
Development and Effectiveness of a Patient Safety Education Program for Inpatients



Abstract
:1. Introduction
2. Methods
3. Development of the Patient Safety Education Program
3.1. Step 1: Literature Review and Pre-Survey
3.2. Step 2: Development of Patient Safety Education Program for Inpatients
3.2.1. Composition of Educational Contents
3.2.2. Development of Video Using Motion Graphics
3.3. Step 3: Evaluation of the Video Education Program
3.3.1. Professional Evaluation
3.3.2. User Evaluation
4. Effectiveness of the Patient Safety Education Program
4.1. Study Design
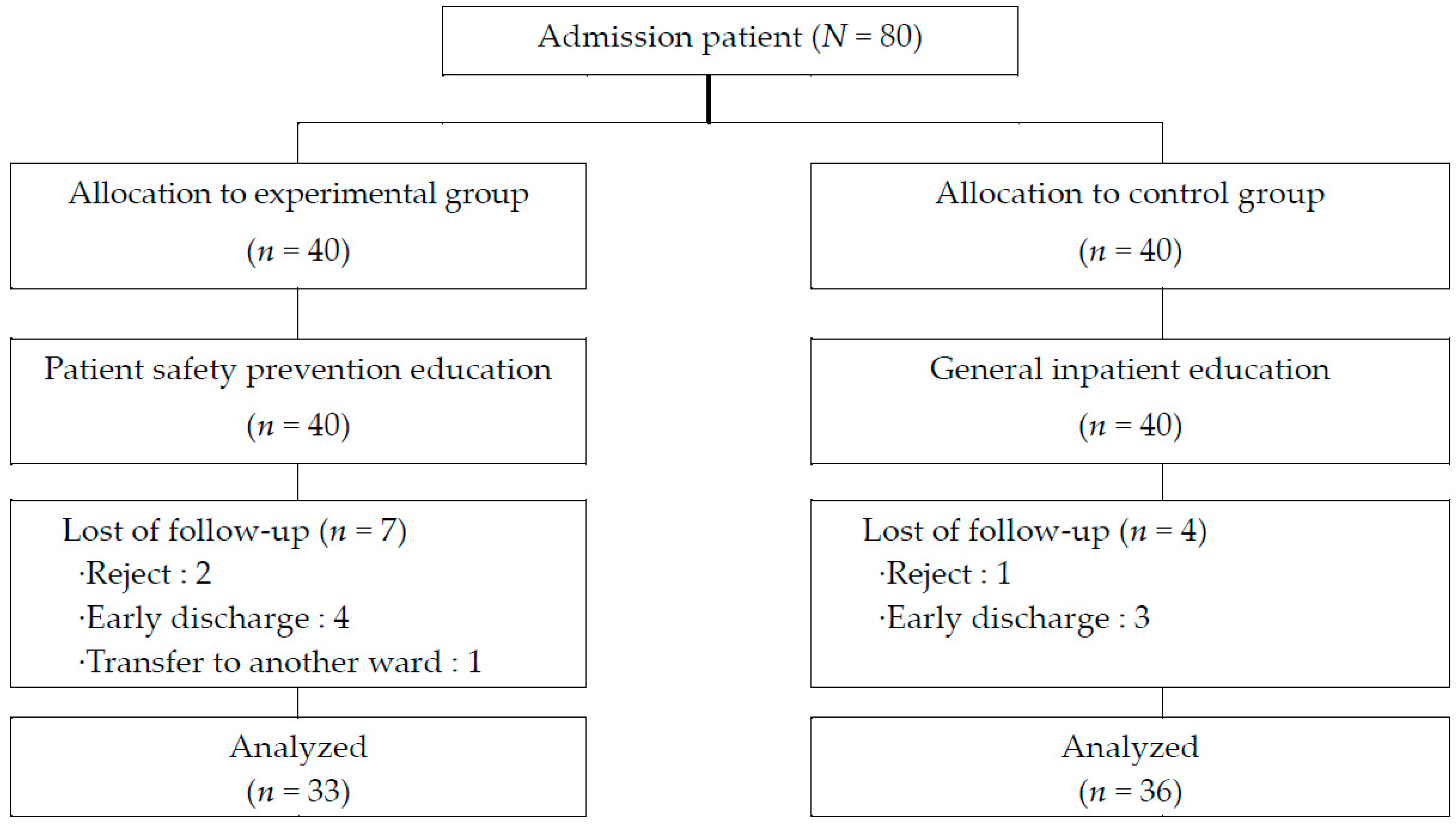
4.2. Participants
4.3. Measurements
4.3.1. Patient Safety Knowledge
4.3.2. Patient Safety Perception
4.3.3. Patient Participation Willingness
4.4. Data Collection and Procedure
4.5. Data Analysis
4.6. Ethical Considerations
5. Results
5.1. Verification of the Sameness of the Subjects
5.2. Validating the Effectiveness of the Patient Safety Education Program
6. Discussion
7. Conclusions
Clinical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Donaldson, M.S. An Overview of to Err is Human: Re-Emphasizing the Message of Patient Safety; Agency for Healthcare Research and Quality(US): Rockville, MD, USA, 2008; Chapter 3. [Google Scholar]
- Fleischut, P.M.; Evans, A.S.; Nugent, W.C.; Faggiani, S.L.; Lazar, E.J.; Liebowitz, R.S.; Forese, L.L.; Kerr, G.E. Ten years after the IOM report: Engaging residents in quality and patient safety by creating a house staff quality council. Am. J. Med. Qual. 2011, 26, 89–94. [Google Scholar] [CrossRef]
- Stelfox, H.T.; Palmisani, S.; Scurlock, C.; Orav, E.J.; Bates, D.W. The “To Err is Human” report and the patient safety literature. BMJ Qual. Saf. 2006, 15, 174–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oikonomou, E.; Carthey, J.; Macrae, C.; Vincent, C. Patient safety regulation in the NHS: Mapping the regulatory landscape of healthcare. BMJ Open 2019, 9, e028663. [Google Scholar] [CrossRef]
- Waring, J. Adaptive regulation or governmentality: Patient safety and the changing regulation of medicine. Sociol. Health Illn. 2007, 29, 163–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, E.-H.; Hyun, K.-S.; Cho, J.-Y. Awareness of hospital safety culture and safety activities of workers in a tertiary care hospital. J. Korean Acad. Soc. Nurs. Educ. 2016, 22, 191–201. [Google Scholar] [CrossRef]
- Kim, L.; Lyder, C.H.; McNeese-Smith, D.; Leach, L.S.; Needleman, J. Defining attributes of patient safety through a concept analysis. J. Adv. Nurs. 2015, 71, 2490–2503. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.E.; Sevdalis, N.; Vincent, C.A. Patient involvement in patient safety: How willing are patients to participate? BMJ Qual. Saf. 2011, 20, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Wachter, R.M. Patient safety at ten: Unmistakable progress, troubling gaps. Health Aff. 2010, 29, 165–173. [Google Scholar] [CrossRef]
- Epstein, R.M.; Fiscella, K.; Lesser, C.S.; Stange, K.C. Why the nation needs a policy push on patient-centered health care. Health Aff. 2010, 29, 1489–1495. [Google Scholar] [CrossRef]
- Rathert, C.; May, D.R. Health care work environments, employee satisfaction, and patient safety: Care provider perspectives. Health Care Manag. Rev. 2007, 32, 2–11. [Google Scholar] [CrossRef] [Green Version]
- Hor, S.-Y.; Godbold, N.; Collier, A.; Iedema, R. Finding the patient in patient safety. Health 2013, 17, 567–583. [Google Scholar] [CrossRef] [PubMed]
- Kirkman, M.A.; Sevdalis, N.; Arora, S.; Baker, P.; Vincent, C.; Ahmed, M. The outcomes of recent patient safety education interventions for trainee physicians and medical students: A systematic review. BMJ Open 2015, 5, e007705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutaimy, R.; Zhang, L.; Blok, D.; Kelly, R.; Kovacevic, N.; Levoska, M.; Gadivemula, R.; Levine, D. Integrating patient safety education into early medical education utilizing cadaver, sponges, and an inter-professional team. BMC Med. Educ. 2018, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Oates, K.; Wilson, I.; Hu, W.; Walker, B.; Nagle, A.; Wiley, J. Changing medical student attitudes to patient safety: A multicentre study. BMC Med. Educ. 2018, 18, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.H.; Jeong, S.Y.; Kwon, M.S. Effects of hazard perception training (HPT) on nursing students’ risk sensitivity to patient safety and developing safety control confidence. Appl. Nurs. Res. 2018, 39, 160–166. [Google Scholar] [CrossRef]
- Torkaman, M.; Sabzi, A.; Farokhzadian, J. The effect of patient safety education on undergraduate nursing students’ patient safety competencies. Int. Q. Community Health Educ. 2020. [Google Scholar] [CrossRef]
- Amiri, M.; Khademian, Z.; Nikandish, R. The effect of nurse empowerment educational program on patient safety culture: A randomized controlled trial. BMC Med. Educ. 2018, 18, 158. [Google Scholar] [CrossRef] [Green Version]
- Burgener, A.M. Enhancing communication to improve patient safety and to increase patient satisfaction. Health Care Manag. 2020, 39, 128–132. [Google Scholar] [CrossRef]
- Lyle-Edrosolo, G.; Waxman, K. Aligning healthcare safety and quality competencies: Quality and safety education for nurses (QSEN), The Joint Commission, and American Nurses Credentialing Center (ANCC) magnet® standards crosswalk. Nurse Lead. 2016, 14, 70–75. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.E.; Sevdalis, N.; Pinto, A.; Darzi, A.; Vincent, C.A. Patients’ attitudes towards patient involvement in safety interventions: Results of two exploratory studies. Health Expect. 2013, 16, e164–e176. [Google Scholar] [CrossRef] [Green Version]
- Pinto, A.; Vincent, C.; Darzi, A.; Davis, R. A qualitative exploration of patients’ attitudes towards the ‘Participate Inform Notice Know’(PINK) patient safety video. Int. J. Qual. Health Care 2013, 25, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Beverstock, A.; Lewis, C.; Bruce, D.; Barnes, J.; Kelly, A. Use of a pediatric admission booklet significantly improves the comprehensiveness of admission documentation: A quality improvement project. Pediatric Qual. Saf. 2020, 5. [Google Scholar] [CrossRef]
- Jung, K.-M.; Joo, M.-C.; Jung, Y.-J.; Kim, H.-H.; Lee, K.-H.; Lee, D.-S.; Choi, J.-W. The effect of smartphone video educational program on educational satisfaction of patients in rehabilitation units at a university hospital. Qual. Improv. Health Care 2017, 23, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.J.; Lee, E. The effects of smartphone application to educate patient on patient safety in hospitalized surgical patients. Korean J. Adult Nurs. 2017, 29, 154–165. [Google Scholar] [CrossRef]
- Rochfort, A.; Beirne, S.; Doran, G.; Patton, P.; Gensichen, J.; Kunnamo, I.; Smith, S.; Eriksson, T.; Collins, C. Does patient self-management education of primary care professionals improve patient outcomes: A systematic review. BMC Fam. Pract. 2018, 19, 1–9. [Google Scholar] [CrossRef]
- Abaraogu, U.; Dall, P.; Seenan, C. The effect of structured patient education on physical activity in patients with peripheral arterial disease and intermittent claudication: A systematic review. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 58–68. [Google Scholar] [CrossRef] [Green Version]
- Waterman, A.D.; Gallagher, T.H.; Garbutt, J.; Waterman, B.M.; Fraser, V.; Burroughs, T.E. Brief report: Hospitalized patients’ attitudes about and participation in error prevention. J. Gen. Intern. Med. 2006, 21, 367–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, J.; Kim, S.J.; Park, S.; Moon, K.T.; Park, E.-C. The effects of patient education on patient safety: Can we change patient perceptions and attitudes?: Lessons from the Armed Forces Capital Hospital in Korea. Int. J. Qual. Health Care 2017, 29, 392–398. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Kwak, M.-J.; Kim, M.-S.; Kim, H.-A.; Kim, H.-S.; Chun, J.-H.; Hwang, J.-I. Safety education programs for patients and families in overseas institutions. Qual. Improv. Health Care 2019, 25, 2–10. [Google Scholar] [CrossRef]
- McCarthy, S.E.; O’Boyle, C.A.; O’Shaughnessy, A.; Walsh, G. Online patient safety education programme for junior doctors: Is it worthwhile? Ir. J. Med. Sci. 2016, 185, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Anthony, R.; Miranda, F.; Mawji, Z.; Davis, R.; Lawrence, S.; Cerimele, R. The LVHHN patient safety video: Patients as partners in safe care delivery. Jt. Comm. J. Qual. Saf. 2003, 29, 640–645. [Google Scholar] [CrossRef]
- Molenda, M. In search of the elusive ADDIE model. Perform. Improv. 2003, 42, 34–37. [Google Scholar] [CrossRef]
- Shin, S.H. Analysis of subgroups with lower level of patient safety perceptions using decision-tree analysis. J. Korean Acad. Nurs. 2020, 50, 686–698. [Google Scholar] [CrossRef]
- Lee, J. The Knowledge and Attitude of Patient Safety of Hospitalized Patients; Catholic University: Seoul, Korea, 2019. [Google Scholar]
- Kim, K.J.; Lee, E.H.; Shin, S.H. Development and validation of the patient safety perception scale for hospitalized patients. Korean J. Adult Nurs. 2018, 30, 404–416. [Google Scholar] [CrossRef] [Green Version]
- Giles, S.J.; Lawton, R.J.; Din, I.; McEachan, R.R. Developing a patient measure of safety (PMOS). BMJ Qual. Saf. 2013, 22, 554–562. [Google Scholar] [CrossRef] [Green Version]
- Lee, K. Willingness toward Patient Participation in Patient Safety; Ulsan University: Ulsan, Korea, 2018. [Google Scholar]
- Jung, H.-S.; Kim, S.H. The development and effect of the patient safety education program using simulated situation. J. Korea Acad.-Ind. Coop. Soc. 2019, 20, 398–409. [Google Scholar] [CrossRef]
- Godlock, G.; Christiansen, M.; Feider, L. Implementation of an evidence-based patient safety team to prevent falls in inpatient medical units. MedSurg Nurs. 2016, 25, 17–23. [Google Scholar]
- Kim, Y.-S.; Kim, M.-S.; Hwang, J.-I.; Kim, H.-R.; Kim, H.-A.; Kim, H.-S.; Chun, J.-H.; Kwak, M.-J. Experiences in patient safety education of patient safety officer using focus group interview. Qual. Improv. Health Care 2019, 25, 2–15. [Google Scholar] [CrossRef] [Green Version]
- Woolley, A.K.; Hadjiconstantinou, M.; Davies, M.; Khunti, K.; Seidu, S. Online patient education interventions in type 2 diabetes or cardiovascular disease: A systematic review of systematic reviews. Prim. Care Diabetes 2019, 13, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Faury, S.; Koleck, M.; Foucaud, J.; M’Bailara, K.; Quintard, B. Patient education interventions for colorectal cancer patients with stoma: A systematic review. Patient Educ. Couns. 2017, 100, 1807–1819. [Google Scholar] [CrossRef] [PubMed]
- The Joint Commission. Sentinel Event Data—General Information; The Joint Commission: Geneva, Switzerland, 2018. [Google Scholar]
- Auraaen, A.; Slawomirski, L.; Klazinga, N. The economics of patient safety in primary and ambulatory care: Flying blind. OECD Health Work. Pap. 2018. [Google Scholar] [CrossRef]
- Kim, S.; Kim, J.; Kim, G.; Lee, A.; Lee, H.; Choi, Y.; Park, Y. Effects of Fall Education Program Using Tablet PCs: Hospitalized Patient. Asia-Pac. J. Multimed. Serv. Converg. Art Humanit. Sociol. 2016, 6, 323–331. [Google Scholar] [CrossRef]
- Pyo, J.; Lee, W.; Choi, E.; Jang, S.; Ock, M.; Lee, S. Promoting awareness of patient safety and patient engagement through patient safety education for the general public: Pilot study. Korean Public Health Res. 2018, 44, 65–88. [Google Scholar] [CrossRef]
- Finn, K.M.; Metlay, J.P.; Chang, Y.; Nagarur, A.; Yang, S.; Landrigan, C.P.; Iyasere, C. Effect of increased inpatient attending physician supervision on medical errors, patient safety, and resident education: A randomized clinical trial. JAMA Intern. Med. 2018, 178, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Sahlström, M.; Partanen, P.; Azimirad, M.; Selander, T.; Turunen, H. Patient participation in patient safety—An exploration of promoting factors. J. Nurs. Manag. 2019, 27, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Doherty, C.; Stavropoulou, C. Patients’ willingness and ability to participate actively in the reduction of clinical errors: A systematic literature review. Soc. Sci. Med. 2012, 75, 257–263. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Composition | Contents | Detail Contents | Time |
|---|---|---|---|
| 1 video (7 min 38 s) | Understanding patient safety | Introduction of patient safety and laws | 28 s |
| Introduction of medical institution certification mark | 26 s | ||
| The importance of patient safety | 34 s | ||
| Patient safety activities | Patient identification | 53 s | |
| Fall prevention | 22 s | ||
| Infection prevention | 31 s | ||
| Bedsores prevention | 22 s | ||
| Fire prevention | 33 s | ||
| Participation in patient safety (accurate communication) | Notify | 51 s | |
| Check | 64 s | ||
| Ask | 34 s | ||
| 2 video (7 min 6 s) | Fall prevention activities | Raise and fix bed railing | 25 s |
| How to use a wheelchair | 22 s | ||
| Wear shoes that fit your feet | 7 s | ||
| Go to the bathroom before sleeping | 10 s | ||
| High risk patient management | 13 s | ||
| Infection prevention activities | Hand hygiene method | 49 s | |
| When to perform hand hygiene | 21 s | ||
| Limited visitor and visit time | 38 s | ||
| Bedsores prevention activities | Skin condition check | 31 s | |
| Change of position | |||
| Participation in patient safety (review) | Notify | 42 s | |
| Check | |||
| Ask | |||
| Coping method in the patient safety problems | Introduction of the “Patient Safety Report Learning System” | 40 s | |
| Introduction of the “Korea Medical Dispute Mediation Arbitration Agency” |
| Pre-Test | Post-Test | Pre-Test | Intervention | Post-Test | ||
|---|---|---|---|---|---|---|
| Period | 20 July–11 September | 20 September–13 November | ||||
| HD 1 | HD 5~7 | HD 1 | HD 3 | HD 5 | HD 7 | |
| Experimental group | E1, X1 | X2 | X3 | E2 | ||
| Control group | C1 | C2 | ||||
| Characteristics | Categories | Total | Exp. (n = 33) | Cont. (n = 36) | χ2 or t | p |
|---|---|---|---|---|---|---|
| n (%) | n (%) or M ± SD | n (%) or M ± SD | ||||
| Gender | Male | 39 (56.5) | 17 (43.6) | 22 (56.4) | 0.65 | 0.472 |
| Female | 30 (43.5) | 16 (53.3) | 14 (46.7) | |||
| Age group | 20–39 | 23 (33.3) | 10 (43.5) | 13 (56.5) | 1.10 | 0.576 |
| 40–59 | 17 (24.6) | 7 (41.2) | 10 (58.8) | |||
| Over 60′s | 28 (42.0) | 16 (55.2) | 13 (44.8) | |||
| Final education | Middle school | 19 (27.5) | 9 (47.4) | 10 (52.6) | 0.89 | 0.956 |
| High school | 26 (37.7) | 13 (50.0) | 13 (50.0) | |||
| University | 24 (34.8) | 11 (45.8) | 13 (54.2) | |||
| Economic level | High | 5 (7.2) | 4 (80.0) | 1 (20.0) | 2.57 | 0.276 |
| Middle | 40 (58.0) | 17 (42.5) | 23 (57.5) | |||
| Low | 24 (34.8) | 12 (50.0) | 12 (50.0) | |||
| Religion | Yes | 23 (33.3) | 12 (52.2) | 11 (47.8) | 2.61 | 0.621 |
| No | 46 (66.7) | 21 (45.7) | 25 (54.3) | |||
| Job | Yes | 47 (68.1) | 21 (44.7) | 26 (55.3) | 0.58 | 0.606 |
| No | 22 (31.9) | 12 (54.5) | 10 (45.5) | |||
| Underlying disease | Yes | 26 (37.7) | 14 (53.8) | 12 (46.2) | 0.61 | 0.466 |
| No | 43 (62.3) | 19 (44.2) | 24 (55.8) | |||
| Medical institution visit | less than once a month | 13 (18.8) | 5 (38.5) | 8 (61.5) | 0.64 | 0.725 |
| less than once in 3 months | 19 (27.5) | 9 (47.4) | 10 (52.6) | |||
| less than once a year | 37 (53.6) | 19 (51.4) | 18 (48.6) | |||
| Operation | Yes | 45 (65.2) | 22 (48.9) | 23 (51.1) | 0.06 | 1.000 |
| No | 24 (34.8) | 11 (45.8) | 13 (54.2) | |||
| Medical department | Medicine | 41 (59.4) | 19 (46.3) | 22 (53.7) | 3.49 | 0.175 |
| Surgery | 22 (31.9) | 13 (59.1) | 9 (40.9) | |||
| Other | 6 (8.7) | 1 (16.7) | 5 (83.3) | |||
| Educational experience | Yes | 55 (79.7) | 29 (52.7) | 26 (47.3) | 2.61 | 0.139 |
| No | 14 (20.3) | 4 (28.6) | 10 (71.4) | |||
| Inpatient period | 10.85 ± 8.20 | 8.92 ± 4.29 | 1.24 | 0.219 | ||
| PS knowledge | 22.88 ± 3.80 | 24.28 ± 3.13 | −1.68 | 0.099 | ||
| PS perception | 97.24 ± 21.81 | 102.28 ± 20.52 | −0.99 | 0.327 | ||
| Willingness to participate in PS | 61.21 ± 8.64 | 60.86 ± 10.73 | 0.15 | 0.882 | ||
| Variables | Group | Pre-Test | Post-Test | Within Group | Difference | Between Group | ||
|---|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | t | p | M ± SD | t | p | ||
| PS knowledge | Exp. (n = 33) | 22.88 ± 3.80 | 25.24 ± 1.98 | 3.94 | <0.001 | 2.36 ± 3.44 | 2.52 | 0.014 |
| Cont. (n = 36) | 24.28 ± 3.13 | 24.83 ± 3.03 | 1.35 | 0.187 | 0.56 ± 2.48 | |||
| PS perception | Exp. (n= 33) | 97.24 ± 21.81 | 109.03 ± 9.95 | 3.78 | 0.001 | 11.79 ± 17.95 | 2.09 | 0.040 |
| Cont. (n = 36) | 102.28 ± 20.52 | 105.44 ± 13.37 | 1.17 | 0.251 | 3.17 ± 16.27 | |||
| Willingness to participate in PS | Exp. (n = 33) | 61.21 ± 8.64 | 65.85 ± 7.71 | 3.33 | 0.002 | 4.64 ± 7.99 | 0.71 | 0.478 |
| Cont. (n = 36) | 60.86 ± 10.73 | 64.14 ± 9.42 | 2.51 | 0.017 | 3.28 ± 7.83 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.H.; Kim, M.J.; Moon, H.J.; Lee, E.H. Development and Effectiveness of a Patient Safety Education Program for Inpatients. Int. J. Environ. Res. Public Health 2021, 18, 3262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063262
Shin SH, Kim MJ, Moon HJ, Lee EH. Development and Effectiveness of a Patient Safety Education Program for Inpatients. International Journal of Environmental Research and Public Health. 2021; 18(6):3262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063262
Chicago/Turabian StyleShin, Sun Hwa, Mi Jung Kim, Ho Jin Moon, and Eun Hye Lee. 2021. "Development and Effectiveness of a Patient Safety Education Program for Inpatients" International Journal of Environmental Research and Public Health 18, no. 6: 3262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063262