
Mental Health, Greenness, and Nature Related Behaviors in the Adult Population of Stockholm County during COVID-19-Related Restrictions

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
2.2. Exposure Assessment
Greenness Exposure
2.3. Other Variables
2.3.1. Walkability
2.3.2. Sociodemographic Variables
2.3.3. Frequency of Nature Visits
2.3.4. Alcohol Consumption
2.3.5. Physical Inactivity
2.4. Outcome Variables
2.4.1. RAND-36: Mental Health/Well-Being and Vitality Scores
2.4.2. SCL90: Core Depression and Anxiety Symptoms
2.4.3. Perceived Stress Scale-PSS
2.4.4. The Cognitive Stress Score
2.5. Statistics
3. Results
3.1. Descriptive Statistics, General
3.2. Frequency of Nature Visits Pre-Pandemic versus during the Pandemic
3.3. Alcohol Intake in the Study Population Pre-Pandemic resp. during the Pandemic
3.4. Sitting Score
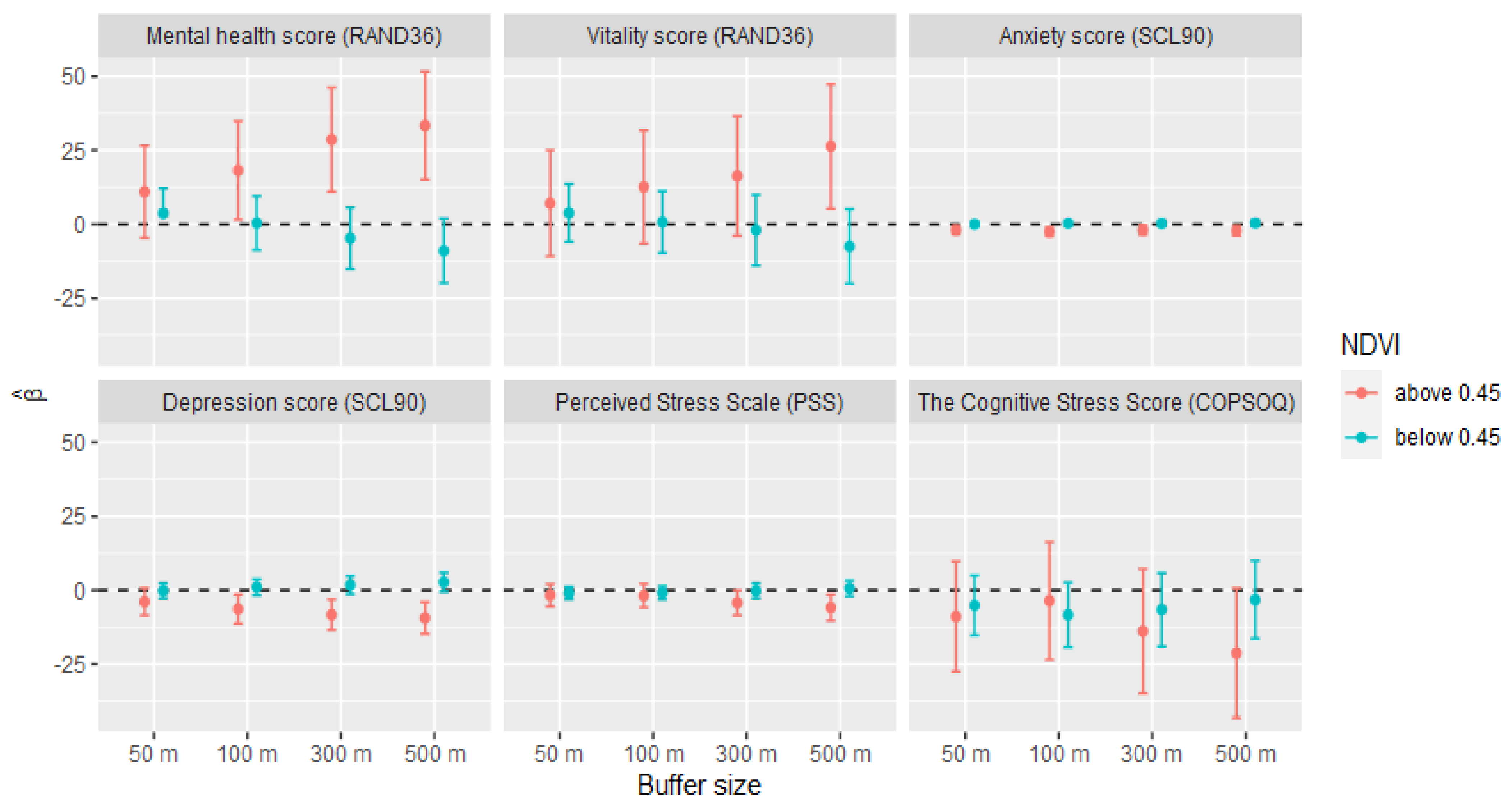
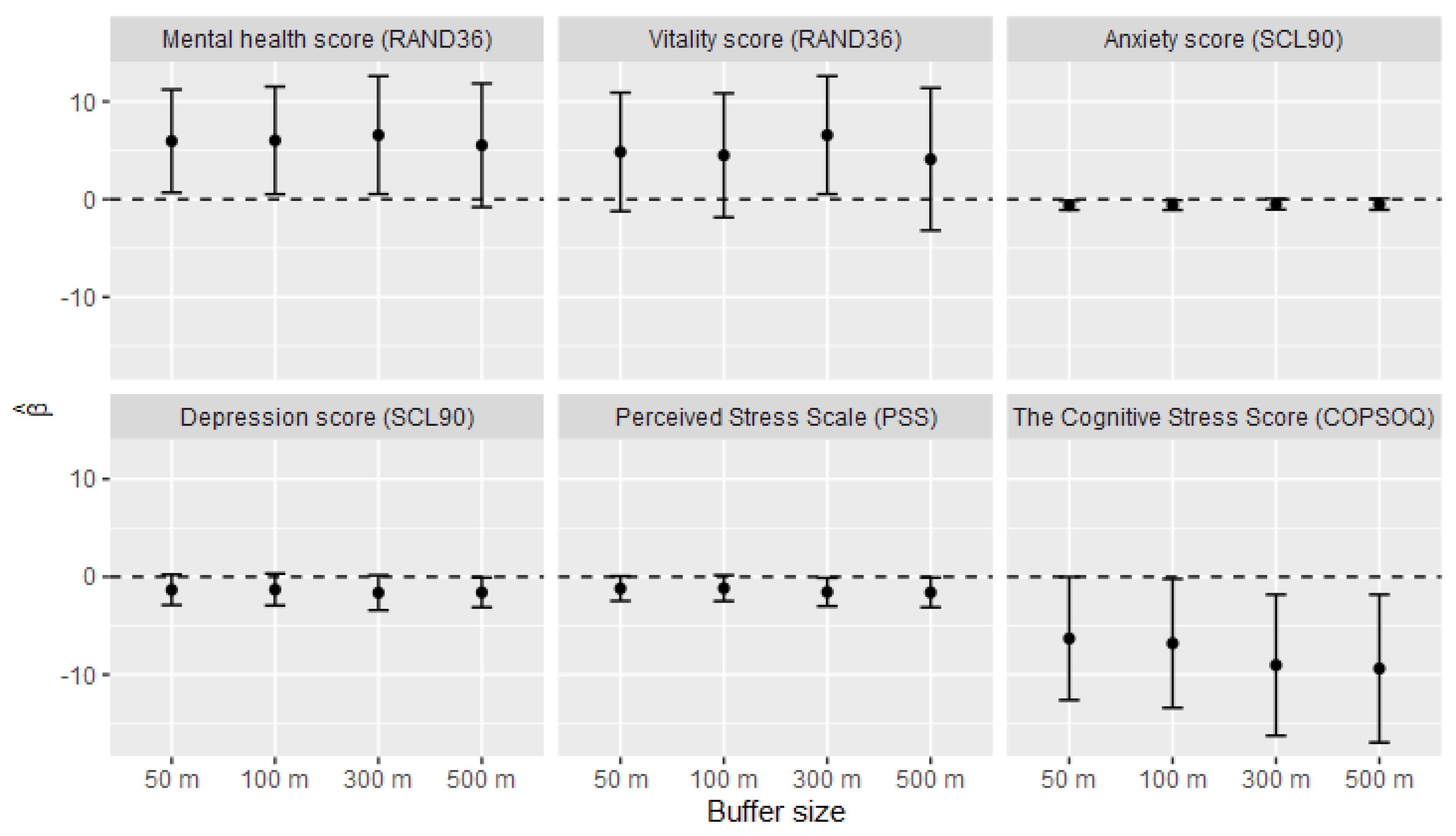
3.5. Associations between Normalized Difference Vegetation Index (NDVI) and the Mental Health Estimates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Douglas, M.; Katikireddi, S.V.; Taulbut, M.; McKee, M.; McCartney, G. Mitigating the wider health effects of COVID-19 pandemic response. BMJ 2020, 369, m1557. [Google Scholar] [CrossRef] [PubMed]
- Soga, M.; Evans, M.J.; Tsuchiya, K.; Fukano, Y. A room with a green view: The importance of nearby nature for mental health during the COVID-19 pandemic. Ecol. Appl. 2021, 31, e2248. [Google Scholar] [CrossRef]
- Baral, S.; Chandler, R.; Prieto, R.G.; Gupta, S.; Mishra, S.; Kulldorff, M. Leveraging epidemiological principles to evaluate Sweden’s COVID-19 response. Ann. Epidemiol. 2020, 54, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; North, C.S. Mental health and the Covid-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Centrum för Epidemiologi och Samhällsmedicin. Coronapandemin och Psykisk Hälsa-En Prognos om Kort- och Långsiktiga Effecter. Available online: https://ces.sll.se/globalassets/verksamheter/forskning-och-utveckling/centrum-for-epidemiologi-och-samhallsmedicin/folkhalsoguiden/rapporter-och-faktablad/coronapandemin-och-psykisk-halsa---en-prognos-om-kort--och-langsiktiga-effekter_uppdaterad-2020-04-28.pdf (accessed on 1 September 2020).
- Jennings, V.; Bamkole, O. The relationship between social cohesion and urban green space: An avenue for health promotion. Int. J. Environ. Res. Public Health 2019, 16, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SCB (Statistics Sweden). Fyra Procent är Socialt Isolerade. Available online: https://www.scb.se/hitta-statistik/artiklar/2019/fyra-procent-ar-socialt-isolerade2019 (accessed on 15 October 2020).
- Williams, S.E.; Braun, B. Loneliness and Social Isolation—A Private Problem, A Public Issue. J. Fam. Consum. Sci. 2019, 111, 7–14. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Lercher, P.; Browning, M.H.E.M.; Stoyanov, D.; Petrova, N.; Novakov, S.; Novakov, S.; Dimitrova, D.D. Does greenery experienced indoors and outdoors provide an escape and support mental health during the COVID-19 quarantine? Environ. Res. 2020, 2020, 110420. [Google Scholar] [CrossRef] [PubMed]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; De Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef] [Green Version]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [Green Version]
- Berman, M.G.; Kross, E.; Krpan, K.M.; Askren, M.K.; Burson, A.; Deldin, P.J.; Kaplan, S.; Sherdell, L.; Gotlib, I.H.; Jonides, J. Interacting with nature improves cognition and affect for individuals with depression. J. Affect. Disord. 2012, 140, 300–305. [Google Scholar] [CrossRef] [Green Version]
- Hartig, T.; Evans, G.W.; Jamner, L.D.; Davis, D.S.; Gärling, T. Tracking restoration in natural and urban field settings. J. Environ. Psychol. 2003, 23, 109–123. [Google Scholar] [CrossRef]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would you be happier living in a greener urban area? A fixed-effects analysis of panel data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Rugel, E.J.; Carpiano, R.M.; Henderson, S.B.; Brauer, M. Exposure to natural space, sense of community belonging, and adverse mental health outcomes across an urban region. Environ. Res. 2019, 171, 365–377. [Google Scholar] [CrossRef]
- Orban, E.; Sutcliffe, R.; Dragano, N.; Jöckel, K.-H.; Moebus, S. Residential Surrounding Greenness, Self-Rated Health and Interrelations with Aspects of Neighborhood Environment and Social Relations. J. Urban Health 2017, 94, 158–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, L.; Burls, A.; Townsend, M.; Ebden, M. Volunteering in nature as a way of enabling people to reintegrate into society. Perspect. Public Health 2010, 131, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Roe, J.; Aspinall, P.A. The restorative benefits of walking in urban and rural settings in adults with good and poor mental health. Health Place 2011, 17, 103–113. [Google Scholar] [CrossRef]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [Green Version]
- Wells, N.M.; Evans, G.W. Nearby nature a buffer of life stress among rural children. Environ. Behav. 2003, 35, 311–330. [Google Scholar] [CrossRef]
- Bratman, G.N.; Hamilton, J.P.; Daily, G.C. The impacts of nature experience on human cognitive function and mental health. Ann. N. Y. Acad. Sci. 2012, 1249, 118–136. [Google Scholar] [CrossRef] [PubMed]
- Wells, N.M. At home with nature effects of “greenness” on children’s cognitive functioning. Environ. Behav. 2000, 32, 775–795. [Google Scholar] [CrossRef] [Green Version]
- Zijlema, W.L.; Triguero-Mas, M.; Smith, G.; Cirach, M.; Martinez, D.; Dadvand, P.; Gascon, M.; Jones, M.; Gidlow, C.; Hurst, G.; et al. The relationship between natural outdoor environments and cognitive functioning and its mediators. Environ. Res. 2017, 155, 268–275. [Google Scholar] [CrossRef]
- Flouri, E.; Papachristou, E.; Midouhas, E. The role of neighbourhood greenspace in children’s spatial working memory. Br. J. Educ. Psychol. 2018, 89, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.F.; Kuo, F.E.; Sullivan, W.C. Views of nature and self-discipline: Evidence from inner city children. J. Environ. Psychol. 2002, 22, 49–63. [Google Scholar] [CrossRef] [Green Version]
- Dadvand, P.; Gascon, M.; Markevych, I. Green Spaces and Child Health and Development. Biodiversity and Health in the Face of Climate Change; Springer: Cham, Germany, 2019; pp. 121–130. [Google Scholar]
- Dadvand, P.; Nieuwenhuijsen, M.J.; Esnaola, M.; Forns, J.; Basagaña, X.; Alvarez-Pedrerol, M.; Rivas, I.; López-Vicente, M.; Pascual, M.d.; Su, J.; et al. Green spaces and cognitive development in primary schoolchildren. Proc. Natl. Acad. Sci. USA 2015, 112, 7937–7942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, M.; Barnes, M.; Jordan, C. Do experiences with nature promote learning? Converging evidence of a cause-and-effect relationship. Front. Psychol. 2019, 10, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenfors, C.U.; Van Hedger, S.C.; Schertz, K.E.; Meyer, F.A.; Smith, K.E.; Norman, G.J.; Bourrier, S.C.; Enns, J.T.; Kardan, O.; Jonides, J.; et al. Positive effects of nature on cognitive performance across multiple experiments: Test order but not affect modulates the cognitive effects. Front. Psychol. 2019, 10, 1413. [Google Scholar] [CrossRef] [Green Version]
- Pouso, S.; Borja, Á.; Fleming, L.E.; Gómez-Baggethun, E.; White, M.P.; Uyarra, M.C. Contact with blue-green spaces during the COVID-19 pandemic lockdown beneficial for mental health. Sci. Total Environ. 2020, 756, 143984. [Google Scholar] [CrossRef]
- Ulrich, R.S. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, R. The nature of the view from home: Psychological benefits. Environ. Behav. 2001, 33, 507–542. [Google Scholar] [CrossRef]
- Jo, H.; Song, C.; Miyazaki, Y. Physiological Benefits of Viewing Nature: A Systematic Review of Indoor Experiments. Int. J. Environ. Res. Public Health 2019, 16, 4739. [Google Scholar] [CrossRef] [Green Version]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and Health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.E.; Williams, K.J.; Sargent, L.D.; Williams, N.S.; Johnson, K.A. 40-second green roof views sustain attention: The role of micro-breaks in attention restoration. J. Environ. Psychol. 2015, 42, 182–189. [Google Scholar] [CrossRef]
- Li, D.; Sullivan, W.C. Impact of views to school landscapes on recovery from stress and mental fatigue. Landsc. Urban Plan. 2016, 148, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Gilchrist, K.; Brown, C.; Montarzino, A. Workplace settings and wellbeing: Greenspace use and views contribute to employee wellbeing at peri-urban business sites. Landsc. Urban Plan. 2015, 138, 32–40. [Google Scholar] [CrossRef]
- Benfield, J.A.; Rainbolt, G.N.; Bell, P.A.; Donovan, G.H. Classrooms with nature views: Evidence of differing student perceptions and behaviors. Environ. Behav. 2015, 47, 140–157. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.-C.; Oh, R.R.Y.; Nghiem, T.P.L.; Zhang, Y.; Tan, C.L.Y.; Lin, B.B.; Gaston, K.J.; Fuller, R.A.; Carrasco, L.R. Life satisfaction linked to the diversity of nature experiences and nature views from the window. Landsc. Urban Plan 2020, 202, 103874. [Google Scholar] [CrossRef]
- Sop Shin, W. The influence of forest view through a window on job satisfaction and job stress. Scand. J. For. Res. 2007, 22, 248–253. [Google Scholar] [CrossRef]
- Masoudinejad, S.; Hartig, T. Window View to the Sky as a Restorative Resource for Residents in Densely Populated Cities. Environ. Behav. 2018, 52, 401–436. [Google Scholar] [CrossRef]
- Soga, M.; Gaston, K.J.; Yamaura, Y. Gardening is beneficial for health: A meta-analysis. Prev. Med. Rep. 2017, 5, 92–99. [Google Scholar] [CrossRef]
- de Bell, S.; White, M.; Griffiths, A.; Darlow, A.; Taylor, T.; Wheeler, B.; Rebecca, L. Spending time in the garden is positively associated with health and wellbeing: Results from a national survey in England. Landsc. Urban Plan. 2020, 200, 103836. [Google Scholar] [CrossRef]
- Dennis, M.; James, P. Evaluating the relative influence on population health of domestic gardens and green space along a rural-urban gradient. Landsc. Urban Plan. 2017, 157, 343–351. [Google Scholar] [CrossRef] [Green Version]
- Björkman, L.-L. Fritidsodlingens Omfattning i Sverige. Alnarp. FritidsOdlingens Riksorganisation & Sveriges lantbruksuniversitet; 2012. Report No.: 918711707X Contract No.: 2012: 8. Available online: https://pub.epsilon.slu.se/8905/7/bjorkman_l_120516.pdf (accessed on 15 October 2020).
- Cervinka, R.; Schwab, M.; Schönbauer, R.; Hämmerle, I.; Pirgie, L.; Sudkamp, J. My garden–my mate? Perceived restorativeness of private gardens and its predictors. Urban For. Urban Green. 2016, 16, 182–187. [Google Scholar] [CrossRef]
- Howarth, M.; Brettle, A.; Hardman, M.; Maden, M. What is the evidence for the impact of gardens and gardening on health and well-being: A scoping review and evidence-based logic model to guide healthcare strategy decision making on the use of gardening approaches as a social prescription. BMJ Open 2020, 10, e036923. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Giessen, L.; Winkel, G. COVID-19-induced visitor boom reveals the importance of forests as critical infrastructure. For. Policy Econ. 2020, 118, 102253. [Google Scholar] [CrossRef]
- Venter, Z.S.; Barton, D.N.; Gundersen, V.; Figari, H.; Nowell, M. Urban nature in a time of crisis: Recreational use of green space increases during the COVID-19 outbreak in Oslo, Norway. Environ. Res. Lett. 2020, 15, 104075. [Google Scholar] [CrossRef]
- The Swedish Population Register. Available online: https://www.statenspersonadressregister.se (accessed on 15 October 2020).
- Allebeck, P.; Andreasson, S.; Wåhlin, S.; Ramstedt, M.; Gripenberg, J.; Damström-Thakker, K. Alkoholkonsumtion och Risknivåer. Kunskapsunderlag och Förslag till Rekommendationer; Centrum för Epidemiologi och Samhällsmedicin, Stockholms läns Landsting: Stockholm, Sweden, 2018. [Google Scholar]
- Andersson, A.M.; Bendtsen, P.; Spak, F. Riskbruk av alkohol. Lakartidningen 2010, 107, 1304–1306. [Google Scholar]
- Andréasson, S. Lågriskkonsumtion av alkohol–nu stöd för lägre gränser. Läkartidningen 2018, 115, FC4W. [Google Scholar]
- Wood, A.M.; Kaptoge, S.; Butterworth, A.S.; Willeit, P.; Warnakula, S.; Bolton, T.; Paige, E.; Paul, D.S.; Sweeting, M.; Burgess, S.; et al. Risk thresholds for alcohol consumption: Combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies. Lancet 2018, 391, 1513–1523. [Google Scholar] [CrossRef] [Green Version]
- Niemelä, O.; Nivukoski, U.; Bloigu, A.; Bloigu, R.; Aalto, M.; Laatikainen, T. Laboratory test based assessment of WHO alcohol risk drinking levels. Scand. J. Clin. Lab. Investig. 2019, 79, 58–64. [Google Scholar] [CrossRef]
- Studenthälsans Alkoholtestportal. Sammanställning av Alkoholvaneundersökning Linköpings Universitet. 2009. Available online: https://www.student.liu.se/studentstod/studenthalsan/Alkoholvanetest/1.199111/AlkoholvanetestResultattermin1ht-09.pdf (accessed on 12 December 2020).
- Hays, R.D.; Morales, L.S. The RAND-36 measure of health-related quality of life. Ann. Med. 2001, 33, 350–357. [Google Scholar] [CrossRef]
- Lundin, A.; Hallgren, M.; Forsell, Y. The validity of the symptom checklist depression and anxiety subscales: A general population study in Sweden. J. Affect. Disord. 2015, 183, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Magnusson Hanson, L.L.; Westerlund, H.; Leineweber, C.; Rugulies, R.; Osika, W.; Theorell, T.; Bech, P. The Symptom Checklist-core depression (SCL-CD6) scale: Psychometric properties of a brief six item scale for the assessment of depression. Scand. J. Public Health 2014, 42, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S. Perceived stress in a probability sample of the United States. In The Claremont Symposium on Applied Social Psychology the Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage Publications, Inc.: Newbury Park, CA, USA, 1988; pp. 31–67. [Google Scholar]
- Vallejo, M.A.; Vallejo-Slocker, L.; Fernández-Abascal, E.G.; Mañanes, G. Determining Factors for Stress Perception Assessed with the Perceived Stress Scale (PSS-4) in Spanish and Other European Samples. Front. Psychol. 2018, 9, 37. [Google Scholar] [CrossRef]
- Setterlind, S.; Larsson, G. The stress profile: A psychosocial approach to measuring stress. Stress Med. 1995, 11, 85–92. [Google Scholar] [CrossRef]
- Stenfors, C.U.D.; Hanson, L.M.; Oxenstierna, G.; Theorell, T.; Nilsson, L.-G. Psychosocial Working Conditions and Cognitive Complaints among Swedish Employees. PLoS ONE 2013, 8, e60637. [Google Scholar] [CrossRef] [Green Version]
- Stenfors, C.U.D.; Marklund, P.; Hanson, L.L.M.; Theorell, T.; Nilsson, L.-G. Subjective Cognitive Complaints and the Role of Executive Cognitive Functioning in the Working Population: A Case-Control Study. PLoS ONE 2013, 8, e83351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrell, F.E., Jr. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis; Springer: New York, NY, USA, 2015. [Google Scholar]
- Engberg, I.; Segerstedt, J.; Waller, G.; Wennberg, P.; Eliasson, M. Fatigue in the general population- associations to age, sex, socioeconomic status, physical activity, sitting time and self-rated health: The northern Sweden MONICA study 2014. BMC Public Health 2017, 17, 654. [Google Scholar] [CrossRef] [Green Version]
- Tinghög, P.; Hemmingsson, T.; Lundberg, I. To what extent may the association between immigrant status and mental illness be explained by socioeconomic factors? Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 990–996. [Google Scholar] [CrossRef]
- Mossakowski, K.N. Dissecting the Influence of Race, Ethnicity, and Socioeconomic Status on Mental Health in Young Adulthood. Res. Aging 2008, 30, 649–671. [Google Scholar] [CrossRef]
- De Vries, S.; Buijs, A.E.; Snep, R.P. Environmental Justice in The Netherlands: Presence and Quality of Greenspace Differ by Socioeconomic Status of Neighbourhoods. Sustainability 2020, 12, 5889. [Google Scholar] [CrossRef]
- Mears, M.; Brindley, P.; Maheswaran, R.; Jorgensen, A. Understanding the socioeconomic equity of publicly accessible greenspace distribution: The example of Sheffield, UK. Geoforum 2019, 103, 126–137. [Google Scholar] [CrossRef]
- Persson, Å.; Eriksson, C.; Lõhmus, M. Inverse associations between neighborhood socioeconomic factors and green structure in urban and suburban municipalities of Stockholm County. Landsc. Urban Plan. 2018, 179, 103–106. [Google Scholar] [CrossRef]
- Buheji, M.; Jahrami, H.; Dhahi, A. Minimizing stress exposure during pandemics similar to COVID-19. PBSIJ 2020, 10, 9–16. [Google Scholar]
- Ramalho, R. Alcohol consumption and alcohol-related problems during the COVID-19 pandemic: A narrative review. Australas. Psychiatry 2020, 28, 524–526. [Google Scholar] [CrossRef]
- Rehm, J.; Kilian, C.; Ferreira-Borges, C.; Jernigan, D.; Monteiro, M.; Parry, C.D.; Sanchez, Z.M.; Manthey, J. Alcohol use in times of the COVID 19: Implications for monitoring and policy. Drug Alcohol Rev. 2020, 39, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Clay, J.M.; Parker, O.M. Alcohol use and misuse during the COVID-19 pandemic: A potential public health crisis? Lancet Public Health 2020, 5, e259. [Google Scholar] [CrossRef]
- Wang, Y.; Di, Y.; Ye, J.; Wei, W. Study on the public psychological states and its related factors during the outbreak of coronavirus disease 2019 (COVID-19) in some regions of China. Psychology Health Med. 2021, 26, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Connolly, C.; Keil, R.; Ali, S.H. Extended urbanisation and the spatialities of infectious disease: Demographic change, infrastructure and governance. Urban Stud. 2021, 58, 245–263. [Google Scholar] [CrossRef]
- Cox, D.T.; Shanahan, D.F.; Hudson, H.L.; Fuller, R.A.; Gaston, K.J. The impact of urbanisation on nature dose and the implications for human health. Landsc. Urban Plan. 2018, 179, 72–80. [Google Scholar] [CrossRef]
- White, M.P.; Pahl, S.; Wheeler, B.W.; Depledge, M.H.; Fleming, L.E. Natural environments and subjective wellbeing: Different types of exposure are associated with different aspects of wellbeing. Health Place 2017, 45, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, B.D.S.; White, M.P.; Clitherow, T.J. Nearby Nature ‘Buffers’ the Effect of Low Social Connectedness on Adult Subjective Wellbeing over the Last 7 Days. Int. J. Environ. Res. Public Health 2018, 15, 1238. [Google Scholar] [CrossRef] [Green Version]
- Länstyrelsen Jämtlands Län. Ökad Vistelse i Naturen under Pandemin. 2020. Available online: https://www.lansstyrelsen.se/jamtland/om-oss/nyheter-och-press/nyheter---jamtland/2020-12-02-okad-vistelse-i-naturen-under-pandemin.html (accessed on 18 March 2021).
- svt NYHETER. Rekordmånga Besökte den Svenska Naturen. 2020. Available online: https://www.svt.se/nyheter/lokalt/ost/pandemin-lockar-manga-ut-i-naturen (accessed on 18 March 2021).
- Aftonbladet. Vår Nya Vurm för Skog och Mark Utmanar Nature. 2020. Available online: https://www.aftonbladet.se/nyheter/a/2dv4QG/var-nya-vurm-for-skog-och-mark-utmanar-naturen (accessed on 18 March 2021).


{kind=link}
{kind=link}
| Variable Name | NDVI Low | NDVI High | p-Value |
|---|---|---|---|
| N (%) | N (%) | ||
| Sex | 0.232 | ||
| Females | 583 (51) | 556 (49) | |
| Males | 447 (49) | 474 (51) | |
| Age group | 0.865 | ||
| <70 years | 842 (50) | 839 (50) | |
| ≥70 years | 188 (49) | 192 (51) | |
| Educational level | 0.000 | ||
| Primary education | 42 (37) | 71 (63) | |
| Secondary education | 247 (45) | 307 (55) | |
| Higher education | 734 (53) | 644 (47) | |
| Income | 0.000 | ||
| <225 tSEK | 111 (40) | 169 (60) | |
| 225–450 tSEK | 304 (45) | 377 (55) | |
| >450 tSEK | 600 (56) | 467 (44) | |
| Country of Birth | 0.019 | ||
| SSB * | 897 (49) | 930 (51) | |
| All other countries | 127 (57) | 94 (43) | |
| Alcohol consumption | 0.019 | ||
| Below risk | 831 (48) | 885 (52) | |
| Above risk | 183 (57) | 136 (43) | |
| Walkability | 0.000 | ||
| Low | 243 (38) | 397 (62) | |
| Average | 323 (48) | 349 (52) | |
| High | 454 (63) | 270 (37) | |
| Sitting score | 0.017 | ||
| Low | 324 (47) | 371 (53) | |
| Average | 338 (49) | 356 (51) | |
| High | 333 (54) | 280 (46) | |
| Frequency of nature visits | 0.020 | ||
| Often | 792 (49) | 835 (51) | |
| Seldom | 238 (55) | 195 (45) |
| Population | Before COVID-19 | During COVID-19 | Difference | ||
|---|---|---|---|---|---|
| n | % (95% CI) | % (95% CI) | % (95% CI) | ||
| Total | 2059 | 65.98 (64.27; 67.69) | 79.02 (77.26; 80.78) | +13.04 (14.77; 11.31) * | |
| Age | <70 years | 1680 | 63.43 (61.52; 65.34) | 77.56 (75.56; 79.56) | +14.13 (16.08; 12.18) * |
| ≥70 years | 379 | 77.31 (73.71; 80.9) | 85.49 (81.93; 89.05) | +8.18 (11.83; 4.53) * | |
| Sex | men | 920 | 62.25 (59.58; 64.92) | 73.91 (71.07; 76.76) | +11.66 (14.21; 9.11) * |
| women | 1139 | 69 (66.8; 71.19) | 83.14 (80.97; 85.32) | +14.15 (16.5; 11.79) * | |
| Education | primary | 113 | 67.89 (60.06; 75.71) | 71.68 (63.25; 80.12) | +3.79 (10.66; −3.08) |
| secondary | 554 | 64.7 (61.32; 68.07) | 75.63 (72.05; 79.22) | +10.93 (14.3; 7.56) * | |
| higher | 1378 | 66.54 (64.48; 68.59) | 81.06 (78.99; 83.13) | +14.52 (16.64; 12.41) * | |
| Ethnic origin | born in SSB 1 | 1806 | 67.32 (65.51; 69.14) | 80.95 (79.14; 82.77) | +13.63 (15.42; 11.84) * |
| not born in SSB 1 | 221 | 55.87 (50.82; 60.91) | 64.23 (58.2; 70.26) | +8.36 (14.39; 2.34) * | |
| both or one of the parents from SSB 1 | 1806 | 67.32 (65.51; 69.14) | 80.95 (79.14; 82.77) | +13.63 (15.42; 11.84) * | |
| neither mother nor father from SSB 1 | 246 | 55.87 (50.82; 60.91) | 64.23 (58.2; 70.26) | +8.36 (14.39; 2.34) * | |
| Residential area walkability | Poor (lowest tertial) | 640 | 64.87 (61.8; 67.93) | 80.31 (77.22; 83.4) | +15.45 (18.64; 12.26) * |
| Good (2nd tertial) | 672 | 65.99 (63; 68.97) | 78.87 (75.77; 81.96) | +12.88 (15.91; 9.85) * | |
| Very Good (highest tertial) | 724 | 66.63 (63.72; 69.54) | 77.9 (74.87; 80.93) | +11.27 (14.12; 8.41) * | |
| Residential NDVI within a 50 m buffer | Low NDVI (0.236–0.343) | 687 | 64.82 (61.83; 67.8) | 76.42 (73.24; 79.6) | +11.6 (14.74; 8.46) * |
| Average NDVI (0.344–0.431) | 686 | 65.54 (62.51; 68.56) | 79.3 (76.26; 82.34) | +13.77 (16.75; 10.78) * | |
| High NDVI (0.5–0.559) | 686 | 67.6 (64.71; 70.48) | 81.34 (78.42; 84.26) | +13.74 (16.61; 10.88) * | |
| Before COVID-19 | During COVID-19 | Difference between before and during COVID-19 | ||
|---|---|---|---|---|
| n = 1928 | % | % | p< | Direction |
| To be in the fresh air | 80.0 | 80.3 | 0.716 | - |
| To recover from stress | 36.0 | 33.8 | 0.028 | ↓ |
| For physical activity | 69.7 | 72.1 | 0.028 | ↑ |
| To experience silence/nature sounds | 45.9 | 38.8 | 0.001 | ↓ |
| For social reasons | 22.0 | 21.3 | 0.456 | - |
| To see other people | 11.9 | 14.6 | 0.001 | ↑ |
| To walk my dog (or other pet) | 12.8 | 12.8 | 0.317 | - |
| To relax | 62.4 | 52.5 | 0.001 | ↓ |
| To enjoy the beauty of nature | 64.8 | 58.7 | 0.001 | ↓ |
| To be alone | 18.6 | 15.7 | 0.001 | ↓ |
| For spiritual experiences | 8.5 | 8.7 | 0.651 | - |
| Because somebody else told me to do that | 3.2 | 3.6 | 0.225 | - |
| Because it is good for my health | 68.8 | 72.5 | 0.001 | ↑ |
| To clear my head/think clearly | 37.1 | 35.0 | 0.016 | ↓ |
| Because my work requires it | 3.1 | 3.4 | 0.331 | - |
| Because it’s part of my regular transportation route | 10.5 | 8.0 | 0.001 | ↓ |
| Before COVID-19 | During COVID-19 | Difference between before and during COVID-19 | ||
|---|---|---|---|---|
| n = 1928 | % | % | p< | Direction |
| Private garden | 40.0 | 41.3 | 0.046 | ↑ |
| Park | 43.7 | 39.8 | 0.016 | ↓ |
| Forest | 51.5 | 52.6 | 0.274 | - |
| Freshwater bodies of water | 41.8 | 39.6 | 0.020 | ↓ |
| Saltwater beach/boating | 16.8 | 15.5 | 0.020 | ↓ |
| Nature reserve | 27.0 | 29.3 | 0.003 | ↑ |
| Green play parks | 15.6 | 14.2 | 0.039 | ↓ |
| Mean Weekly Consumption (In Glasses) | Difference between before and during COVID-19 | Individuals above the Low Risk Level (%) * | Difference between before and during COVID-19 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Before COVID-19 | During COVID-19 | p | Direction | Before COVID-19 | During COVID-19 | p | Direction | |
| Total | 2025 | 3.83 | 3.95 | 0.022 | ↑ | 13.80 | 15.70 | 0.000 | ↑ |
| Sex | |||||||||
| Men | 903 | 4.48 | 4.66 | 0.036 | ↑ | 7.60 | 9.90 | 0.001 | ↑ |
| Women | 1122 | 3.32 | 3.38 | 0.276 | - | 18.80 | 20.40 | 0.034 | ↑ |
| Age group | |||||||||
| <70 years | 1658 | 3.67 | 3.79 | 0.005 | ↑ | 13.30 | 15.10 | 0.002 | ↑ |
| ≥70 years | 367 | 4.55 | 4.71 | 0.180 | - | 16.30 | 18.40 | 0.032 | ↑ |
| Education | |||||||||
| primary | 110 | 3.81 | 2.64 | 0.436 | - | 14.40 | 13.50 | 0.320 | - |
| secondary | 546 | 3.97 | 4.03 | 0.554 | - | 12.30 | 15.60 | 0.001 | ↑ |
| higher | 1122 | 3.76 | 3.93 | 0.008 | ↑ | 14.30 | 15.90 | 0.014 | ↑ |
| Subgroup | n | Mean Sitting Score | Between Period Difference | |||
|---|---|---|---|---|---|---|
| Before COVID-19 | During COVID-19 | Difference | p< | Direction | ||
| Sex | ||||||
| men | 889 | 6.7 | 7.3 | 0.6 | 0.001 | ↑ |
| women | 1111 | 6.6 | 7.1 | 0.5 | 0.001 | ↑ |
| Age group | ||||||
| <70 years | 1642 | 6.9 | 7.5 | 0.5 | 0.001 | ↑ |
| ≥70 years | 345 | 5.4 | 5.9 | 0.5 | 0.001 | ↑ |
| Country of birth | ||||||
| SSB | 1780 | 6.7 | 7.2 | 0.5 | 0.001 | ↑ |
| outside SSB | 214 | 6.7 | 7.4 | 0.7 | 0.001 | ↑ |
| Education | ||||||
| primary | 105 | 5.1 | 5.8 | 0.7 | 0.006 | ↑ |
| secondary | 537 | 6.4 | 7.0 | 0.6 | 0.001 | ↑ |
| higher | 1350 | 6.9 | 7.4 | 0.5 | 0.001 | ↑ |
| Neighborhood walkability (tertials) | ||||||
| poor | 628 | 6.6 | 7.2 | 0.6 | 0.001 | ↑ |
| good | 656 | 6.6 | 7.2 | 0.5 | 0.001 | ↑ |
| very good | 704 | 6.7 | 7.2 | 0.5 | 0.001 | ↑ |
| NDVI within 50 m | ||||||
| low (0–0.29) | 373 | 6.6 | 7.2 | 0.5 | 0.001 | ↑ |
| average (0.3–0.49) | 901 | 6.8 | 7.3 | 0.5 | 0.001 | ↑ |
| high (0.5–1) | 726 | 6.5 | 7.0 | 0.5 | 0.001 | ↑ |
| Mental Health Estimate | Average Score (CI 95%) at below Median NDVI | Average Score (CI 95%) at above Median NDVI | p< | Cronbach’s Alpha * |
|---|---|---|---|---|
| Mental health score (RAND36) | 71.82 (70.735; 72.905) | 73.007 (71.949; 74.065) | 0.124 | 0.833 |
| Vitality score (RAND36) | 60.093 (58.839; 61.347) | 61.116 (59.864; 62.368) | 0.257 | 0.833 |
| Anxiety score (SCL90) | 1.231 (1.129; 1.333) | 1.115 (1.023; 1.206) | 0.096 | N/A ** |
| Depression score (SCL90) | 5.906 (5.58; 6.232) | 5.68 (5.377; 5.984) | 0.320 | 0.900 |
| Perceived Stress Scale (PSS) | 8.732 (8.469; 8.996) | 8.477 (8.229; 8.724) | 0.166 | 0.755 |
| The Cognitive Stress Score (COPSOQ) | 31.55 (30.279; 32.821) | 30.626 (29.352; 31.901) | 0.314 | 0.888 |
| Variable Name | Mental Health Score (RAND36) | Vitality (RAND36) | Anxiety Score (SCL90) | Depression Score (SCL90) | Perceived Stress Scale (PSS) | The Cognitive Stress Score (COPSOQ) |
|---|---|---|---|---|---|---|
| β (95% CI) | ||||||
| NDVI 50 m | 5.951 (0.688; 11.213) * | 4.842 (−1.219; 10.902) | −0.615 (−1.095; −0.136) * | −1.331 (−2.889; 0.227) | −1.202 (−2.465; 0.061) | −6.307 (−12.604; −0.01) * |
| Walkability | 0.199 (0.136; 0.261) * | 0.222 (0.15; 0.294) * | −0.016 (−0.021; −0.01) * | −0.056 (−0.074; −0.037) * | −0.042 (−0.057; −0.027) * | −0.149 (−0.224; −0.074) * |
| Sex | ||||||
| male | ref. | ref. | ref. | ref. | ref. | ref. |
| female | −2.419 (−3.92; −0.919) * | −2.44 (−4.168; −0.711) * | 0.146 (0.009; 0.283) * | 0.461 (0.016; 0.905) * | 0.586 (0.225; 0.946) * | 3.033 (1.236; 4.83) * |
| Age | 0.253 (0.203; 0.303) * | 0.303 (0.246; 0.361) * | −0.024 (−0.029; −0.019) * | −0.066 (−0.081; −0.051) * | −0.069 (−0.081; −0.057) * | −0.309 (−0.369; −0.249) * |
| Annual Income | 1.548 (1.1; 1.995) * | 1.448 (0.933; 1.964) * | −0.156 (−0.197; −0.115) * | −0.55 (−0.682; −0.417) * | −0.249 (−0.357; −0.141) * | −1.735 (−2.271; −1.199) * |
| Physical inactivity | −0.554 (−0.791; −0.317) * | −0.952 (−1.225; −0.68) * | 0.04 (0.018; 0.061) * | 0.204 (0.133; 0.274) * | 0.065 (0.008; 0.122) * | 0.577 (0.294; 0.86) * |
| Frequency of nature visits | ||||||
| seldom | ref. | ref. | ref. | ref. | ref. | ref. |
| often | 3.638 (1.811; 5.466) * | 6.685 (4.581; 8.79) * | −0.157 (−0.323; 0.01) | −1.004 (−1.545; −0.464) * | −0.617 (−1.055; −0.178) * | −2.6 (−4.784; −0.417) * |
| Place of birth | ||||||
| Sweden | ref. | ref. | ref. | ref. | ref. | ref. |
| other SBC | 1.577 (−1.975; 5.129) | 2.351 (−1.739; 6.442) | 0.03 (−0.294; 0.354) | −0.714 (−1.766; 0.338) | 0.007 (−0.852; 0.865) | −2.854 (−7.109; 1.4) |
| rest of the Europe | −4.415 (−7.861; −0.97) * | −3.159 (−7.126; 0.809) | 0.457 (0.144; 0.769) * | 0.465 (−0.55; 1.481) | 1.578 (0.746; 2.41) * | 2.726 (−1.379; 6.831) |
| rest of the world | −2.963 (−6.159; 0.233) | −2.907 (−6.587; 0.774) | 0.397 (0.105; 0.688) * | 0.515 (−0.432; 1.461) | 1.148 (0.383; 1.912) * | 0.731 (−3.097; 4.558) |
| Alcohol consumption | ||||||
| below the risk level | ref. | ref. | ref. | ref. | ref. | ref. |
| above the risk level | −3.09 (−5.105; −1.076) * | −3.449 (−5.769; −1.129) * | 0.155 (−0.029; 0.338) | 1.018 (0.421; 1.615) * | 0.663 (0.178; 1.148) * | 1.459 (−0.957; 3.874) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lõhmus, M.; Stenfors, C.U.D.; Lind, T.; Lauber, A.; Georgelis, A. Mental Health, Greenness, and Nature Related Behaviors in the Adult Population of Stockholm County during COVID-19-Related Restrictions. Int. J. Environ. Res. Public Health 2021, 18, 3303. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063303
Lõhmus M, Stenfors CUD, Lind T, Lauber A, Georgelis A. Mental Health, Greenness, and Nature Related Behaviors in the Adult Population of Stockholm County during COVID-19-Related Restrictions. International Journal of Environmental Research and Public Health. 2021; 18(6):3303. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063303
Chicago/Turabian StyleLõhmus, Mare, Cecilia U. D. Stenfors, Tomas Lind, André Lauber, and Antonios Georgelis. 2021. "Mental Health, Greenness, and Nature Related Behaviors in the Adult Population of Stockholm County during COVID-19-Related Restrictions" International Journal of Environmental Research and Public Health 18, no. 6: 3303. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063303