
Reliability of IMU-Derived Static Balance Parameters in Neurological Diseases

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
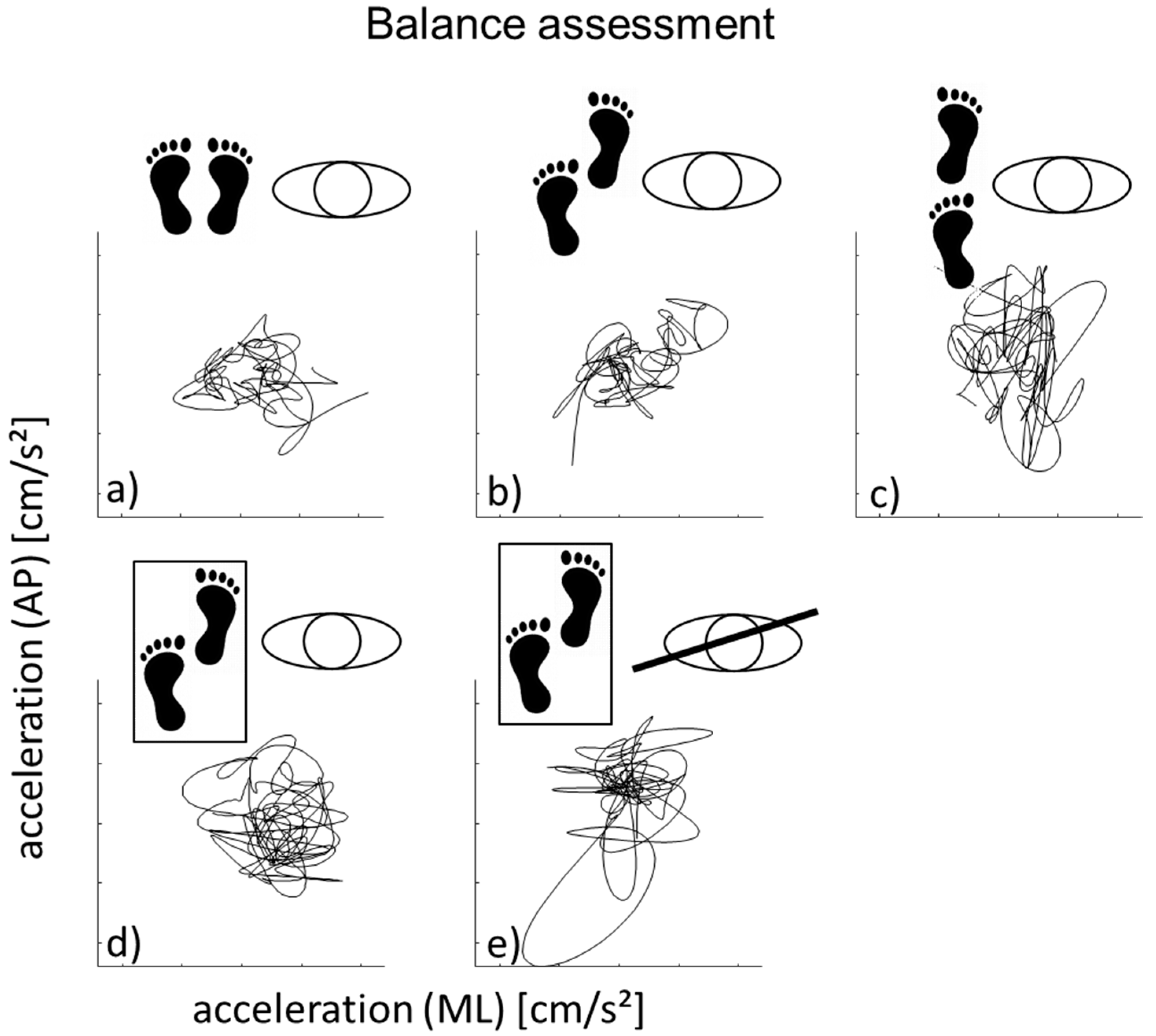
2.1. Quantitative Gait and Balance Assessment
2.2. Sensor Data Processing
2.3. Statistical Analysis
3. Results
3.1. Side-by-Side Stance
3.2. Semi-Tandem Stance on a Hard Surface
3.3. Tandem Stance on a Hard Surface
3.4. Semi Tandem Stance a Soft Surface (Eyes Open)
3.5. Semi Tandem Stance a Soft Surface (Eyes Closed)
3.6. MDC95% Values of All Parameters and Experimental Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Van Der Kooij, H.; Jacobs, R.; Koopman, B.; Grootenboer, H. A multisensory integration model of human stance control. Biol. Cybern. 1999, 80, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Salzman, B. Gait and balance disorders in older adults. Am. Fam. Physician 2010, 82, 61–68. [Google Scholar]
- Winter, D. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Trepel, M. Hirnnervenkerne. In Neuroanatomie—Struktur und Funktion, 3rd ed.; Urban & Fischer: Freiburg, Germany, 2004; pp. 117–119, 224–228. [Google Scholar]
- Gang, N.T. Gleichgewicht und stürze—Ursachen und konsequenzen. Dtsch. Med. Wochenschr. 2005, 130, 958–960. [Google Scholar]
- Montemurro, N.; Perrini, P.; Mangini, V.; Galli, M.; Papini, A. The Y-shaped trabecular bone structure in the odontoid process of the axis: A CT scan study in 54 healthy subjects and biomechanical considerations. J. Neurosurg. Spine 2019, 30, 585–592. [Google Scholar] [CrossRef]
- Houlden, H.; Charlton, P.; Singh, D. Neurology and orthopaedics. J. Neurol. Neurosurg. Psychiatry 2006, 78, 224–232. [Google Scholar] [CrossRef]
- Stella, A.B.; Morelli, M.E.; Giudici, F.; Sartori, A.; Manganotti, P.; Di Prampero, P.E. Comfortable walking speed and energy cost of locomotion in patients with multiple sclerosis. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 120, 551–566. [Google Scholar]
- Morelli, N.; Morelli, H. Dual task training effects on gait and balance outcomes in multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2021, 49, 102794. [Google Scholar] [CrossRef] [PubMed]
- Agurto, C.; Heisig, S.; Abrami, A.; Ho, B.K.; Caggiano, V. Parkinson’s disease medication state and severity assessment based on coordination during walking. PLoS ONE 2021, 16, e0244842. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.; Wei, Q.; Shieh, J.-S.; Fourcade, P.; Isableu, B.; Majed, L. Sample Entropy, Univariate, and Multivariate Multi-Scale Entropy in Comparison with Classical Postural Sway Parameters in Young Healthy Adults. Front. Hum. Neurosci. 2017, 11, 206. [Google Scholar] [CrossRef] [Green Version]
- Pinsault, N.; Vuillerme, N. Test-retest reliability of centre of foot pressure measures to assess postural control during unperturbed stance. Med. Eng. Phys. 2009, 31, 276–286. [Google Scholar] [CrossRef]
- Golriz, S.; Hebert, J.J.; Foreman, K.B.; Walker, B.F. The reliability of a portable clinical force plate used for the assessment of static postural control: Repeated measures reliability study. Chiropr. Man. Ther. 2012, 20, 14. [Google Scholar] [CrossRef] [Green Version]
- Del Din, S.; Elshehabi, M.; Galna, B.; Hobert, M.A.; Warmerdam, E.; Suenkel, U.; Brockmann, K.; Metzger, F.; Hansen, C.; Berg, D.; et al. Gait analysis with wearables predicts conversion to Parkinson disease. Ann. Neurol. 2019, 86, 357–367. [Google Scholar] [CrossRef]
- Pantall, A.; Del Din, S.; Rochester, L. Longitudinal changes over thirty-six months in postural control dynamics and cognitive function in people with Parkinson’s disease. Gait Posture 2018, 62, 468–474. [Google Scholar] [CrossRef] [Green Version]
- Bernhard, F.P.; Sartor, J.; Bettecken, K.; Hobert, M.A.; Arnold, C.; Weber, Y.G.; Poli, S.; Margraf, N.G.; Schlenstedt, C.; Hansen, C.; et al. Wearables for gait and balance assessment in the neurological ward - study design and first results of a prospective cross-sectional feasibility study with 384 inpatients. BMC Neurol. 2018, 18, 1–8. [Google Scholar] [CrossRef]
- Geritz, J.; Maetzold, S.; Steffen, M.; Pilotto, A.; Corrà, M.F.; Moscovich, M.; Rizzetti, M.C.; Borroni, B.; Padovani, A.; Alpes, A.; et al. Motor, cognitive and mobility deficits in 1000 geriatric patients: Protocol of a quantitative observational study before and after routine clinical geriatric treatment—The ComOn-study. BMC Geriatr. 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Mancini, M.; Horak, F.B.; Zampieri, C.; Carlson-Kuhta, P.; Nutt, J.G.; Chiari, L. Trunk accelerometry reveals postural instability in untreated Parkinson’s disease. Park. Relat. Disord. 2011, 17, 557–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancini, M.; Salarian, A.; Carlson-Kuhta, P.; Zampieri, C.; King, L.; Chiari, L.; Horak, F.B. ISway: A sensitive, valid and reliable measure of postural control. J. Neuroeng. Rehabil. 2012, 9, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasreddine, Z. Montreal Cognitive Assessment (MoCA) Administration, Administration and Scoring Instructions. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Spain, R.; George, R.S.; Salarian, A.; Mancini, M.; Wagner, J.; Horak, F.; Bourdette, D. Body-worn motion sensors detect balance and gait deficits in people with multiple sclerosis who have normal walking speed. Gait Posture 2012, 35, 573–578. [Google Scholar] [CrossRef] [Green Version]
- Lexell, J.E.; Downham, D.Y. How to Assess the Reliability of Measurements in Rehabilitation. Am. J. Phys. Med. Rehabil. 2005, 84, 719–723. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Schwenk, M.; Gogulla, S.; Englert, S.; Czempik, A.; Hauer, K. Test-retest reliability and minimal detectable change of repeated sit-to-stand analysis using one body fixed sensor in geriatric patients. Physiol. Meas. 2012, 33, 1931–1946. [Google Scholar] [CrossRef] [PubMed]
- Hollman, J.H.; Beckman, B.A.; Brandt, R.A.; Merriwether, E.N.; Williams, R.T.; Nordrum, J.T. Minimum Detectable Change in Gait Velocity during Acute Rehabilitation following Hip Fracture. J. Geriatr. Phys. Ther. 2008, 31, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.; Schepens, S. Measurement error and minimum detectable change in 4-meter gait speed in older adults. Aging Clin. Exp. Res. 2011, 23, 406–412. [Google Scholar] [CrossRef]
- Haley, S.M.; A Fragala-Pinkham, M. Interpreting Change Scores of Tests and Measures Used in Physical Therapy. Phys. Ther. 2006, 86, 735–743. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, A.; Casby, A.; Wasielewski, M. Minimum detectable change for single-leg-stance-time in older adults. Gait Posture 2011, 33, 737–739. [Google Scholar] [CrossRef]
- Hiengkaew, V.; Jitaree, K.; Chaiyawat, P. Minimal Detectable Changes of the Berg Balance Scale, Fugl-Meyer Assessment Scale, Timed “Up & Go” Test, Gait Speeds, and 2-Minute Walk Test in Individuals With Chronic Stroke With Different Degrees of Ankle Plantarflexor Tone. Arch. Phys. Med. Rehabil. 2012, 93, 1201–1208. [Google Scholar] [PubMed]
- Steffen, T.; Seney, M. Test-Retest Reliability and Minimal Detectable Change on Balance and Ambulation Tests, the 36-Item Short-Form Health Survey, and the Unified Parkinson Disease Rating Scale in People With Parkinsonism. Phys. Ther. 2008, 88, 733–746. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Horn, D.; Marclay, S.; Crews, R.T.; Wu, S.; Wrobel, J.S. Assessing Postural Control and Postural Control Strategy in Diabetes Patients Using Innovative and Wearable Technology. J. Diabetes Sci. Technol. 2010, 4, 780–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nashner, L.M.; Mccollum, G. The organization of human postural movements: A formal basis and experimental synthesis. Behav. Brain Sci. 1985, 8, 135–150. [Google Scholar] [CrossRef]
- PGatev, P.; Tankov, N.; Gantchev, G.; Krizkova, M. Postural adjustments upon arm movement during sinusoidal induced body oscillations. Acta Physiol. Pharmacol. Bulg. 1991, 17, 3–6. [Google Scholar]
- Kuo, A. An optimal control model for analyzing human postural balance. IEEE Trans. Biomed. Eng. 1995, 42, 87–101. [Google Scholar] [CrossRef]
- Runge, C.; Shupert, C.; Horak, F.; Zajac, F. Ankle and hip postural strategies defined by joint torques. Gait Posture 1999, 10, 161–170. [Google Scholar] [CrossRef]
- Horak, F.B.; Nashner, L.M. Central programming of postural movements: Adaptation to altered support-surface configurations. J. Neurophysiol. 1986, 55, 1369–1381. [Google Scholar] [CrossRef]
- Beyea, J.; McGibbon, C.A.; Sexton, A.; Noble, J.; O’Connell, C. Convergent validity of a wearable sensor system for measuring sub-task performance during the timed up-and-go test. Sensors 2017, 17, 934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Washabaugh, E.P.; Kalyanaraman, T.; Adamczyk, P.G.; Claflin, E.S.; Krishnan, C. Validity and repeatability of inertial measurement units for measuring gait parameters. Gait Posture 2017, 55, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donath, L.; Faude, O.; Lichtenstein, E.; Pagenstert, G.; Nüesch, C.; Mündermann, A.; Muendermann, A. Mobile inertial sensor based gait analysis: Validity and reliability of spatiotemporal gait characteristics in healthy seniors. Gait Posture 2016, 49, 371–374. [Google Scholar] [CrossRef]
- Pham, M.H.; Warmerdam, E.; Elshehabi, M.; Schlenstedt, C.; Bergeest, L.-M.; Heller, M.; Haertner, L.; Ferreira, J.J.; Berg, D.; Schmidt, G.; et al. Validation of a Lower Back “Wearable”-Based Sit-to-Stand and Stand-to-Sit Algorithm for Patients With Parkinson’s Disease and Older Adults in a Home-Like Environment. Front. Neurol. 2018, 9, 652. [Google Scholar] [CrossRef] [Green Version]
- Horak, F.B.; Mancini, M. Objective biomarkers of balance and gait for Parkinson’s disease using body-worn sensors. Mov. Disord. 2013, 28, 1544–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinn, N.P. Classification of fluctuations in patients with Parkinson’s disease. Neurology 1998, 51, S25–S29. [Google Scholar] [CrossRef]
- Mehta, S.; Bastero-Caballero, R.F.; Sun, Y.; Zhu, R.; Murphy, D.K.; Hardas, B.; Koch, G. Performance of intraclass correlation coefficient (ICC) as a reliability index under various distributions in scale reliability studies. Stat. Med. 2018, 37, 2734–2752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Parameter | Meant1 | SDt1 | Meant2 | SDt2 | pt1-T2 | ICC | MDC95% |
|---|---|---|---|---|---|---|---|
| SURFACE (CM2/S4) | 20.9 | 9.8 | 20.1 | 9.1 | 0.657 | 0.26 | 109 |
| VELAP (CM/S) | 2.62 | 1.51 | 2.34 | 1.62 | 0.336 | 0.35 | 141 |
| VELML (CM/S) | 1.02 | 0.45 | 0.88 | 0.43 | 0.160 | 0.11 | 123 |
| ACCAP (CM/S2) | 1.24 | 0.43 | 1.19 | 0.37 | 0.469 | 0.36 | 73 |
| ACCML (CM/S2) | 0.87 | 0.16 | 0.84 | 0.14 | 0.413 | 0.21 | 43 |
| JERKAP (CM/S3) | 1072 | 832 | 1110 | 765 | 0.827 | 0.06 | 195 |
| JERKML (CM/S3) | 944 | 765 | 987 | 534 | 0.777 | 0.02 | 186 |
| FREQUENCY (HZ) | 1.57 | 0.34 | 1.55 | 0.30 | 0.735 | 0.29 | 48 |
| Parameter | Meant1 | SDt1 | Meant2 | SDt2 | pt1-T2 | ICC | MDC95% |
|---|---|---|---|---|---|---|---|
| SURFACE (CM2/S4) | 23.5 | 10.8 | 22.4 | 9.5 | 0.538 | 0.5 | 87 |
| VELAP (CM/S) | 2.29 | 1.30 | 2.27 | 1.42 | 0.950 | 0.28 | 140 |
| VELML (CM/S) | 1.26 | 0.64 | 1.27 | 0.57 | 0.946 | 0.27 | 113 |
| ACCAP (CM/S) | 1.19 | 0.35 | 1.19 | 0.33 | 0.937 | 0.52 | 54 |
| ACCML (CM/S2) | 1.09 | 0.32 | 1.02 | 0.19 | 0.122 | 0.45 | 51 |
| JERKAP (CM/S3) | 1067 | 586 | 974 | 641 | 0.507 | 0.06 | 162 |
| JERKML (CM/S3) | 1057 | 833 | 976 | 711 | 0.660 | 0.03 | 213 |
| FREQUENCY (HZ) | 1.70 | 0.32 | 1.62 | 0.32 | 0.151 | 0.34 | 43 |
| Parameter | Meant1 | SDt1 | Meant2 | SDt2 | pt1-T2 | ICC | MDC95% |
|---|---|---|---|---|---|---|---|
| SURFACE (CM2/S4) | 43.2 | 25.6 | 46.4 | 34.5 | 0.736 | 0.25 | 160 |
| VELAP (CM/S) | 3.62 | 2.00 | 3.22 | 2.35 | 0.500 | 0.27 | 150 |
| VELML (CM/S) | 1.97 | 0.99 | 1.71 | 0.96 | 0.377 | 0.16 | 134 |
| ACCAP (CM/S2) | 1.48 | 0.60 | 1.69 | 0.88 | 0.238 | 0.48 | 95 |
| ACCML (CM/S2) | 1.83 | 0.71 | 1.65 | 0.78 | 0.397 | 0.26 | 101 |
| JERKAP (CM/S3) | 1632 | 1211 | 964 | 889 | 0.044 | 0.13 | 220 |
| JERKML (CM/S3) | 1265 | 785 | 1230 | 953 | 0.901 | 0.01 | 190 |
| FREQUENCY (HZ) | 1.72 | 0.46 | 1.69 | 0.42 | 0.812 | 0.35 | 57 |
| Parameter | Meant1 | SDt1 | Meant2 | SDt2 | pt1-T2 | ICC | MDC95% |
|---|---|---|---|---|---|---|---|
| SURFACE (CM2/S4) | 49.3 | 35.3 | 49.2 | 35.5 | 0.992 | 0.66 | 115 |
| VELAP (CM/S) | 8.44 | 6.06 | 9.05 | 7.71 | 0.703 | 0.53 | 149 |
| VELML (CM/S) | 3.23 | 1.63 | 2.88 | 1.41 | 0.296 | 0.65 | 81 |
| ACCAP (CM/S2) | 1.76 | 0.79 | 1.82 | 0.72 | 0.704 | 0.55 | 77 |
| ACCML (CM/S2) | 1.41 | 0.51 | 1.36 | 0.56 | 0.564 | 0.75 | 53 |
| JERKAP (CM/S3) | 1339 | 1035 | 1363 | 1009 | 0.941 | 0.03 | 204 |
| JERKML (CM/S3) | 1207 | 1018 | 1119 | 739 | 0.753 | 0.09 | 200 |
| FREQUENCY (HZ) | 1.57 | 0.48 | 1.58 | 0.41 | 0.925 | 0.48 | 55 |
| Parameter | Meant1 | SDt1 | Meant2 | SDt2 | pt1-T2 | ICC | MDC95% |
|---|---|---|---|---|---|---|---|
| SURFACE (CM2/S4) | 105.3 | 74.9 | 71.9 | 43.0 | 0.125 | 0.5 | 137 |
| VELAP (CM/S) | 9.67 | 7.06 | 8.56 | 6.75 | 0.719 | 0.08 | 197 |
| VELML (CM/S) | 6.14 | 3.85 | 4.75 | 2.19 | 0.139 | 0.59 | 103 |
| ACCAP (CM/S2) | 2.55 | 1.00 | 2.01 | 0.62 | 0.025 | 0.6 | 66 |
| ACCML (CM/S2) | 2.14 | 0.71 | 1.93 | 0.76 | 0.302 | 0.69 | 55 |
| JERKAP (CM/S3) | 1067 | 897 | 1055 | 942 | 0.98 | −0.41 | 278 |
| JERKML (CM/S3) | 1171 | 573 | 1025 | 834 | 0.678 | −0.13 | 188 |
| FREQUENCY (HZ) | 1.58 | 0.30 | 1.69 | 0.39 | 0.364 | 0.54 | 39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, C.; Beckbauer, M.; Romijnders, R.; Warmerdam, E.; Welzel, J.; Geritz, J.; Emmert, K.; Maetzler, W. Reliability of IMU-Derived Static Balance Parameters in Neurological Diseases. Int. J. Environ. Res. Public Health 2021, 18, 3644. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073644
Hansen C, Beckbauer M, Romijnders R, Warmerdam E, Welzel J, Geritz J, Emmert K, Maetzler W. Reliability of IMU-Derived Static Balance Parameters in Neurological Diseases. International Journal of Environmental Research and Public Health. 2021; 18(7):3644. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073644
Chicago/Turabian StyleHansen, Clint, Maximilian Beckbauer, Robbin Romijnders, Elke Warmerdam, Julius Welzel, Johanna Geritz, Kirsten Emmert, and Walter Maetzler. 2021. "Reliability of IMU-Derived Static Balance Parameters in Neurological Diseases" International Journal of Environmental Research and Public Health 18, no. 7: 3644. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073644