
Evaluation of Quality of Life and Satisfaction in Patients with Fixed Prostheses on Zygomatic Implants Compared with the All-on-Four Concept: A Prospective Randomized Clinical Study

 ,
, 
Abstract
:1. Introduction
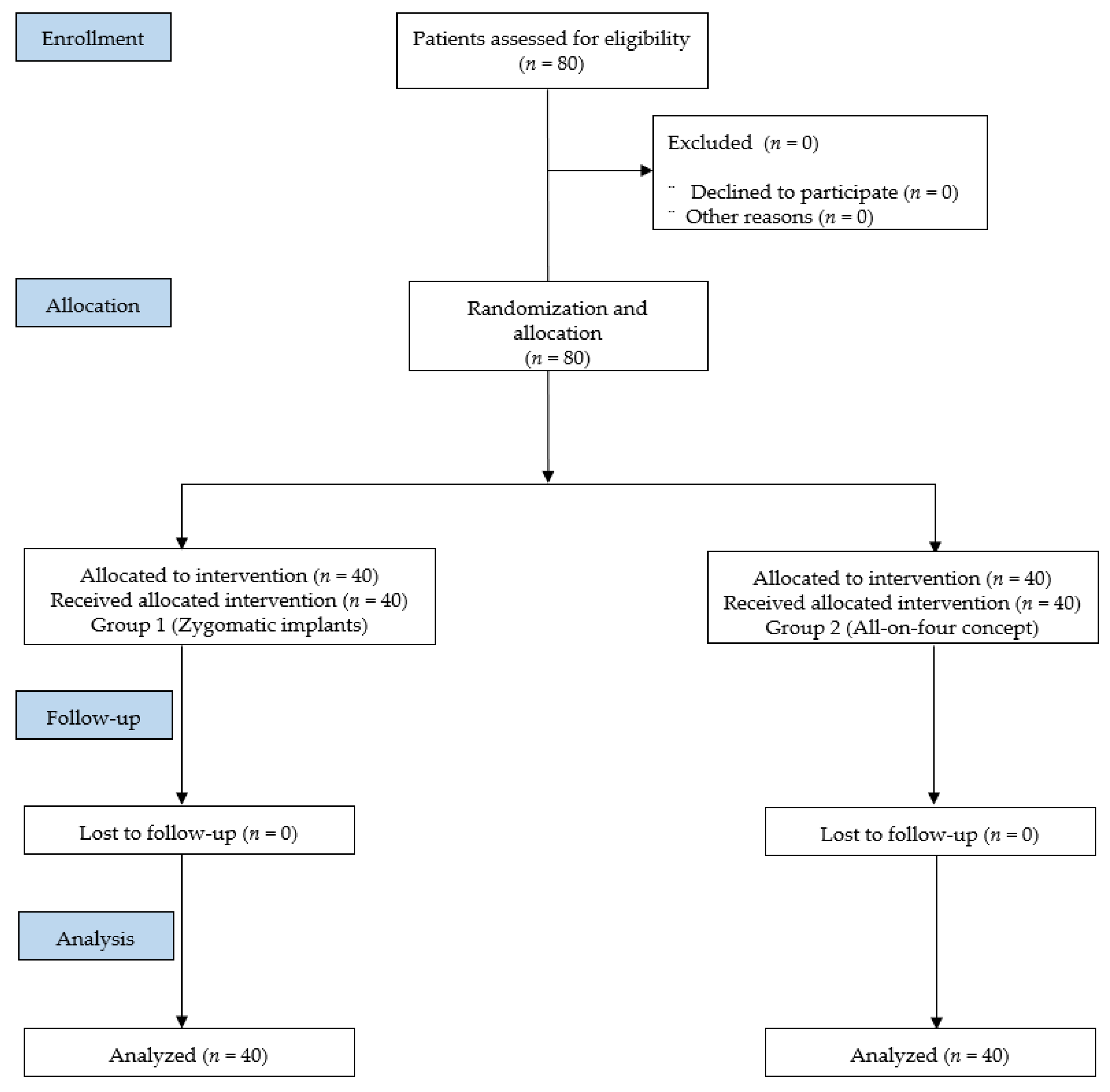
2. Materials and Methods
2.1. Recruitment and Patient Characteristics
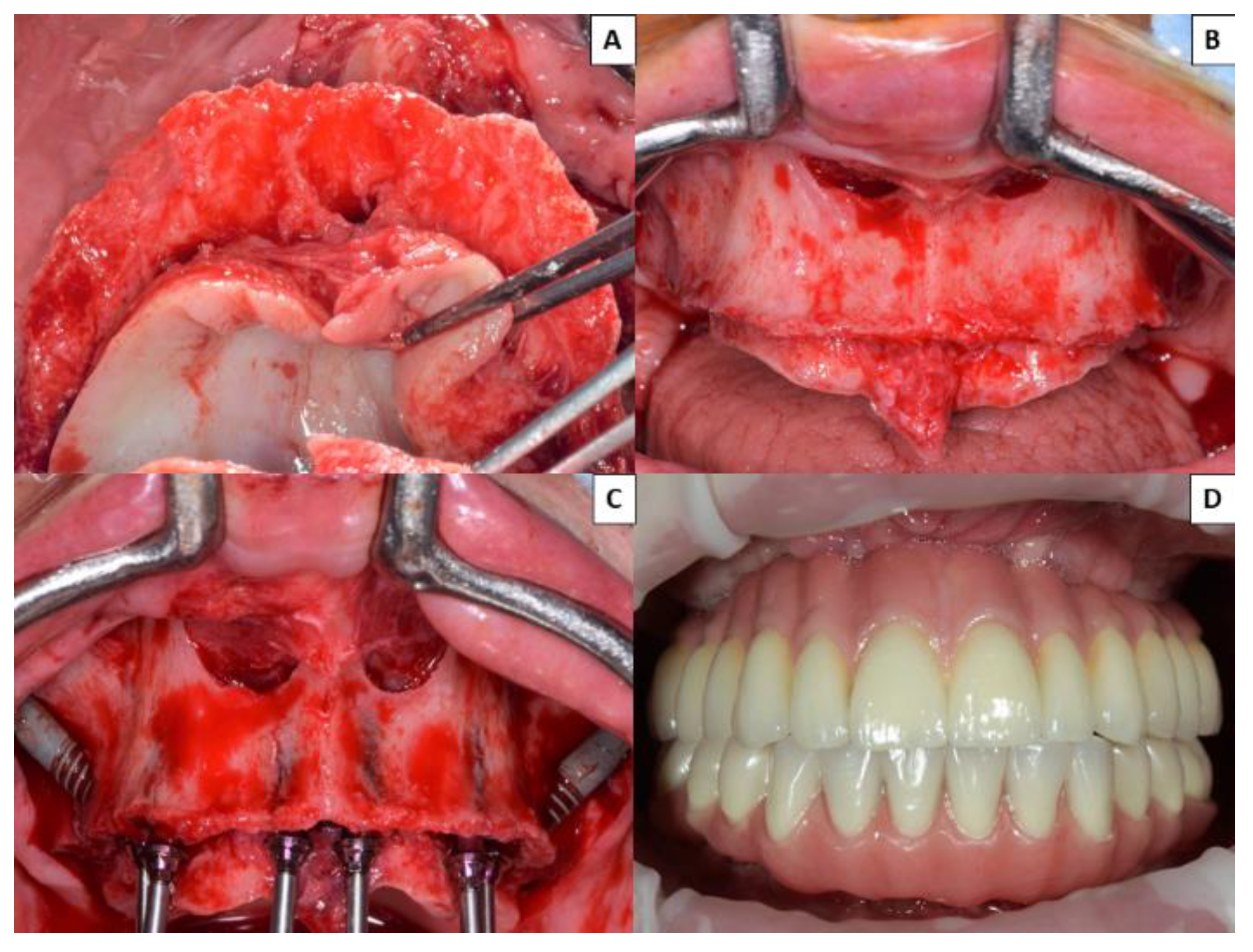
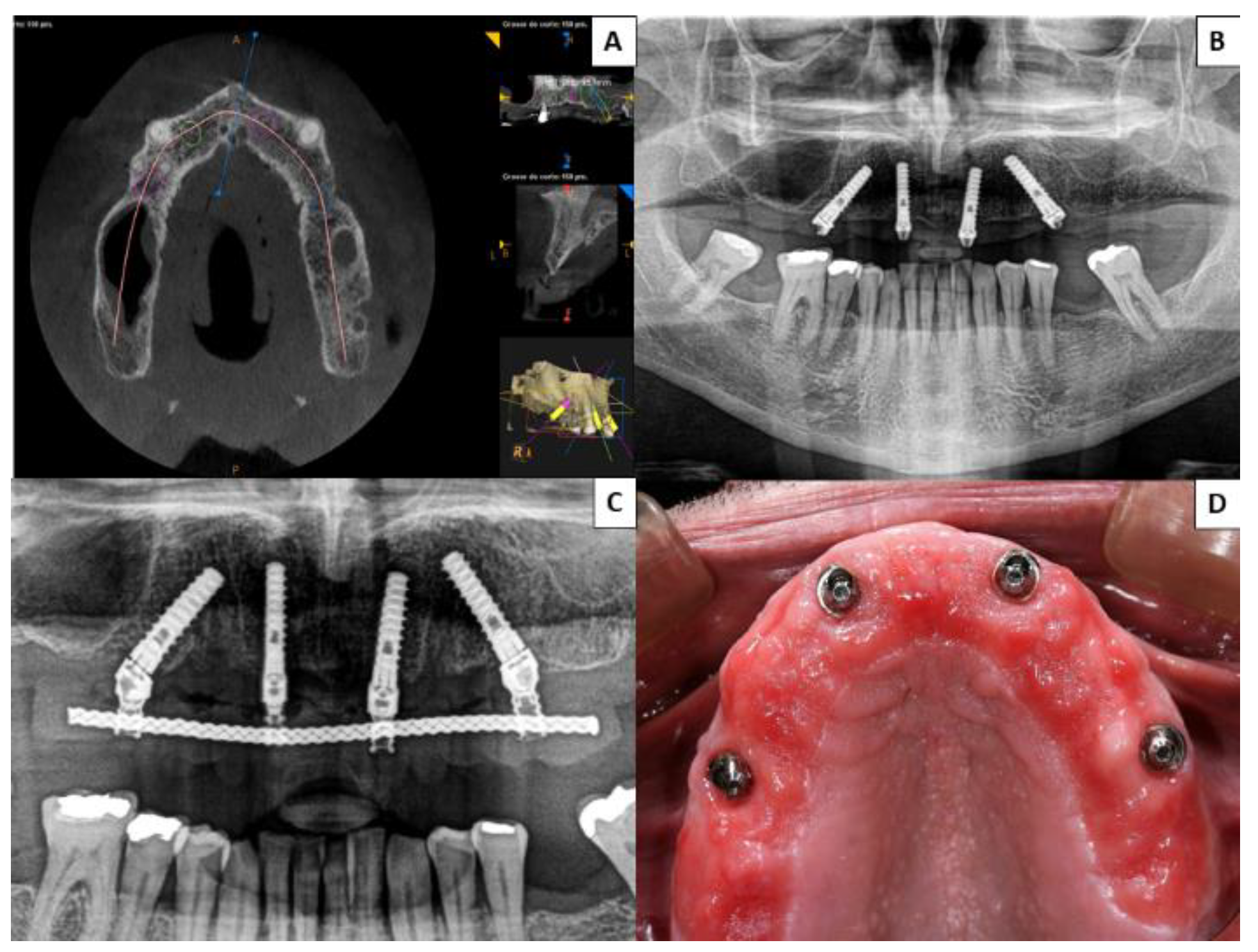
2.2. Study Groups
2.3. Oral Health Impact Profile-14
2.4. Level of Satisfaction with Prosthesis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Padhye, N.M.; Bhatavadekar, N. Quantitative assessment of the edentulous posterior maxilla for implant therapy: A retrospective cone beam computed tomographic study. J. Maxillofac. Oral Surg. 2020, 19, 125–130. [Google Scholar] [CrossRef]
- Kivovics, M.; Szabó, B.T.; Németh, O.; Iványi, D.; Trimmel, B.; Szmirnova, I.; Orhan, K.; Mijiritsky, E.; Szabó, G.; Dobó-Nagy, C. Comparison between micro-computed tomography and cone-beam computed tomography in the assessment of bone quality and a long-term volumetric study of the augmented sinus grafted with an albumin impregnated allograft. J. Clin. Med. 2020, 9, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, M.; Grusovin, M.G.; Felice, P.; Karatzopoulos, G.; Worthington, H.V.; Coulthard, P. Interventions for replacing missing teeth: Horizontal and vertical bone augmentation techniques for dental implant treatment. Cochrane Database Syst. Rev. 2009, 7, CD003607. [Google Scholar] [CrossRef]
- Peñarrocha, M.; Viña, J.A.; Carrillo, C.; Penarrocha, D. Rehabilitation of reabsorbed maxillae with implants in buttresses in patients with combination syndrome. J. Oral Maxillofac. Surg. 2012, 70, e322–e330. [Google Scholar] [CrossRef] [PubMed]
- Alzoubi, F.; Bedrossian, E.; Wong, A.; Farrell, D.; Park, C.; Indresano, T. Outcomes assessment of treating completely edentulous patients with a fixed implant-supported profile prosthesis utilizing a graftless approach. Part 1: Clinically related outcomes. Int. J. Oral Maxillofac. Implant. 2017, 32, 897–903. [Google Scholar] [CrossRef] [Green Version]
- Candel-Marti, E.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M. Satisfaction and quality of life with palatal positioned implants in severely atrophic maxillae versus conventional implants supporting fixed ful-arch prostheses. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e751–e756. [Google Scholar] [CrossRef] [PubMed]
- Alzoubi, F.; Bedrossian, E.; Wong, A.; Ferrell, D.; Park, C.; Indresano, T. Outcomes assessment of treating completely edentulous patients with a fixed implant-supported profile prosthesis utilizing a graftless approach. Part 2: Patient-related outcomes. Int. J. Oral Maxillofac. Implant. 2017, 32, 1080–1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higuchi, K.W. The zygomaticus fixture: An alternative approach for implant anchorage in the posterior maxilla. Ann. R. Australas. Coll. Dent. Surg. 2000, 15, 23–33. [Google Scholar]
- Brånemark, P.I.; Gröndahl, K.; Ohrnell, L.O.; Nilsson, P.; Petruson, B.; Svensson, B.; Engstrand, P.; Nannmark, U. Zygoma fixture in the management of advanced atrophy of the maxilla: Technique and long-term results. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2004, 38, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Ouazzani, W.; Hatano, N. The use of zygomatic implants for prosthetic rehabilitation of the severely resorbed maxilla. Periodontology 2000 2008, 47, 1621–1671. [Google Scholar] [CrossRef]
- Aparicio, C.; Ouazzani, W.; Garcia, R.; Arevalo, X.; Muela, R.; Fortes, V. A prospective clinical study on titanium implants in the zygomatic arch for prosthetic rehabilitation of the atrophic edentulous maxilla with a follow up of 6 months to 5 years. Clin. Implant Dent. Relat. Res. 2006, 8, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Ouazzani, W.; Aparicio, A.; Fortes, V.; Muela, R.; Pascual, A.; Codesal, M.; Barluenga, N.; Franch, M. Immediate/Early loading of zygomatic implants: Clinical experiences after 2 to 5 years of follow-up. Clin. Implant Dent. Relat. Res. 2010, 12, e77–e82. [Google Scholar] [CrossRef]
- Aparicio, C. A proposed classification for zygomatic implant patient based on the zygoma anatomy guided approach (ZAGA): A cross-sectional survey. Eur. J. Oral Implantol. 2011, 4, 269–275. [Google Scholar] [PubMed]
- Aparicio, C.; Manresa, C.; Francisco, K.; Aparicio, A.; Nunes, J.; Claros, P.; Potau, J.M. Zygomatic implants placed using the zygomatic anatomy-guided approach versus the classical technique. A proposed system to report rhinosinusitis diagnosis. Clin. Implant Dent. Relat. Res. 2014, 16, 627–642. [Google Scholar] [CrossRef]
- Esposito, M.; Davó, R.; Marti-Pages, C.; Ferrer-Fuertes, A.; Barausse, C.; Pistilli, R.; Ippolito, D.R.; Felice, P. Immediately loaded zygomatic implants vs conventional dental implants in augmented atrophic maxillae: 4 months post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 11–28. [Google Scholar]
- Maló, P.; Nobre, M.D.A.; Lopes, A.; Ferro, A.; Moss, S. Extramaxillary surgical technique: Clinical outcome of 352 patients rehabilitated with 747 zygomatic implants with a follow-up between 6 months and 7 years. Clin. Implant Dent. Relat. Res. 2015, 17, e153–e162. [Google Scholar] [CrossRef] [PubMed]
- de Araújo Nobre, M.; Maló, P.; Gonçalves, I. Evaluation of clinical soft tissue parameters for extramaxillary zygomatic implants and conventional implants in all-on-4 hybrid rehabilitations: Short-term outcome and proposal of clinical recommendations for intervention in recall appointments. Implant Dent. 2015, 24, 267–274. [Google Scholar] [PubMed]
- Al-Nawas, B.; Wegener, J.; Bender, C.; Wagner, W. Critical soft tissue parameters of zygomatic implant. J. Clin. Periodontol. 2004, 31, 497–500. [Google Scholar] [CrossRef]
- Maló, P.; Nobre Mde, A.; Lopes, I. A new approach to rehabilitate the severely atrophic maxilla using extramaxillary anchored implants in immediate function: A pilot study. J. Prosthet. Dent. 2008, 100, 354–366. [Google Scholar] [CrossRef]
- Davó, R. Zygomatic implants placed with a two-stage procedure: A 5-year retrospective study. Eur. J. Oral Implantol. 2009, 2, 115–124. [Google Scholar] [PubMed]
- Davo, R.; Malevez, C.; Rojas, J. Immediate function in the atrophic maxilla using zygoma implants: A preliminary study. J. Prosthet. Dent. 2007, 97, S44–S51. [Google Scholar] [CrossRef]
- Becktor, J.P.; Isaksson, S.; Abrahamsson, P.; Sennerby, L. Evaluation of 31 zygomatic implants and 74 regular dental implants used in 16 patients for prosthetic reconstruction of the atrophic maxilla with cross-arch fixed bridges. Clin. Implant Dent. Relat. Res. 2005, 7, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, N.P.; Berglundh, T.; Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: Where are we now?--Consensus of the Seventh European Workshop on Periodontology. J. Clin. Periodontol. 2011, 38, 178–181. [Google Scholar] [CrossRef] [Green Version]
- Maló, P.; Rangert, B.; Nobre, M. “All-on-Four” immediate-function concept with Brånemark System implants for completely dentulous mandibles: A retrospective clinical study. Clin. Implant Dent. Relat. Res. 2003, 5, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Francetti, L.; Romeo, D.; Corbella, S.; Taschieri, S.; Del Fabbro, M. Bone level changes around axial and tilted implants in full-arch fixed immediate restorations. Interim results of a prospective study. Clin. Implant Dent. Relat. Res. 2012, 14, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Vinci, R.; Capparé, P.; Romanos, G.E.; Gherlone, E. A clinical study of edentulous patients rehabilitated according to the “all on four” immediate function protocol. Int. J. Oral Maxillofac. Implant. 2012, 27, 428–434. [Google Scholar]
- Hinze, M.; Thalmair, T.; Bolz, W.; Wachtel, H. Immediate loading of fixed provisional prostheses using four implants for the rehabilitation of the edentulous arch: A prospective clinical study. Int. J. Oral Maxillofac. Implant. 2010, 25, 1011–1018. [Google Scholar]
- Malo, P.; de Araújo Nobre, M.; Lopes, A.; Moss, S.M.; Molina, G.J. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. J. Am. Dent. Assoc. 2011, 142, 310–320. [Google Scholar] [CrossRef]
- Patzelt, S.B.M.; Bahat, O.; Reynolds, M.A.; Strub, J.R. The all-on-four treatment concept: A systematic review. Clin. Implant. Dent. Relat. Res. 2013, 16, 836–855. [Google Scholar] [CrossRef]
- Sánchez-Siles, M.; Ballester-Ferrandis, J.F.; Salazar-Sánchez, N.; Gómez-García, F.J.; Moraleja-Ruiz, R.; Camacho-Alonso, F. Long-term evaluation of quality of life and satisfaction between implant bar overdentures and conventional complete dentures: A 23 years retrospective study. Clin. Implant Dent. Relat. Res. 2018, 20, 208–214. [Google Scholar] [CrossRef]
- Slade, G.D. Derivation and validation of a short-form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef]
- Montero, J.; Lopez, J.; Vicente, M.; Galindo, M.; Albaladejo, A.; Bravo, M. Comparative validity of the OIDP and OHIP-14 in describing the impact of oral health on quality of life in a cross-sectional study performed in Spanish adults. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e816–e821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velasco-Ortega, E.; Valente, N.A.; Iezzi, G.; Petrini, M.; Derchi, G.; Barone, A. Maxillary sinus augmentation with three different biomaterials: Histological, histomorphometric, clinical, and patient-reported outcomes from a randomized controlled trial. Clin. Implant Dent. Relat. Res. 2021, 23, 86–95. [Google Scholar] [PubMed]
- De Kok, I.J.; Chang, K.H.; Lu, T.S.; Cooper, L.F. Comparison of three-implant-supported fixed dentures and two-implant-retained overdentures in the edentulous mandible: A pilot study of treatment efficacy and patient satisfaction. Int. J. Oral Maxillofac. Implant. 2011, 26, 415–426. [Google Scholar]
- Sanchez-Siles, M.; Muñoz-Cámara, D.; Salazar-Sánchez, N.; Ballester-Ferrandis, J.; Camacho-Alonso, F. Incidence of peri-implantitis and oral quality of life in patients rehabilitated with different neck designs: A 10-year retrospective study. J. Craniomaxillofac. Surg. 2015, 43, 2168–2174. [Google Scholar] [CrossRef] [PubMed]
- Dellepiane, E.; Pera, F.; Zunino, P.; Mugno, M.G.; Pesce, P.; Menini, M. Patient satisfaction and comfort after a full-arch immediate loaded prosthesis. J. Oral Implantol. 2020, 46, 540–549. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient Sample Characteristics | Group with Zygomatic Implants (n = 40) | Group with All-on-Four (n = 40) |
|---|---|---|
| Follow-up (months): mean ± SD * (range) | 19.40 ± 4.37 (12.00–22.00) | 20.25 ± 3.01 (12.00–24.00) |
| Age: mean ± SD | 60.18 ± 8.75 | 60.90 ± 7.01 |
| Sex: n (%) | ||
| Male | 17 (42.40) | 24 (60.00) |
| Female | 23 (57.50) | 16 (40.00) |
| Smoking Status: n (%) | ||
| Non-smoker | 31 (77.50) | 31 (77.50) |
| ≤10 | 1 (2.50) | 3 (7.50) |
| 11–20 | 5 (12.50) | 5 (12.50) |
| >20 | 3 (7.50) | 2 (5.00) |
| Alcohol Consumption: n (%) | ||
| None | 39 (97.50) | 35 (87.50) |
| Daily | 0 (0) | 0 (0) |
| Weekend drinker | 1 (2.50) | 5 (12.50) |
| Diseases: n (%) | ||
| Myocardial infarction | 3 (7.50) | 4 (10.00) |
| Hypercholesterolemia | 3 (7.50) | 4 (10.00) |
| Arterial hypertension | 6 (15.00) | 8 (20.00) |
| Hepatitis B | 1 (2.50) | 0 (0) |
| Hepatitis C | 2 (5.00) | 0 (0) |
| HIV | 1 (2.50) | 0 (0) |
| Epilepsy | 1 (2.50) | 0 (0) |
| Cardiac arrhythmias | 2 (5.00) | 0 (0) |
| Hypothyroidism | 0 (0) | 2 (5.00) |
| Hyperuricemia | 1 (2.50) | 0 (0) |
| Occlusion | ||
| Natural teeth | 28 (70.00) | 24 (60.00) |
| Metal–porcelain fixed crowns on teeth | 1 (2.50) | 2 (5.00) |
| Metal–porcelain fixed crowns on dental implants | 9 (22.50) | 9 (22.50) |
| Resin prostheses without dental implants | 0 (0) | 1 (2.50) |
| Resin prostheses with dental implants | 2 (5.00) | 4 (10.00) |
| Characteristics | Total, n (%) | Group with Zygomatic Implants, n (%) | Group with All-on-Four, n (%) |
|---|---|---|---|
| Number of dental implants | 396 (100) | 236 (100) | 160 (100) |
| Site | |||
| 1.1 | 36 (9.09) | 36 (15.25) | 0 (0) |
| 1.2 | 42 (10.61) | 2 (0.84) | 40 (25.00) |
| 1.3 | 39 (9.84) | 39 (16.52) | 0 (0) |
| 1.4 | 1 (0.25) | 1 (0.42) | 0 (0) |
| 1.5 | 77 (19.44) | 37 (15.67) | 40 (25.00) |
| 1.6 | 3 (0.75) | 3 (1.27) | 0 (0) |
| 1.7 | 1 (0.25) | 1 (0.42) | 0 (0) |
| 2.1 | 36 (9.09) | 36 (15.25) | 0 (0) |
| 2.2 | 42 (10.61) | 2 (0.84) | 40 (25.00) |
| 2.3 | 39 (9.84) | 39 (16.52) | 0 (0) |
| 2.4 | 1 (0.25) | 1 (0.42) | 0 (0) |
| 2.5 | 77 (19.44) | 37 (15.67) | 40 (25.00) |
| 2.6 | 1 (0.25) | 1 (0.25) | 0 (0) |
| 2.7 | |||
| Length | 1 (0.25) | 1 (0.25) | 0 (0) |
| 10 mm | 64 (16.16) | 20 (8.47) | 44 (27.50) |
| 12 mm | 154 (38.88) | 46 (19.49) | 108 (67.50) |
| 14 mm | 39 (9.84) | 31 (13.13) | 8 (5.00) |
| 35 mm | 13 (3.28) | 13 (5.51) | 0 (0) |
| 37.5 mm | 6 (1.51) | 6 (2.54) | 0 (0) |
| 40 mm | 40 (10.11) | 40 (16.94) | 0 (0) |
| 42.5 mm | 25 (6.31) | 25 (10.59) | 0 (0) |
| 45 mm | 28 (7.07) | 28 (11.86) | 0 (0) |
| 47.5 mm | 8 (2.02) | 8 (3.38) | 0 (0) |
| 50 mm | 11 (2.78) | 11 (4.66) | 0 (0) |
| 52.5 mm | 2 (0.50) | 2 (0.84) | 0 (0) |
| 55 mm | 3 (0.75) | 3 (1.27) | 0 (0) |
| 60 mm | 3 (0.75) | 3 (1.27) | 0 (0) |
| Diameter | |||
| 3.5 mm2 | 106 (26.76) | 18 (7.64) | 88 (55.00) |
| 4.0 mm2 | 151 (38.13) | 79 (33.47) | 72 (45.00) |
| 4.2 mm2 | 139 (35.11) | 139 (58.89) | 0 (0) |
| Characteristics | Zygomatic Implants (n = 139 Implants), n (%) | Conventional Implants for All-on-Four (n = 160 Implants), n (%) |
|---|---|---|
| Number of peri-implantitis (p-value = 0.113) | 17 (100) | 19 (100) |
| Percussion-induced pain (p-value = 0.847) | ||
| Yes | 4 (23.52) | 5 (26.31) |
| No | 13 (76.48) | 14 (73.69) |
| Mobility (p-value = 0.615) | ||
| Yes | 1 (5.88) | 2 (10.52) |
| No | 16 (94.12) | 17 (89.48) |
| Bleeding (p-value = 0.087) | ||
| Yes | 0 (0) | 3 (15.78) |
| No | 17 (100) | 16 (84.22) |
| Suppuration | ||
| Yes | 0 (0) | 0 (0) |
| No | 0 (0) | 0 (0) |
| Hyperplasia or granuloma | ||
| Yes | 0 (0) | 0 (0) |
| No | 0 (0) | 0 (0) |
| OHIP-14 | Group with Zygomatic Implants (n = 40) mean ± SD * | Group with All-on-Four (n = 40) mean ± SD | p-Value |
|---|---|---|---|
| Functional limitation | 3.03 ± 1.29 | 6.35 ± 1.84 | <0.001 |
| Physical pain | 2.15 ± 0.89 | 3.80 ± 0.72 | <0.001 |
| Psychological discomfort | 2.20 ± 1.15 | 4.23 ± 1.18 | <0.001 |
| Physical disability | 3.23 ± 1.23 | 5.08 ± 1.65 | <0.001 |
| Psychological disability | 3.38 ± 0.71 | 4.10 ± 1.66 | 0.013 |
| Social disability | 2.60 ± 0.81 | 4.18 ± 1.31 | <0.001 |
| Handicap | 1.93 ± 0.69 | 2.75 ± 0.84 | <0.001 |
| Total scores | 18.48 ± 3.42 | 30.43 ± 4.37 | <0.001 |
| Satisfaction (p-Value < 0.001) | Group with Zygomatic Implants (n = 40), n (%) | Group with All-on-Four (n = 40), n (%) |
|---|---|---|
| Extremely satisfied | 31 (77.50) | 0 (0) |
| Satisfied | 9 (22.50) | 6 (15.00) |
| A little satisfied | 0 (0) | 30 (75.00) |
| No change | 0 (0) | 3 (7.50) |
| Dissatisfied | 0 (0) | 1 (2.50) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Ruiz, J.A.; Sánchez-Siles, M.; Guerrero-Sánchez, Y.; Pato-Mourelo, J.; Camacho-Alonso, F. Evaluation of Quality of Life and Satisfaction in Patients with Fixed Prostheses on Zygomatic Implants Compared with the All-on-Four Concept: A Prospective Randomized Clinical Study. Int. J. Environ. Res. Public Health 2021, 18, 3426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073426
Fernández-Ruiz JA, Sánchez-Siles M, Guerrero-Sánchez Y, Pato-Mourelo J, Camacho-Alonso F. Evaluation of Quality of Life and Satisfaction in Patients with Fixed Prostheses on Zygomatic Implants Compared with the All-on-Four Concept: A Prospective Randomized Clinical Study. International Journal of Environmental Research and Public Health. 2021; 18(7):3426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073426
Chicago/Turabian StyleFernández-Ruiz, Juan Alberto, Mariano Sánchez-Siles, Yolanda Guerrero-Sánchez, Jesús Pato-Mourelo, and Fabio Camacho-Alonso. 2021. "Evaluation of Quality of Life and Satisfaction in Patients with Fixed Prostheses on Zygomatic Implants Compared with the All-on-Four Concept: A Prospective Randomized Clinical Study" International Journal of Environmental Research and Public Health 18, no. 7: 3426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073426