
COVID-Well Study: Qualitative Evaluation of Supported Wellbeing Centres and Psychological First Aid for Healthcare Workers during the COVID-19 Pandemic

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants and Setting
2.3. The Supported Wellbeing Centres
2.4. Procedure
2.5. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Qualitative Interviews
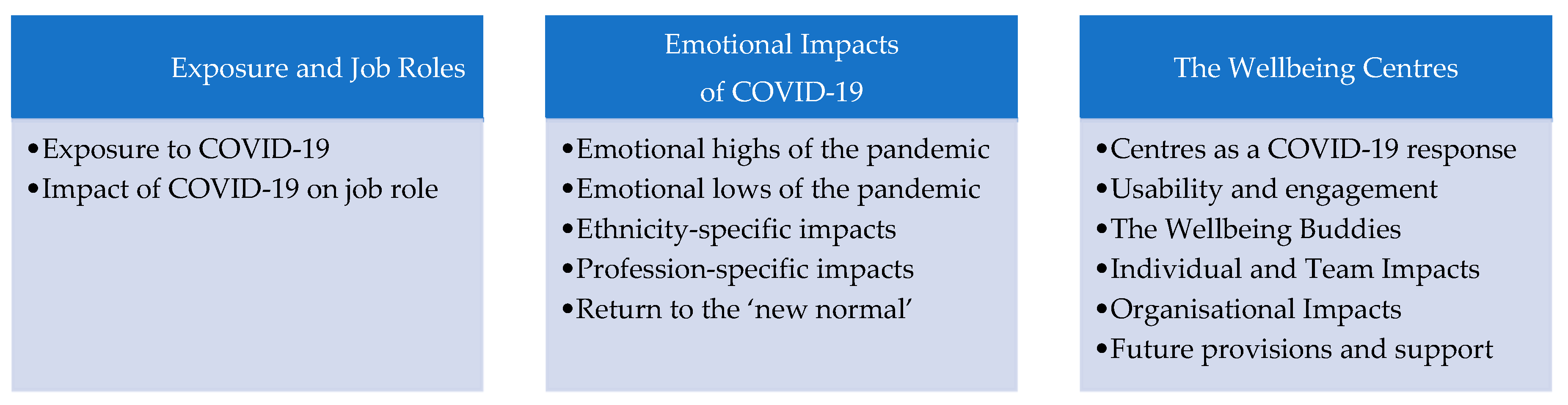
3.2.1. Exposure and Job Roles
Exposure to COVID-19
COVID-19 Impact on Job Role
3.2.2. Emotional Impact of COVID-19
Emotional Highs of the Pandemic
Emotional Lows of the Pandemic
Ethnicity-Specific Impacts
Profession-Specific Impacts
Return to the New Normal
3.2.3. The Wellbeing Centres
Centres as a Workplace COVID-19 Response
Usability and Engagement
“So usually my breaks weren’t longer than half an hour and by the time you’d finished task, got off the ward, you know, taken off your PPE, washed your hands, made your way to the wellbeing centre, you weren’t able to actually be there for a very long period of time before coming back, so if I was, had been particularly run of my feet in the lead up to my break, sometimes it was easier just to sit on the chairs in our normal staffroom on the ward, because that would be a longer period of rest than it was to move over to the wellbeing centre.”(ID129)
“As soon as you walk in, the volunteers rushing you a drink and a chat if you need it and, and any support. And yeah, it’s really nice and I think it’s nice to encourage each other as a team and to remember that the wellbeing centers are there, and that they are there for--to use them--if you need them.”(ID147)
“I used the wellbeing centre because I did a COVID debrief with all of them individually took them off the ward to the wellbeing centre and just sat down and had 20 min half an hour with them after we’d come out or gone into this new pathway just to say ‘how are you?’ ‘how did you find it?’, ‘what could we learn’ ‘what could we have done differently?”(ID123)
“…we saw lots of nurses, doctors, front line staff coming in and just really just sitting for 15, 20 min having a coffee, getting away from…the imminent danger and the imminent pressure from what they’re actually doing on the front line.”(ID135)
The Wellbeing Buddies
“…being able to be what I would call useful at a time of crisis when I am not a frontline member of staff and I’m not clinical. Erm, but that helped me to see that at work I was making a difference.”(ID101)
“…making connections with more people across the hospital and understanding, um, other people’s roles because I, I think that is always beneficial, because people work in silence and never understand what people do.”(ID101)
“my fellow buddies were people that I didn’t know, they weren’t from my own service, so it gave me an opportunity to meet some other people and to meet some frontline staff.”(ID104)
“The training was really useful and I think everybody should have to go on it, I just think it helps people see things. The training was very simple … it was just nice, insightful, easy to understand. A lot of people are so busy that that they don’t take the time to just sit and watch and listen … the training … it just made you see different things.”(ID105)
“I think most importantly they’re just someone to listen, they can’t fix all the problems and everything like that, but, they’re people to listen and offload on to and you know, problem shared, problem halved.”(ID129)
“Well I’ve used them a lot, erm, because I was obviously going through a lot of, you know, stuff in my head…and I found them [centres] very relaxing. To go in there and just be able to just talk a few things through … it certainly gave, err, people a bit of tranquility.”(ID115)
Individual and Team Impacts
“the lighting was fantastic, they had calming music in there, you had some individual booths where if you wanted your solitude you could go into sort of a couple of booth areas where you could just sit by yourself if you wanted to.”(ID135)
“I actually found it quite nice to talk to people in there…you got to hear a lot of people how they were coping with things, and…it did make me feel a little bit better with what was going on in my life thinking I’m not really alone.”(ID115)
“When we were boiling in our own blood walking around the place, the wellbeing centre seemed to be just this cool, gently lit, quiet, calm corner that you could just step into and as soon as you walked through the door you felt yourself relax, you felt your shoulders go down, you felt yourself breathe easier and there you’d have these lovely people saying ‘hi how are you? can we get you anything? have a seat we’ll bring your tea to you.’”(ID132)
“I would have got more upset if I hadn’t gone into the wellbeing centre. So being able to go onto that ward and you know, go-go back to somewhere, even though it wasn’t really anything to do with COVID. Being able to go back and face going in without immediately bursting into tears which is, I think probably what I would have done had I not had the chance go into the- into the wellbeing centre.”(ID118)
“Absolutely essential… just life-savers, literally, um giving us space to sit down and the ability to replenish on fluids and sometimes food.”(ID131)
Organizational Impacts
“I’m really impressed with the Trust full stop, particularly because of COVID and how they’ve reacted.”(ID118)
“Told them [buddy] about obviously how I was feeling and how mentally I was absolutely drained ... what was going on and ... it was nice to chat I have to admit.”(ID115)
“We’ve had staff in the past that are still stuck with ... work-related stress and I think this really helps support those people.”(ID147)
“Makes a team work better together and is more cohesive and is better understanding I think surely that’s got to be safer and beneficial to patient care.”(ID131)
“My team leader has been excellent, he said to me, look whenever you’re feeling you need a bit of a pick me up then go there, so he’s been really good. I’ve been quite lucky because my team leader has been very supportive.”(ID115)
“There has to be, um, senior leadership always, because …if you have got a senior leader who is not invested and …quite cynical about it [wellbeing]… ”(ID118)
Future Provisions and Support
“The problem we have got is that because they have all people whose main role was ramped down when the pandemic started, we’re going to start losing them to their main job.”(ID120)
“You’d definitely want someone that had … even beginning [level] person-centred sort of skills in counselling so that they knew how to, you know, let someone talk and how to actively listen …and then on top of that if you could have some ... erm ... HR or-or some sort of other personnel skills that would be sort of ideal I think... You can ask people to volunteer, erm but you obviously then aren’t guaranteed the quality and the skillset that you’re really looking for.”(ID131)
“Some mistakes about accepting donations because that meant that there were people, you know, tens of people queuing to get whatever it was, the freebee that had been delivered that day.”(ID101)
“There was just people who … were happy with someone just making them a drink, err, you know, maybe just have some chit chat … they did have people who had a bit of a wobble and what have you … I’m not sure whether the two should be combined or whether they should be separate.”(ID104)
“Going to need to increase the funding so that they [the trust] can meet the needs of the staff …because I think we’re gonna’ experience more requests than they’re used to, and that might over-run them, because if people can receive support early and get that early intervention, they may need less help in the long run, and be able to stay in work, recover quicker, etcetera. So we don’t want people trying to access support but feeling like they can’t get it.”(ID129)
4. Discussion
4.1. Exposure and Job Roles
4.2. Emotional Impacts of COVID-19
4.3. The Wellbeing Centres
4.4. Study Considerations
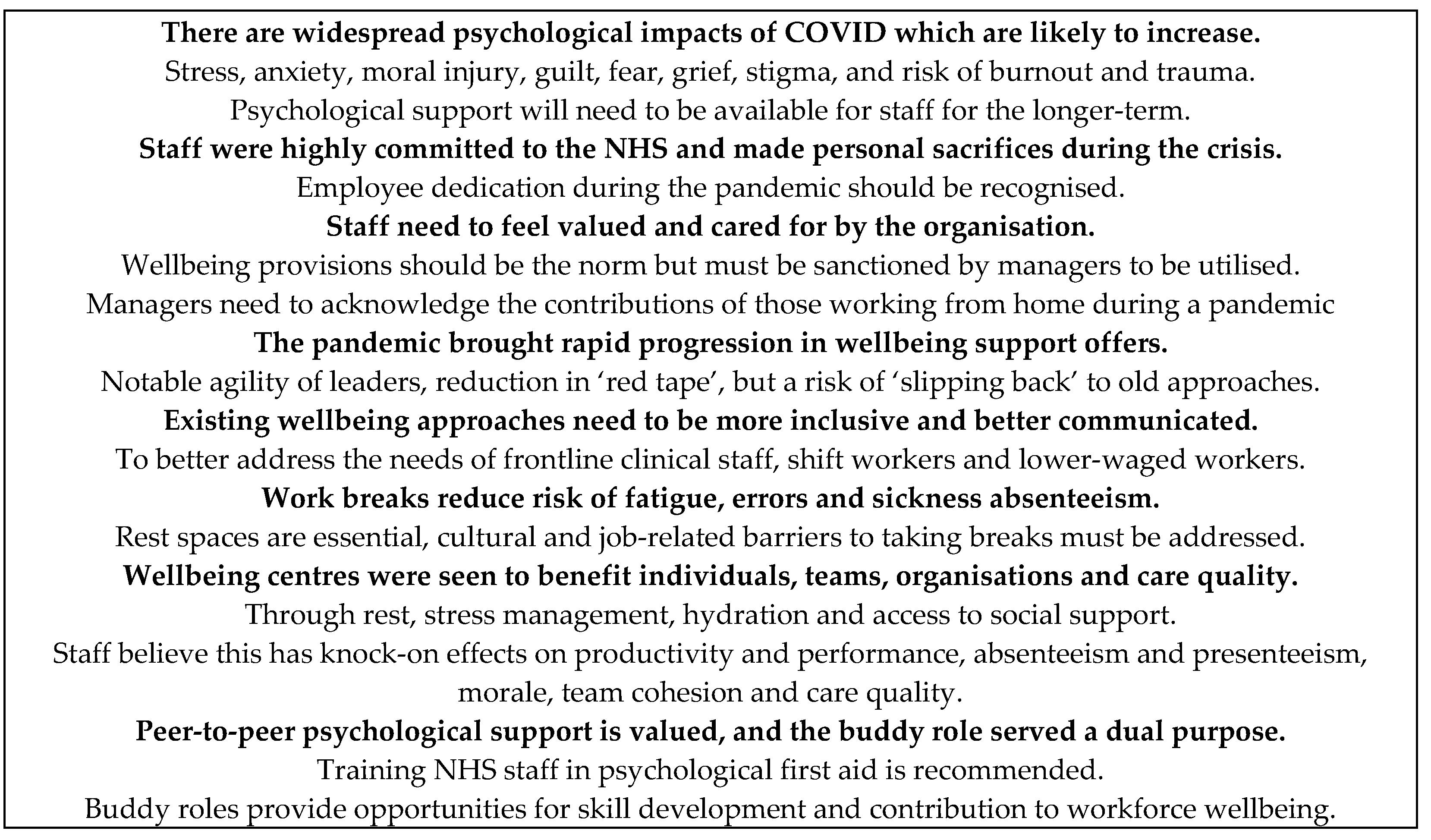
4.5. Summary of Key Findings and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, 1642. [Google Scholar] [CrossRef]
- Cabarkapa, S.; Nadjidai, S.E.; Murgier, J.; Ng, C.H. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain Behav. Immun. Health 2020, 8, 100144. [Google Scholar] [CrossRef]
- Krishnamoorthy, Y.; Nagarajan, R.; Saya, G.K.; Menon, V. Prevalence of psychological morbidities among general population, healthcare workers and COVID-19 patients amidst the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2020, 293, 113382. [Google Scholar] [CrossRef]
- de Pablo, G.S.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Sanghera, J.; Pattani, N.; Hashmi, Y.; Varley, K.F.; Cheruvu, M.S.; Bradley, A.; Burke, J.R. The impact of SARS-CoV-2 on the mental health of healthcare workers in a hospital setting-A Systematic Review. Occup. Health 2020, 62, e12175. [Google Scholar] [CrossRef]
- Stuijfzand, S.; Deforges, C.; Sandoz, V.; Sajin, C.T.; Jaques, C.; Elmers, J.; Horsch, A. Psychological impact of an epidemic/pandemic on the mental health of healthcare professionals: A rapid review. BMC Public Health 2020, 20, 1230. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Bermingham, F.; Johnson, G.; Tabner, A. Mitigating the Psychological Impact of COVID-19 on Healthcare Workers: A Digital Learning Package. Int. J. Environ. Res. Public Health 2020, 17, 2997. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Vicente, M.A.; Lopez-Pineda, A.; Carrillo, I.; Guilabert, M.; Fernández, C.; Pérez-Jover, V.; Delgado, J.M.; Pérez-Pérez, P.; Vargas, A.C.; et al. Preventing and Addressing the Stress Reactions of Health Care Workers Caring for Patients With COVID-19: Development of a Digital Platform (Be + Against COVID). JMIR Mhealth Uhealth 2020, 8, e21692. [Google Scholar] [CrossRef]
- Albott, S.; Wozniak, J.R.; McGlinch, B.P.; Wall, M.H.; Gold, B.S.; Vinogradov, S. Battle Buddies: Rapid Deployment of a Psychological Resilience Intervention for Health Care Workers During the COVID-19 Pandemic. Anesth. Analg. 2020, 131, 43–54. [Google Scholar] [CrossRef]
- Heath, C.; Sommerfield, A.; von Ungern-Sternberg, B.S. Resilience strategies to manage psychological distress among healthcare workers during the COVID-19 pandemic: A narrative review. Anaesthesia 2020, 75, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.; Campbell, P.; Cheyne, J.; Cowie, J.; Davis, B.; McCallum, J.; McGill, K.; Elders, A.; Hagen, S.; McClurg, D.; et al. Interventions to support the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic: A mixed methods systematic review. Cochrane Database Syst. Rev. 2020, 5, CD013779. [Google Scholar]
- Shah, K.; Bedi, S.; Onyeaka, H.; Singh, R.; Chaudhari, G. The Role of Psychological First Aid to Support Public Mental Health in the COVID-19 Pandemic. Cureus 2020, 12, e8821. [Google Scholar] [CrossRef]
- Sijbrandij, M.; Horn, R.; Esliker, R.; O’May, F.; Reiffers, R.; Ruttenberg, L.; Stam, K.; de Jong, J.; Ager, A. The Effect of Psychological First Aid Training on Knowledge and Understanding about Psychosocial Support Principles: A Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Everly, G.S., Jr.; Flynn, B.W. Principles and practical procedures for acute psychological first aid training for personnel without mental health experience. Int. J. Emerg. Ment. Health 2006, 8, 93–100. [Google Scholar] [PubMed]
- IFRC. Remote Psychological First Aid during COVID; Reference Centre for Psychosocial Support: Copenhagen, Denmark, 2020. [Google Scholar]
- Maunder, R.G.; Leszcz, M.; Savage, D.; Adam, M.A.; Peladeau, N.; Romano, D.; Rose, M.; Schulman, B. Applying the lessons of SARS to pandemic influenza: An evidence-based approach to mitigating the stress experienced by healthcare workers. J. Public Health 2008, 99, 486–488. [Google Scholar] [CrossRef]
- Veronese, G.; Cavazzoni, F.; Cavalera, C.M.; Deprà, C.; Deseri, G.; Pepe, A.; Farina, E.; Firenze, D.; Scheriani, D.; Luraschi, S.; et al. Rapid response to: Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368. [Google Scholar] [CrossRef] [Green Version]
- Blake, H.; Remote Healthcare Options for Employees are Rapidly Expanding. Employee Benefits, 25 June. Available online: https://employeebenefits.co.uk/dr-holly-blake-remote-healthcare-employees/ (accessed on 5 February 2021).
- Sulaiman, A.H.; Sabki, Z.A.; Jaafa, M.J.; Francis, B.; Razali, K.A.; Rizal, A.J.; Mokhtar, N.H.; Juhari, J.A.; Zainal, S.; Ng, C.G. Development of a Remote Psychological First Aid Protocol for Healthcare Workers Following the COVID-19 Pandemic in a University Teaching Hospital, Malaysia. Healthcare 2020, 8, 228. [Google Scholar] [CrossRef]
- Department of Health and Social Care. Press Release: Psychological First Aid in Emergencies Training for Frontline Staff and Volunteers. 15 June. Available online: https://www.gov.uk/government/news/psychological-first-aid-in-emergencies-training-for-frontline-staff-and-volunteers (accessed on 31 December 2020).
- Rajamohan, S.; Davis, C.R.; Ader, M. REST: Break through to resilience. Nursing 2020, 50, 53–56. [Google Scholar] [CrossRef]
- Sagherian, K.; Steege, L.M.; Cobb, S.J.; Cho, H. Insomnia, fatigue and psychosocial well-being during COVID-19 pandemic: A cross-sectional survey of hospital nursing staff in the United States. J. Clin. Nurs. 2020. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake, H.; Yildirim, M.; Wood, B.; Knowles, S.; Mancini, H.; Coyne, E.; Cooper, J. COVID-Well: Evaluation of the Implementation of Supported Wellbeing Centres for Hospital Employees during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9401. [Google Scholar] [CrossRef]
- Kallio, H.; Pietilä, A.-M.; Johnson, M.; Kangasniemi, M. Systematic methodological review: Developing a framework for a qualitative semi-structured interview guide. J. Adv. Nurs. 2016, 72, 2954–2965. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furber, C. Framework analysis: A method for analysing qualitative data. Afr. J. Midwifery Women’s Health 2013, 4, 2. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.; Goldblatt, P.; Herd, E.; Morrison, J. Build. Back Fairer: The COVID-19 Marmot Review. The Pandemic, Socioeconomic and Health Inequalities in England; Institute of Health Equity: London, UK, 2020. [Google Scholar]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, X.B. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Cawcutt, K.A.; Starlin, R.; Rupp, M.E. Fighting fear in healthcare workers during the COVID-19 pandemic. Infect. Control. Hosp. Epidemiol. 2020, 25, 1–2. [Google Scholar] [CrossRef]
- Ho, S.M.; Kwong-Lo, R.S.; Mak, C.W.; Wong, J.S. Fear of severe acute respiratory syndrome (SARS) among health care workers. J. Consult. Clin. Psychol. 2005, 73, 344–349. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.J.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Coronavirus Pandemic Epidemiology Consortium. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers: A Living Rapid Review. Ann. Intern. Med. 2020, 173, 120–136. [Google Scholar] [CrossRef]
- Karlsson, U.; Fraenkel, C.J. Covid-19: Risks to healthcare workers and their families. BMJ 2020, 371, 3944. [Google Scholar] [CrossRef]
- Shah, A.S.V.; Wood, R.; Gribben, C.; Cadwell, D.; Bishop, J.; Weir, A.; Kennedy, S.; Martin, R.; Palmer-Smith, A.; Goldberg, D.; et al. Risk of hospital admission with coronavirus disease 2019 in healthcare workers and their households: Nationwide linkage cohort study. BMJ 2020, 371, 3582. [Google Scholar] [CrossRef] [PubMed]
- Bagcchi, S. Stigma during the COVID-19 pandemic. Lancet Infect. Dis. 2020, 20, 782. [Google Scholar] [CrossRef]
- American Nurses Association. Update on Nurses and PPE: Survey Reveals Alarming Conditions. Available online: https://www.nursingworld.org/~4a558d/globalassets/covid19/ana-ppe-survey-one-pager---final.pdf (accessed on 19 February 2021).
- Tonkin, T.; Call for Enhanced PPE. British Medical Association. Available online: https://www.bma.org.uk/news-and-opinion/call-for-enhanced-ppe (accessed on 4 January 2021).
- Gemine, R.; Davies, G.R.; Tarrant, S.; Davies, R.M.; James, M.; Lewis, K. Factors associated with work-related burnout in NHS staff during COVID-19: A cross-sectional mixed methods study. BMJ Open 2021, 28, e042591. [Google Scholar] [CrossRef]
- Mistry, P.; The digital revolution: Eight technologies that will change health and care. The Kings Fund, 13 November. Available online: https://www.kingsfund.org.uk/publications/digital-revolution (accessed on 19 February 2021).
- Tsao, N.; Hayward, J. COVID-19 Brings Unprecedented Shifts in Healthcare Technology Adoption. IdTechX, Dec 7. Available online: https://www.idtechex.com/en/research-article/covid-19-brings-unprecedented-shifts-in-healthcare-technology-adoption/22322 (accessed on 5 February 2021).
- Bateman, M.E.; Hammer, R.; Byrne, A.; Ravindran, N.; Chiurco, J.; Lasky, S.; Denson, R.; Brown, M.; Myers, L.; Zu, Y.; et al. Death Cafés for prevention of burnout in intensive care unit employees: Study protocol for a randomized controlled trial (STOPTHEBURN). Trials 2020, 21, 1019. [Google Scholar] [CrossRef] [PubMed]
- Dean, W.; Jacobs, B.; Manfredi, R.A. Moral Injury: The Invisible Epidemic in COVID Health Care Workers. Ann. Emerg. Med. 2020, 76, 385–386. [Google Scholar] [CrossRef]
- Litz, B.T.; Stein, N.; Delaney, E.; Lebowitz, L.; Nash, W.P.; Silva, C.; Maguen, S. Moral injury and moral repair in war veterans: A preliminary model and intervention strategy. Clin. Psychol. Rev. 2009, 29, 695–706. [Google Scholar] [CrossRef]
- Hines, S.E.; Chin, K.H.; Glick, D.R.; Wickwire, E.M. Trends in Moral Injury, Distress, and Resilience Factors among Healthcare Workers at the Beginning of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 488. [Google Scholar] [CrossRef] [PubMed]
- Corley, M.C.; Elswick, R.K.; Gorman, M.; Clor, T. Development and evaluation of a moral distress scale. J. Adv. Nurs. 2001, 33, 250–256. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, 1211. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, E.; Chadwick, R.; Goodrich, J.; Ford, C.; Wickens, R. Reflection for all healthcare staff: A national evaluation of Schwartz rounds. J. Interprof. Care 2020, 34, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Falcó-Pegueroles, A.; Rosa, D.; Tolotti, A.; Graffigna, G.; Bonetti, L. The psychosocial impact of flu influenza pandemics on healthcare workers and lessons learnt for the COVID-19 emergency: A rapid review. Int. J. Public Health 2020, 65, 1205–1216. [Google Scholar] [CrossRef]
- Dye, T.D.; Alcantara, L.; Siddiqi, S.; Barbosu, M.; Sharma, S.; Panko, T.; Pressman, E. Risk of COVID-19-related bullying, harassment and stigma among healthcare workers: An analytical cross-sectional global study. BMJ Open 2020, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Chopra, K.K.; Arora, V.K. Covid-19 and social stigma: Role of scientific community. Indian J. Tuberc. 2020, 67, 284–285. [Google Scholar] [CrossRef] [PubMed]
- Hafner, M.; Van Stolk, C.; Saunders, C.L.; Krapels, J.; Baruch, B. Health, Wellbeing and Productivity in the Workplace: A Britain’s Healthiest Company Summary Report May 22, RAND Corporation. Available online: https://www.rand.org/pubs/research_reports/RR1084.html (accessed on 5 February 2021).
- Deloitte. Mental Health and Employers: Refreshing the Case for Investment; Deloitte: London, UK, 2020. [Google Scholar]
- Hassard, J.; Toeh, K.; Thomson, L.; Blake, H. Understanding the cost of mental health at work: An integrative framework. In The SAGE Handbook of Organisational Wellbeing SAGE; Wall, T., Cooper, C.L., Brough, P., Eds.; SAGE: London, UK, in press.
- Vindrola-Padros, C.; Andrews, L.; Dowrick, A.; Djellouli, N.; Fillmore, H.; Gonzalez, E.B.; Javadi, D.; Lewis-Jackson, S.; Manby, L.; Mitchinson, L.; et al. Perceptions and experiences of healthcare workers during the COVID-19 pandemic in the UK. BMJ Open 2020, 10, e040503. [Google Scholar] [CrossRef]
- Voon, J.; Helping ‘Shielded’ Staff to Continue to Contribute. Nursing and Midwifery COVID-19 Catalogue of Change. NHS England. Available online: https://www.england.nhs.uk/nursingmidwifery/shared-governance-and-collective-leadership/nursing-covid-19-catalogue-of-change/helping-shielded-staff-to-continue-to-contribute/ (accessed on 5 February 2021).
- Chattopadhyay, I.; Davies, G.; Adhiyaman, V. The Contributions of NHS Healthcare Workers Who are Shielding or Working from Home during COVID-Future Healthcare Journal. Available online: https://www.rcpjournals.org/content/futurehosp/7/3/e57 (accessed on 5 February 2021).
- Bailey, S.; West, M. Covid-19: Why Compassionate Leadership Matters in a Crisis; The Kings Fund: London, UK, 2020. [Google Scholar]
- Lindsay, K.J.; Leonard, D.A.; Higgins, G.C.; Robertson, E.; Perks, G. Invited editorial from the social media editor of JPRAS. Leadership in the time of COVID-J Plast Reconstr. Aesthet. Surg. 2020, 73, 1405–1408. [Google Scholar] [CrossRef]
- Santosa, A.; Cross, G.; Oon, J.E.L.; Archuleta, S.; Dan, Y.Y. Coronavirus 2019 Silver Linings. Open Forum Infect. Dis. 2020, 12, 230. [Google Scholar] [CrossRef]
- Blake, H.; Lloyd, S. Influencing organizational change in the NHS: Lessons learned from workplace wellness initiatives in practice. Qual. Prim. Care 2008, 16, 449–455. [Google Scholar]
- Lee, S.; Blake, H.; Lloyd, S. The Price is Right: Making Workplace Wellness Financially Sustainable. Int. J. of Workplace Health Manag. 2010, 3, 58–69. [Google Scholar] [CrossRef]
- Blake, H.; Zhou, D.; Batt, M.E. Five-year workplace wellness intervention in the NHS. Perspect Public Health 2013, 133, 262–271. [Google Scholar] [CrossRef]
- Ryde, G.C.; Atkinson, P.; Stead, M.; Gorely, T.; Evans, J.M.M. Physical activity in paid work time for desk-based employees: A qualitative study of employers’ and employees’ perspectives. BMC Public Health 2020, 20, 460. [Google Scholar] [CrossRef]
- Chatfield, C. Give us a break. BMJ 2019, 364, l481. [Google Scholar] [CrossRef]
- Royal College of Physicians. Being a Junior Doctor: Experiences from the Front. Line of the NHS; Royal College of Physicians: London, UK, December 2016; Available online: https://www.rcplondon.ac.uk/guidelines-policy/being-junior-doctor (accessed on 4 January 2021).
- Koy, V.; Yunibhand, J.; Turale, S. “It is really so exhausting”: Exploring intensive care nurses’ perceptions of 24-hour long shifts. J. Clin. Nurs. 2020, 29, 3506–3515. [Google Scholar] [CrossRef]
- Duffin, C. Lack of breaks leaves nurses burnt out. Nurs. Stand. 2005, 20, 16. [Google Scholar] [CrossRef]
- Witkoski, A.; Dickson, V.V. Hospital Staff Nurses’ Work Hours, Meal Periods, and Rest Breaks: A Review from an Occupational Health Nurse Perspective. AAOHN J. 2010, 58, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.; Kuykendall, L.; Zhang, X. The impact of within-day work breaks on daily recovery processes: An event-based pre-/post-experience sampling study. J. Occup. Organ. Psychol. 2019, 92, 191–211. [Google Scholar] [CrossRef] [Green Version]
- Nejati, A.; Shepley, M.; Rodiek, S. A Review of Design and Policy Interventions to Promote Nurses’ Restorative Breaks in Health Care Workplaces. AAOHN J. 2016, 64, 70–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nejati, A.; Rodiek, S.; Shepley, M. The implications of high-quality staff break areas for nurses’ health, performance, job satisfaction and retention. Nurs. Manag. 2016, 24, 512–523. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, G.A. Checks and balances: The role of managers in work–life balance policies and practices. J. Retail. Consum. Serv. 2005, 12, 179–189. [Google Scholar] [CrossRef]
- Baptiste, N.R. Tightening the link between employee wellbeing at work and performance. Manag. Decis. 2008, 46, 284–309. [Google Scholar] [CrossRef]
- Edmundson, H. Can we change the culture around breaks in the NHS? 28 June. The BMJ Opinion. 2019. Available online: https://0-blogs-bmj-com.brum.beds.ac.uk/bmj/2019/06/28/heidi-edmundson-can-we-change-the-culture-around-breaks-in-the-nhs/ (accessed on 19 February 2021).
- Sunley, K. Breaks must be taken to ensure safety: Workplace pressures make it hard to stop what you’re doing, so here’s how to alert your employer if you have no time for time out. Nurs. Stand. 2020, 35, 28. [Google Scholar] [CrossRef]
- Rosa, D.; Terzoni, S.; Dellafiore, F.; Destrebecq, A. Systematic review of shift work and nurses’ health. Occup. Med. 2019, 69, 237–243. [Google Scholar] [CrossRef]
- Maidstone, R.; Anderson, S.G.; Ray, D.W.; Rutter, M.R.; Durringtonn, H.J.; Blaikley, J.F. Shift Work is Associated with Positive COVID-19 Status in Hospitalised Patients. MedRVix. pre-print. 7 December. Available online: https://www.medrxiv.org/content/10.1101/2020.12.04.20244020v1.full (accessed on 19 February 2021).
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Burton, N.W.; Kolbe-Alexander, T.L. Shift Work and Poor Mental Health: A Meta-Analysis of Longitudinal Studies. Am. J. Public Health 2019, 109, e13–e20. [Google Scholar] [CrossRef]
- Zhao, Y.; Richardson, A.; Poyser, C.; Butterworth, P.; Strazdins, L.; Leach, L.S. Shift work and mental health: A systematic review and meta-analysis. Int. Arch. Occup. Environ. Health 2019, 92, 763–793. [Google Scholar] [CrossRef]
- Cubrich, M. On the frontlines: Protecting low-wage workers during COVID. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S186–S187. [Google Scholar] [CrossRef] [PubMed]
- Office for National Statistics. Provisional Counts of the Number of Deaths and Age-Standardised Mortality Rates Involving the Coronavirus (COVID-19) between 1 March and 30 April 2020 in the UK; Office for National Statistics: London, UK, 2020.
- Cabinet Office Briefing Rooms. Press Conference, April. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/882562/2020–04–30_COVID-19_Press_Conference_Slides.pdf (accessed on 19 February 2021).
- Office for National Statistics. Deaths Registered Weekly in England and Wales, Provisional: Week Ending 17 July 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsregisteredweeklyinenglandandwalesprovisional/weekending17july2020 (accessed on 19 February 2021).
- Office for National Statistics. Deaths Registered Weekly in England and Wales, Provisional: Week Ending 14 August. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsregisteredweeklyinenglandandwalesprovisional/weekending14august2020 (accessed on 19 February 2021).
- Office for National Statistics. Coronavirus and the Social Impacts on Great Britain: 23 October. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandthesocialimpactsongreatbritain/23october2020 (accessed on 26 January 2021).
- Hussain-Gambles, M.; Atkin, K.; Leese, B. South Asian participation in clinical trials: The views of lay people and health professionals. Health Policy 2006, 77, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Redwood, S.; Gill, P.S. Under-representation of minority ethnic groups in research—Call for action. Br. J. Gen. Pract. 2013, 63, 342–343. [Google Scholar] [CrossRef] [Green Version]
- Gill, P.S.; Plumridge, G.; Khunti, K.; Greenfield, S. Under-representation of minority ethnic groups in cardiovascular research: A semi-structured interview study. Fam. Pract. 2012, 30, 233–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooney, L.K.; Bhopal, R.; Halani, L.; Levy, M.L.; Partridge, M.R.; Netuveli, G.; Car, J.; Griffiths, C.; Atkinson, J.; Lindsay, G.; et al. Promoting recruitment of minority ethnic groups into research: Qualitative study exploring the views of South Asian people with asthma. J. Public Health 2011, 33, 604–615. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| ID † | Gender | Type of Participants | Occupation | Clinical or Non-Clinical Role |
|---|---|---|---|---|
| 101 | F | Visitor/Buddy * | Manager | Non-clinical |
| 102 | M | Visitor | Ancillary/Maintenance | Non-clinical |
| 103 | F | Service */Buddy | Manager | Non-clinical |
| 104 | F | Visitor/Buddy * | Manager | Non-clinical |
| 105 | F | Visitor/Buddy * | Administrator | Non-clinical |
| 106 | F | Visitor/Buddy * | AHP | Clinical |
| 107 | M | Visitor/Buddy * | Administrator | Non-clinical |
| 108 | F | Service */Buddy | Administrator | Non-clinical |
| 109 | F | Service/Buddy * | Administrator | Non-clinical |
| 110 | F | Buddy | Nurse | Clinical |
| 115 | M | Visitor | Ancillary/Maintenance | Non-clinical |
| 116 | M | Visitor | Hospital Volunteer | Non-clinical |
| 118 | F | Visitor | Nurse | Clinical |
| 120 | M | Visitor | Hospital volunteer | Non-clinical |
| 123 | F | Visitor | Nurse | Clinical |
| 125 | F | Service/Buddy * | AHP | Clinical |
| 126 | F | Buddy | AHP | Clinical |
| 129 | F | Visitor | Healthcare Assistant | Clinical |
| 131 | F | Visitor | Nurse (redeployed) | Clinical |
| 132 | F | Visitor | Nurse | Clinical |
| 135 | M | Visitor | Hospital volunteer | Clinical |
| 136 | F | Visitor | AHP | Clinical |
| 145 | F | Visitor Service */Buddy | Administrator | Non-clinical |
| 147 | F | Visitor | AHP | Clinical |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blake, H.; Gupta, A.; Javed, M.; Wood, B.; Knowles, S.; Coyne, E.; Cooper, J. COVID-Well Study: Qualitative Evaluation of Supported Wellbeing Centres and Psychological First Aid for Healthcare Workers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3626. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073626
Blake H, Gupta A, Javed M, Wood B, Knowles S, Coyne E, Cooper J. COVID-Well Study: Qualitative Evaluation of Supported Wellbeing Centres and Psychological First Aid for Healthcare Workers during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(7):3626. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073626
Chicago/Turabian StyleBlake, Holly, Alisha Gupta, Mahnoor Javed, Ben Wood, Steph Knowles, Emma Coyne, and Joanne Cooper. 2021. "COVID-Well Study: Qualitative Evaluation of Supported Wellbeing Centres and Psychological First Aid for Healthcare Workers during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 7: 3626. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073626