
An Overview of Thermal Infrared Imaging-Based Screenings during Pandemic Emergencies



Abstract
:1. Introduction
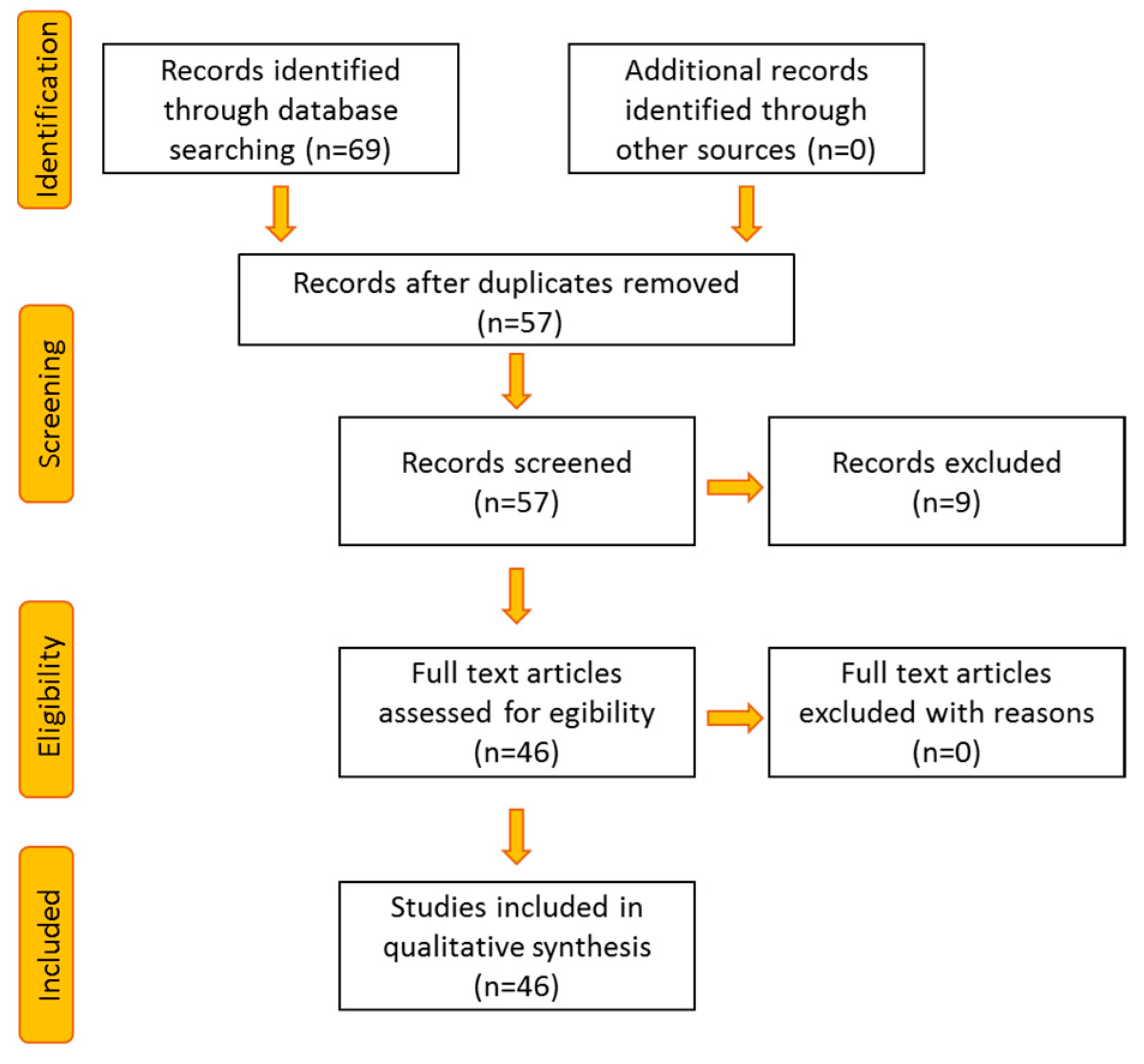
2. Study Organization and Search Processing Method
3. Methodologies for IRI-Based Fever Detection
3.1. External and Internal Confounding for Fever Assessment
3.2. Inner Canthi Identification and Face Segmentation Algorithms in Pandemic Outbreaks
4. Mass IRI-Based Fever Screening in Public Environments
4.1. Mass Fever Screening in Hospitals
4.2. Mass Fever Screening in Airports
5. Machine Learning Applications for Respiratory Diseases Assessment
6. Smart Technologies to Limit COVID-19 Diffusion
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 28 December 2020).
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Heal. 2020, 25, 278–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2020, 19, 1–14. [Google Scholar] [CrossRef]
- Al-Qahtani, W.S.; Alneghery, L.M.; Alqahtani, A.Q.S.; ALKahtani, M.D.; Alkahtani, S. A Review of comparison study between corona viruses (SARS-cov, MERS-cov) and novel corona virus (Covid-19). Rev. Mexicana Ing. Quím. 2020, 19, 201–212. [Google Scholar] [CrossRef]
- Chen, J. Pathogenicity and transmissibility of 2019-nCoV—A quick overview and comparison with other emerging viruses. Microbes Infect. 2020, 22, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Rothe, C.; Schunk, M.; Seilmaier, M.; Drosten, C.; Vollmar, P.; Zwirglmaier, K.; Zange, S.; Wölfel, R.; Hoelscher, M.; Sothmann, P.; et al. Transmission of 2019-nCoV infection from an asymptomaticcontact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance 2020, 25, 2000062. [Google Scholar] [CrossRef] [Green Version]
- Eurosurveillance editorial team Updated rapid risk assessment from ECDC on the novel coronavirus disease 2019 (COVID-19) pandemic: Increased transmission in the EU/EEA and the UK. Eurosurveillance 2020, 25, 2003121. [CrossRef]
- Khan, R.S.; Rehman, I.U. Spectroscopy as a tool for detection and monitoring of Coronavirus (COVID-19). Expert Rev. Mol. Diagn. 2020, 20, 647–649. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, J.; Reuss, J.E.; Suresh, K.; Feller-Kopman, D.; Forde, P.M.; Steinke, S.M.; Rock, C.; Johnson, D.B.; Nishino, M.; Brahmer, J.R. Immune-related (IR)-pneumonitis during the COVID-19 pandemic: Multidisciplinary recommendations for diagnosis and management. J. Immunother. Cancer 2020, 8, e000984. [Google Scholar] [CrossRef] [PubMed]
- Aw, J. The non-contact handheld cutaneous infra-red thermometer for fever screening during the COVID-19 global emergency. J. Hosp. Infect. 2020, 104, 451. [Google Scholar] [CrossRef]
- Aggarwal, N.; Garg, M.; Dwarakanathan, V.; Gautam, N.; Kumar, S.S.; Jadon, R.S.; Gupta, M.; Ray, A. Diagnostic accuracy of non-contact infrared thermometers and thermal scanners: A systematic review and meta-analysis. J. Travel Med. 2020, 27, 193. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Rogalski, A. Infrared Detectors; CRC Press: Boca Raton, FL, USA, 2010; ISBN 1-4200-7672-8. [Google Scholar]
- Hildebrandt, C.; Raschner, C.; Ammer, K. An overview of recent application of medical infrared thermography in sports medicine in Austria. Sensors 2010, 10, 4700–4715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchis-Sánchez, E.; Vergara-Hernández, C.; Cibrián, R.M.; Salvador, R.; Sanchis, E.; Codoñer-Franch, P. Infrared thermal imaging in the diagnosis of musculoskeletal injuries: A systematic review and meta-analysis. Am. J. Roentgenol. 2014, 203, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Sillero-Quintana, M.; Fernández-Jaén, T.; Fernández-Cuevas, I.; Gómez-Carmona, P.M.; Arnaiz-Lastras, J.; Pérez, M.-D.; Guillen, P. Infrared thermography as a support tool for screening and early diagnosis in emergencies. J. Med. Imaging Heal. Inform. 2015, 5, 1223–1228. [Google Scholar] [CrossRef]
- Kennedy, D.A.; Lee, T.; Seely, D. A comparative review of thermography as a breast cancer screening technique. Integr. Cancer Ther. 2009, 8, 9–16. [Google Scholar] [CrossRef]
- Hernandez-Contreras, D.; Peregrina-Barreto, H.; Rangel-Magdaleno, J.; Gonzalez-Bernal, J. Narrative review: Diabetic foot and infrared thermography. Infrared Phys. Technol. 2016, 78, 105–117. [Google Scholar] [CrossRef]
- Capo, A.; Ismail, E.; Cardone, D.; Celletti, E.; Auriemma, M.; Sabatini, E.; Merla, A.; Amerio, P. Joint functional impairment and thermal alterations in patients with Psoriatic Arthritis: A thermal imaging study. Microvasc. Res. 2015, 102, 86–91. [Google Scholar] [CrossRef]
- Perpetuini, D.; Trippetti, N.; Cardone, D.; Breda, L.; D’Attilio, M.; Merla, A. Detection of temporomandibular joint disfunction in juvenile idiopathic arthritis through infrared thermal imaging and a machine learning procedure. In Proceedings of the 8th European Medical and Biological Engineering Conference, Portorož, Slovenia, 29 November–3 December 2020; Metzlerarmn, J.B., Cvetko, T., Mahnič-Kalamiza, A., Mityle, A., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 372–381. [Google Scholar]
- Filippini, C.; Perpetuini, D.; Cardone, D.; Chiarelli, A.M.; Merla, A. Thermal infrared imaging-based affective computing and its application to facilitate human robot interaction: A review. Appl. Sci. 2020, 10, 2924. [Google Scholar] [CrossRef]
- Cardone, D.; Perpetuini, D.; Filippini, C.; Spadolini, E.; Mancini, L.; Chiarelli, A.M.; Merla, A. Driver stress state evaluation by means of thermal imaging: A supervised machine learning approach based on ECG signal. Appl. Sci. 2020, 10, 5673. [Google Scholar] [CrossRef]
- Perpetuini, D.; Cardone, D.; Bucco, R.; Zito, M.; Merla, A. Assessment of the autonomic response in alzheimer’s patients during the execution of memory tasks: A functional thermal imaging study. Curr. Alzheimer Res. 2018, 15, 951–958. [Google Scholar] [CrossRef]
- Magalhaes, C.; Mendes, J.; Vardasca, R. Meta-analysis and systematic review of the application of machine learning classifiers in biomedical applications of infrared thermography. Appl. Sci. 2021, 11, 842. [Google Scholar] [CrossRef]
- Kitchenham, B. Procedures for Performing Systematic Reviews; Keele University Technical Report; Keele University: Newcastle, UK, 2004; pp. 1–26. [Google Scholar]
- Hausfater, P.; Zhao, Y.; Defrenne, S.; Bonnet, P.; Riou, B. Cutaneous infrared thermometry for detecting febrile patients. Emerg. Infect. Dis. 2008, 14, 1255–1258. [Google Scholar] [CrossRef]
- Zhou, Y.; Ghassemi, P.; Chen, M.; McBride, D.; Casamento, J.P.; Pfefer, T.J.; Wang, Q. Clinical evaluation of fever-screening thermography: Impact of consensus guidelines and facial measurement location. J. Biomed. Opt. 2020, 25, 097002. [Google Scholar] [CrossRef]
- Chen, H.-Y.; Chen, A.; Chen, C. Investigation of the impact of infrared sensors on core body temperature monitoring by comparing measurement sites. Sensors 2020, 20, 2885. [Google Scholar] [CrossRef] [PubMed]
- Ring, E.; Jung, A.; Zuber, J.; Rutkowski, P.; Kalicki, B.; Bajwa, U. Detecting fever in Polish children by infrared thermography. In Proceedings of the 9th International Conference on 2008 Quantitative InfraRed Thermography; QIRT Council, Krakow, Poland, 2–5 July 2008; Volume 2. [Google Scholar]
- Dzien, C.; Halder, W.; Winner, H.; Lechleitner, M. Covid-19 screening: Are forehead temperature measurements during cold outdoor temperatures really helpful? Wien. Klin. Wochenschr. 2020, 1–5. [Google Scholar] [CrossRef]
- Ghassemi, P.; Pfefer, J.; Casamento, J.; Wang, Q. Standardized assessment of infrared thermographic fever screening system performance. In Proceedings of the Design and Quality for Biomedical Technologies X; International Society for Optics and Photonics, San Francisco, CA, USA, 28–29 January 2017; Volume 10056, p. 100560H. [Google Scholar] [CrossRef]
- Ghassemi, P.; Pfefer, T.J.; Casamento, J.P.; Simpson, R.; Wang, Q. Best practices for standardized performance testing of infrared thermographs intended for fever screening. PLoS ONE 2018, 13, e0203302. [Google Scholar] [CrossRef] [Green Version]
- Chu, N.; Zhong, Y.; Hou, Y. High-precision thermography based on JMAP inference for human face temperature. In Proceedings of the Infrared, Millimeter-Wave, and Terahertz Technologies VII.; SPIE-Intl Soc Optical Eng, 11–16 October 2020; Online Only. Volume 11559, p. 115590. [Google Scholar]
- Ring, E.F.J.; Jung, A.; Kalicki, B.; Zuber, J.; Rustecka, A.; Vardasca, R. New standards for fever screening with thermal imaging systems. J. Mech. Med. Biol. 2013, 13. [Google Scholar] [CrossRef]
- Dwith, C.Y.N.; Ghassemi, P.; Pfefer, J.; Casamento, J.; Wang, Q. Multi-modality image registration for effective thermographic fever screening. In Proceedings of the Multimodal Biomedical Imaging XII; International Society for Optics and Photonics, San Francisco, CA, USA, 28 January 2017; Volume 10057, p. 100570. [Google Scholar] [CrossRef]
- Chenna, Y.N.D.; Ghassemi, P.; Pfefer, T.J.; Casamento, J.; Wang, Q. Free-form deformation approach for registration of visible and infrared facial images in fever screening. Sensors 2018, 18, 125. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, C.; Berlincioni, L.; Bertini, M.; Del Bimbo, A. Inner eye canthus localization for human body temperature screening. arXiv 2020, arXiv:2008.12046. Available online: https://arxiv.org/abs/2008.12046 (accessed on 20 December 2020).
- Cardone, D.; Spadolini, E.; Perpetuini, D.; Filippini, C.; Chiarelli, A.M.; Merla, A. Automated warping procedure for facial thermal imaging based on features identification in the visible domain. Infrared Phys. Technol. 2021, 112, 103595. [Google Scholar] [CrossRef]
- Baltrusaitis, T.; Robinson, P.; Morency, L.-P. OpenFace: An open source facial behavior analysis toolkit. In Proceedings of the 2016 IEEE Winter Conference on Applications of Computer Vision (WACV), Lake Placid, NY, USA, 7–10 March 2016. [Google Scholar]
- Müller, D.; Ehlen, A.; Valeske, B. Convolutional neural networks for semantic segmentation as a tool for multiclass face analysis in thermal infrared. J. Nondestruct. Evaluation 2021, 40, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Radzi, S.; Ghazali, K.; AlHarpy, A.M.; Naim, F.; Zan, N.C.; Mohammad, S. Using bimodal gaussian mixture model-based algorithm for background segmentation in thermal fever mass screening. Procedia Comput. Sci. 2011. [Google Scholar]
- Vardasca, R. The influence of angles and distance on assessing inner-canthi of the eye skin temperature. Thermol. Int. 2017, 27, 130–135. [Google Scholar]
- Vardasca, R.; Magalhaes, C.; Marques, D.; Moreira, J.; Frade, R.A.; Seixas, A.; Mendes, J.G.; Ring, F. Bilateral assessment of body core temperature through axillar, tympanic and inner canthi thermometers in a young population. Physiol. Meas. 2019, 40, 094001. [Google Scholar] [CrossRef]
- Hewlett, A.L.; Kalil, A.C.; Strum, R.A.; Zeger, W.G.; Smith, P.W. Evaluation of an infrared thermal detection system for fever recognition during the H1N1 influenza pandemic. Infect. Control. Hosp. Epidemiol. 2011, 32, 504–506. [Google Scholar] [CrossRef] [PubMed]
- Chiu, W.T.; Lin, P.W.; Deng, W.; Hsu, C.; Chiou, H.; Lee, W.; Lee, C.; Yang, Y.; Lee, H.; Hsieh, M.; et al. Infrared thermography to mass-screen suspected sars patients with fever. Asia Pac. J. Public Health 2005, 17, 26–28. [Google Scholar] [CrossRef]
- Bardou, M.; Seng, P.; Meddeb, L.; Gaudart, J.; Honnorat, E.; Stein, A. Modern approach to infectious disease management using infrared thermal camera scanning for fever in healthcare settings. J. Infect. 2017, 74, 95–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, A.V.; Cohen, N.J.; Roberts, R.R.; Stryker, D.W.; Fishbein, D.B.; Lipman, H.; Brown, C.M.; Molinari, N.-A.; Jackson, W.L.; Kirking, H.; et al. Comparison of 3 infrared thermal detection systems and self-report for mass fever screening. Emerg. Infect. Dis. 2010, 16, 1710–1717. [Google Scholar] [CrossRef]
- Chiang, M.-F.; Lin, P.-W.; Lin, L.-F.; Chiou, H.-Y.; Chien, C.-W.; Chu, S.-F.; Chiu, W.-T. Mass screening of suspected febrile patients with remote-sensing infrared thermography: Alarm temperature and optimal distance. J. Formos. Med. Assoc. 2008, 107, 937–944. [Google Scholar] [CrossRef] [Green Version]
- McConeghy, K.W.; White, E.; Panagiotou, O.A.; Santostefano, C.; Halladay, C.; Feifer, R.A.; Blackman, C.; Rudolph, J.L.; Mor, V.; Gravenstein, S. Temperature screening for SARS-CoV-2 in nursing homes: Evidence from two national cohorts. J. Am. Geriat. Soc. 2020. [Google Scholar] [CrossRef]
- Nishiura, H.; Kamiya, K. Fever screening during the influenza (H1N1-2009) pandemic at Narita International Airport, Japan. BMC Infect. Dis. 2011, 11, 111. [Google Scholar] [CrossRef] [Green Version]
- Kuan, M.-M.; Lin, T.; Chuang, J.-H.; Wu, H.-S. Epidemiological trends and the effect of airport fever screening on prevention of domestic dengue fever outbreaks in Taiwan, 1998–2007. Int. J. Infect. Dis. 2010, 14, e693–e697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuan, M.-M.; Chang, F.-Y. Airport sentinel surveillance and entry quarantine for dengue infections following a fever screening program in Taiwan. BMC Infect. Dis. 2012, 12, 182. [Google Scholar] [CrossRef] [Green Version]
- Shu, P.-Y.; Chien, L.-J.; Chang, S.-F.; Su, C.-L.; Kuo, Y.-C.; Liao, T.-L.; Ho, M.-S.; Lin, T.-H.; Huang, J.-H. Fever screening at airports and imported Dengue. Emerg. Infect. Dis. 2005, 11, 460–462. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.S.; Yoon, J. Fever screening and detection of febrile arrivals at an international airport in Korea: Association among self-reported fever, infrared thermal camera scanning, and tympanic temperature. Epidemiol. Heal. 2014, 36, e2014004. [Google Scholar] [CrossRef] [Green Version]
- Sun, G.; Abe, S.; Takei, O.; Matsui, T. A portable screening system for onboard entry screening at international airports using a microwave radar, reflective photo sensor and thermography. In Proceedings of the 2011 2nd International Conference on Instrumentation, Communications, Information Technology, and Biomedical Engineering; Institute of Electrical and Electronics Engineers (IEEE), Bandung, West Java, Indonesia, 9–11 November 2011; pp. 107–110. [Google Scholar]
- Bradski, G.; Kaehler, A. Learning OpenCV: Computer Vision with the OpenCV Library; O’Reilly Media, Inc.: Gravenstain Highway North, Sebastopol, CA, USA, 2008; ISBN 978-0-596-55404-0. [Google Scholar]
- Dell’Isola, G.B.; Cosentini, E.; Canale, L.; Ficco, G.; Dell’Isola, M. Noncontact body temperature measurement: Uncertainty evaluation and screening decision rule to prevent the spread of COVID-19. Sensors 2021, 21, 346. [Google Scholar] [CrossRef]
- Sun, G.; Matsui, T.; Hakozaki, Y.; Abe, S. An infectious disease/fever screening radar system which stratifies higher-risk patients within ten seconds using a neural network and the fuzzy grouping method. J. Infect. 2015, 70, 230–236. [Google Scholar] [CrossRef]
- Dagdanpurev, S.; Sun, G.; Choimaa, L.; Abe, S.; Matsui, T. Clinical application of multiple vital signs-based infection screening system in a mongolian hospital: Optimization of facial temperature measurement by thermography at various ambient temperature conditions using linear regression analysis. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC); Institute of Electrical and Electronics Engineers (IEEE), Honolulu, HI, USA, 17–21 July 2018; Volume 2018, pp. 5313–5316. [Google Scholar]
- Ng, E.Y.K. Advanced Integrative Thermography in Identification of Human Elevated Temperature; Advances in Biomedical Research, WSEAS Press, Stevens Point: Wisconsin, MN, USA, 2010; pp. 190–195. [Google Scholar]
- Ng, E.Y.-K. Is thermal scanner losing its bite in mass screening of fever due to SARS? Med Phys. 2004, 32, 93–97. [Google Scholar] [CrossRef]
- Jiang, Z.; Hu, M.; Gao, Z.; Fan, L.; Dai, R.; Pan, Y.; Tang, W.; Zhai, G.; Lu, Y. Detection of respiratory infections using RGB-infrared sensors on portable device. IEEE Sensors J. 2020, 20, 13674–13681. [Google Scholar] [CrossRef]
- Jiang, Z.; Hu, M.; Fan, L.; Pan, Y.; Tang, W.; Zhai, G.; Lu, Y. Combining Visible Light and Infrared Imaging for Efficient Detection of Respiratory Infections Such as COVID-19 on Portable Device. arXiv 2020, arXiv:2004.06912. Available online: https://arxiv.org/abs/2004.06912 (accessed on 20 December 2020).
- Jiang, Z.; Hu, M.; Zhai, G. Portable health screening device of respiratory infectionsa. In Proceedings of the 2020 IEEE International Conference on Multimedia & Expo Workshops (ICMEW); Institute of Electrical and Electronics Engineers (IEEE), London, UK, 6–10 July 2020; pp. 1–2. [Google Scholar]
- Martinez-Jimenez, M.A.; Loza-Gonzalez, V.M.; Kolosovas-Machuca, E.S.; Yanes-Lane, M.E.; Ramirez-GarciaLuna, A.S.; Ramirez-GarciaLuna, J.L. Diagnostic accuracy of infrared thermal imaging for detecting COVID-19 infection in minimally symptomatic patients. Eur. J. Clin. Investig. 2020, e13474. [Google Scholar] [CrossRef]
- Al-Humairi, S.N.S.; Zainol, M.H.; Razalli, H.; Raya, L.; Irsyad, M. Conceptual design: A novel COVID-19 smart AI helmet. Int. J. Emerg. Technol. 2020, 11, 389–396. [Google Scholar]
- Rane, K.P. Design and development of low cost humanoid robot with thermal temperature scanner for COVID-19 virus preliminary identification. Int. J. Adv. Trends Comput. Sci. Eng. 2020, 9, 3485–3493. [Google Scholar] [CrossRef]
- Mohammed, M.N.; Syamsudin, H.; Al-Zubaidi, S.; AKS, R.R.; Yusuf, E. Novel COVID-19 Detection and diagnosis system using iot based smart helmet. Int. J. Psychosoc. Rehabilit. 2020, 24, 2296–2303. [Google Scholar]
- Sun, G.; Matsui, T.; Kim, S.; Takei, O. KAZEKAMO: An infection screening system remote monitoring of multiple vital-signs for prevention of pandemic diseases. In Proceedings of the 2014 IEEE 3rd Global Conference on Consumer Electronics (GCCE); Institute of Electrical and Electronics Engineers (IEEE), Tokyo, Japan, 7–10 October 2014; pp. 225–226. [Google Scholar]
- Kumar, A.; Sharma, K.; Singh, H.; Naugriya, S.G.; Gill, S.S.; Buyya, R. A drone-based networked system and methods for combating coronavirus disease (COVID-19) pandemic. Futur. Gener. Comput. Syst. 2021, 115, 1–19. [Google Scholar] [CrossRef]
- Tsai, C.-Y.; Chang, N.-C.; Fang, H.-C.; Chen, Y.-C.; Lee, S.-S. A novel non-contact self-injection-locked radar for vital sign sensing and body movement monitoring in COVID-19 isolation ward. J. Med Syst. 2020, 44, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.; Nakayama, Y.; Dagdanpurev, S.; Abe, S.; Nishimura, H.; Kirimoto, T.; Matsui, T. Remote sensing of multiple vital signs using a CMOS camera-equipped infrared thermography system and its clinical application in rapidly screening patients with suspected infectious diseases. Int. J. Infect. Dis. 2017, 55, 113–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, V.; Staffa, E.; Mornstein, V.; Bourek, A. Infrared camera assessment of skin surface temperature–Effect of emissivity. Phys. Medica 2013, 29, 583–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, A.A.; Moreira, D.G.; Brito, C.J.; Da Silva, C.D.; Sillero-Quintana, M.; Pimenta, E.M.; Bach, A.J.; Garcia, E.S.; Marins, J.C.B. Validity of inner canthus temperature recorded by infrared thermography as a non-invasive surrogate measure for core temperature at rest, during exercise and recovery. J. Therm. Biol. 2016, 62, 50–55. [Google Scholar] [CrossRef]
- Perpetuini, D.; Cardone, D.; Filippini, C.; Chiarelli, A.M.; Merla, A. Modelling impulse response function of functional infrared imaging for general linear model analysis of autonomic activity. Sensors 2019, 19, 849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Formenti, D.; Ludwig, N.; Gargano, M.; Gondola, M.; Dellerma, N.; Caumo, A.; Alberti, G. Thermal imaging of exercise-associated skin temperature changes in trained and untrained female subjects. Ann. Biomed. Eng. 2012, 41, 863–871. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Pathology | Environment | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|
| Hewlett et al. [45] | Fever | Hospital | 0.70 | 0.92 | 0.42 | 0.97 |
| Chiu et al. [46] | Fever | Hospital | 0.75 | 1.00 | - | - |
| Bardou et al. [47] | Fever | Hospital | 0.93 | 1.00 | 0.87 | 1.00 |
| Nishiura and Kamiya [51] | H1N1 | Airport | 0.51–0.70 | 0.64–0.82 | - | - |
| Kuan et al. [52] | Dengue fever | Airport | - | - | 0.31–0.63 | - |
| Kuan and Chang [53] | Dengue fever | Airport | - | - | 0.24 | 1.00 |
| Sun et al. [56] | SARS | Airport | 1.00 | 0.88 | 0.33 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perpetuini, D.; Filippini, C.; Cardone, D.; Merla, A. An Overview of Thermal Infrared Imaging-Based Screenings during Pandemic Emergencies. Int. J. Environ. Res. Public Health 2021, 18, 3286. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063286
Perpetuini D, Filippini C, Cardone D, Merla A. An Overview of Thermal Infrared Imaging-Based Screenings during Pandemic Emergencies. International Journal of Environmental Research and Public Health. 2021; 18(6):3286. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063286
Chicago/Turabian StylePerpetuini, David, Chiara Filippini, Daniela Cardone, and Arcangelo Merla. 2021. "An Overview of Thermal Infrared Imaging-Based Screenings during Pandemic Emergencies" International Journal of Environmental Research and Public Health 18, no. 6: 3286. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063286