
“The Problem Is that We Hear a Bit of Everything…”: A Qualitative Systematic Review of Factors Associated with Alcohol Use, Reduction, and Abstinence in Pregnancy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Selection Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Search Strategy
2.4. Quality Appraisal
2.5. Data Extraction
2.6. Analysis and Synthesis
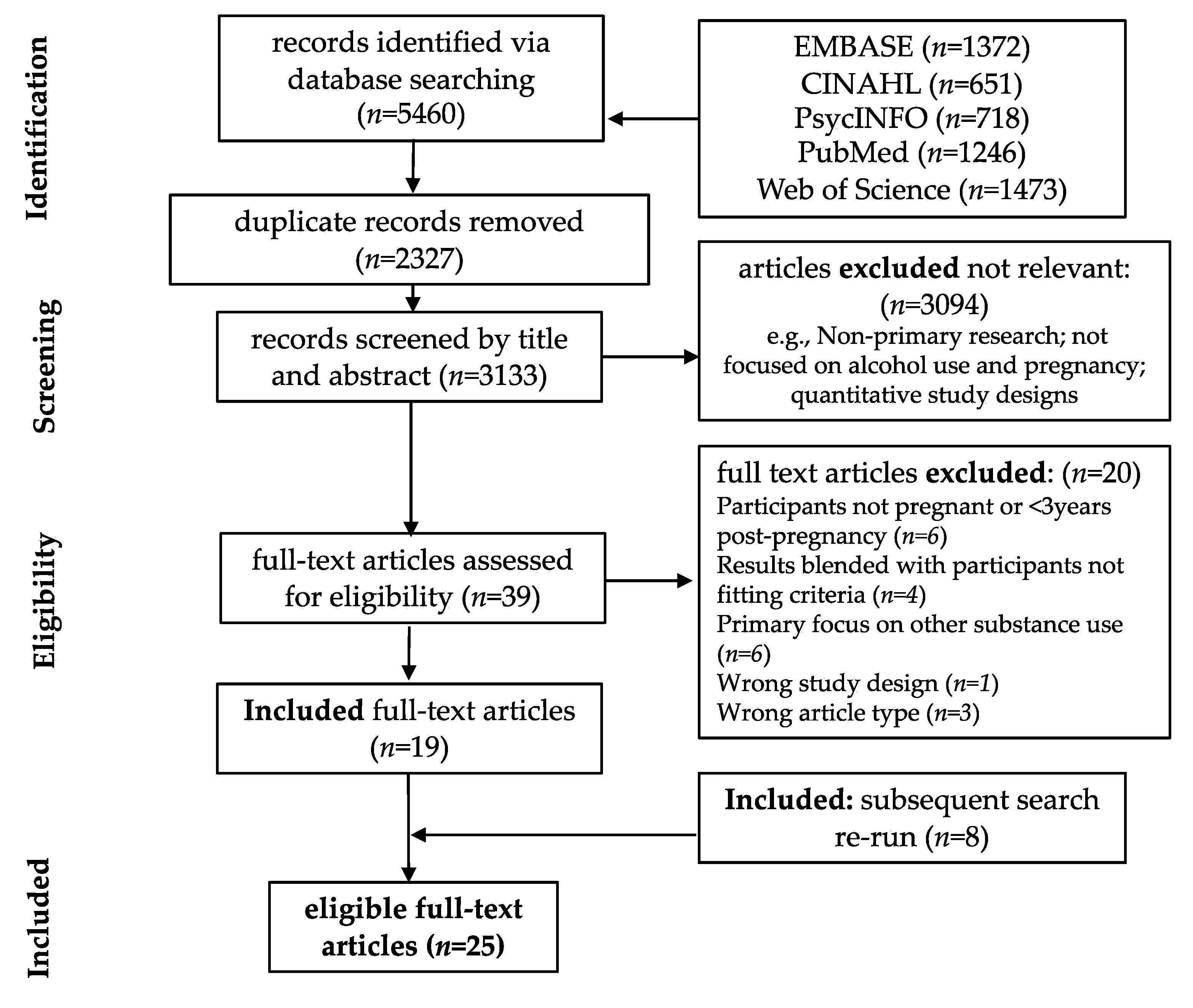
3. Results—Studies Identified
3.1. Study Selection and Characteristics
3.2. Quality Assessment
4. Results—Qualitative Synthesis
4.1. Social Relationships and Norms
“…it [alcohol use] goes along with a social occasion and it goes along with a celebration…”[36]
“…Especially if they’re teenagers, all of their friends are teenagers and all of their friends are out drinking. They want to follow their friends and drink”[29]
“It’s tough when [the pregnancy] is secret! There is really a social pressure regarding alcohol. It’s crazy!”[37]
“Several women perceived abstinence as a shared norm among their relatives, which made it easier for them to change their alcohol consumption since they did not feel the need to justify themselves”[37]
“I’m a major outcast because I don’t drink, I don’t smoke, I don’t do the drugs. When my grandparents have birthdays and stuff, they don’t invite me.... they think I’m high-class. Any person who is pregnant, they become a designated driver… You become an adult babysitter”[45]
“Then we stopped drinking… He wanted to stand by me. We actually did it for our baby”[49]
“I thought he was gonna be a bit more supportive with having the child, we wouldn’t drink together or he would slow down but, he just carried on as before”[56]
4.2. Stigma
“If they drink, they don’t deserve to have a baby. I’m sorry, but they don’t. Because they’re not thinking of the baby. They’re thinking of themselves”[44]
“I’ve sort of become more aware of … how I look, so you sort of don’t feel as comfortable, I guess. Even though you might drink at home, in public you sort of feel a bit scrutinised sometimes. People have pretty strong views on it, so for me, I’ve tended to go out less to have a drink, whereas I might have a drink at home”[30]
“I suppose being pregnant you don’t intentionally want to harm your baby. I know a lot of friends who still drink small amounts while they’re pregnant but I don’t know whether truthfully if they were asked whether they drink what they would say, I suppose there’s those barriers, whether people think they can be honest with those sorts of things”[35]
4.3. Trauma and Other Stressors
“I just know that it gives me just that total relaxation feeling… which I guess could outweigh the fact that you’re having alcohol”[48]
“I would have gotten more stressed out if I hadn’t drunk during pregnancy. It would have been harder”[51]
“I was very scared. I was afraid my parents would ask me to leave the house. I was thinking how my first born was given to my parents by the social workers. I didn’t have an income and my husband did not support me in any way. I panicked all the time because I did not know where I was going to live with this baby”[28]
“The mothers’ own low level of trust in people, combined with what they perceived as lack of understanding from providers, sometimes caused women to express anger at providers, withdraw from traditional care, continue care tentatively, or minimize contact with physicians and nurses”[33]
4.4. Alcohol Use Messaging and Information
“My midwife said that having a glass of red wine was actually better for the baby”[30]
“Many non-Indigenous women were aware that the research evidence for harm associated with low or occasional alcohol use was inconsistent and often described low level drinking as being safe.”
“The problem is that we hear a bit of everything. … We learn a little bit of information everywhere, and we say, ‘All right, let’s split the difference. We diminish, or we drink a sip, and that’s all’”[37]
“Some of them [billboard messages promoting abstinence during pregnancy] exaggerate a little bit more than what it should be. Where they have the baby drinking the 40 oz …even though the baby is drinking with it, the baby isn’t going to sit there and turn no 40-oz up to its mouth. That is overexaggerating”[45]
“…if you have any alcohol at all, you’re a bad person, you’re harming your unborn child, you don’t care, that’s the message that’s coming out; a very judgmental, a very policing, that kind of message”[41]
“Women also reported that advice from health professionals was a factor that strongly influenced their choices and behavior during pregnancy. Hence, another positive motivation was to comply with professional advice. For those who had received advice to abstain, this strengthened their decision to avoid alcohol during pregnancy”[39]
“I guess my mom works with children with FASD, so I understand what happens when you drink during pregnancy. But I also think that there are people out there, that probably don’t understand the risks”[29]
4.5. Access to Trusted, Equitable Care, and Essential Resources
“All the participants suggested ways to improve health care for recovering women. These suggestions included, ‘understand their situation,’ ‘be there for them,’ and ‘be gentle’”[33]
“… it could be good to have a couple of familiar faces, that’s when you build the kind of relationship where you feel comfortable talking in-depth. and asking questions. And maybe have a bit more time to explain, so you can ask, ‘Hey remember last time when I had this question about this, can we follow it up?’”[40]
5. Discussion and Application of the Stigma Action Framework
5.1. Social Norms, Relationships, and Alcohol Use Information
Brief Interventions
5.2. Access to Trusted, Non-Stigmatizing, and Equitable Prenatal Health and Substance Use Services
Holistic, Integrated Support for Pregnant Women with Substance Use Concerns
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Popova, S.P.; Lange, S.M.P.H.; Probst, C.M.; Gmel, G.M.; Rehm, J.P. Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e290–e299. [Google Scholar] [CrossRef] [Green Version]
- Greaves, L.; Poole, N.; Brabete, A.C.; Hemsing, N.; Stinson, J.; Wolfson, L. Integrating Sex. and Gender Informed Evidence into Your Practices: Ten Key Questions on Sex., Gender & Substance Use; Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2020. [Google Scholar]
- Grucza, R.A.; Bucholz, K.K.; Rice, J.P.; Bierut, L.J. Secular Trends in the Lifetime Prevalence of Alcohol Dependence in the United States: A Re-evaluation. Alcohol. Clin. Exp. Res. 2008, 32, 763–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bond, J.C.; Roberts, S.C.M.; Greenfield, T.K.; Korcha, R.; Ye, Y.; Nayak, M.B. Gender differences in public and private drinking contexts: A multi-level GENACIS analysis. Int J. Environ. Res. Public Health 2010, 7, 2136–2160. [Google Scholar] [CrossRef] [Green Version]
- Maani Hessari, N.; van Schalkwyk, M.C.; Thomas, S.; Petticrew, M. Alcohol Industry CSR Organisations: What Can Their Twitter Activity Tell Us about Their Independence and Their Priorities? A Comparative Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2576. [Google Scholar] [CrossRef] [Green Version]
- Pettigrew, S.; Jongenelis, M.I.; Jongenelis, G.; Pierce, H.; Stafford, J.; Keric, D. Get Them Laughing to Get Them Drinking: An Analysis of Alcohol Advertising Themes Across Multiple Media in Australia. J. Stud. Alcohol Drugs 2020, 81, 311–319. [Google Scholar] [CrossRef]
- Jernigan, D.; Ross, C.S. The Alcohol Marketing Landscape: Alcohol Industry Size, Structure, Strategies, and Public Health Responses. J. Stud. Alcohol Drugs Suppl. 2020, 19, 13–25. [Google Scholar] [CrossRef]
- Poole, N.; Schmidt, R.A.; Bocking, A.; Bergeron, J.; Fortier, I. The Potential for Fetal Alcohol Spectrum Disorder Prevention of a Harmonized Approach to Data Collection about Alcohol Use in Pregnancy Cohort Studies. Int. J. Environ. Res. Public Health 2019, 16, 2019. [Google Scholar] [CrossRef] [Green Version]
- Canadian Centre on Substance Use and Addiction. Canada’s Low-Risk Alcohol Drinking Guidelines. Available online: https://www.ccsa.ca/sites/default/files/2020-07/2012-Canada-Low-Risk-Alcohol-Drinking-Guidelines-Brochure-en_0.pdf (accessed on 5 November 2019).
- National Health and Medical Research Council. Australian Alcohol Guidelines Revised. Available online: https://www.nhmrc.gov.au/health-advice/alcohol (accessed on 5 November 2019).
- Streissguth, A.P.; Bookstein, F.L.; Barr, H.M.; Sampson, P.D.; O’Malley, K.; Kogan Young, J. Risk factors for adverse Life outcomes in Fetal Alcohol Syndrome and Fetal Alcohol Effects. J. Dev. Behav Pediatr 2004, 25, 228–238. [Google Scholar] [CrossRef]
- Popova, S.; Lange, S.; Temple, V.; Poznyak, V.; Chudley, A.E.; Burd, L.; Murray, M.; Rehm, J. Profile of Mothers of Children with Fetal Alcohol Spectrum Disorder: A Population-Based Study in Canada. Int. J. Environ. Res. Public Health 2020, 17, 7986. [Google Scholar] [CrossRef]
- Floyd, R.L.; Decouflé, P.; Hungerford, D.W. Alcohol use prior to pregnancy recognition. Am. J. Prev. Med. 1999, 17, 101–107. [Google Scholar] [CrossRef]
- Muggli, E.; O’Leary, C.; Donath, S.; Orsini, F.; Forster, D.; Anderson, P.J.; Lewis, S.; Nagle, C.; Craig, J.M.; Elliott, E.; et al. “Did you ever drink more?” A detailed description of pregnant women’s drinking patterns. BMC Public Health 2016, 16, 683. [Google Scholar] [CrossRef] [Green Version]
- Poole, N.; Schmidt, R.A.; Green, C.; Hemsing, N. Prevention of Fetal Alcohol Spectrum Disorder: Current Canadian Efforts and Analysis of Gaps. Subst. Abuse 2016, 2016, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Nathoo, T.; Poole, N.; Wolfson, L.; Schmidt, R.; Hemsing, N.; Gelb, K. Doorways to Conversation: Brief Intervention on Substance Use with Girls and Women. Available online: https://bccewh.bc.ca/wp-content/uploads/2018/06/Doorways_ENGLISH_July-18-2018_online-version.pdf (accessed on 18 September 2019).
- Aspler, J.; Zizzo, N.; Bell, E.; Di Pietro, N.; Racine, E. Stigmatisation, Exaggeration, and Contradiction: An Analysis of Scientific and Clinical Content in Canadian Print Media Discourse About Fetal Alcohol Spectrum Disorder. Can. J. Bioeth. 2019, 2, 23–35. [Google Scholar] [CrossRef] [Green Version]
- Cook, M.; Leggat, G.; Pennay, A. Change over Time in Australian Newspaper Reporting of Drinking During Pregnancy: A Content Analysis (2000–2017). Alcohol Alcohol. Oxf. 2020, 55, 690–697. [Google Scholar] [CrossRef]
- Hubberstey, C.; Rutman, D. HerWay Home Program for Pregnant and Parenting Women Using Substances: A Brief Social Return on Investment Analysis. Can. J. Addict. 2019, 11, 6–14. [Google Scholar] [CrossRef]
- Milligan, K.; Usher, A.M.; Urbanoski, K.A. Supporting pregnant and parenting women with substance-related problems by addressing emotion regulation and executive function needs. Addict. Res. Theory 2017, 25, 251–261. [Google Scholar] [CrossRef]
- Wolfson, L.; Poole, N.; Morton Ninomiya, M.; Rutman, D.; Letendre, S.; Winterhoff, T.; Finney, C.; Carlson, E.; Prouty, M.; McFarlane, A.; et al. Collaborative Action on Fetal Alcohol Spectrum Disorder Prevention: Principles for Enacting the Truth and Reconciliation Commission Call to Action #33. Int. J. Environ. Res. Public Health 2019, 16, 1589. [Google Scholar] [CrossRef] [Green Version]
- Samaroden, M. Challenges and Resiliency in Aboriginal Adults with Fetal Alcohol Spectrum Disorder. First Peoples Child. Family Rev. 2018, 13, 8–19. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol 2012, 12, 181. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Tam, T. Addresing Stigma: Towards a More Inclusive Health System. Available online: https://www.canada.ca/content/dam/phac-aspc/documents/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/addressing-stigma-what-we-heard/stigma-eng.pdf (accessed on 18 September 2019).
- Watt, M.H.; Eaton, L.A.; Choi, K.W.; Velloza, J.; Kalichman, S.C.; Skinner, D.; Sikkema, K.J. “It’s better for me to drink, at least the stress is going away”: Perspectives on alcohol use during pregnancy among South African women attending drinking establishments. Soc. Sci. Med. 2014, 116, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Gibson, S.; Nagle, C.; Paul, J.; McCarthy, L.; Muggli, E. Influences on drinking choices among Indigenous and non-Indigenous pregnant women in Australia: A qualitative study. PLoS ONE 2020, 15, e0224719. [Google Scholar] [CrossRef]
- Crawford-Williams, F.; Steen, M.; Esterman, A.; Fielder, A.; Mikocka-Walus, A. “My midwife said that having a glass of red wine was actually better for the baby”: A focus group study of women and their partner’s knowledge and experiences relating to alcohol consumption in pregnancy. BMC Pregnancy Childbirth 2016, 15, 79. [Google Scholar] [CrossRef] [Green Version]
- Stengel, C. The risk of being ‘too honest’: Drug use, stigma and pregnancy. Health Risk Soc. 2014, 16, 36–50. [Google Scholar] [CrossRef]
- Rutman, D.; Hubberstey, C. National Evaluation of Canadian Multi-Service FASD Prevention Programs: Interim Findings from the Co-Creating Evidence Study. Int. J. Environ. Res. Public Health 2019, 16, 1767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brudenell, I. A Grounded Theory of Balancing Alcohol Recovery and Pregnancy. West. J. Nurs Res. 1996, 18, 429–440. [Google Scholar] [CrossRef]
- Brudenell, I. A Grounded Theory of Protecting Recovery during Transition to Motherhood. Am. J. Drug Alcohol Abuse 1997, 23, 453–466. [Google Scholar] [CrossRef]
- Jones, S.C.; Eval, M.; Telenta, J.; Cert, G.; Shorten, A.; Johnson, K. Midwives and pregnant women talk about alcohol: What advice do we give and what do they receive? Midwifery 2011, 27, 489–496. [Google Scholar] [CrossRef]
- Jones, S.C.; Telenta, J. What influences Australian women to not drink alcohol during pregnancy? Aust. J. Prim. Health 2012, 18, 68–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gouilhers, S.; Meyer, Y.; Inglin, S.; Pfister Boulenaz, S.; Schnegg, C.; Hammer, R. Pregnancy as a transition: First-time expectant couples′ experience with alcohol consumption. Drug Alcohol Rev. 2019, 38, 758–765. [Google Scholar] [CrossRef] [Green Version]
- Hammer, R. ‘I can tell when you’re staring at my glass…’: Self- or co-surveillance? Couples’ management of risks related to alcohol use during pregnancy. Health Risk Soc. 2019, 21, 335–351. [Google Scholar] [CrossRef]
- France, K.E.; Donovan, R.J.; Henley, N.; Bower, C.; Elliott, E.J.; Payne, J.M.; D’Antoine, H.; Bartu, A.E. Promoting abstinence from alcohol during pregnancy: Implications from formative research. Subst. Use Misuse 2013, 48, 1509–1521. [Google Scholar] [CrossRef] [Green Version]
- Hocking, M.; O’Callaghan, F.; Reid, N. Women’s experiences of messages relating to alcohol consumption, received during their first antenatal care visit: An interpretative phenomenological analysis. Women Birth 2019, 33, e122–e128. [Google Scholar] [CrossRef]
- Holland, K.; McCallum, K.; Walton, A. ‘I’m not clear on what the risk is’: Women’s reflexive negotiations of uncertainty about alcohol during pregnancy. Health, Risk Soc. 2016, 18, 38–58. [Google Scholar] [CrossRef]
- Meurk, C.S.; Broom, A.; Adams, J.; Hall, W.; Lucke, J. Factors influencing women’s decisions to drink alcohol during pregnancy: Findings of a qualitative study with implications for health communication. BMC Pregnancy Childbirth 2014, 14, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbour, B.G. Alcohol and pregnancy. J. Nurse Midwifery 1990, 35, 78–85. [Google Scholar] [CrossRef]
- Baxter, L.A.; Hirokawa, R.; Lowe, J.B.; Nathan, P.; Pearce, L. Dialogic Voices in Talk about Drinking and Pregnancy. J. Appl. Commun. Res. 2004, 32, 224–248. [Google Scholar] [CrossRef]
- Branco, E.I.; Kaskutas, L.A. “If it burns going down…”: How focus groups can shape fetal alcohol syndrome (FAS) prevention. Subst Use Misuse 2001, 36, 333–345. [Google Scholar] [CrossRef]
- Sheridan, K. Substance-Using Pregnant and Parenting Adolescent Girls: Considerations for Preventive Intervention Using a Resilience Lens. J. Soc. Work Pract. Addict. 2018, 18, 128–152. [Google Scholar] [CrossRef]
- Grant, A.; Morgan, M.; Mannay, D.; Gallagher, D. Understanding health behaviour in pregnancy and infant feeding intentions in low-income women from the UK through qualitative visual methods and application to the COM-B (Capability, Opportunity, Motivation-Behaviour) model. BMC Pregnancy Childbirth 2019, 19, 56. [Google Scholar] [CrossRef] [PubMed]
- Raymond, N.; Beer, C.; Glazebrook, C.; Sayal, K. Pregnant women’s attitudes towards alcohol consumption. BMC Public Health 2009, 9, 175. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.F.; Ward, C.L. Women who drank while pregnant: The importance of social context in the lives of South African pregnant women. Drugs Educ. Prev. Policy 2018, 25, 438–445. [Google Scholar] [CrossRef]
- Hammer, R.; Inglin, S. ‘I don’t think it’s risky, but…’: Pregnant women’s risk perceptions of maternal drinking and smoking. Health Risk Soc. 2014, 16, 22–35. [Google Scholar] [CrossRef]
- Martinelli, J.L.; Germano, C.M.R.; de Avó, L.R.d.S.; Fontanella, B.J.B.; Melo, D.G. Motivation for alcohol consumption or abstinence during pregnancy: A clinical-qualitative study in Brazil. PLoS ONE 2019, 14, e0223351. [Google Scholar] [CrossRef] [PubMed]
- Bianchini, B.V.; Maroneze, M.C.; Timm, M.S.; dos Santos, B.Z.; Dotto, P.P. Prevalence of Alcohol and Tobacco Use and Perceptions Regarding Prenatal Care among Pregnant Brazilian Women, 2017 to 2018: A Mixed-Methods Study. Matern. Child Health J. 2020, 24, 1438–1445. [Google Scholar] [CrossRef]
- Toutain, S. What women in France say about alcohol abstinence during pregnancy. Drug Alcohol Rev. 2010, 29, 184–188. [Google Scholar] [CrossRef]
- Pati, S.; Chauhan, A.S.; Mahapatra, P.; Hansdah, D.; Sahoo, K.C.; Pati, S. Weaved into the cultural fabric: A qualitative exploration of alcohol consumption during pregnancy among tribal women in Odisha, India. Subst Abuse Treat. Prev Policy 2018, 13, 9. [Google Scholar] [CrossRef] [Green Version]
- van der Wulp, N.Y.; Hoving, C.; de Vries, H. A qualitative investigation of alcohol use advice during pregnancy: Experiences of Dutch midwives, pregnant women and their partners. Midwifery 2013, 29, e89–e98. [Google Scholar] [CrossRef] [PubMed]
- Schölin, L.; Hughes, K.; Bellis, M.A.; Eriksson, C.; Porcellato, L. Exploring practices and perceptions of alcohol use during pregnancy in England and Sweden through a cross-cultural lens. Eur. J. Public Health 2017, 28, 533–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, R.; Wolfson, L.; Stinson, J.; Poole, N.; Greaves, L. Mothering and Opioids: Addressing Stigma and Acting Collaboratively; Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2019. [Google Scholar]
- Poole, N.A. Fetal Alcohol Spectrum Disorder (FASD) Prevention: Canadian Perspectives (2008); Division of Childhood and Adolescence; Public Health Agency of Canada: Ottawa, ON, Canada, 2008.
- Reid, N. Fetal alcohol spectrum disorder in Australia: What is the current state of affairs? Drug Alcohol Rev. 2018, 37, 827–830. [Google Scholar] [CrossRef] [PubMed]
- Implementing Trauma- and Violence-Informed Care: A Handbook for Health & Social Services; University of Toronto Press: Toronto, ON, Canada, forthcoming.
- Hubberstey, C.; Rutman, D.; Schmidt, R.A.; Van Bibber, M.; Poole, N. Multi-Service Programs for Pregnant and Parenting Women with Substance Use Concerns: Women’s Perspectives on Why They Seek Help and Their Significant Changes. Int. J. Environ. Res. Public Health 2019, 16, 3299. [Google Scholar] [CrossRef] [Green Version]
- Bodin, M.; Käll, L.; Tydén, T.; Stern, J.; Drevin, J.; Larsson, M. Exploring men’s pregnancy-planning behaviour and fertility knowledge:a survey among fathers in Sweden. Ups. J. Med. Sci. 2017, 122, 127–135. [Google Scholar] [CrossRef]
- McBride, N.; Johnson, S. Fathers’ Role in Alcohol-Exposed Pregnancies: Systematic Review of Human Studies. Am. J. Prev Med. 2016, 51, 240–248. [Google Scholar] [CrossRef]
- Wolfson, L.; Harding, K.; Poole, N. The Role of Partners in Fetal Alcohol Spectrum Disorder Prevention. Available online: https://canfasd.ca/wp-content/uploads/publications/the-role-of-partners-in-fetal-alcohol-spectrum-disorder-prevention.pdf (accessed on 10 September 2019).
- Schölin, L.; Hughes, K.; Bellis, M.A.; Eriksson, C.; Porcellato, L. “I think we should all be singing from the same hymn sheet”—English and Swedish midwives’ views of advising pregnancy women about alcohol. Drugs Educ. Prev. Policy 2018, 26, 394–400. [Google Scholar] [CrossRef]
- Morrison, K.; Wolfson, L.; Harding, K. The Efficacy of Warning Labels on Alcohol Containers for Fetal Alcohol Spectrum Disorder Prevention. Available online: https://canfasd.ca/wp-content/uploads/publications/Warning-Labels-Issue-Paper-Final.pdf (accessed on 7 September 2019).
- Stead, M.; Parkes, T.; Nicoll, A.; Wilson, S.; Burgess, C.; Eadie, D.; Fitzgerald, N.; McKell, J.; Reid, G.; Jepson, R.; et al. Delivery of alcohol brief interventions in community-based youth work settings: Exploring feasibility and acceptability in a qualitative study. BMC Public Health 2017, 17, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathoo, T.; Wolfson, L.; Gelb, K.; Poole, N. New Approaches to Brief Intervention on Substance Use during Pregnancy. Can. J. Midwifery Res. Pract. 2019, 18, 10–21. [Google Scholar]
- Ford-Gilboe, M.; Varcoe, C.; Scott-Storey, K.; Perrin, N.; Wuest, J.; Wathen, C.N.; Case, J.; Glass, N. Longitudinal impacts of an online safety and health intervention for women experiencing intimate partner violence: Randomized controlled trial. BMC Public Health 2020, 20, 260. [Google Scholar] [CrossRef] [Green Version]
- Varcoe, C.; Ford-Gilboe, M.; Browne, A.J.; Perrin, N.; Bungay, V.; McKenzie, H.; Smye, V.; Price Elder, R.; Inyallie, J.; Khan, K.; et al. The Efficacy of a Health Promotion Intervention for Indigenous Women: Reclaiming Our Spirits. J. Interpers Violence 2019, 0886260518820818. [Google Scholar] [CrossRef] [Green Version]
- Carlson, B.E. Best Practices in the Treatment of Substance-Abusing Women in the Child Welfare System. J. Soc. Work Pract. Addict. 2006, 6, 97–115. [Google Scholar] [CrossRef]
- Blakey, J.M. From surviving to thriving: Understanding reunification among African American mothers with histories of addiction. Child. Youth Serv. Rev. 2012, 34, 91–102. [Google Scholar] [CrossRef]
- Howard, H. Experiences of opioid-dependent women in their prenatal and postpartum care: Implications for social workers in health care. Soc. Work Health Care 2016, 55, 61–85. [Google Scholar] [CrossRef]
- Tarasoff, L.A.; Milligan, K.; Le, T.L.; Usher, A.M.; Urbanoski, K. Integrated treatment programs for pregnant and parenting women with problematic substance use: Service descriptions and client perceptions of care. J. Subst Abuse Treat. 2018, 90, 9–18. [Google Scholar] [CrossRef]
- Eggerston, L. Stigma a major barrier to treatment for pregnant women with addictions. Can. Med Assoc. J. 2013, 185, 1562. [Google Scholar]
- Browne, A.J.; Varcoe, C.M.; Fridkin, A. Addressing trauma, violence, and pain: Research on health services for women at the intersections of history and economics. In Health Inequalities in Canada: Intersectional Frameworks and Practices; Hankivsky, O., Ed.; UBC Press: Vancouver, BC, Canada, 2011; pp. 295–311. [Google Scholar]
- Le, T.L.; Kenaszchuk, C.; Milligan, K.; Urbanoski, K. Levels and predictors of participation in integrated treatment programs for pregnant and parenting women with problematic substance use. BMC Public Health 2019, 19, 154. [Google Scholar] [CrossRef] [Green Version]
- Huebner, R.A.; Hall, M.T.; Smead, E.; Willauer, T.; Posze, L. Peer mentoring services, opportunities, and outcomes for child welfare families with substance use disorders. Child. Youth Serv. Rev. 2018, 84, 239–246. [Google Scholar] [CrossRef]
- Huebner, R.A.; Willauer, T.; Posze, L.; Hall, M.T.; Oliver, J. Application of the Evaluation Framework for Program Improvement of START. J. Public Child Welf. 2015, 9, 42–64. [Google Scholar] [CrossRef]
- Doab, A.; Fowler, C.; Dawson, A. Factors that influence mother–child reunification for mothers with a history of substance use: A systematic review of the evidence to inform policy and practice in Australia. Int. J. Drug Policy 2015, 26, 820–831. [Google Scholar] [CrossRef]
- Meixner, T.; Milligan, K.; Urbanoski, K.; McShane, K. Conceptualizing integrated service delivery for pregnant and parenting women with addictions: Defining key factors and processes. Can. J. Addict. 2016, 7, 57–65. [Google Scholar] [CrossRef]
- Grant, T.M.; Ernst, C.C.; Streissguth, A.; Stark, K. Preventing Alcohol and Drug Exposed Births in Washington State: Intervention Findings From Three Parent-Child Assistance Program Sites. Am. J. Drug Alcohol Abuse 2005, 31, 471–490. [Google Scholar] [CrossRef] [PubMed]
- Grant, T.; Christopher Graham, J.; Ernst, C.C.; Michelle Peavy, K.; Brown, N.N. Improving pregnancy outcomes among high-risk mothers who abuse alcohol and drugs: Factors associated with subsequent exposed births. Child. Youth Serv. Rev. 2014, 46, 11–18. [Google Scholar] [CrossRef]
- Grant, T.; Ernst, C.C.; Pagalilauan, G.; Streissguth, A. Postprogram follow-up effects of paraprofessional intervention with high-risk women who abused alcohol and drugs during pregnancy. J. Community Psychol. 2003, 31, 211–222. [Google Scholar] [CrossRef]
- L’Espérance, N.; Bertrand, K.; Perreault, M. Cross-training to work better together with women in Quebec who use substances: Care providers’ perceptions. Health Soc. Care Community 2017, 25, 505–513. [Google Scholar] [CrossRef]


{kind=link}
| Level of Stigma | How Stigma is Operationalized | |
|---|---|---|
| Individual | Person who experiences stigma | Unfair treatment Internalized feelings of shame and guilt Anticipated stigma (e.g., may not access support) |
| Interpersonal | Family, friends, social networks, healthcare and social service providers | Using derogatory or dehumanizing language Intrusive attention and questions Hate crimes and assault |
| Institutional | Health system organizations, health, community, and social service organizations | Restrictions to care based on behaviours or sociodemographic status Unwelcoming or unsafe environments Institutional policies that cause harm (e.g., low investment of services; unnecessary drug tests) |
| Population | Mass media, policies, and law | Societal norms and values Widely held stereotypes Discriminatory laws and policies Inadequate legal protection (or lack of enforcement) |
| Author(s) & Year | Country | Method (Orientation, Data Collection, Analysis) | Population(s) | Research Aim | COREQ Critical Appraisal |
|---|---|---|---|---|---|
| Barbour (1990) [43] | USA | Semi-structured interviews | 20 women in their third trimester of pregnancy | Explore the drinking behaviours and factors that influence alcohol use among pregnant women | Partially fulfilled |
| Baxter et al. (2004) [44] | USA | Semi-structured interviews; thematic analysis | 60 lower-income women who were pregnant or <12 months postpartum and resided in rural Iowa | Identify women’s attitudes, beliefs, and behaviours around alcohol and pregnancy | Partially fulfilled |
| Bianchini et al. (2020) [52] | Brazil | Semi-structured interviews; thematic content analysis | 14 pregnant women who received prenatal care | Investigate the perceptions of the advice pregnant women received from prenatal care providers about alcohol and tobacco use during pregnancy | Inadequately fulfilled |
| Branco and Kaskutas (2001) [45] | USA | Focus groups; thematic analysis | 11 pregnant and recently postpartum Indigenous and Black women | Understand women’s beliefs and opinions regarding alcohol use during pregnancy | Inadequately fulfilled |
| Brudenell (1996 & 1997) [33,34] | USA | Grounded theory; participant observation, semi-structured interview, diaries; constant comparative analysis | 11 women who self-identified as alcoholics/addicts in recovery and were pregnant or recently postpartum (5 pregnant, 6 with infants younger than one year) | Explore women’s concurrent experiences of alcohol and drug use recovery and the transition to parenthood | Partially fulfilled |
| Crawford-Willams et al. (2016) [30] | Australia | Focus groups; thematic analysis | 9 pregnant women and 8 women who were 4–20 weeks postpartum | Identify knowledge gaps about the effects of alcohol use in pregnancy among pregnant and recently postpartum women, and their partners | Partially fulfilled |
| France et al. (2013) [39] | Australia | Focus group; thematic analysis | 23 women who were pregnant, <3 years postpartum, or were considering pregnancy. Mothers and prospective mothers had to have screened positive for alcohol use in the previous month. | Identify effective population-level messaging strategies to prevent prenatal alcohol exposure | Partially fulfilled |
| Gibson et al. (2020) [29] | Australia | Interviews and focus groups; content analysis | 14 Indigenous and 15 non-Indigenous pregnant women aged 18+ years | Explore influences on pregnant women’s alcohol decision-making in a population with frequent and heavy peer drinking | Partially fulfilled |
| Gouilhers et al. (2019) [37] | Switzerland | Semi-directive joint interviews; thematic analysis | 30 couples expecting their first baby in French Switzerland. Couples were not included if mothers did not drink alcohol prior to pregnancy or had an alcohol use disorder | Explore pregnant women and their partner’s experiences of pregnancy related alcohol behaviour change | Partially fulfilled |
| Grant et al. (2019) [47] | United Kingdom | Visual data production (timelines, collaging, and dyad sandboxes); elicitation interviews; thematic analysis | 10 pregnant women who lived in the highest quintile of deprivation (Welsh Index of Multiple Deprivation) and were claiming welfare benefits | Understand pregnant women from low-income communities’ health experiences during pregnancy | Fulfilled |
| Hammer and Inglin (2014) [50] | Switzerland | Semi-structured interviews; thematic analysis | 50 pregnant women experiencing healthy pregnancies in French Switzerland | Identify pregnant women’s perceptions of the risks of alcohol and tobacco use during pregnancy | Inadequately fulfilled |
| Hammer (2019) [38] | Switzerland | See Gouilhers (2019) | See Gouilhers (2019) | Understand couples’ risk management related to alcohol use during pregnancy | Partially fulfilled |
| Hocking, O’Callaghan and Reid (2019) [40] | Australia | Phenomenological; semi-structured interview | 12 women who attended an initial prenatal appointment within the past two years | Explore and interpret the messages women receive regarding alcohol use during their first prenatal care visit | Partially fulfilled |
| Holland, McCallum and Walton (2016) [41] | Australia | Semi-structured interviews and focus groups | 20 women who were pregnant, recently postpartum, or were planning a pregnancy | Examine pregnant women’s experiences of alcohol consumption and their perspectives on related health advice | Inadequately fulfilled |
| Jones et al. (2011) [35] | Australia | Semi-structured interviews | 12 midwives and 12 pregnant women | Explore midwives’ advice regarding alcohol consumption, how it corresponds to the National Health and Medical Research Council (NHMRC) Low-Risk Drinking Guidelines, and how pregnant women understand and interpret the advice | Partially fulfilled |
| Jones and Telenta (2012) [36] | Australia | Semi-structured interviews | See Jones et al. (2011) | Explore attitudes around alcohol consumption during pregnancy and factors that may impact women’s ability to follow the recommendations to abstain from alcohol while pregnant | Inadequately fulfilled |
| Kelly and Ward (2018) [49] | South Africa | Episodic interviews, focus groups; thematic decomposition analysis | 14 pregnant or recently postpartum women who were identified as binge drinkers, dependent on, or addicted to alcohol during pregnancy (using the AUDIT screening tool) and were enrolled in the Healthy Mother Healthy Baby programme and 13 community members (4 men, 9 women) ages 18+ | Identify social representations of alcohol use among women who drank alcohol while pregnant | Partially fulfilled |
| Martinelli et al. (2019) [51] | Brazil | Semi-structured interviews; thematic content analysis | 14 pregnant women who were identified as at-risk drinkers during pregnancy (using the Brazilian validated revised T-ACE screening tool) | Explore the motivations behind abstinence and alcohol consumption during pregnancy | Partially fulfilled |
| Meurk et al. (2014) [42] | Australia | Semi-structured interviews; framework analysis | 40 pregnant and recently postpartum women, ages 34–39, from the Australia Longitudinal Study on Women’s Health | Contextualize how women understand their personal identity and act upon risk perceptions related to alcohol use during pregnancy | Partially fulfilled |
| Pati et al. (2018) [54] | India | Structured interviews 1, focus groups; thematic analysis | 19 women who were lactating in the past three months and reported alcohol consumption during pregnancy, 18 family members, and 20 local community leaders and frontline workers | Explore the beliefs and perceptions of women from the Santal and Munda tribes around alcohol use in pregnancy | Fulfilled |
| Raymond et al. (2009) [48] | United Kingdom | Semi-structured interviews; thematic analysis | 20 pregnant women | Explore pregnant women’s attitudes around alcohol use in pregnancy and towards sources of information about alcohol use in pregnancy following changes in government guidance | Partially fulfilled |
| Schölin et al. (2017) [56] | United Kingdom, Sweden | Socio-ecological; semi-structured interviews; thematic analysis | 21 parents in England and 22 parents in Sweden with an infant <18 months | Examine perceptions and practices of alcohol use during pregnancy in England and Sweden | Partially fulfilled |
| Sheridan (2018) [46] | USA | Grounded theory; mixed-methods 2, survey, semi-structured interviews; content analysis | 14 pregnant or parenting girls, ages 13–19 years, enrolled in an alternative high school for pregnant and parenting girls | Explore the experiences and perceptions of substance use, pregnancy, and motherhood among young mothers | Partially fulfilled |
| Toutain (2010) [53] | France | Online chat rooms; Thematic analysis | 42 pregnant women in three Internet chat rooms | Identify future mothers’ perceptions of alcohol consumption during pregnancy through Internet chat rooms | Inadequately fulfilled |
| Van der Wulp, Hoving and de Vries (2013) [55] | The Netherlands | Focus groups and semi-structured interviews 3; content analysis | 25 pregnant women and 9 partners | Explore what information pregnant women and their partners receive about alcohol in pregnancy from their partners | Partially fulfilled |
| Watt et al. (2014) [28] | South Africa | Semi-structured interviews; thematic analysis | 12 pregnant and 12 women <12 months postpartum, aged 18+ years | Examine the experiences of pregnant and postpartum South African women who reported alcohol consumption during pregnancy | Partially fulfilled |
| Themes and Subthemes | Individual | Interpersonal | Institutional | Population | |
|---|---|---|---|---|---|
| Social relationships and norms | Unsupportive | Feeling as though there are a lack of alternatives to alcohol use Perception that alcohol use is not risky/harmful | Lack of support from friends, family, and partners to reduce alcohol use Partners unchanged alcohol use Normalized alcohol use in social situations | Abstinence-only policies | Unsupportive norms favouring alcohol use in moderation Misinformation Lack of awareness regarding harms of alcohol use and FASD |
| Supportive | Personal strengths Feeling connected to the fetus/baby | Support from others to reduce/abstain from alcohol Joint alcohol use decisions with partners | Abstinence-related policies Non-judgmental care | Supportive social norms that normalize alcohol reduction | |
| Harm reducing institutional policies/culture | |||||
| Stigma (as a barrier to reducing alcohol use in pregnancy) | Limited self-esteem/capacity to seek support Internalized stigma (limiting self-esteem/capacity to seek support) | Judgement related to alcohol use in pregnancy Belief that alcohol use in pregnancy results in an inability to parent | Punitive institutional policies that prompt child welfare or justice involvement | Dichotomous notions of ‘good’ and ‘bad’ mothers | |
| Discriminatory institutional practices that prejudice based on SES, ethnocultural identity, pregnancy status, alcohol or substance use, or mental health | Discrimination related to SES, gender, mental health status Punitive laws and policies Racism Punitive approaches for alcohol use | ||||
| Trauma and Stressors (as barriers to reducing alcohol use in pregnancy) | Alcohol as a coping mechanism Feeling unsafe Feeling disconnected from the fetus/baby | Lack of trusted relationships/social support network Lack of safety due to another External expressions of trauma Domestic and intimate partner violence | Lack of access to essential resources | Colonial policies Intergenerational trauma Structural disparities (e.g., poverty) | |
| Lack of outreach/access to care Intergenerational/recent institutional trauma Institutional lack of safety | |||||
| Alcohol messaging and information | Harmful | Confusion around how to interpret information See internalized stigma and trauma | Conflicting, unclear and/or harmful messaging from healthcare providers, friends, and family Limited provision of brief interventions and health information related to pregnancy and alcohol use | Abstinence-only, judgmental, and stigmatizing alcohol use messaging, education and policy Gendered care that is only geared towards women’s health | Unclear and evolving national alcohol use policies and guidelines Stigmatizing public alcohol abstinence messages Lack of awareness harms of alcohol use and FASD |
| Gendered policies that frame preconception and prenatal care as a women’s-only issue | |||||
| Harm Reducing | See supportive relationships and norms | Receiving trusted, clear and consistent messaging from healthcare providers | Trauma-informed, harm reducing, non-stigmatizing messaging and policy Patient-oriented care/information Integration of partners in prenatal care | Harm reduction-oriented policies and guidelines for alcohol use during pregnancy Harm reducing mass media campaigns and messaging | |
| Access to trusted, equitable care and essential resources (facilitating alcohol reduction/abstinence in pregnancy) | Access to care without fear of failing to reduce alcohol use | Supportive relationships Support accessing resources Consistent access to prenatal care | Adoption of harm reduction oriented, gender-, violence-, and trauma-informed practice Holistic and integrated pregnancy care Addressing structural disparities Adoption of patient-oriented care Integration of partners in prenatal care | Laws, policies and media supporting women and men’s health and wellbeing Structural security Gender transformative interventions and campaigns for men | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyall, V.; Wolfson, L.; Reid, N.; Poole, N.; Moritz, K.M.; Egert, S.; Browne, A.J.; Askew, D.A. “The Problem Is that We Hear a Bit of Everything…”: A Qualitative Systematic Review of Factors Associated with Alcohol Use, Reduction, and Abstinence in Pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 3445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073445
Lyall V, Wolfson L, Reid N, Poole N, Moritz KM, Egert S, Browne AJ, Askew DA. “The Problem Is that We Hear a Bit of Everything…”: A Qualitative Systematic Review of Factors Associated with Alcohol Use, Reduction, and Abstinence in Pregnancy. International Journal of Environmental Research and Public Health. 2021; 18(7):3445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073445
Chicago/Turabian StyleLyall, Vivian, Lindsay Wolfson, Natasha Reid, Nancy Poole, Karen M. Moritz, Sonya Egert, Annette J. Browne, and Deborah A. Askew. 2021. "“The Problem Is that We Hear a Bit of Everything…”: A Qualitative Systematic Review of Factors Associated with Alcohol Use, Reduction, and Abstinence in Pregnancy" International Journal of Environmental Research and Public Health 18, no. 7: 3445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073445