
A Pilot Evaluation of mHealth App Accessibility for Three Top-Rated Weight Management Apps by People with Disabilities



Abstract
:1. Introduction
2. Materials and Methods
2.1. mHealth App Selection Process
- High consumer review ratings evenly reported on both the iOS App Store and in Google Play
- High download/installation user-base on both iOS and Android OS devices
- Commercially available on both iOS and Android OS devices
- Free with in-app purchases for both iOS and Android device users
2.2. App Accessibility Testing Protocol
- Explore: initial familiarization to app screens, functions, and navigational elements
- Core Tasks: logging meals, physical activity, and diet or fitness goals
2.2.1. System Usability Scale (SUS)
- I think that I would like to use this system frequently.
- I found the system unnecessarily complex.
- I thought the system was easy to use.
- I think I would need the support of a technical person to be able to use this system.
- I found the various functions in this system were well integrated.
- I thought there was too much inconsistency in this system.
- I would imagine that most people would learn to use this system very quickly.
- I found the system very cumbersome to use.
- I felt very confident using the system.
- I needed to learn a lot of things before I could get going with this system.
2.2.2. Tierney’s 7-Minute Accessibility Assessment and App Rating System
- Please rate your experience completing [name of task or task section], based on ease of use, on a scale of 1 to 5 stars using the following rating key:
- ○
- 1 Star: Very Difficult (lowest tolerance for issues)—Unable to complete most tasks independently; Prohibitive confusion or frustration
- ○
- 2 Stars: Difficult—Unable to complete a few tasks independently; Significant confusion or frustration
- ○
- 3 Stars: Moderate Ease/Difficulty—Able to complete all tasks independently; Moderate confusion or frustration
- ○
- 4 Stars: Easy—Able to complete all tasks independently; Infrequent confusion or frustration
- ○
- 5 Stars: Very Easy (highest tolerance for issues)—Able to complete all tasks independently; Minimal to no confusion or frustration
- While completing [name of task or task section], was there anything of note, that made the process difficult? If yes, please describe the source(s) of difficulty.
- While completing [name of task or task section], was there anything of note, that you would want to change about the process or app interface to make accomplishing the tasks easier? If yes, please describe what you would like to see changed.
2.3. Participant Recruitment and Testing Procedure
3. Results
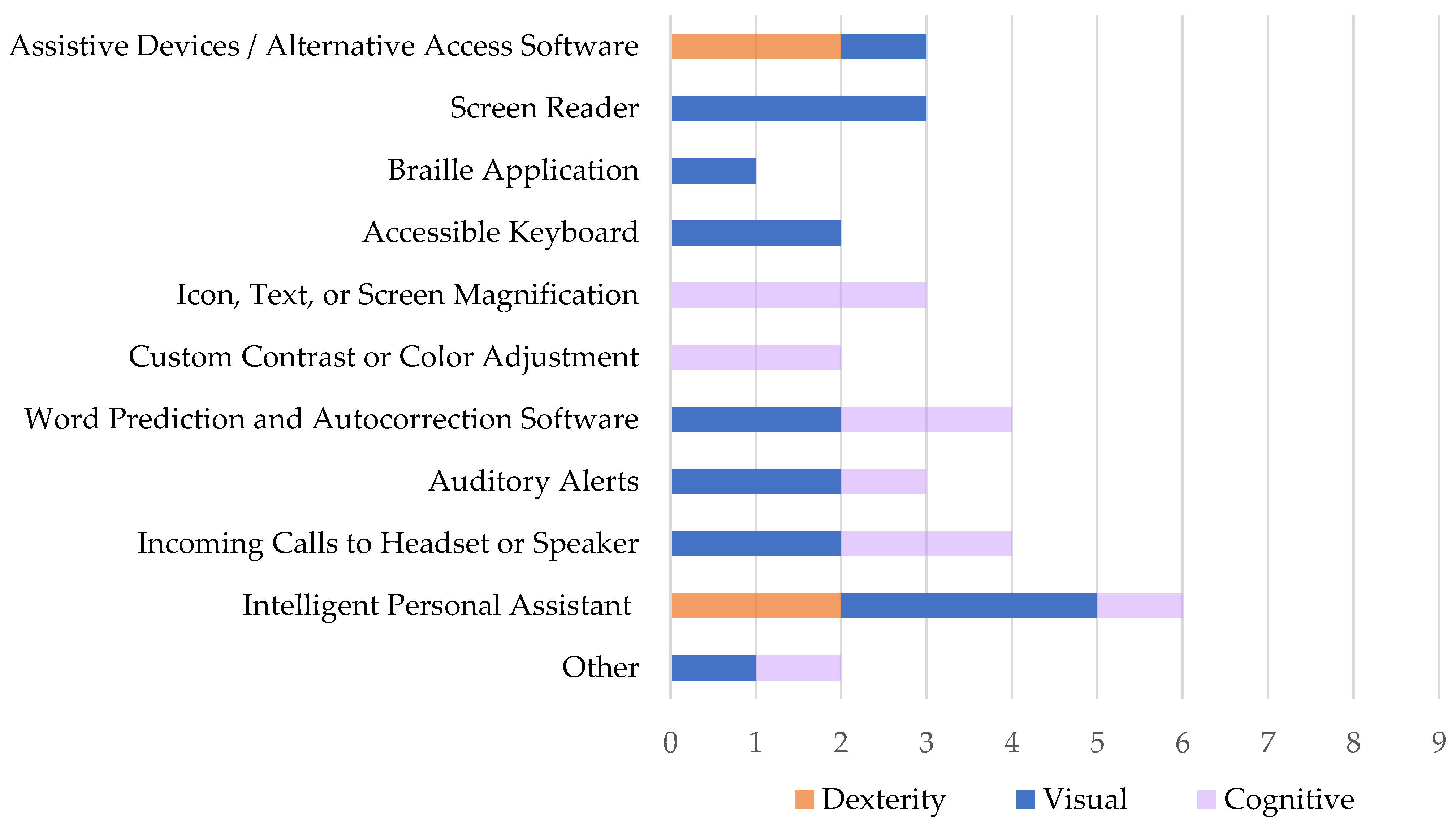
3.1. Participant Characteristics and Assistive Technology Usage
3.2. Quantitative Results
3.2.1. Quantitative SUS Score Results
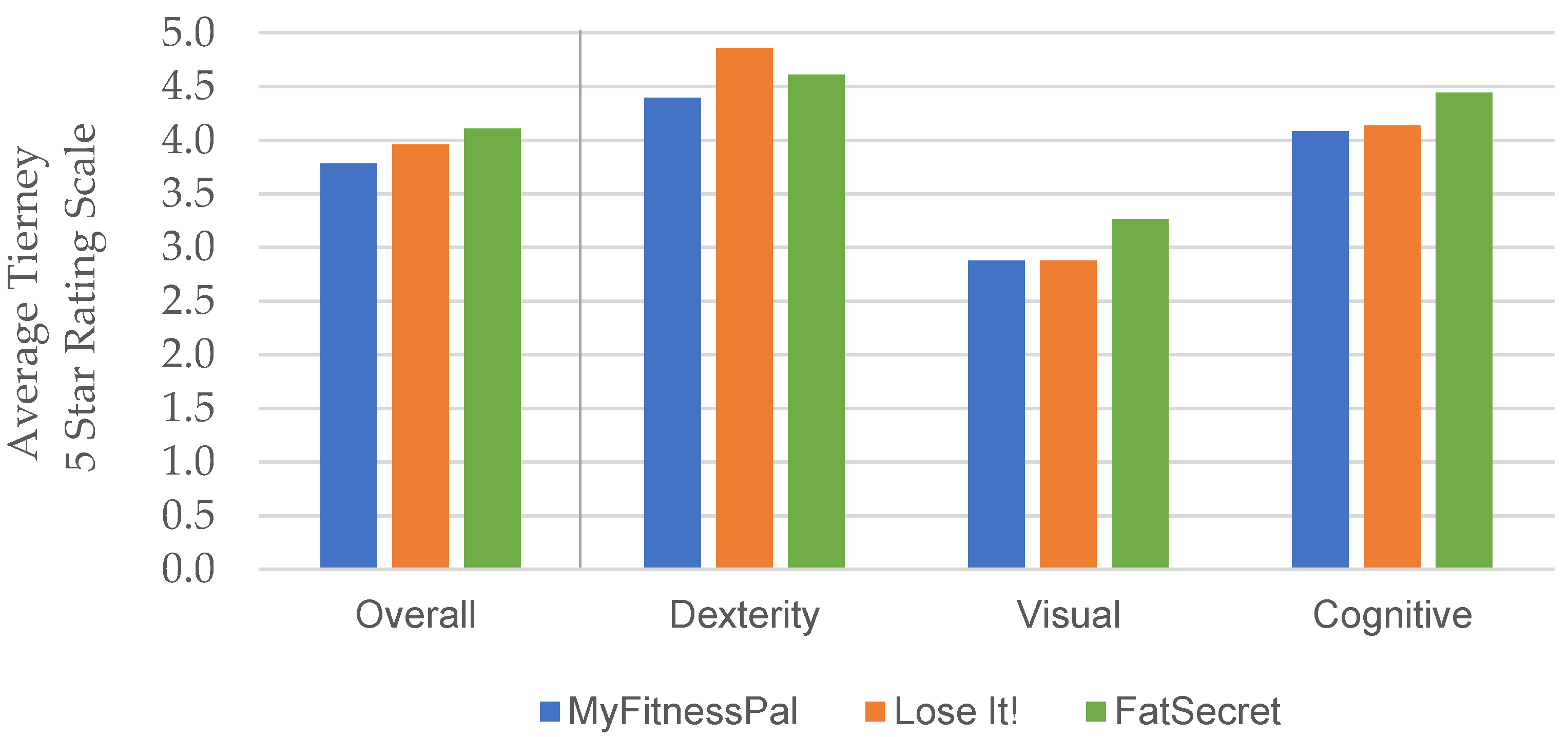
3.2.2. Quantitative Tierney Rating Results
- 1 Star: Very Low—Severe accessibility issues and overall inattention to accessibility will prevent some users from using the app.
- 2 Stars: Low—Accessibility issues will prevent some users from completing core tasks in the app, due to poor overall accessibility quality.
- 3 Stars: Moderate—Accessibility issues may prevent some users from completing non-core tasks. Users may experience significant annoyances and confusion, due to lack of attention to detail across the application.
- 4 Stars: High—Some minor impact issues may exist, but no accessibility issues prevent user from completing core tasks, despite annoyances.
- 5 Stars: Very High—Low incidence of issues. Some minor impact issues may exist, but no accessibility issues prevent user from completing core tasks.
3.3. Qualitative Results
4. Discussion
4.1. Opportunities for Improved Mobile App Accessibility:
4.2. Limitations
4.3. Future Work
- To provide app users with disabilities clear ratings and information on accessibility issues they may encounter while using each evaluated app, based on their disability or the assistive technology they may use to access their mobile devices. This information is meant to help app users make informed decisions when selecting an mHealth app to meet their needs.
- To invite and enable app users with disabilities to provide their own accessibility ratings and “consumer reviews” for selected mHealth apps.
- To make recommendations to developers on steps they can take to improve their app’s accessibility and usability for people with disabilities.
- Apps that track and support individualized goals and health habits;
- Apps that track multiple areas of health in one app;
- Clinical portal apps that enable personal health information management, appointment scheduling, access to lab results and vital sign tracking, and correspondence with healthcare providers (e.g., MyChart);
- Apps that support stress, PTSD, and mental health management;
- Apps that track and support healthy sleep patterns;
- Apps that support diabetes management via blood pressure, blood sugar, and heart rate monitoring;
- Sensor-enhanced activity monitoring apps that support remote physical rehabilitation;
- Exercise apps for wheelchair users.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kinne, S.; Patrick, D.L.; Lochner, D.D. Prevalence of secondary conditions among people with disabilities. Am. J. Public Health 2004, 94, 443–445. [Google Scholar] [CrossRef] [PubMed]
- Krahn, G.L.; Reyes, M.; Fox, M. Chronic conditions and disability: Toward a conceptual model for national policy and practice considerations. Disabil. Health J. 2014, 7, 13–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iezzoni, L.I. Eliminating health and health care disparities among the growing population of people with disabilities. Health Aff. 2011, 30, 1947–1954. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Morris, J.; Deruyter, F. Mobile healthcare and people with disabilities: Current state and future needs. Int. J. Environ. Res. Public Health 2018, 15, 515. [Google Scholar] [CrossRef] [Green Version]
- Ballantyne, M.; Archit, J.; Anna, J.; Hawker, J.S.; El-Glaly, Y.N. Study of Accessibility Guidelines of Mobile Applications. In Proceedings of the 17th International Conference on Mobile and Ubiquitous Multimedia (MUM 2018), Cairo, Egypt, 25–28 November 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 305–315. [Google Scholar]
- Siebra, C.; Anjos, M.; Florentin, F.; Gouveia, T.; Filho, A.; Correia, W.; Penha, M.; Silva, F.; Santos, A. Accessibility Devices for Mobile Interfaces Extensions: A Survey. In Proceedings of the 17th International Conference on Human-Computer Interaction with Mobile Devices and Services Adjunct (MobileHCI ’15), Copenhagen, Denmark, 24 August 2015; Association for Computing Machinery: New York, NY, USA, 2015; pp. 644–651. [Google Scholar]
- Damaceno, R.J.P.; Braga, J.C.; Mena-Chalco, J.P. Mobile device accessibility for the visually impaired: Problems mapping and recommendations. Univ. Access Inf. Soc. 2018, 17, 421–435. [Google Scholar] [CrossRef]
- Alajarmeh, N. The extent of mobile accessibility coverage in WCAG 2.1: Sufficiency of success criteria and appropriateness of relevant conformance levels pertaining to accessibility problems encountered by users who are visually impaired. Univ. Access Inf. Soc 2021, 1–26. [Google Scholar] [CrossRef]
- Dixon-Ibarra, A.; Horner-Johnson, W. Disability status as an antecedent to chronic conditions: National health interview survey, 2006–2012. Prev. Chronic. Dis. 2014, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Morris, J.; Jones, M.; Sweatman, M. Wireless technology use by people with disabilities: A national survey. J. Technol. Pers. Disabil. 2016, 101–113. [Google Scholar]
- Dombrowski, S.U.; Sniehotta, F.F.; Avenell, A.; Johnston, M.; MacLennan, G.; Araújo-Soares, V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: A systematic review. Health Psychol. Rev. 2012, 6, 7–32. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Whitehead, M.; Sheats, J.Q.; Mastromonico, J.; Hardy, D.; Smith, S.A. Smartphone Applications for Promoting Healthy Diet and Nutrition: A Literature Review. Jacobs J. Food Nutr. 2015, 2, 1–14. [Google Scholar]
- Coughlin, S.S.; Whitehead, M.; Sheats, J.Q.; Mastromonico, J.; Smith, S. A Review of Smartphone Applications for Promoting Physical Activity. Jacobs J. Community Med. 2016, 2, 1–22. [Google Scholar]
- Jake-Schoffman, D.E.; Turner-McGrievy, G.M.; Jones, S.J.; Wilcox, S. Mobile apps for pediatric obesity prevention and treatment, healthy eating, and physical activity promotion: Just fun and games? TBM 2013, 3, 320–325. [Google Scholar]
- Barlow, S.E. The Expert Committee, Expert committee recommendations regarding the preventions, assessment, an treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120, S164–S192. [Google Scholar] [CrossRef] [Green Version]
- Bondaronek, P.; Alkhaldi, G.; Slee, A.; Hamilton, F.L.; Murray, E. Quality of Publicly Available Physical Activity Apps: Review and Content Analysis. JMIR Mhealth Uhealth. 2018, 6, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardus, M.; van Beurden, S.; Smith, J.; Abraham, C. A review and content analysis of engagement, function, aesthetics, information quality, and change techniques in the most popular commercial apps for weight management. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- My Fitness Pal. Available online: https://www.myfitnesspal.com (accessed on 2 September 2020).
- Lose It! Available online: https://www.loseit.com (accessed on 20 December 2020).
- Fat Secret Calorie Counter App. Available online: http://www.FatSecret.com (accessed on 2 September 2020).
- Noom. Available online: https://www.noom.com (accessed on 23 March 2021).
- WW (Weight Watchers). Available online: https://www.weightwatchers.com (accessed on 23 March 2021).
- MyPlate. Available online: https://www.livestrong.com/myplate (accessed on 23 March 2021).
- VA MOVE! Coach. Available online: https://www.move.va.gov/MOVE/movecoach.asp (accessed on 23 March 2021).
- MyNetDiary. Available online: https://www.mynetdiary.com (accessed on 23 March 2021).
- My Diet Diary. Available online: https://www.mydietdiary.co.uk (accessed on 23 March 2021).
- SparkPeople. Available online: https://www.sparkpeople.com (accessed on 23 March 2021).
- Wharton, C.M.; Johnston, C.S.; Cunningham, B.K.; Sterner, D. Dietary self-monitoring, but not dietary quality, improves with use of smartphone app technology in an 8-week weight loss trial. J. Nutr. Educ. Behav. 2014, 46, 440–444. [Google Scholar] [CrossRef]
- Laing, B.Y.; Mangione, C.M.; Tseng, C.H.; Leng, M.; Vaisberg, E.; Mahida, M.; Bholat, M.; Glazier, E.; Morisky, D.; Bell, D. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: A randomized, controlled trial. Ann. Intern. Med. 2014, 161, S5–S12. [Google Scholar] [CrossRef]
- Serrano, K.J.; Yu, M.; Coa, K.I.; Collins, L.M.; Atienza, A.A. Mining health app data to find more and less successful weight loss subgroups. J. Med. Internet Res. 2016, 18, 1–23. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.M.; Beets, M.W.; Moore, J.B.; Kaczynski, A.T.; Barr-Anderson, D.J.; Tate, D.F. Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mHealth weight loss program. J. Am. Med. Inform. Assoc. 2013, 20, 513–518. [Google Scholar] [CrossRef]
- Jake-Schoffman, D.E.; Silfee, V.J.; Waring, M.E.; Boudreaux, E.; Sadasivam, R.; Mullen, S.P.; Carey, J.L.; Hayes, R.B.; Ding, E.Y.; Bennett, G.G.; et al. Methods for evaluating the content, usability, and efficacy of commercial mobile health apps. JMIR Mhealth Uhealth 2017, 5, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tierney, A. The 7-Minute Accessibility Assessment and App Rating System. In Proceedings of the 32nd Annual CSUN Assistive Technology Conference, San Diego, CA, USA, 2 March 2017; Available online: https://www.slideshare.net/aidantierney/the-7-minute-accessibility-assessment-and-app-rating-system (accessed on 19 September 2019).
- Brooke, J. SUS: A retrospective. J. Usability Stud. 2013, 8, 29–40. [Google Scholar]
- System Usability Scale (SUS): A Quick-and-Dirty Usability Scale. Available online: https://hell.meiert.org/core/pdf/sus.pdf (accessed on 2 September 2020).
- Finstad, K. The system usability scale and non-native English speakers. J. Usability Stud. 2006, 1, 185–188. [Google Scholar]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An empirical evaluation of the system usability scale. Int. J. Hum. Comput Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Lewis, J.R. Psychometric evaluation of the PSSUQ using data from five years of usability studies. Int. J. Hum. Comput. Interact. 2011, 14, 463–488. [Google Scholar]
- Frankfort-Nachmias, C.; Leon-Guerrero, A. Social Statistics for a Diverse Society, 8th ed.; Sage Publication: Thousand Oaks, CA, USA, 2018; pp. 303–324. [Google Scholar]
- Apple. Accessibility-Mobility. Available online: https://www.apple.com/accessibility/mobility/ (accessed on 6 January 2021).
- GlassOuse Assistive Device. Available online: https://glassouse.com/ (accessed on 6 January 2021).
- Harrison, R.; Flood, D.; Duce, D. Usability of mobile applications: Literature review and rationale for a new usability model. J. Interact. Sci. 2013, 1, 1–16. [Google Scholar] [CrossRef] [Green Version]
- The World Wide Web Consortium (W3C). Web Content Accessibility Guidelines (WCAG) 2.0. Available online: https://www.w3.org/TR/WCAG20/ (accessed on 26 March 2021).
- The World Wide Web Consortium (W3C). Mobile Accessibility Examples from UAAG 2.0 Reference. Available online: https://www.w3.org/TR/2015/NOTE-UAAG20-Reference-20151215/mobile.html (accessed on 26 March 2021).
- The World Wide Web Consortium (W3C). Mobile Accessibility at W3C. Available online: https://www.w3.org/WAI/standards-guidelines/mobile/ (accessed on 26 March 2021).
- Google, LLC. Principles for improving app accessibility. Available online: https://developer.android.com/guide/topics/ui/accessibility/principles (accessed on 26 March 2021).
- Google, LLC. Make apps more accessible. Available online: https://developer.android.com/guide/topics/ui/accessibility/apps (accessed on 26 March 2021).
- Google, LLC. Accessibility Testing Checklist. Available online: https://stuff.mit.edu/afs/sipb/project/android/docs/tools/testing/testing_accessibility.html (accessed on 26 March 2021).
- Apple, Inc. Human Interface Guidelines. Available online: https://developer.apple.com/design/human-interface-guidelines/accessibility/overview/best-practices/ (accessed on 26 March 2021).
- Apple, Inc. Testing for Accessibility on OS X. Available online: https://developer.apple.com/library/archive/documentation/Accessibility/Conceptual/AccessibilityMacOSX/OSXAXTestingApps.html (accessed on 26 March 2021).
- AppleVis. Information for Developers on how to Build Accessible iOS, iPadOS, Mac, Apple Watch, and Apple TV Apps. Available online: https://www.applevis.com/information-developers-how-build-accessible-ios-ipados-mac-apple-watch-and-apple-tv-apps (accessed on 26 March 2021).
- Apple. Accessibility. Available online: https://www.apple.com/accessibility/ (accessed on 26 March 2021).
- Andorid. Accessibility. Available online: https://www.android.com/accessibility/ (accessed on 26 March 2021).
- Yan, S.; Ramachandran, P. The Current Status of Accessibility in Mobile Apps. ACM Trans. Access. Comput. 2019, 12, 1–31. [Google Scholar] [CrossRef]
- Eler, M.M.; Rojas, J.M.; Ge, Y.; Fraser, G. Automated Accessibility Testing of Mobile Apps. In Proceedings of the IEEE 11th International Conference on Software Testing, Verification and Validation (ICST), Västerås, Sweden, 9–13 April 2018; pp. 116–126. [Google Scholar]
- Aguado-Delgado, J.; Castillo-Martinez, A.; Gutierrez-Martinez, J.M.; Hilera, J.R.; de-Marcos, L. Accessibility and usability evaluation techniques for mobile applications: A case study on industrial helping application. Initiatives 2017, 5, 6. [Google Scholar]
- DeRuyter, F.; Jones, M.; Morris, J. Mobile Health and Mobile Rehabilitation for People with Disabilities: Current State, Challenges and Opportunities. In Computers Helping People with Special Needs; Miesenberger, K., Manduchi, R., Covarrubias Rodriguez, M., Peňáz, P., Eds.; Lecture Notes in Computer Science; Springer International Publishing: New York, NY, USA, 2020; Volume 12377, pp. 219–223. [Google Scholar]
- World Health Organization. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Lippincott, B.; Thompson, N.; Morris, J.; Jones, M.; DeRuyter, F. Survey of User Needs: Mobile Apps for mHealth and People with Disabilities. In Computers Helping People with Special Needs; Miesenberger, K., Manduchi, R., Covarrubias Rodriguez, M., Peňáz, P., Eds.; Lecture Notes in Computer Science; Springer International Publishing: New York, NY, USA, 2020; Volume 12377, pp. 266–273. [Google Scholar]
- Biggest App Stores in the World 2020. Available online: www.statista.com/statistics/276623/number-of-apps-available-in-leading-app-stores/ (accessed on 24 November 2020).



{kind=link}
{kind=link}
| Demographic Variable | Participant Sample Characteristics |
|---|---|
| Impairment Category | 3 Dexterity, 3 Visual, 3 Cognitive |
| Age (years) | Mean: 41; range: 25–64 |
| Time with Impairments (years) | Mean: 16; range: 1–37 |
| Gender | 4 Female, 5 Male |
| Race/Ethnicity | 1 Black, 8 White; 2 Hispanic/Latino |
| Level of Education (years) | Mean = 16; range = 14–18 |
| Annual Income | Mean: USD 22 K; range: <USD 15 K to USD 100–150 K |
| Mobile Platform | 5 iOS, 4 Android |
| mHealth App | Task Completion Section | Dexterity (N = 3) 1 | Visual (N = 3) | Cognitive (N = 3) | ANOVA Results | ||
|---|---|---|---|---|---|---|---|
| M | M | M | F | P | Sig. | ||
| MyFitnessPal (N = 8, df = 7) | Explore | 77.5 | 44.2 | 70.0 | 0.853 | 0.480 | ns |
| Core Tasks | 70.0 | 61.7 | 78.3 | 0.812 | 0.495 | ns | |
| Lose It! (N = 9, df = 8) | Explore | 83.3 | 31.7 | 81.7 | 14.286 | 0.005 | * |
| Core Tasks | 89.2 | 47.5 | 82.5 | 3.601 | 0.094 | ns | |
| FatSecret (N = 9, df = 8) | Explore | 94.2 | 41.7 | 89.2 | 17.028 | 0.003 | * |
| Core Tasks | 90.8 | 57.5 | 77.5 | 2.593 | 0.154 | ns | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radcliffe, E.; Lippincott, B.; Anderson, R.; Jones, M. A Pilot Evaluation of mHealth App Accessibility for Three Top-Rated Weight Management Apps by People with Disabilities. Int. J. Environ. Res. Public Health 2021, 18, 3669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073669
Radcliffe E, Lippincott B, Anderson R, Jones M. A Pilot Evaluation of mHealth App Accessibility for Three Top-Rated Weight Management Apps by People with Disabilities. International Journal of Environmental Research and Public Health. 2021; 18(7):3669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073669
Chicago/Turabian StyleRadcliffe, Erin, Ben Lippincott, Raeda Anderson, and Mike Jones. 2021. "A Pilot Evaluation of mHealth App Accessibility for Three Top-Rated Weight Management Apps by People with Disabilities" International Journal of Environmental Research and Public Health 18, no. 7: 3669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073669