
Changes to Physical Activity during a Global Pandemic: A Mixed Methods Analysis among a Diverse Population-Based Sample of Emerging Adults in the U.S.

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Survey Measures
2.3. Analysis
3. Results
3.1. Quantiative Changes in Hours of PA from 2018 to 2020 (during COVID-19)
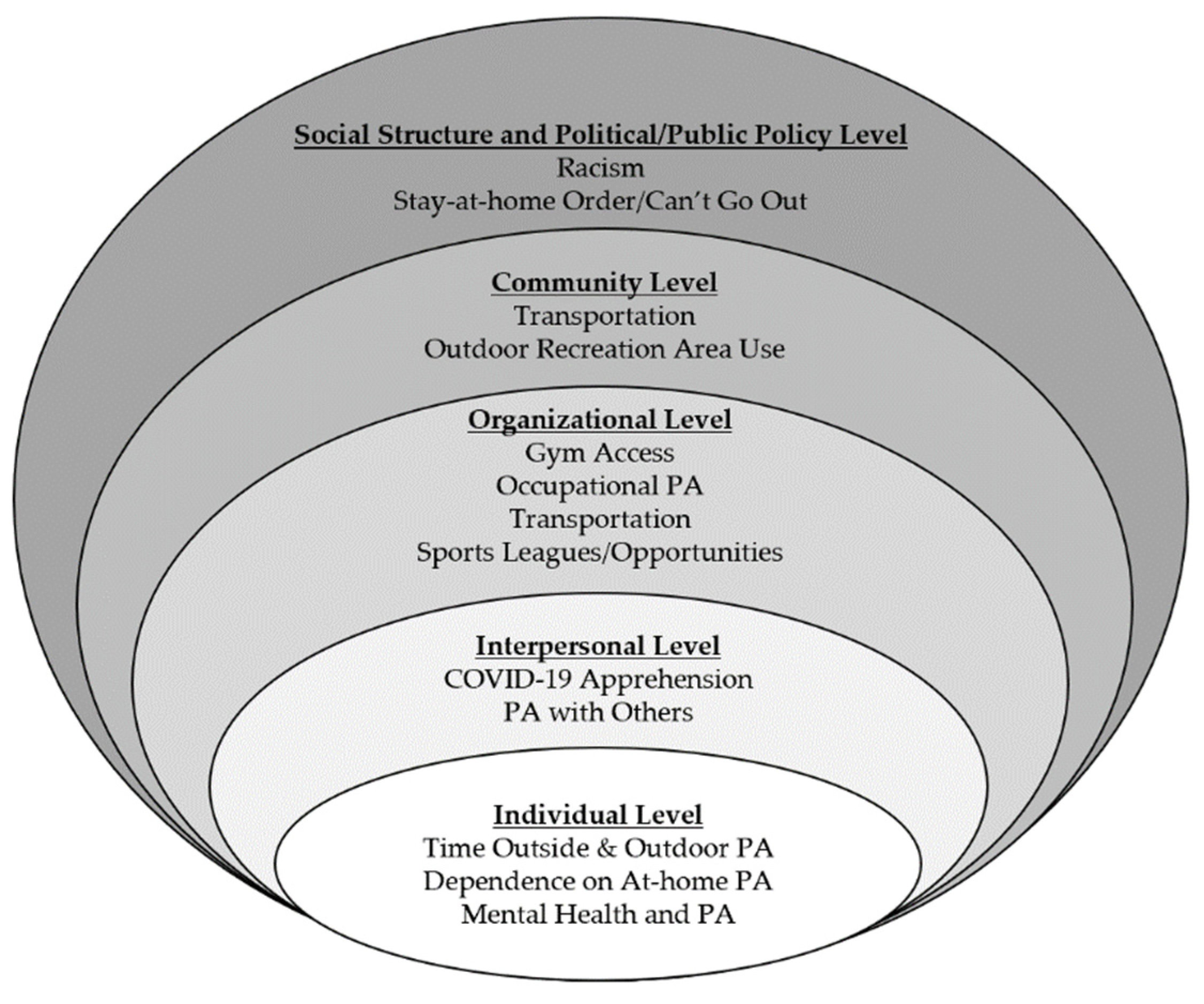
3.2. Qualitative Changes in PA Due to COVID-19 Related Events
3.2.1. Social Structure and Political/Public Policy Level
“I didn’t feel comfortable going on walks or runs around my neighborhood, especially because I am Asian.”
“The recent string of protests and rioting is probably going to impact my physical activity even more.”
“The current stay-at-home restrictions have limited the places that I can workout in public.”
3.2.2. Community Level
“My physical activity has decreased since parks, beaches, etc. are closed.”
“Since the COVID-19 outbreak I do not feel comfortable going outside on trails and paths that I typically frequent.”
3.2.3. Organizational Level
“Due to all the gyms being closed I have been unable to continue my regular exercise routine.”
“I get a lot of exercise from work but…I can’t work so I haven’t exercised at all.”
“I am out of work and at home, so I am exercising with my extra time that I have.”
“While I’m at school, I walk to get to class…and use public transit and bike shares to get around the city. So not having that regular commute/movement has really reduced my activity.”
“I would…enjoy soccer/volleyball. But no one wants to risk exposure, so we cancel that now.”
3.2.4. Interpersonal Level
“The fear of going out and getting sick has kept me from going to exercise…I’m in contact with a lot of people [due to work] so it’s hard to know if I have contact.”
“I would also go on a handful of walks during the week with my family or a friend to get out of the house and stay active.”
“I go on 3-4 mile runs every morning with my dog and evening walks as well”.
3.2.5. Individual Level
“I think COVID-19 is going to shape how I look at outdoor activity from now on and that it is ALWAYS an option whether it’s in the midst of a pandemic or not.”
“I have tried at-home workouts…but it doesn’t stick as well.”
“COVID-19 has caused a bit of depression and lack of energy to get out of bed most days.”
“My physical activity changed when I realized how mentally bad I felt after spending an entire day indoors. I have been getting out every day now.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-NCoV). Available online: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 10 January 2021).
- Proclamation on Declaring a National Emergency Concerning the Novel Coronavirus Disease (COVID-19) Outbreak. Available online: https://www.whitehouse.gov/presidential-actions/proclamation-declaring-national-emergency-concerning-novel-coronavirus-disease-covid-19-outbreak/ (accessed on 10 January 2021).
- Caputo, E.L.; Reichert, F.F. Studies of Physical Activity and COVID-19 during the Pandemic: A Scoping Review. J. Phys. Act. Health 2020, 17, 1275–1284. [Google Scholar] [CrossRef]
- Stults-Kolehmainen, M.A.; Sinha, R. The Effects of Stress on Physical Activity and Exercise. Sports Med. 2014, 44, 81–121. [Google Scholar] [CrossRef]
- Warburton, D.E.R. Health Benefits of Physical Activity: The Evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Penedo, F.J.; Dahn, J.R. Exercise and Well-Being: A Review of Mental and Physical Health Benefits Associated with Physical Activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 Pandemic on Mental Health in the General Population: A Systematic Review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- North, C.S. Mental Health and the Covid-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Emery, R.L.; Johnson, S.T.; Simone, M.; Loth, K.A.; Berge, J.M.; Neumark-Sztainer, D. Understanding the Impact of the COVID-19 Pandemic on Stress, Mood, and Substance Use among Young Adults during Initial Stay-at-Home Orders: A Mixed-Methods Study from Project EAT; Unpublished manuscript; Division of Epidemiology and Community Health, School of Public Health, University of Minnesota: Minneapolis, MN, USA, 2020. [Google Scholar]
- Wood, D.; Crapnell, T.; Lau, L.; Bennett, A.; Lotstein, D.; Ferris, M.; Kuo, A. Emerging Adulthood as a Critical Stage in the Life Course. In Handbook of Life Course Health Development; Halfon, N., Forrest, C.B., Lerner, R.M., Faustman, E.M., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 123–143. ISBN 978-3-319-47143-3. [Google Scholar]
- Germani, A.; Buratta, L.; Delvecchio, E.; Mazzeschi, C. Emerging Adults and COVID-19: The Role of Individualism-Collectivism on Perceived Risks and Psychological Maladjustment. Int. J. Environ. Res. Public Health 2020, 17, 3497. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion, Division of Nutrition, Physical Activity, and Obesity Health Equity Resource Toolkit for State Practitioners Addressing Obesity Disparities; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2017; p. 84.
- Arcan, C.; Larson, N.; Bauer, K.; Berge, J.; Story, M.; Neumark-Sztainer, D. Dietary and Weight-Related Behaviors and Body Mass Index among Hispanic, Hmong, Somali, and White Adolescents. J. Acad. Nutr. Diet. 2014, 114, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Larson, N.; Laska, M.N.; Neumark-Sztainer, D. Food Insecurity, Diet Quality, Home Food Availability, and Health Risk Behaviors Among Emerging Adults: Findings From the EAT 2010–2018 Study. Am. J. Public Health 2020, 110, 1422–1428. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.M.; Levine, A.; Barr-Anderson, D.J.; Eisenberg, M.E.; Larson, N. Yoga Practice among Ethnically/Racially Diverse Emerging Adults: Associations with Body Image, Mindful and Disordered Eating, and Muscle-Enhancing Behaviors. Int. J. Eat. Disord. 2020. [Google Scholar] [CrossRef]
- Larson, N.I.; Wall, M.M.; Story, M.T.; Neumark-Stzainer, D. Home/Family, Peer, School, and Neighborhood Correlates of Obesity in Adolescents. Obesity 2013, 21, 1858–1869. [Google Scholar] [CrossRef] [Green Version]
- Godin, G. The Godin-Shephard Leisure-Time Physical Activity Questionnaire. Health Fit. J. Can. 2011, 4, 18–22. [Google Scholar] [CrossRef]
- Sherwood, N.E.; Wall, M.; Neumark-Sztainer, D.; Story, M. Effect of Socioeconomic Status on Weight Change Patterns in Adolescents. Prev. Chronic Dis. 2009, 6, A19. [Google Scholar]
- Denzin, N.K.; Lincoln, Y.S. The SAGE Handbook of Qualitative Research; SAGE: Thousand Oaks, CA, USA, 2011; ISBN 978-1-4129-7417-2. [Google Scholar]
- Addison, R. A grounded hermeneutic editing approach. In Doing Qualitative Data Analysis; Crabtree, B., Miller, W., Eds.; Sage Thousand Oaks: Thousand Oaks, CA, USA, 1999. [Google Scholar]
- Prasad, S.; Westby, A.; Crichlow, R. Family Medicine, Community, and Race: A Minneapolis Practice Reflects. Ann. Fam. Med. 2021, 19, 69–71. [Google Scholar] [CrossRef]
- Pridgeon, L.; Grogan, S. Understanding Exercise Adherence and Dropout: An Interpretative Phenomenological Analysis of Men and Women’s Accounts of Gym Attendance and Non-Attendance. Qual. Res. Sport Exerc. Health 2012, 4, 382–399. [Google Scholar] [CrossRef]
- McArthur, D.; Dumas, A.; Woodend, K.; Beach, S.; Stacey, D. Factors Influencing Adherence to Regular Exercise in Middle-Aged Women: A Qualitative Study to Inform Clinical Practice. BMC Womens Health 2014, 14, 49. [Google Scholar] [CrossRef] [Green Version]
- Schvey, N.A.; Sbrocco, T.; Bakalar, J.L.; Ress, R.; Barmine, M.; Gorlick, J.; Pine, A.; Stephens, M.; Tanofsky-Kraff, M. The Experience of Weight Stigma among Gym Members with Overweight and Obesity. Stigma Health 2017, 2, 292–306. [Google Scholar] [CrossRef]
- Richardson, E.V.; Smith, B.; Papathomas, A. Disability and the Gym: Experiences, Barriers and Facilitators of Gym Use for Individuals with Physical Disabilities. Disabil. Rehabil. 2017, 39, 1950–1957. [Google Scholar] [CrossRef] [Green Version]
- Eime, R.M.; Harvey, J.; Charity, M.J.; Casey, M.; Westerbeek, H.; Payne, W.R. The Relationship of Sport Participation to Provision of Sports Facilities and Socioeconomic Status: A Geographical Analysis. Aust. N. Z. J. Public Health 2017, 41, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does Participating in Physical Activity in Outdoor Natural Environments Have a Greater Effect on Physical and Mental Wellbeing than Physical Activity Indoors? A Systematic Review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- Eigenschenk, B.; Thomann, A.; McClure, M.; Davies, L.; Gregory, M.; Dettweiler, U.; Inglés, E. Benefits of Outdoor Sports for Society. A Systematic Literature Review and Reflections on Evidence. Int. J. Environ. Res. Public Health 2019, 16, 937. [Google Scholar] [CrossRef] [Green Version]
- Dominski, F.H.; Brandt, R. Do the Benefits of Exercise in Indoor and Outdoor Environments during the COVID-19 Pandemic Outweigh the Risks of Infection? Sport Sci. Health 2020, 16, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Hammami, A.; Harrabi, B.; Mohr, M.; Krustrup, P. Physical Activity and Coronavirus Disease 2019 (COVID-19): Specific Recommendations for Home-Based Physical Training. Manag. Sport Leis. 2020, 1–6. [Google Scholar] [CrossRef]
- Carvalho, V.O.; Gois, C.O. COVID-19 Pandemic and Home-Based Physical Activity. J. Allergy Clin. Immunol. Pract. 2020, 8, 2833–2834. [Google Scholar] [CrossRef]
- Tietjen, A.M.J.; Devereux, G.R. Physical Demands of Exergaming in Healthy Young Adults. J. Strength Cond. Res. 2019, 33, 1978–1986. [Google Scholar] [CrossRef] [PubMed]
- Mohd Jai, N.A.; Mat Rosly, M.; Abd Razak, N.A. Physiological Responses of Exergaming Boxing in Adults: A Systematic Review and Meta-Analysis. Games Health J. 2020. [Google Scholar] [CrossRef]
- Douris, P.C.; McDonald, B.; Vespi, F.; Kelley, N.C.; Herman, L. Comparison Between Nintendo Wii Fit Aerobics and Traditional Aerobic Exercise in Sedentary Young Adults. J. Strength Cond. Res. 2012, 26, 1052–1057. [Google Scholar] [CrossRef]
- O’Loughlin, E.; Sabiston, C.M.; Kakinami, L.; McGrath, J.J.; Consalvo, M.; O’Loughlin, J.L.; Barnett, T.A. Development and Validation of the Reasons to Exergame (RTEX) Scale in Young Adults: Exploratory Factors Analysis. JMIR Serious Games 2020, 8, e16261. [Google Scholar] [CrossRef]
- Sallis, J.F.; Saelens, B.E. Assessment of Physical Activity by Self-Report: Status, Limitations, and Future Directions. Res. Q. Exerc. Sport 2000, 71, 1–14. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID-19 Hospitalization and Death by Race/Ethnicity; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020.
- Farmer, N.; Wallen, G.R.; Baumer, Y.; Powell-Wiley, T.M. COVID-19: Growing Health Disparity Gaps and an Opportunity for Health Behavior Discovery? Health Equity 2020, 4, 316–319. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Total |
|---|---|
| Age, mean ± SD | 24.7 ± 2.0 |
| Gender, n (%) | |
| Female | 447 (62.1) |
| Male | 263 (36.5) |
| Different identity | 10 (1.4) |
| Race/Ethnicity, n (%) | |
| White | 213 (29.6) |
| Black or African American | 130 (18.2) |
| Hispanic or Latino | 119 (16.5) |
| Asian American | 172 (23.9) |
| Native Hawaiian or other Pacific Islander | 4 (0.6) |
| American Indian or Native American | 21 (2.9) |
| Other 2 | 60 (8.3) |
| Parent Socioeconomic Status, n (%) | |
| Low | 231 (32.7) |
| Middle | 279 (37.6) |
| High | 210 (29.7) |
| Employment Status, n (%) | |
| Working full-time | 354 (50.9) |
| Working part-time | 114 (16.4) |
| Temporarily laid off or unemployed | 66 (9.5) |
| At-home caregiver/not working for pay | 162 (23.3) |
| Living Alone, n (%) | |
| Yes | 62 (8.6) |
| No | 658 (91.4) |
| Living with a parent(s), n (%) | |
| Yes | 324 (45.0) |
| No | 396 (55.0) |
| Living with a child(ren) of your own, n (%) | |
| Yes | 122 (16.9) |
| No | 598 (83.1) |
| Mild Physical Activity (hours/week), mean ± SD | |
| EAT 2018 | 3.09 ± 2.91 |
| C-EAT | 2.57 ± 2.77 * |
| Moderate-to-Vigorous Physical Activity (hours/week), mean ± SD | |
| EAT 2018 | 4.55 ± 4.13 |
| C-EAT | 3.62 ± 3.84 * |
| Total Physical Activity (hours/week), mean ± SD | |
| EAT 2018 | 7.63 ± 6.09 |
| C-EAT | 6.16 ± 5.68 * |
| Characteristic | Mild Intensity PA | Moderate-to-Vigorous PA | Total PA | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Decrease (%) | No Change (%) | Increase (%) | p-Value 1 | Decrease (%) | No Change (%) | Increase (%) | p-Value 1 | Decrease (%) | No Change (%) | Increase (%) | p-Value 1 | |
| Overall | 42.6 | 26.0 | 31.4 | 53.8 | 11.8 | 34.4 | 55.6 | 6.4 | 38.1 | |||
| Gender 2 | 0.68 | 0.56 | 0.90 | |||||||||
| Female | 43.8 | 26.0 | 30.2 | 52.1 | 11.9 | 36.0 | 54.6 | 6.7 | 38.7 | |||
| Male | 40.7 | 26.2 | 33.1 | 55.9 | 12.2 | 31.9 | 56.6 | 6.1 | 37.3 | |||
| Different identity | 40.0 | 20.0 | 40.0 | 70.0 | 0.0 | 30.0 | 70.0 | 0.0 | 30.0 | |||
| Race/Ethnicity | 0.11 | 0.64 | 0.16 | |||||||||
| White | 38.5 | 31.5 | 30.0 | 54.5 | 9.4 | 36.2 | 55.4 | 5.63 | 39.0 | |||
| Black or African American | 38.5 | 26.2 | 35.4 | 56.9 | 12.3 | 30.8 | 59.2 | 7.7 | 33.1 | |||
| Hispanic or Latino | 42.0 | 21.0 | 37.0 | 56.3 | 8.4 | 35.3 | 56.3 | 3.4 | 40.3 | |||
| Asian American | 51.7 | 21.5 | 26.7 | 51.7 | 15.7 | 32.6 | 57.0 | 5.8 | 37.2 | |||
| Native Hawaiian or other Pacific Islander | 50.0 | 0.0 | 50.0 | 50.0 | 0.0 | 50.0 | 50.0 | 0.0 | 50.0 | |||
| American Indian or Native American | 52.4 | 33.3 | 14.3 | 52.4 | 19.0 | 28.6 | 66.7 | 4.8 | 28.6 | |||
| Other | 36.7 | 28.3 | 35.0 | 45.0 | 13.3 | 41.7 | 38.3 | 15.0 | 46.7 | |||
| Parent Socioeconomic Status | 0.39 | 0.21 | 0.001 * | |||||||||
| Low | 46.3 | 23.4 | 30.3 | 56.7 | 12.6 | 30.7 | 57.6 | 6.5 | 35.9 | |||
| Middle | 41.9 | 28.7 | 29.4 | 52.7 | 13.6 | 33.7 | 57.4 | 9.0 | 33.7 | |||
| High | 39.5 | 25.2 | 35.2 | 51.9 | 8.6 | 39.5 | 50.1 | 2.9 | 46.2 | |||
| Employment Status | 0.44 | 0.23 | 0.28 | |||||||||
| Working full-time | 41.5 | 24.9 | 33.6 | 52.8 | 10.4 | 36.7 | 54.2 | 5.1 | 40.7 | |||
| Working part-time | 45.6 | 22.8 | 31.6 | 58.8 | 11.4 | 29.8 | 54.4 | 8.8 | 36.8 | |||
| Temporarily laid off or unemployed | 53.0 | 25.8 | 21.2 | 62.1 | 9.1 | 28.8 | 66.7 | 4.6 | 28.8 | |||
| At-home caregiver/not working for pay | 39.5 | 27.8 | 32.7 | 49.4 | 16.7 | 34.0 | 53.7 | 8.6 | 37.6 | |||
| Living Alone | 0.90 | 0.43 | 0.36 | |||||||||
| Yes | 45.2 | 24.2 | 31.5 | 61.3 | 11.3 | 35.1 | 62.9 | 3.2 | 33.9 | |||
| No | 42.4 | 26.1 | 30.6 | 53.0 | 11.8 | 27.4 | 54.9 | 6.7 | 38.4 | |||
| Living with a parent(s) | 0.22 | 0.28 | 0.44 | |||||||||
| Yes | 46.0 | 25.3 | 28.7 | 54.3 | 13.6 | 32.1 | 56.5 | 7.4 | 36.1 | |||
| No | 39.9 | 26.5 | 33.6 | 53.3 | 10.4 | 36.4 | 54.8 | 5.6 | 39.6 | |||
| Living with a child(ren) of your own | 0.52 | 0.91 | 0.89 | |||||||||
| Yes | 43.4 | 22.1 | 34.4 | 54.9 | 12.3 | 32.8 | 54.9 | 7.4 | 37.7 | |||
| No | 42.5 | 26.8 | 30.8 | 53.5 | 11.7 | 34.8 | 55.7 | 6.2 | 38.1 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Folk, A.L.; Wagner, B.E.; Hahn, S.L.; Larson, N.; Barr-Anderson, D.J.; Neumark-Sztainer, D. Changes to Physical Activity during a Global Pandemic: A Mixed Methods Analysis among a Diverse Population-Based Sample of Emerging Adults in the U.S. Int. J. Environ. Res. Public Health 2021, 18, 3674. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073674
Folk AL, Wagner BE, Hahn SL, Larson N, Barr-Anderson DJ, Neumark-Sztainer D. Changes to Physical Activity during a Global Pandemic: A Mixed Methods Analysis among a Diverse Population-Based Sample of Emerging Adults in the U.S. International Journal of Environmental Research and Public Health. 2021; 18(7):3674. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073674
Chicago/Turabian StyleFolk, Amanda L., Brooke E. Wagner, Samantha L. Hahn, Nicole Larson, Daheia J. Barr-Anderson, and Dianne Neumark-Sztainer. 2021. "Changes to Physical Activity during a Global Pandemic: A Mixed Methods Analysis among a Diverse Population-Based Sample of Emerging Adults in the U.S." International Journal of Environmental Research and Public Health 18, no. 7: 3674. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073674