
High Job Burnout Predicts Low Heart Rate Variability in the Working Population after a First Episode of Acute Coronary Syndrome

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Collection of Sociodemographic and Medical Data
2.3. Assessment of Job Burnout, Anxiety, and Depression
2.4. Measurement of HRV
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics of Study Participants
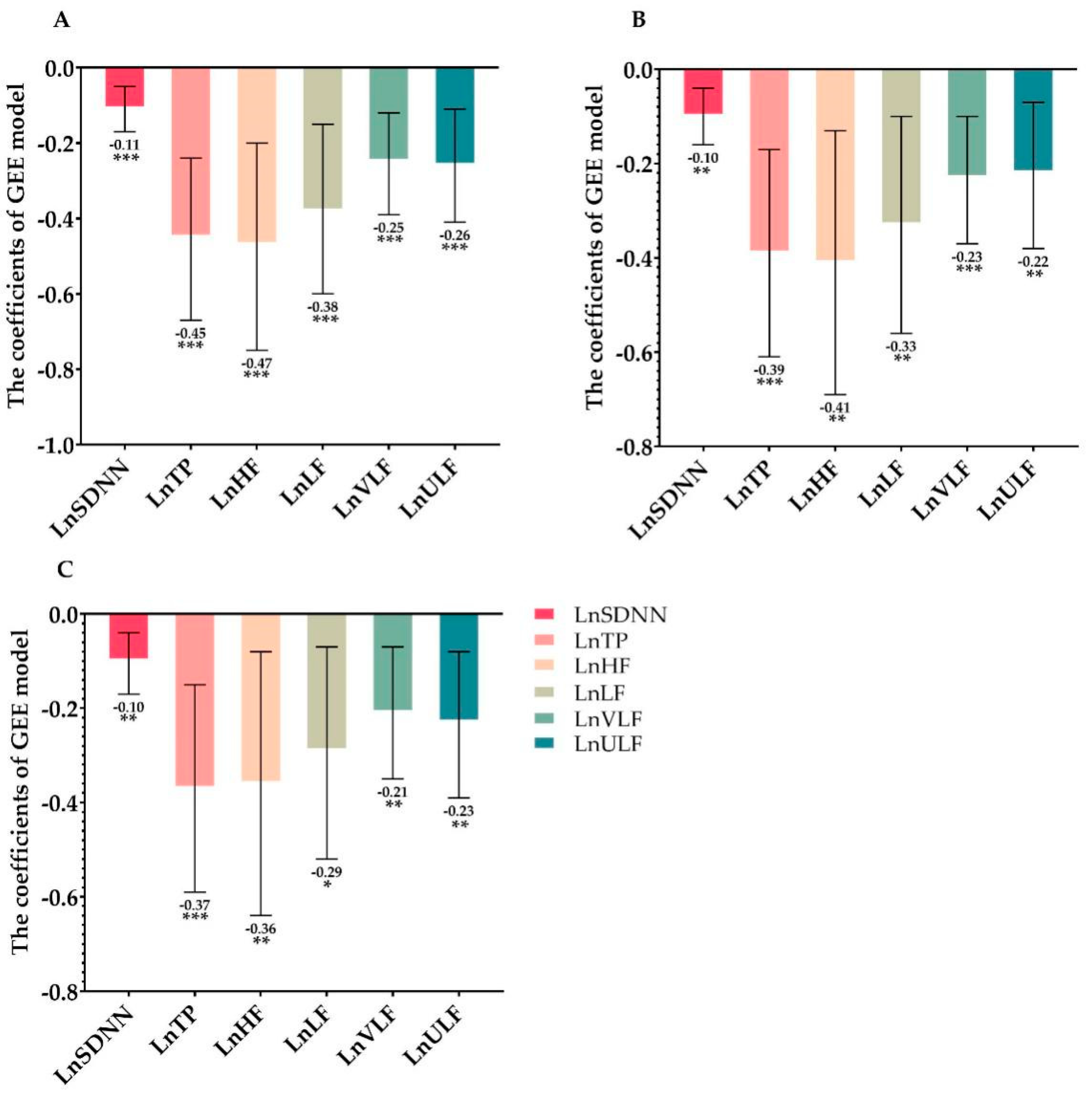
3.2. Prospective Association of Job Burnout on HRV during Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jernberg, T.; Hasvold, P.; Henriksson, M.; Hjelm, H.; Thuresson, M.; Janzon, M. Cardiovascular risk in post-myocardial infarction patients: Nationwide real world data demonstrate the importance of a long-term perspective. Eur. Heart J. 2015, 36, 1163–1170. [Google Scholar] [CrossRef] [Green Version]
- Puymirat, E.; Simon, T.; Cayla, G.; Cottin, Y.; Elbaz, M.; Coste, P.; Lemesle, G.; Motreff, P.; Popovic, B.; Khalife, K.; et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation 2017, 136, 1908–1919. [Google Scholar] [CrossRef] [PubMed]
- Nichols, M.; Townsend, N.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe 2014: Epidemiological update. Eur. Heart J. 2014, 35, 2950–2959. [Google Scholar] [CrossRef] [Green Version]
- Kaasenbrood, L.; Boekholdt, S.M.; van der Graaf, Y.; Ray, K.K.; Peters, R.J.; Kastelein, J.J.; Amarenco, P.; LaRosa, J.C.; Cramer, M.J.; Westerink, J.; et al. Distribution of Estimated 10-Year Risk of Recurrent Vascular Events and Residual Risk in a Secondary Prevention Population. Circulation 2016, 134, 1419–1429. [Google Scholar] [CrossRef] [PubMed]
- McAloon, C.J.; Boylan, L.M.; Hamborg, T.; Stallard, N.; Osman, F.; Lim, P.B.; Hayat, S.A. The changing face of cardiovascular disease 2000–2012: An analysis of the world health organisation global health estimates data. Int. J. Cardiol. 2016, 224, 256–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avezum, A.; Makdisse, M.; Spencer, F.; Gore, J.M.; Fox, K.A.; Montalescot, G.; Eagle, K.A.; White, K.; Mehta, R.H.; Knobel, E.; et al. Impact of age on management and outcome of acute coronary syndrome: Observations from the Global Registry of Acute Coronary Events (GRACE). Am. Heart J. 2005, 149, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Ranasinghe, I.; Wang, Y.; Dharmarajan, K.; Hsieh, A.F.; Bernheim, S.M.; Krumholz, H.M. Readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia among young and middle-aged adults: A retrospective observational cohort study. PLoS Med. 2014, 11, e1001737. [Google Scholar] [CrossRef] [Green Version]
- Jenča, D.; Melenovský, V.; Stehlik, J.; Staněk, V.; Kettner, J.; Kautzner, J.; Adámková, V.; Wohlfahrt, P. Heart failure after myocardial infarction: Incidence and predictors. ESC Heart Fail. 2020, 8, 222–237. [Google Scholar] [CrossRef]
- Kim, Y.; Soffler, M.; Paradise, S.; Jelani, Q.U.; Dziura, J.; Sinha, R.; Safdar, B. Depression is associated with recurrent chest pain with or without coronary artery disease: A prospective cohort study in the emergency department. Am. Heart J. 2017, 191, 47–54. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Xia, K.; Wang, L.F.; Yang, X.C.; Jiang, H.Y.; Zhang, L.J.; Yao, D.K.; Hu, D.Y.; Ding, R.J. Comparing the effects of depression, anxiety, and comorbidity on quality-of-life, adverse outcomes, and medical expenditure in Chinese patients with acute coronary syndrome. Chin. Med. J. 2019, 132, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Mittag, O.; Kolenda, K.D.; Nordman, K.J.; Bernien, J.; Maurischat, C. Return to work after myocardial infarction/coronary artery bypass grafting: Patients’ and physician’ initial viewpoints and outcome 12 months later. Soc. Sci. Med. 2001, 52, 1441–1450. [Google Scholar] [CrossRef]
- Sirois, B.C.; Burg, M.M. Negative emotion and coronary heart disease. A review. Behav. Modif. 2003, 27, 83–102. [Google Scholar] [CrossRef]
- Thombs, B.D.; Bass, E.B.; Ford, D.E.; Stewart, K.J.; Tsilidis, K.K.; Patel, U.; Fauerbach, J.A.; Bush, D.E.; Ziegelstein, R.C. Prevalence of depression in survivors of acute myocardial infarction. J. Gen. Intern. Med. 2006, 21, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Meijer, A.; Conradi, H.J.; Bos, E.H.; Thombs, B.D.; van Melle, J.P.; de Jonge, P. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: A meta-analysis of 25 years of research. Gen. Hosp. Psychiatry 2011, 33, 203–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholson, A.; Kuper, H.; Hemingway, H. Depression as an aetiologic and prognostic factor in coronary heart disease: A meta-analysis of 6362 events among 146 538 participants in 54 observational studies. Eur. Heart J. 2006, 27, 2763–2774. [Google Scholar] [CrossRef] [Green Version]
- Brenninkmeyer, V.; VanYperen, N.W.; Buunk, B.P. Burnout and depression are not identical twins: Is decline of superiority a distinguishing feature? Pers. Individ. Dif. 2001, 30, 873–880. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Occup. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Melamed, S.; Shirom, A.; Toker, S.; Berliner, S.; Shapira, I. Burnout and risk of cardiovascular disease: Evidence, possible causal paths, and promising research directions. Psychol. Bull. 2006, 132, 327–353. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Shi, Y.; Yang, Y.; Liu, L.; Xiao, J.; Guo, T.; Li, J. Burnout is associated with poor recovery of physical performance and low quality of life in patients after their first episode of acute coronary syndrome: A hospital-based prospective cohort study. Int. J. Cardiol. 2017, 227, 503–507. [Google Scholar] [CrossRef]
- Frestad, D.; Prescott, E. Vital Exhaustion and Coronary Heart Disease Risk: A Systematic Review and Meta-Analysis. Psychosom. Med. 2017, 79, 260–272. [Google Scholar] [CrossRef]
- Yaghini Bonabi, S.; El-Hamad, F.; Müller, A.; Dommasch, M.; Steger, A.; Schmidt, G.; Baumert, M. Recording duration and short-term reproducibility of heart rate and QT interval variability in patients with myocardial infarction. Physiol. Meas. 2016, 37, 1925–1933. [Google Scholar] [CrossRef] [PubMed]
- Compostella, L.; Lakusic, N.; Russo, N.; Setzu, T.; Compostella, C.; Vettore, E.; Isabella, G.; Tarantini, G.; Iliceto, S.; Bellotto, F. Functional parameters but not heart rate variability correlate with long-term outcomes in St-elevation myocardial infarction patients treated by primary angioplasty. Int. J. Cardiol. 2016, 224, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T., Jr.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1987, 59, 256–562. [Google Scholar] [CrossRef]
- Muhadi, M.; Nasution, S.A.; Putranto, R.; Harimurti, K. The Ability of Detecting Heart Rate Variability with the Photoplethysmography to Predict Major Adverse Cardiac Event in Acute Coronary Syndrome. Acta Med. Indones. 2016, 48, 48–53. [Google Scholar] [PubMed]
- Harris, P.R.; Stein, P.K.; Fung, G.L.; Drew, B.J. Heart rate variability measured early in patients with evolving acute coronary syndrome and 1-year outcomes of rehospitalization and mortality. Vasc. Health Risk Manag. 2014, 10, 451–464. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Liu, L.; Shi, Y.; Yang, Y.; Yu, X.; Angerer, P.; Kristensen, T.S.; Li, J. Longitudinal associations of burnout with heart rate variability in patients following acute coronary syndrome: A one-year follow-up study. Gen. Hosp. Psychiatry 2018, 53, 59–64. [Google Scholar] [CrossRef]
- Guseva Canu, I.; Marca, S.C.; Dell’Oro, F.; Balázs, Á.; Bergamaschi, E.; Besse, C.; Bianchi, R.; Bislimovska, J.; Koscec Bjelajac, A.; Bugge, M.; et al. Harmonized definition of occupational burnout: A systematic review, semantic analysis, and Delphi consensus in 29 countries. Scand. J. Work Environ. Health 2021, 47, 95–107. [Google Scholar] [CrossRef]
- De Looff, P.C.; Cornet, L.J.M.; Embregts, P.; Nijman, H.L.I.; Didden, H.C.M. Associations of sympathetic and parasympathetic activity in job stress and burnout: A systematic review. PLoS ONE 2018, 13, e0205741. [Google Scholar] [CrossRef]
- Kanthak, M.K.; Stalder, T.; Hill, L.K.; Thayer, J.F.; Penz, M.; Kirschbaum, C. Autonomic dysregulation in burnout and depression: Evidence for the central role of exhaustion. Scand. J. Work Environ. Health 2017, 43, 475–484. [Google Scholar] [CrossRef]
- Wekenborg, M.K.; Hill, L.K.; Thayer, J.F.; Penz, M.; Wittling, R.A.; Kirschbaum, C. The Longitudinal Association of Reduced Vagal Tone With Burnout. Psychosom. Med. 2019, 81, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Yeh, W.Y.; Cheng, Y.; Chen, C.J.; Hu, P.Y.; Kristensen, T.S. Psychometric properties of the Chinese version of Copenhagen burnout inventory among employees in two companies in Taiwan. Int. J. Behav. Med. 2007, 14, 126–133. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Bigger, J.T., Jr.; Fleiss, J.L.; Rolnitzky, L.M.; Steinman, R.C.; Schneider, W.J. Time course of recovery of heart period variability after myocardial infarction. J. Am. Coll. Cardiol. 1991, 18, 1643–1649. [Google Scholar] [CrossRef] [Green Version]
- Buccelletti, E.; Gilardi, E.; Scaini, E.; Galiuto, L.; Persiani, R.; Biondi, A.; Basile, F.; Silveri, N.G. Heart rate variability and myocardial infarction: Systematic literature review and metanalysis. Eur. Rev. Med. Pharmacol. Sci. 2009, 13, 299–307. [Google Scholar]
- Martens, E.J.; Nyklícek, I.; Szabó, B.M.; Kupper, N. Depression and anxiety as predictors of heart rate variability after myocardial infarction. Psychol. Med. 2008, 38, 375–383. [Google Scholar] [CrossRef]
- Thayer, J.F.; Ahs, F.; Fredrikson, M.; Sollers, J.J., 3rd; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- Kim, H.G.; Cheon, E.J.; Bai, D.S.; Lee, Y.H.; Koo, B.H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzo, M.R.; Sasso, F.C.; Marfella, R.; Siniscalchi, M.; Paolisso, P.; Carbonara, O.; Capoluongo, M.C.; Lascar, N.; Pace, C.; Sardu, C.; et al. Autonomic dysfunction is associated with brief episodes of atrial fibrillation in type 2 diabetes. J. Diabetes Complicat. 2015, 29, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.K.; Claxton, J.S.; Soliman, E.Z.; Chen, L.Y.; Lewis, T.T.; Mosley, T., Jr.; Alonso, A. Associations of anger, vital exhaustion, anti-depressant use, and poor social ties with incident atrial fibrillation: The Atherosclerosis Risk in Communities Study. Eur. J. Prev. Cardiol. 2020, 2047487319897163. [Google Scholar] [CrossRef] [PubMed]
- Habibović, M.; Pedersen, S.S.; Broers, E.R.; Alings, M.; Theuns, D.; van der Voort, P.H.; Bouwels, L.; Herrman, J.P.; Denollet, J. Prevalence of anxiety and risk associated with ventricular arrhythmia in patients with an implantable cardioverter defibrillator. Int. J. Cardiol. 2020, 310, 80–85. [Google Scholar] [CrossRef]


{kind=link}
| Low Job Burnout (n = 52) | High Job Burnout (n = 68) | t/χ2 | p | ||
|---|---|---|---|---|---|
| Age (y) | 48.75 ± 8.23 | 50.07 ± 7.00 | −0.951 | 0.344 | |
| Sex [n(%)] | |||||
| Male | 47 (90.4) | 54 (79.4) | 2.662 | 0.103 | |
| Female | 5 (9.6) | 14 (20.6) | |||
| ACS type [n(%)] | |||||
| UA | 8 (15.4) | 9 (13.2) | 0.248 | 0.884 | |
| STEMI | 23 (44.2) | 33 (48.5) | |||
| NSTEMI | 21 (40.4) | 26 (38.3) | |||
| Education level [n(%)] | |||||
| Junior middle school or below | 11 (21.1) | 23 (33.8) | 5.118 | 0.077 | |
| High school/technical secondary school | 33 (63.5) | 29 (42.6) | |||
| College or higher | 8 (15.4) | 16 (23.6) | |||
| Number of family members (n) | 4.00 ± 1.25 | 4.02 ± 1.37 | −0.061 | 0.952 | |
| Monthly family income (Yuan) | 7463.46 ± 2382.70 | 7095.59 ± 1952.61 | 0.929 | 0.355 | |
| Medical history (%) | |||||
| Hypertension | 13.3 | 28.3 | 4.484 | 0.034 * | |
| Diabetes | 8.3 | 15.0 | 0.863 | 0.353 | |
| Hyperlipemia | 15.8 | 20.8 | 0.001 | 0.98 | |
| Stroke | 0.8 | 4.2 | – | 0.232 # | |
| Family history of CVD | 19.2 | 13.3 | 5.756 | 0.016 * | |
| Smoking at present | 32.5 | 35.0 | 2.353 | 0.125 | |
| Heavy drinker | 15.8 | 16.7 | 0.682 | 0.409 | |
| Serum biochemistry (mmol/L) | |||||
| Glucose | 6.25 ± 2.29 | 6.58 ± 2.72 | −0.700 | 0.485 | |
| Total cholesterol | 4.52 ± 1.27 | 4.38 ± 1.28 | 0.606 | 0.546 | |
| Triglyceride | 2.17 ± 1.13 | 1.79 ± 1.07 | 1.885 | 0.062 | |
| HDL-C | 1.17 ± 0.71 | 1.12 ± 0.40 | 0.549 | 0.584 | |
| LDL-C | 2.83 ± 1.05 | 2.89 ± 1.25 | −0.294 | 0.769 | |
| Anxiety score | 6.71 ± 3.79 | 8.29 ± 3.67 | −2.311 | 0.023 * | |
| Depression score | 5.52 ± 2.00 | 6.28 ± 2.28 | −1.910 | 0.059 | |
| Medication (%) | |||||
| Aspirin | 100 | 100 | - | - | |
| P2Y12 receptor antagonists | 100 | 100 | - | - | |
| Statin | 100 | 100 | - | - | |
| Beta blockers | 100 | 100 | - | - | |
| ACEI or ARB | 100 | 100 | - | - |
| HRV Parameters | Discharge | 1 Month | 6 Months | 12 Months |
|---|---|---|---|---|
| Time domain HRV | ||||
| Ln(SDNN) (ln ms) | 4.96 ± 4.67 | 4.99 ± 4.57 | 5.14 ± 4.31 | 5.15 ± 4.39 |
| Frequency domain HRV | ||||
| Ln(TP) (ln ms2) | 8.75 ± 1.97 | 9.23 ± 1.42 | 9.76 ± 1.27 | 10.23 ± 1.95 |
| Ln(HF) (ln ms2) | 7.60 ± 1.52 | 7.65 ± 1.85 | 8.31 ± 1.74 | 8.88 ± 1.04 |
| Ln(LF) (ln ms2) | 7.36 ± 1.27 | 7.53 ± 1.58 | 7.99 ± 1.47 | 8.19 ± 1.66 |
| Ln(VLF) (ln ms2) | 7.59 ± 0.98 | 7.83 ± 1.01 | 8.28 ± 0.86 | 8.56 ± 0.97 |
| Ln(ULF) (ln ms2) | 7.86 ± 0.97 | 8.01 ± 1.00 | 8.48 ± 1.04 | 9.34 ± 1.24 |
| Model I | Model II | Model III | |||||
|---|---|---|---|---|---|---|---|
| Coefficients (95% CIs) | p Value | Coefficients (95% CIs) | p Value | Coefficients (95% CIs) | p Value | ||
| LnSDNN | |||||||
| Job burnout | Low | 0.00 | 0.00 | 0.00 | |||
| High | −0.19 (−0.31, −0.07) | 0.002 | −0.18 (−0.30, −0.05) | 0.005 | −0.18 (−0.30, −0.06) | 0.004 | |
| LnTP | |||||||
| Job burnout | Low | 0.00 | 0.00 | 0.00 | |||
| High | −0.78 (−1.21, −0.36) | <0.001 | −0.69 (−1.12, −0.26) | 0.002 | −0.68 (−1.09, −0.26) | 0.002 | |
| LnHF | |||||||
| Job burnout | Low | 0.00 | 0.00 | 0.00 | |||
| High | −0.70 (−1.24, −0.15) | 0.012 | −0.60 (−1.13, −0.06) | 0.029 | −0.56 (−1.10, −0.03) | 0.038 | |
| LnLF | |||||||
| Job burnout | Low | 0.00 | 0.00 | 0.00 | |||
| High | −0.54 (−0.99, −0.10) | 0.016 | −0.47 (−0.91, −0.03) | 0.036 | −0.44 (−0.88, −0.01) | 0.044 | |
| LnVLF | |||||||
| Job burnout | Low | 0.00 | 0.00 | 0.00 | |||
| High | −0.43 (−0.69, −0.16) | 0.002 | −0.39 (−0.66, −0.13) | 0.004 | −0.37 (−0.63, −0.11) | 0.005 | |
| LnULF | |||||||
| Job burnout | Low | 0.00 | 0.00 | 0.00 | |||
| High | −0.47 (−0.76, −0.18) | 0.001 | −0.42 (−0.71, −0.13) | 0.005 | −0.43 (−0.72, −0.14) | 0.003 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, Y.; Jiang, R.; Zhu, C.; Zhang, M.; Cai, H.; Hu, Z.; Ye, Y.; Liu, Y.; Sun, H.; Ma, Y.; et al. High Job Burnout Predicts Low Heart Rate Variability in the Working Population after a First Episode of Acute Coronary Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 3431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073431
Shi Y, Jiang R, Zhu C, Zhang M, Cai H, Hu Z, Ye Y, Liu Y, Sun H, Ma Y, et al. High Job Burnout Predicts Low Heart Rate Variability in the Working Population after a First Episode of Acute Coronary Syndrome. International Journal of Environmental Research and Public Health. 2021; 18(7):3431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073431
Chicago/Turabian StyleShi, Yunke, Ruxin Jiang, Caifeng Zhu, Min Zhang, Hongyan Cai, Zhao Hu, Yujia Ye, Yixi Liu, Huang Sun, Yiming Ma, and et al. 2021. "High Job Burnout Predicts Low Heart Rate Variability in the Working Population after a First Episode of Acute Coronary Syndrome" International Journal of Environmental Research and Public Health 18, no. 7: 3431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073431