physiol. Meas. 2016, 37, 1653. [Google Scholar] [CrossRef] [Green Version]
- Migueles, J.; Rowlands, A.; Huber, F.; Sabia, S.; van Hees, V. GGIR: A Research Community—Driven Open Source R Package for Generating Physical Activity and Sleep Outcomes From Multi-Day Raw Accelerometer Data. J. Meas. Phys. Behav. 2019, 2, 188–196. [Google Scholar] [CrossRef] [Green Version]
- van Hees, V.; Sabia, S.; Jones, S.; Wood, A.; Anderson, K.; Kivimäki, N.; Frayling, T.; Pack, A.; Bucan, M.; Trenell, M.; et al. Estimating sleep parameters using an accelerometer without sleep diary. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, V.; Sabia, S.; Anderson, K.; Denton, S.; Oliver, J.; Catt, M.; Abell, J.; Kivimäki, M.; Trenell, M.; Singh-Manoux, A. A novel, open access method to assess sleep duration using a wrist-worn accelerometer. PLoS ONE 2015, 10, e0142533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Transportation Research and Marketing. A Report on the Determination and Evaluation of the Role of Fatigue in Heavy Truck Accidents; Prepared for the AAA Foundation for Traffic Safety in cooperation with the Commercial Vehicle Safety Alliance; AAA Foundation for Traffic Safety: Falls Church, VA, USA, 1985. [Google Scholar]
- Basu, N.; Yang, X.; Luben, R.; Whibley, D.; Macfarlane, G.; Wareham, N.; Khaw, K.; Myint, P. Fatigue is associated with excess mortality in the general population: Results from the EPIC-Norfolk study. BMC Med. 2016, 14, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lifestyles Team, NHS Digital. Health Survey for England 2019. Health and Social Care Information Centre. 2020. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2019 (accessed on 18 February 2021).
- Ng, M.; Yousuf, B.; Bigelow, P.; Van Eerd, D. Effectiveness of health promotion programmes for truck drivers: A systematic review. Health Educ. J. 2015, 74, 270–286. [Google Scholar] [CrossRef]
- Cullen, W.; Kearney, Y.; Bury, G. Prevalence of fatigue in general practice. Ir. J. Med. Sci. 2002, 171, 10–12. [Google Scholar] [CrossRef]
- Cathebras, P.; Robbins, J.; Kirmayer, L.; Hayton, B. Fatigue in primary care: Prevalence, psychiatric comorbidity, illness behavior, and outcome. J. Gen. Intern. Med. 1992, 7, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Galland-Decker, C.; Marques-Vidal, P.; Vollenweider, P. Prevalence and factors associated with fatigue in the Lausanne middle-aged population: A population-based, cross-sectional survey. BMJ Open 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loge, J.; Ekeberg, O.; Kaasa, S. Fatigue in the general Norwegian population: Normative data and associations. J. Psychosom. Res. 1998, 45, 53–65. [Google Scholar] [CrossRef]
- Bültmann, U.; Kant, I.; Kasl, S.; Beurskens, A.; van den Brandt, P. Fatigue and psychological distress in the working population: Psychometrics, prevalence, and correlates. J. Psychosom. Res. 2002, 52, 445–452. [Google Scholar] [CrossRef] [Green Version]
- Pawlikowska, T.; Chalder, T.; Hirsch, S.; Wallace, P.; Wright, D.; Wessely, S. Population based study of fatigue and psychological distress. BMJ 1994, 308, 763–766. [Google Scholar] [CrossRef] [Green Version]
- Lerdal, A.; Wahl, A.; Rustøen, T.; Hanestad, B.; Moum, T. Fatigue in the general population: A translation and test of the psychometric properties of the Norwegian version of the fatigue severity scale. Scand. J. Public Health 2005, 33, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Eldevik, M.; Flo, E.; Moen, B.; Pallesen, S.; Bjorvatn, B. Insomnia, excessive sleepiness, excessive fatigue, anxiety, depression and shift work disorder in nurses having less than 11 hours in-between shifts. PLoS ONE 2013, 8, e70882. [Google Scholar] [CrossRef]
- Shen, J.; Botly, L.; Chung, S.; Gibbs, A.; Sabanadzovic, S.; Shapiro, C. Fatigue and shift work. J. Sleep Res. 2006, 15, 1–5. [Google Scholar] [CrossRef]
- Dorrian, J.; Baulk, S.; Dawson, D. Work hours, workload, sleep and fatigue in australian rail industry employees. Appl. Erg. 2011, 42, 202–209. [Google Scholar] [CrossRef]
- Costa, G. Shift work and occupational medicine: An overview. Occup. Med. 2003, 53, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Patterson, P.; Runyon, M.; Higgins, J.; Weaver, M.; Teasley, E.; Kroemer, A.; Martin-Gill, C. Shorter versus longer shift durations to mitigate fatigue and fatigue-related risks in emergency medical services personnel and related shift workers: A systematic review. Prehospital Emerg. 2018, 22, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Taylor, Y.; Merat, N.; Jamson, S. The effects of fatigue on cognitive performance in police officers and staff during a forward rotating shift pattern. Saf. Health Work 2019, 10, 67–74. [Google Scholar] [CrossRef]
- Wong, F.; Chiang, Y.; Abidoye, F.; Liang, S. Interrelation between human factor–related accidents and work patterns in construction industry. J. Constr. Eng. Manag. 2019, 145, 04019021. [Google Scholar] [CrossRef]
- Miyazaki, Y. Shinrin Yoku: The Japanese Art of Forest Bathing; Timber Press: Portland, OR, USA, 2018. [Google Scholar]
- Tapaninen, M.; Kajala, L.; Erkkonen, J.; Aarnio, M. Healthy Parks, Healthy People. In Proceedings of the 6th International Conference on Monitoring and Management of Visitors in Recreational and Protected Areas: Outdoor Recreation in Change—Current Knowledge and Future Challenges, MMV 6-Proceedings, Stockholm, Sweden, 21–24 August 2012; Available online: https://www.iucn.org/sites/dev/files/content/documents/healthy_parks_finland.pdf (accessed on 28 January 2021).
- Robinson, J.; Jorgensen, A.; Cameron, R.; Brindley, P. Let Nature Be Thy Medicine: A Socioecological Exploration of Green Prescribing in the UK. Int. J. Environ. Res. Public Health 2020, 17, 3460. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological effects of visual stimulation with forest imagery. Int. J. Environ. Res. Public Health 2018, 15, 213. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, R.; Simons, R.; Losito, B.; Fiorito, E.; Miles, M.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Kawada, T. Effect of forest environments on human natural killer (NK) activity. Int. J. Immunopathol. Pharmacol. 2011, 24, 39S–44S. [Google Scholar]
- Sakuragawa, S.; Kaneko, T.; Miyazaki, Y. Effects of contact with wood on blood pressure and subjective evaluation. J. Wood Sci. 2008, 54, 107–113. [Google Scholar] [CrossRef]
- White, M.; Alcock, I.; Grellier, J.; Wheeler, B.; Hartig, T.; Warber, S.; Bone, A.; Depledge, M.; Fleming, L. Spending at least 120 minutes a week in nature is associated with good health and wellbeing. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Sabbagh-Ehrlich, S.; Friedman, L.; Richter, E. Working conditions and fatigue in professional truck drivers at Israeli ports. Inj. Prev. 2005, 11, 110–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Freight Transport Association. Logistics Report. 2019. Available online: https://www.santandercb.co.uk/factsheet/fta-logistics-report-2019.pdf (accessed on 18 February 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | n | Mean (SD) |
|---|---|---|
| Age (y) | 89 | 49.9 (8.9) |
| Height (cm) | 88 | 178.6 (6.7) |
| Weight (kg) | 88 | 94.9 (14.6) |
| BMI (kgm−2) | 88 | 29.9 (4.7) |
| Working hours per week | 89 | 46.6 (8.4) |
| Years as HGV driver | 89 | 18.3 (10.6) |
| Do You Spend Time in Nature at Least Once a Week? | Comparison of Nature vs. No Nature | |||
|---|---|---|---|---|
| Yes (n = 64) Mean (SD) | No (n = 25) Mean (SD) | t | p | |
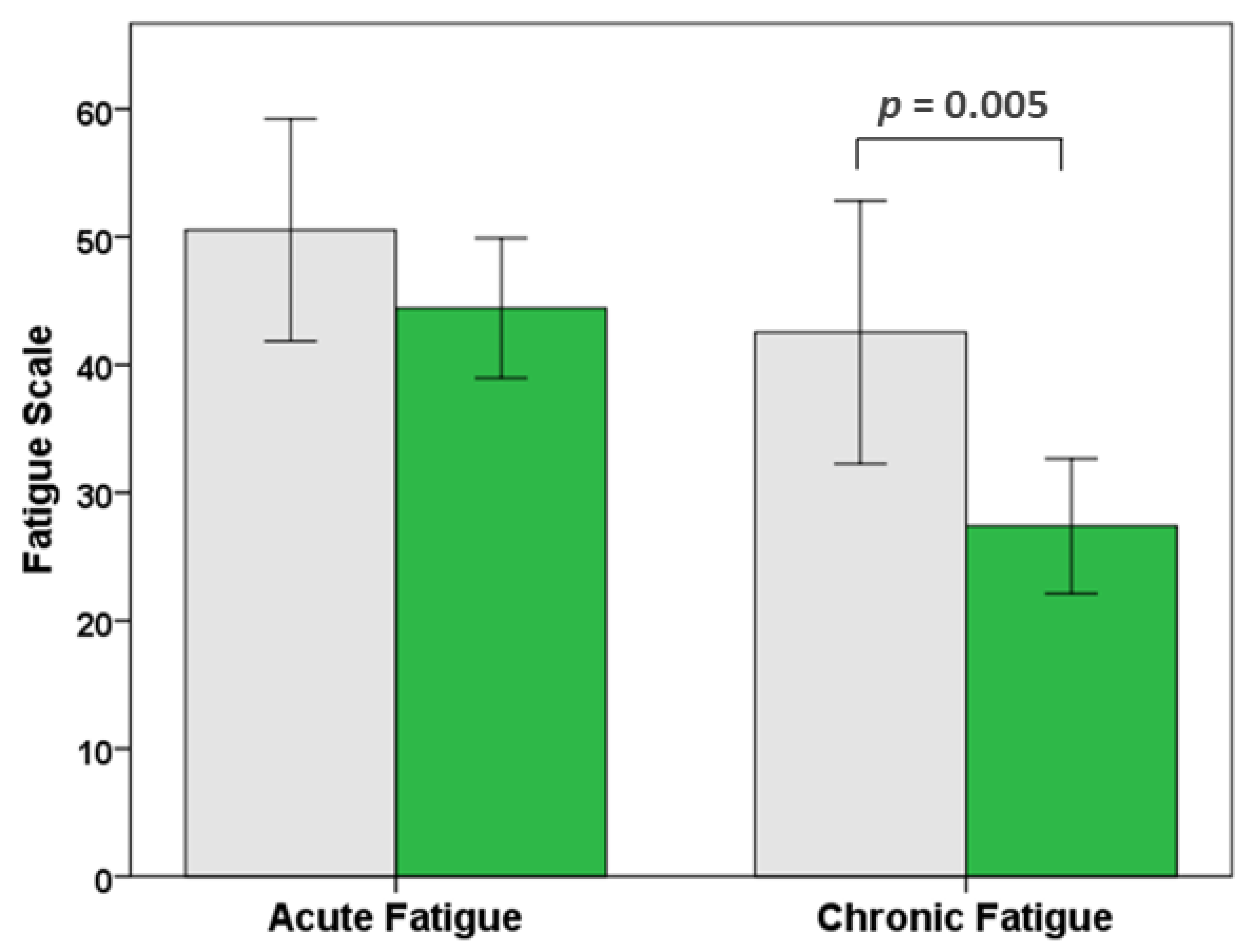
| Chronic fatigue | 27.40 (23.63) | 42.53 (24.86) | −2.888 | 0.005 |
| Acute fatigue | 44.23 (21.86) | 50.53 (21.03) | −1.197 | 0.235 |
| HADS Anxiety | 4.45 (2.85) | 5.04 (2.98) | −0.863 | 0.390 |
| HADS Depression | 7.84 (1.61) | 8.16 (1.38) | 0.868 | 0.388 |
| R | R2 | R2 Change | B | SE | Beta | t | |
|---|---|---|---|---|---|---|---|
| Step 1 | 0.542 | 0.294 *** | |||||
| Weekly hours | 0.648 | 0.261 | 0.459 * | 2.480 | |||
| Anxiety | 3.697 | 0.778 | 0.469 *** | 4.754 | |||
| Step count | 0.004 | 0.003 | 0.591 | 1.480 | |||
| MVPA | −0.522 | 0.298 | −0.289 | −1.753 | |||
| LPA | −18.294 | 14.826 | −0.549 | −1.234 | |||
| Step 2 | 0.617 | 0.381 ** | 0.087 | ||||
| Weekly hours | 0.679 | 0.247 | 0.251 ** | 2.752 | |||
| Anxiety | 3.457 | 0.737 | 0.429 *** | 4.693 | |||
| Step count | 0.006 | 0.003 | 0.864 * | −2.342 | |||
| MVPA | −0.665 | 0.284 | −0.368 * | −2.342 | |||
| LPA | −30.405 | 14.447 | −0.912 * | −2.105 | |||
| Time in nature | −15.822 | 4.787 | −0.311 ** | −3.305 |
| Do You Spend Time in Nature at Least Once a Week? | Comparison of Nature vs. No Nature | |||
|---|---|---|---|---|
| Yes (n = 51) Mean (SD) | No (n = 21) Mean (SD) | t | p | |
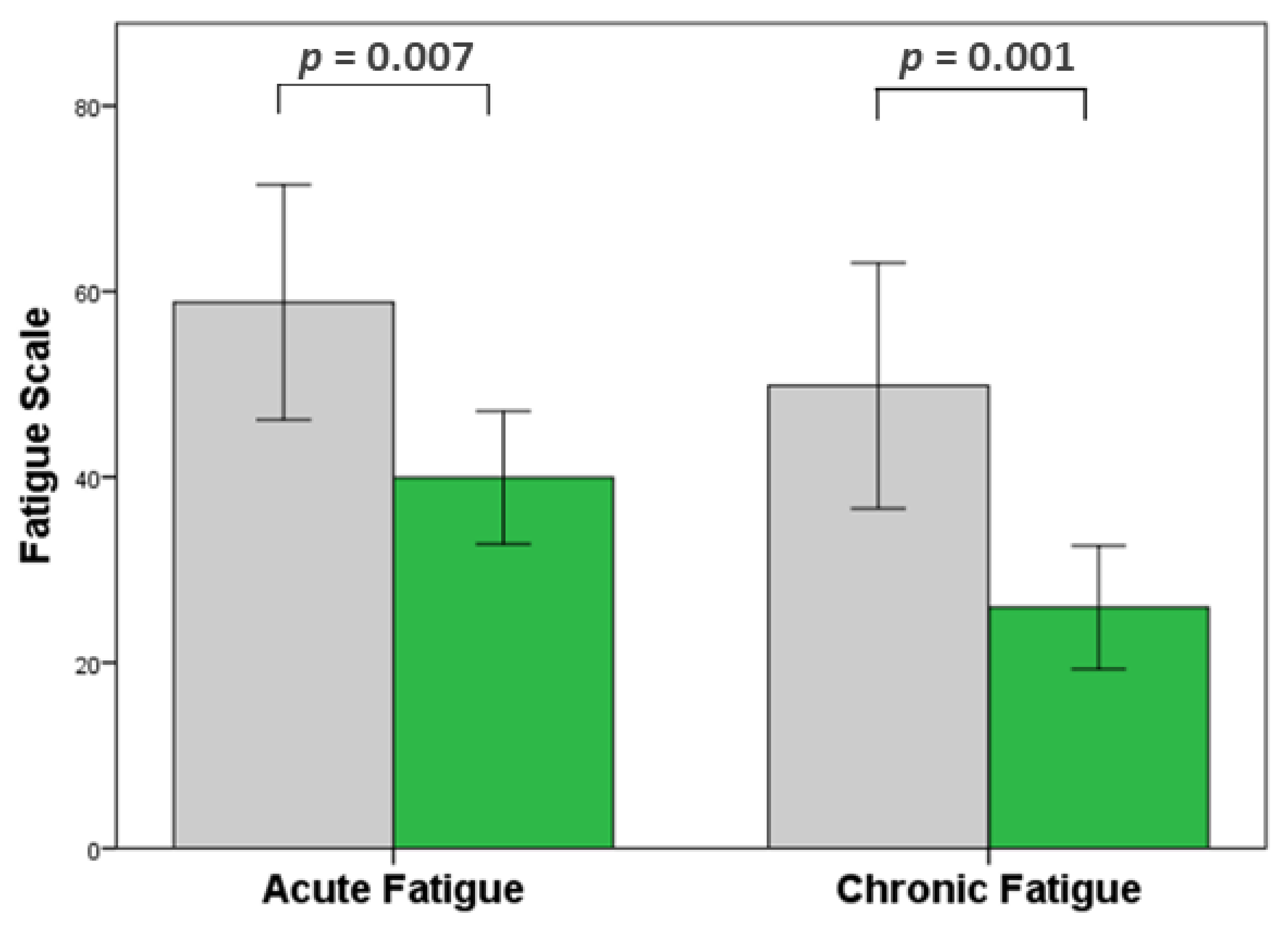
| Chronic fatigue | 25.95 (23.63) | 49.83 (28.29) | −3.621 | 0.001 |
| Acute fatigue | 39.94 (25.40) | 58.83 (27.06) | −2.769 | 0.007 |
| HADS Anxiety | 4.08 (4.00) | 4.45 (4.30) | −0.345 | 0.731 |
| HADS Depression | 3.43 (4.33) | 3.35 (3.62) | 0.074 | 0.941 |
| R | R2 | R2 Change | B | SE | Beta | t | |
|---|---|---|---|---|---|---|---|
| Step 1 | 0.570 | 0.325 *** | |||||
| Anxiety | 3.805 | 0.660 | 0.570 *** | 5.765 | |||
| Step 2 | 0.683 | 0.467 ** | 0.142 | ||||
| Anxiety | 3.700 | 0.591 | 0.555 *** | 6.256 | |||
| Time in nature | −22.511 | 5.298 | −0.377 ** | −4.249 |
| R | R2 | R2 Change | B | SE | Beta | t | |
|---|---|---|---|---|---|---|---|
| Step 1 | 0.522 | 0.273 *** | |||||
| Depression | 3.438 | 0.675 | 0.522 *** | 5.090 | |||
| Step 2 | 0.613 | 0.376 ** | 0.103 | ||||
| Anxiety | 3.457 | 0.630 | 0.525 *** | 5.484 | |||
| Time in nature | −19.180 | 5.725 | −0.350 ** | −3.350 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longman, D.P.; Shaw, C.N.; Varela-Mato, V.; Sherry, A.P.; Ruettger, K.; Sayyah, M.; Guest, A.; Chen, Y.-L.; Paine, N.J.; King, J.A.; et al. Time in Nature Associated with Decreased Fatigue in UK Truck Drivers. Int. J. Environ. Res. Public Health 2021, 18, 3158. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063158
Longman DP, Shaw CN, Varela-Mato V, Sherry AP, Ruettger K, Sayyah M, Guest A, Chen Y-L, Paine NJ, King JA, et al. Time in Nature Associated with Decreased Fatigue in UK Truck Drivers. International Journal of Environmental Research and Public Health. 2021; 18(6):3158. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063158
Chicago/Turabian StyleLongman, Daniel P., Colin N. Shaw, Veronica Varela-Mato, Aron P. Sherry, Katharina Ruettger, Mohsen Sayyah, Amber Guest, Yu-Ling Chen, Nicola J. Paine, James A. King, and et al. 2021. "Time in Nature Associated with Decreased Fatigue in UK Truck Drivers" International Journal of Environmental Research and Public Health 18, no. 6: 3158. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063158