
Neurophysiological Approach by Self-Control of Your Stress-Related Autonomic Nervous System with Depression, Stress and Anxiety Patients



Abstract
:1. Introduction
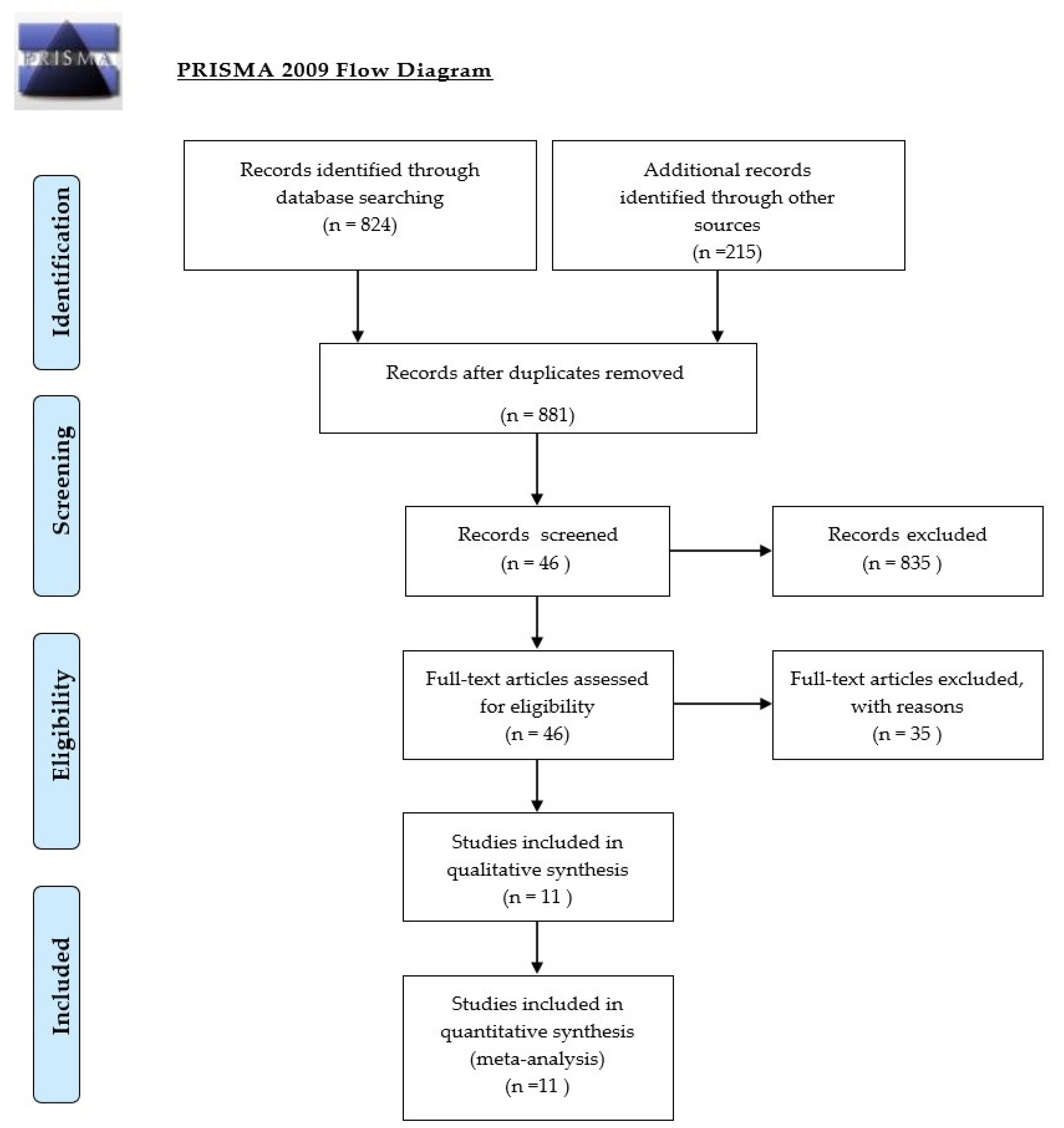
2. Method
3. Results
3.1. HRVB as Additional Treatment of Depression
3.2. HRVB as Additional Treatment of PTSD
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Taskforce of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart Rate Variability, Standards of measurement, physiological interpretation and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Lin, I.M.; Fan, S.Y.; Lu, H.C.; Lin, T.H.; Chu, C.S.; Kuo, H.F.; Lee, C.S.; Lu, Y.H. Randomized contolled trial of heart rate variability biofeedback in cardiac autonomic and hostility among patients with coronary artery disease. Behav. Res. Ther. 2015, 70, 38–46. [Google Scholar] [CrossRef]
- Agelink, M.; Boz, C.; Ullrich, J. Relationship between major depressive disorder and heart rate variability. Clinical consequences and implications for antidepressive treatment. Psychiatry Res. 2002, 113, 139–149. [Google Scholar] [CrossRef]
- Berntson, G.G.; Bigger, J.T.; Eckberg, D.L.; Grossman, P. HRV: Origins, methods and interpretive caveats. J. Psychophysiol. 1997, 34, 623–648. [Google Scholar] [CrossRef] [PubMed]
- Gevirtz, R.; Lehrer, P. Resonance frequency heart rate feedback. In Biofeedback, a Practitioner’s Guide, 3rd ed.; Schwartz, M.S., Andrasik, F., Eds.; Guilford: New York, NY, USA, 2003; pp. 245–264. [Google Scholar]
- Porges, S.W. The Polyvagal Theory; Neuropsychological Foundations of Emotions, Attachment, Communication and Selfregulation; Norton: New York, NY, USA; London, UK, 2011. [Google Scholar]
- Blase, K.; van Dijke, A.; Cluitmans, P.; Vermetten, E. Effectiviteit van hartritme variabiliteit biofeedback als aanvulling bij behandeling van depressie en posttraumatische stressstoornis. Tijdschr. Voor Psychiatr. 2016, 4, 293–300. [Google Scholar]
- Gevirtz, R. Autonomic nervous system markers for psychophysiological, anxiety and physical disorders. Integr. Neurosci. Pers. Med. 2010, 164–180. [Google Scholar]
- Gevirtz, R. The promise of Heart Rate Variability Biofeedback: Evidence-based application. Biofeedback 2013, 41, 110–120. [Google Scholar] [CrossRef] [Green Version]
- Sloan, R.; Shapiro, P.A.; Gorenstein, E.E.; Tager, F.A.; Monk, C.E.; McKinley, P.S.; Myers, M.M.; Bagiella, E.; Chen, I.; Steinman, R.; et al. Cardiac autonomic control and treatment of hostility: A randomized contolled trial. Psychosom. Med. 2010, 72, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.L.; Huang, C.Y.; Shiu, S.P.; Yeh, S.H. Effects of yoga on stress, stress adaptation and Heart Rate Variability among mental health professionals. Worldviews Evid. Based Nurs. 2015, 12, 236–245. [Google Scholar] [CrossRef]
- Chalmers, J.A.; Quintana, D.S.; Abbott, M.J.; Kemp, A.H. Anxiety disorders are associated with reduced heart rate variability. Front. Psychiatry 2014, 5, 80. [Google Scholar] [CrossRef] [Green Version]
- Larkey, L.; Kim, W.; James, D. Mind-body and psychosocial interventions may similarly affect Heart Rate Variability patterns in cancer recovery. Integr. Cancer Ther. 2019, 19, 1–10. [Google Scholar]
- Blase, K.; van Waning, A. Heart Rate Variability, cortisol and attention focus during Shamatha quiescence meditation. Appl. Psychophysiol. Biofeedback 2019, 44, 331–342. [Google Scholar] [CrossRef]
- Kiviniemi, A.M.; Hautala, A.J.; Kinnunen, H.; Nissilä, J.; Virtanen, P.; Karjalainen, J.; Tulppo, M.P. Daily exercise prescription on the basis of HRV among men and women (Randomied Controlled Trial). Med. Sci. Sports Exerc. 2010, 42, 1355–1363. [Google Scholar] [CrossRef]
- Prinsloo, G.; Derman, W.; Lambert, M.; Rauch, H. The effect of a single session of short duration biofeedback induced deep breathing on measures of HRV during laboratory induced cognitive stress. Appl. Psychophysiol. Biofeedback 2013, 38, 81–90. [Google Scholar] [CrossRef]
- Lewis, G.; Hourani, L.; Tueller, S.; Weimer, B. Relaxation training assisted by HRVB: Implication for a military predeployment stress inoculation protocol. Psychophysiology 2015, 52, 1167–1174. [Google Scholar] [CrossRef]
- Goessl, V.; Curtiss, J.; Hofmann, S. The effect of HRV biofeedback training on stress and anxiety: A meta-analysis. Psychol. Med. 2017, 47, 2578–2586. [Google Scholar] [CrossRef]
- Lehrer, P.; Gevirtz, R. Heart Rate Variability biofeedback: How and why does it work? Front. Psychol. 2014, 5, 756. [Google Scholar] [CrossRef] [Green Version]
- Carney, R.M.; Freedland, K.E.; Skala, E.A.; Jaffe, A.S. Change in heart rate and heart rate variability during treatment for depression in patients with coronary heart disease. Psychosom Med. 2000, 62, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.J.; Benjamin, J.; Matar, M.A.; Kaplan, Z. Autonomic dysregulation in panic disorder and in posttraumatic stress disorder: Application of power spectrum analysis of heart rate variability at rest and in response to recollection of trauma or attacks. Psychiatry Res. 2000, 96, 1–13. [Google Scholar] [CrossRef]
- Porges, S.W.; Dana, D.A. Clinical Applications of the Polyvagal Theory: The Emergence of Polyvagal-Informed Therapies; Norton Series on Interpersonal Neurobiology; WW Norton & Company: New York, NY, USA, 2018. [Google Scholar]
- Van der Kolk, B. Clinical Implications of Neuroscience Research in PTSD. Psychobiology of Posttraumatic Stress Disorders; Annals of the New York Academy of Sciences; Blackwell Publishing: Oxford, UK, 2006; Volume 1071, pp. 277–293. [Google Scholar]
- Lanius, R.; Vermetten, E.; Pain, C. The Hidden Epidemic; the Impact of Early Life Trauma on Health and Disease; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Licht, C.; de Geus, E.; Zitman, F.; Hoogendijk, W.; van Dijck Penninx, B. Association between major depression disorder and HRV in the Netherlands Study of Depression and Anxiety (NESDA). Arch. Gen. Psychiatry 2008, 65, 1358–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sgoifo, A.; Carnevali, I.; Alfonso, M.; Amore, M. Autonomic dysfunction and heart rate variability in depression. Stress 2015, 18, 343–352. [Google Scholar] [CrossRef]
- GRADE Working Group. Grading quality of evidence and strength of recommandations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [Green Version]
- Zucker, T.L.; Samuelson, K.W.; Muench, F.; Gevirtz, R.N. The effects of respiratory sinus arrhythmia biofeedback on heart rate variability and posttraumatic stress disorder symptoms. Appl. Psychophysiol. Biofeedback 2009, 34, 135–143. [Google Scholar] [CrossRef]
- Tan, G.; Dao, T.K.; Farmer, L.; Sutherland, R.J.; Gevirtz, R. Heart Rate Variability and Posttraumatic Stress Disorder: A pilot study. Appl. Psychophysiol. Biofeedback 2011, 36, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Rene, R. The efficacy of a portable HRV feedback device in conjunction with mental health treatment of clients with major depressive disorder enrolled in a country welfare-to-work program. Diss. Abstr. Int. Sect. B Sci. Eng. 2008, 69, 2000. [Google Scholar]
- Chaudhri, P. The Effects of Cardiorespiratory Biofeedback and Dialectical Behavioral Skills Training with Sertraline on Post Myocardial Infarction Major Depression and Low Heart Rate Variability; Alliant University: San Diego, CA, USA, 2008. [Google Scholar]
- Patron, E.; Benvenutti, G.F.; Palomba, D. Biofeedback assisted control of RSA as a biobehavioral intervention for depressive symptoms in patients after cardiac surgery: A preliminary study. Appl. Psychophysiol. Biof. 2013, 38, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Van der Zwan, J.; Huizink, A.; Lehrer, P.; Koot, H.; Vente, W. The effect of Heart Rate Variability Biofeedback training on mental health of pregnant and non-pregnant women: A randomized contolled trial. Int. J. Environ. Res. Public Health 2019, 16, 1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karavidas, M.; Lehrer, P.; Vaschillo, E.; Vaschillo, B.; Marin, H.; Buyske, S. Preliminary results of an open label study of heart rate variability biofeedback for the treatment of major depression. Appl. Psychophysiol. Biofeedback 2007, 32, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Siepman, M.; Aykac, V.; Unterdorfer, J.; Mueck-Weymann, M. A pilot study on the effects of heart rate variability biofeedback in patients with depression and in healthy subjects. Appl. Psychophysiol. Biofeedback 2008, 33, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Thode, L. Heart Rate Variability Biofeedback as a Complementary Treatment for Depression in Latinos; Alliant International University: San Diego, CA, USA, 2019. [Google Scholar]
- Lin, I.M.; Ko, J.M.; Fan, S.Y.; Yen, C.F. Heart Rate Variability and the efficacy of biofeedback in heroin users with depressive symptoms. Clin. Psychopharmacol. Neurosci. 2016, 14, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Lin, I.M.; Fan, S.Y.; Yen, C.F.; Yeh, Y.C.; Tang, T.C.; Huang, M.F.; Liu, T.L.; Wang, P.W.; Lin, H.C.; Tsai, H.Y.; et al. Heart Rate Variability biofeedback increased autonomic activation and improved symptoms of depression and insomnia among patients with Major Depression Disorder. Clin. Psychopharmacol. Neurosci. 2019, 17, 222–232. [Google Scholar] [CrossRef]
- Karavidas, M.K. Heartrate variability biofeedback for major depression. Biofeedback 2008, 36, 18–21. [Google Scholar]
- Rene, R. The Efficacy of a Portable Heart Rate Variability Feedback Device in Conjunction with Mental Health Treatment of Clients with Major Depressive Disorder Enrolled in a County Welfare-to-Work Program; Alliant University: San Diego, CA, USA, 2011. [Google Scholar]
- De Bruin, E.; Van der Zwan, J.; Bogels, S. A RCT Compairing Daily Mindfulness meditations, Biofeedback Exercises and Physical Exercise on Attention Control, Executive Functioning, Mindful Awareness, SelfCompassion and Worrying in Stressed Young Adults. Mindfullness 2016, 7, 1182–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porges, S. Respiratory sinus arrhythmia: Physiological basis, quantitative methods and clinical implications. In Cardiorespiratory and Cardiosomatic Psychophysiology; Plenum Press: New York, NY, USA, 1986; pp. 101–115. [Google Scholar]
- Blanchard, E. Elevated basal level of cardiovascular responses in Vietnam veterans with PTSD: a health problem I the making? J. Anxiety Disord. 1990, 4, 233–237. [Google Scholar] [CrossRef]
- Cohen, H.; Kotler, M.; Matar, M.; Kaplan, Z. Power spectral analysis of heart rate variability in posttraumatic stress disorder patients. Biol. Psychiatry 1997, 41, 627–629. [Google Scholar] [CrossRef]
- Schoenberg, P.L.; David, A.S. Biofeedback for psychiatric disorders: A systematic review. Appl. Psychophysiol. Biofeedback 2014, 39, 109–135. [Google Scholar] [CrossRef]
- Lehrer, P.; Kaur, K.; Sharma, A.; Shah, K.; Huseby, R.; Bhavsar, J.; Zhang, Y. Heart Rate Variability Biofeedback Improves Emotional and Physical Health and Performance: A Systematic Review and Meta Analysis. Appl. Psychophysiol. Biofeedback 2020, 45, 109–129. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, P.; Vaschillo, E.; Vaschillo, B.; Habib, H. Biofeedback treatment for asthma. Chest 2004, 126, 352–361. [Google Scholar] [CrossRef] [Green Version]
- Nolan, R.P.; Kamath, M.V.; Floras, J.S.; Picton, P. Heart Rate Variability biofeedback as a behavioral neurocardiac intervention to enhance vagal heart rate control. Am. Heart J. 2005, 149, 1137.e1–1137.e7. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, J.; Wachholtz, A. The benefit of heart rate variability biofeedback and relaxation training in reduction trait anxiety. Hanguk Simni Hakhoe Chi. Kongang 2015, 20, 391–408. [Google Scholar]
- Henriques, G.; Keffer, S.; Abrahamson, C.; Horst, S.J. Exploring the effectiveness of a computer-based HRV biofeedback program in reducing anxiety in college students. Appl. Psychophysiol. Biofeedback 2011, 36, 101–112. [Google Scholar] [CrossRef]
- De Couck, M.; de Leeuw, I.; Blase, K.; Gidron, Y. Effects of heart rate variability biofeedback on the tumor marker CEA in metastatic colon cancer. J. Immunol. Res. 2018, 79, A18. [Google Scholar]
- Windthorst, P.; Mazurak, N.; Kuske, M.; Hipp, A.; Giel, K.E.; Enck, P.; Nieß, A.; Zipfel, S.; Teufel, M. Heart Rate Variability biofeedback therapy and graded exercise training in management of chronic fatigue syndrome. J. Psychosom. Res. 2017, 93, 6–13. [Google Scholar] [CrossRef]
- Berry, M.; Ginsberg, J.; Nagpal, M. Non-pharmalogical intervention for chronic pain in veterans: A pilot study of HRV. Glob. Adv. Health Med. 2014, 3, 28–33. [Google Scholar] [PubMed] [Green Version]
- Del Pozo, J.M.; Gevirtz, R.N.; Scher, B.; Guarneri, E. Biofeedback treatment increases heart rate variability in patients with known coronary artery disease. Am. Heart J. 2004, 147, 545. [Google Scholar] [CrossRef]
- Yu, L.C.; Lin, I.M.; Fan, S.Y.; Chien, C.L.; Lin, T.H. One year cardiovascular prognosis of the randomized controlled short term HRV biofeedback among patients with coronary artery disease. Int. J. Behav. Med. 2018, 25, 271–282. [Google Scholar]
- Francis, H.; Penglis, K.; Mc Donald, S. Manipulation of heart rate variability can modify response to anger-inducing stimuli. Soc. Neurosci. 2016, 11, 545–552. [Google Scholar] [CrossRef]
- Sequeira, V.; Bandeira, P.; Azevedo, J. Heart Rate Variability in adults with obstructive sleep apnea: A systematic review. Sleep Sci. 2019, 12, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Hasuo, H.; Kanbara, K.; Fukunaga, M. Effect of Heart Rate Variability biofeedback sessions with resonant breathing on sleep. Sci. Rep. 2020, 10, 7427. [Google Scholar]
- Clamor, A.; Koenig, J.; Thayer, J.; Lincoln, T. A randomized-controlled trial of heart rate variability for psychotic symptoms. Behav. Res. 2016, 87, 207–215. [Google Scholar] [CrossRef]
- Van der Zwan, J.; de Vente, W.; Huizink, A.; Bögels, S.; de Bruin, E. Physical activity, mindfulness meditation, or HRVbiofeedback for stress reduction: a randomized contolled trial. Appl. Psychophysiol Biofeedback 2015, 40, 257–268. [Google Scholar] [CrossRef] [Green Version]
- Stern, M.; Guilles, R.; Gevirtz, R. HRVBiofeedback for Pedriatic Irritable Bowel Syndrome and Functional Abdominal Pain: a clinical replication series. Appl. Psychophysiol. Biofeedback 2014, 39, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Kudo, N.; Shinohara, H.; Kodama, H. Heart Rate Variability biofeedback intervention for reduction of psychological stress during the early postpartum period. Appl. Psychophysiol. Biofeedback 2014, 39, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Lande, R.G.; Williams, L.B.; Marin, M.L. Efficacy of biofeedback for post-traumatic stress disorder. Complement. Med. 2010, 18, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.; Strosahl, K.; Wilson, K. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Gevirtz, R. Incorporating HRV biofeedback info Acceptance and Commitment Therapy. Biofeedback 2020, 48, 16–19. [Google Scholar] [CrossRef]
- Brinkman, A.; Press, S.; Helmert, E.; Hautzinger, M.; Khazan, I.; Vagedes, J. Comparing effectiveness of HRVB and mindfulness for workplace stressreduction: A Randomized controlled trial. Appl. Psychophysiol. Biofeedback 2020, 45, 307–322. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RCT Studies HRVB for Treatment PTSD and Depression | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| RELEVANCE | RESULTS | ||||||||||
| Autor | Design | n | Domain | Setting | Period | Scale | Pre | Post | Reduction | Signif. | |
| RCT/SGT | Exp | Exp | Exp | Cont | Pre-Post | ||||||
| Zucker (2009)[28] | RCT HRVB vs. PMR | 38 | PTSD | 1e line | 4 weeks daily | PCL | 52.6 | 38.6 | 27% | 18% | p < 0.05 |
| BDI-II | 26.4 | 12.3 | 53% | 24% | p < 0.05 | ||||||
| Tan (2011) [29] | RCT HRVB vs. TAU | 20 | PTSD | Veteran hosp | 8 weeks daily | PCL-S | 64.8 | 54.4 | 16% | 2% | p < 0.05 |
| CAPS | 86.4 | 71.2 | 18% | 9% | p < 0.001 | ||||||
| Rene (2008) [30] | RCT HRVB vs. PMR | 46 | Depression | 1e line | 8 weeks daily | BDI-II | 35.0 | 7.8 | 78% | 44% | p < 0.005 |
| Chaudhri (2008) [31] | RCT HRVB+DBT vs sertraline | 60 | Depression | univ.hos | 12 weeks daily | BDI-II | 31.0 | 7.5 | 76% | 29% | p < 0.001 |
| DERS | 123.1 | 64.2 | 48% | 8% | p < 0.001 | ||||||
| Patron (2013) [32] | RCT HRVB vs. TAU | 26 | Depression after infarct | univ.hos | 2 weeks daily | CES-D | 15.3 | 8.9 | 42% | 1% | p = 0.02 |
| Van der Zwan (2019) [33] | RCT HRVB vs. waitinglist | 50 | Depression Anxiety Stress | University pregnant Women | 5 weeks daily | DASS PSQI | 5.45 6.55 | 2. 84.7 | 49% 21% | 35% 10% | p = 0.039 p = 0.063 |
| Karavidas (2007) [34] | SGT | 11 | Depression | univ.hos | 10 weeks | BDI | 26.0 | 12.5 | 52% | - | p < 0.001 |
| Siepman (2008) [35] | HRVB vs. healthy | 38 | Depression | univ.h vs. stud | 4 weeks 3× a Week | BDI | 21.5 | 5.5 | 74% | - | p < 0.05 |
| Thode (2019) [36] | RCT HRVB vs. TAU | 37 | MDD | LatinoHealth center | 4 weeks | PHQ-9 GAD-7 | 16.42 11.08 | 10.85 6.50 | 40% 41% | 7% 9% | p <0.05 p < 0.05 |
| Lin (2016)[37] | Case control study | 9 | MDD Depression | Heroin users | 5weeks 1× a week | BDI-II BDI cogn | 23 19 | 18.3 14.3 | 20% 25% | - | p > 0.05 |
| Lin (2019) [38] | RCT HRVB vs. med.care | 48 | MDD | 3 hospitals | 6 weeks | BDI-II PSQI | 24.25 12.42 | 15.04 8.92 | 38% 28% | 1% 5% | p = 0.007 p = 0.012 |
| Asthma [47] | n = 64 | p < 0.003 | USA |
| Angina Pectoris [48] | n = 63 | p < 0.001 | Canada |
| Angina Pectoris [11] | n = 154 | sig | Taiwan |
| Anxiety [49] | n = 15 | sig | South Korea |
| Anxiety [50] | n = 40 | p < 0.05 | USA |
| Cancer [51] | n = 5 | p < 0.06 | Belgium |
| Chronic fatigue syndrome [52] | n = 28 | sig | Germany |
| Chronic Pain [53] | n = 20 | p < 0.001 | USA |
| Coronary artery disease [54] | n = 63 | p < 0.001 | USA |
| Coronary artery disease [55] | n = 210 | p = 0.001 | Taiwan |
| Depression (see Table 1) | n = 230 | sig | USA, Italy, Taiwan, Netherlands |
| Emotion regulation [56] | n = 58 | sig | Australia |
| Sleep apnea [57] | n = 853 | sig | Brazil |
| Sleep [58] | n = 69 | p = 0.001 | Japan |
| Selfcontrol Psychotic sympt [59] | n = 84 | p = 0.006 | Germany |
| Stress and anxiety [18] | n = 484 | Hedges g = 0.81 | USA |
| Stressreduction [60] | n = 23 | sig | Netherlands |
| Pediatric Irritable Bowel Syndr [61] | n = 24 | sig | USA |
| Postpartum depression [62] | n = 55 | p < 0.001 | Japan |
| PTSD (see Table 1) | n = 97 | p < 0.05 | USA |
| Trait Anxiety [49] | n = 15 | sig | South Korea |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blase, K.; Vermetten, E.; Lehrer, P.; Gevirtz, R. Neurophysiological Approach by Self-Control of Your Stress-Related Autonomic Nervous System with Depression, Stress and Anxiety Patients. Int. J. Environ. Res. Public Health 2021, 18, 3329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073329
Blase K, Vermetten E, Lehrer P, Gevirtz R. Neurophysiological Approach by Self-Control of Your Stress-Related Autonomic Nervous System with Depression, Stress and Anxiety Patients. International Journal of Environmental Research and Public Health. 2021; 18(7):3329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073329
Chicago/Turabian StyleBlase, Kees, Eric Vermetten, Paul Lehrer, and Richard Gevirtz. 2021. "Neurophysiological Approach by Self-Control of Your Stress-Related Autonomic Nervous System with Depression, Stress and Anxiety Patients" International Journal of Environmental Research and Public Health 18, no. 7: 3329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073329