
Midday Nap Duration and Hypertension among Middle-Aged and Older Chinese Adults: A Nationwide Retrospective Cohort Study




Abstract
:1. Introduction
2. Materials and Methods
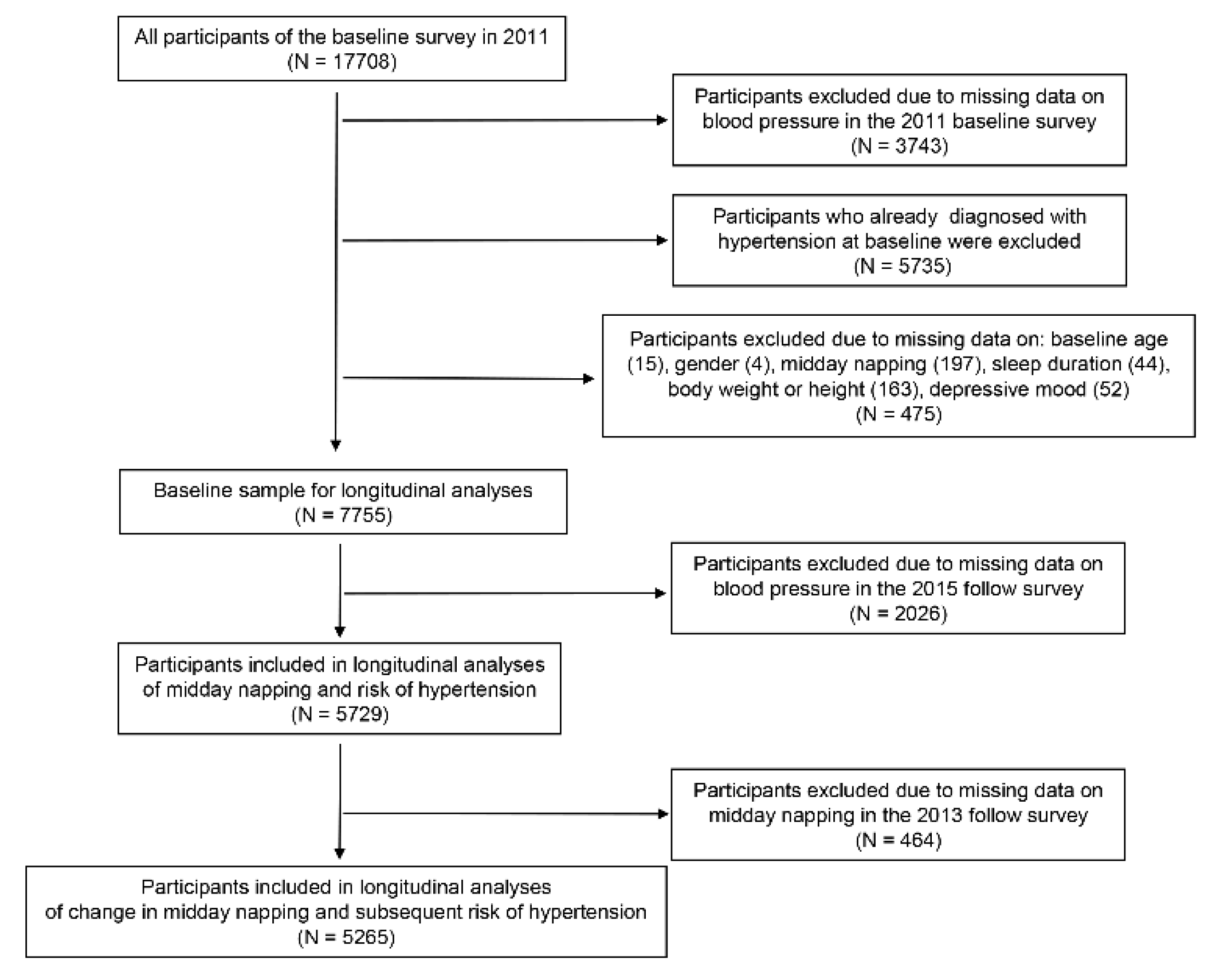
2.1. Study Participants
2.2. Measurements of Sleep Duration and Hypertension
2.3. Potential Confounders
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Variables | 0 min (N = 2839) | 1–29 min (N = 495) | 30–59 min (N = 485) | 60–89 min (N = 1210) | ≥90 min (N = 700) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Person-Years | Adjusted HR | Person-Years | Adjusted HR (95% CI) | Person-Years | Adjusted HR (95% CI) | Person-Years | Adjusted HR (95% CI) | Person-Years | Adjusted HR (95% CI) | |
| Age (years) | ||||||||||
| 45–60 | 7090 | 1.00 (ref.) | 1144 | 1.23 (0.93–1.61) | 1184 | 1.19 (0.90–1.57) | 2900 | 1.01 (0.82–1.24) | 1546 | 1.17 (0.92–1.50) |
| ≥60 | 3626 | 1.00 (ref.) | 690 | 1.01 (0.76–1.34) | 634 | 1.00 (0.75–1.35) | 1692 | 0.78 (0.62–0.97) * | 1024 | 1.18 (0.94–1.48) |
| Gender | ||||||||||
| Male | 5184 | 1.00 (ref.) | 940 | 1.14 (0.87–1.49) | 808 | 1.19 (0.89–1.59) | 2240 | 0.95 (0.77–1.17) | 1158 | 1.19 (0.93–1.52) |
| Female | 5532 | 1.00 (ref.) | 894 | 1.09 (0.82–1.45) | 1010 | 1.03 (0.78–1.36) | 2352 | 0.85 (0.68–1.05) | 1412 | 1.18 (0.94–1.48) |
| BMI (kg/m2) | ||||||||||
| <24 | 7474 | 1.00 (ref.) | 1170 | 1.09 (0.85–1.40) | 1242 | 1.01 (0.78–1.31) | 2966 | 0.85 (0.70–1.02) | 1614 | 1.10 (0.89–1.37) |
| ≥ 24 | 3242 | 1.00 (ref.) | 664 | 1.17 (0.85–1.60) | 576 | 1.25 (0.90–1.72) | 1626 | 0.97 (0.76–1.24) | 956 | 1.31 (1.01–1.71) * |
| Sleep duration (hours) | ||||||||||
| ≤6 | 5582 | 1.00 (ref.) | 884 | 0.94 (0.70–1.26) | 960 | 1.04 (0.79–1.38) | 2134 | 0.86 (0.69–1.06) | 1024 | 1.08 (0.83–1.40) |
| 6–8 | 2034 | 1.00 (ref.) | 408 | 1.32 (0.88–1.97) | 376 | 0.90 (0.56–1.46) | 1040 | 0.86 (0.62–1.20) | 504 | 1.28 (0.89–1.83) |
| ≥8 | 3100 | 1.00 (ref.) | 542 | 1.32 (0.93–1.89) | 482 | 1.34 (0.92–1.94) | 1418 | 1.00 (0.76–1.32) | 1042 | 1.35 (1.02–1.78) * |
| Smoking | ||||||||||
| Current | 3094 | 1.00 (ref.) | 560 | 1.54 (1.12–2.11) ** | 484 | 1.18 (0.81–1.71) | 1574 | 1.10 (0.86–1.41) | 992 | 1.34 (1.02–1.75) * |
| Former | 602 | 1.00 (ref.) | 152 | 0.81 (0.38–1.75) | 120 | 1.43 (0.73–2.83) | 474 | 1.09 (0.69–1.73) | 246 | 1.23 (0.70–2.14) |
| Never | 7020 | 1.00 (ref.) | 1122 | 1.15 (0.88–1.49) | 1214 | 1.01 (0.76–1.33) | 2544 | 0.92 (0.75–1.13) | 1332 | 1.27 (1.01–1.60) * |
| Drinking | ||||||||||
| Current | 3116 | 1.00 (ref.) | 660 | 1.22 (0.89–1.66) | 590 | 1.15 (0.82–1.61) | 1774 | 0.93 (0.73–1.18) | 1050 | 1.14 (0.87–1.49) |
| Former | 638 | 1.00 (ref.) | 94 | 0.49 (0.15–1.60) | 142 | 1.37 (0.73–2.57) | 322 | 0.75 (0.42–1.34) | 198 | 1.09 (0.59–1.98) |
| Never | 6962 | 1.00 (ref.) | 1080 | 1.16 (0.89–1.50) | 1086 | 1.02 (0.77–1.34) | 2496 | 0.91 (0.74–1.11) | 1322 | 1.30 (1.03–1.64) * |
| Depression | ||||||||||
| Yes | 5220 | 1.00 (ref.) | 808 | 1.11 (0.82–1.50) | 890 | 0.96 (0.70–1.31) | 2054 | 0.82 (0.65–1.04) | 1166 | 1.18 (0.92–1.52) |
| No | 5496 | 1.00 (ref.) | 1026 | 1.13 (0.87–1.47) | 928 | 1.18 (0.91–1.55) | 2538 | 0.94 (0.78–1.15) | 1404 | 1.17 (0.93–1.46) |
| Hyperlipidemia | ||||||||||
| Yes | 408 | 1.00 (ref.) | 112 | 0.88 (0.35–2.23) | 104 | 0.49 (0.14–1.67) | 244 | 0.79 (0.37–1.68) | 176 | 1.30 (0.64–2.61) |
| No | 10,308 | 1.00 (ref.) | 1722 | 1.14 (0.94–1.40) | 1374 | 1.14 (0.93–1.39) | 4592 | 0.91 (0.78–1.06) | 3260 | 1.20 (1.01–1.42) * |
| Diabetes | ||||||||||
| Yes | 292 | 1.00 (ref.) | 48 | 0.46 (0.11–1.95) | 100 | 0.82 (0.35–1.91) | 188 | 0.65 (0.33–1.30) | 104 | 0.82 (0.35–1.94) |
| No | 10,424 | 1.00 (ref.) | 1786 | 1.15 (0.94–1.40) | 1718 | 1.11 (0.90–1.37) | 4404 | 0.90 (0.77–1.05) | 2466 | 1.19 (1.00–1.41) * |
References
- Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903. [Google Scholar] [CrossRef]
- Lassere, M.N.; Johnson, K.R.; Schiff, M.; Rees, D. Is blood pressure reduction a valid surrogate endpoint for stroke prevention? an analysis incorporating a systematic review of randomised controlled trials, a by-trial weighted errors-in-variables regression, the surrogate threshold effect (STE) and the biomarker-surrogacy (BioSurrogate) evaluation schema (BSES). BMC Med. Res. Methodol. 2012, 12, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Wagner, J.; Ball, J. Implications of the institute of medicine report: Evaluation of biomarkers and surrogate endpoints in chronic disease. Clin. Pharmacol. Ther. 2015, 98, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.; Stockbridge, N.; Temple, R. Blood pressure as an example of a biomarker that functions as a surrogate. AAPS J. 2006, 8, E146–E152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulter, N.R.; Prabhakaran, D.; Caulfield, M. Hypertension. Lancet 2015, 386, 801–812. [Google Scholar] [CrossRef]
- Zhou, B.; Bentham, J.; Di Cesare, M.; Bixby, H.; Danaei, G.; Cowan, M.J.; Paciorek, C.J.; Singh, G.; Hajifathalian, K.; Bennett, J.E.; et al. Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef] [Green Version]
- GBD 2017 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study Lancet 2018, 392, 1923–1994. [CrossRef] [Green Version]
- Lu, J.; Lu, Y.; Wang, X.; Li, X.; Linderman, G.C.; Wu, C.; Cheng, X.; Mu, L.; Zhang, H.; Liu, J.; et al. Prevalence, awareness, treatment, and control of hypertension in China: Data from 1·7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet 2017, 390, 2549–2558. [Google Scholar] [CrossRef]
- Staessen, J.A.; Wang, J.; Bianchi, G.; Birkenhäger, W.H. Essential hypertension. Lancet 2003, 361, 1629–1641. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, D.; Liu, Y.; Sun, X.; Han, C.; Wang, B.; Ren, Y.; Zhou, J.; Zhao, Y.; Shi, Y.; et al. Dose–Response Association Between Physical Activity and Incident Hypertension. Hypertensionaha 2017, 69, 813–820. [Google Scholar] [CrossRef]
- Seravalle, G.; Grassi, G. Obesity and hypertension. Pharmacol. Res. 2017, 122, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Srivali, N.; Vijayvargiya, P.; Andersen, C.A.; Kittanamongkolchai, W.; Sathick, I.J.J.; Caples, S.M.; Erickson, S.B. The effects of napping on the risk of hypertension: A systematic review and meta-analysis. J. Evid. Based Med. 2016, 9, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Lan, T.-Y.; Lan, T.-H.; Wen, C.-P.; Lin, M.Y.-H.; Chuang, M.Y.-L. Nighttime Sleep, Chinese Afternoon Nap, and Mortality in the Elderly. Sleep 2007, 30, 1105–1110. [Google Scholar] [CrossRef] [Green Version]
- Milner, C.E.; Cote, K.A. Benefits of napping in healthy adults: Impact of nap length, time of day, age, and experience with napping. J. Sleep Res. 2009, 18, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Faraut, B.; Andrillon, T.; Vecchierini, M.-F.; Leger, D. Napping: A public health issue. From epidemiological to laboratory studies. Sleep Med. Rev. 2017, 35, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Hara, K.; Shojima, N.; Yamauchi, T.; Kadowaki, T. Daytime Napping and the Risk of Cardiovascular Disease and All-Cause Mortality: A Prospective Study and Dose-Response Meta-Analysis. Sleep 2015, 38, 1945–1953. [Google Scholar] [CrossRef]
- Leng, Y.; Ahmadi-Abhari, S.; Wainwright, N.W.J.; Cappuccio, F.P.; Surtees, P.G.; Luben, R.; Brayne, C.; Khaw, K.-T. Daytime napping, sleep duration and serum C reactive protein: A population-based cohort study. BMJ Open 2014, 4, e006071. [Google Scholar] [CrossRef]
- Tanabe, N.; Iso, H.; Seki, N.; Suzuki, H.; Yatsuya, H.; Toyoshima, H.; Tamakoshi, A.; JACC Study Group. Daytime napping and mortality, with a special reference to cardiovascular disease: The JACC study. Int. J. Epidemiol. 2009, 39, 233–243. [Google Scholar] [CrossRef] [Green Version]
- Léger, D.; Torres, M.J.; Bayon, V.; Hercberg, S.; Galan, P.; Chennaoui, M.; Andreeva, V.A. The association between physical and mental chronic conditions and napping. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Bangdiwala, S.; Rangarajan, S.; Lear, S.; Alhabib, K.F.; Mohan, V.; Teo, K.; Poirier, P.; Tse, L.A.; Liu, Z.; et al. Association of estimated sleep duration and naps with mortality and cardiovascular events: A study of 116 632 people from 21 countries. Eur. Heart J. 2019, 40, 1620–1629. [Google Scholar] [CrossRef]
- Zhou, J.; Kessler, A.S.; Su, D. Association between Daytime Napping and Chronic Diseases in China. Am. J. Health Behav. 2016, 40, 182–193. [Google Scholar] [CrossRef]
- Cao, Z.; Shen, L.; Wu, J.; Yang, H.; Fang, W.; Chen, W.; Yuan, J.; Wang, Y.; Liang, Y.; Wu, T. The effects of midday nap duration on the risk of hypertension in a middle-aged and older Chinese population. J. Hypertens. 2014, 32, 1993–1998. [Google Scholar] [CrossRef]
- Lin, M.; Su, Q.; Wen, J.; Wei, S.; Yao, J.; Huang, H.; Liang, J.; Li, L.; Lin, W.; Lin, L.; et al. Self-reported sleep duration and daytime napping are associated with renal hyperfiltration in general population. Sleep Breath. 2017, 22, 223–232. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, W.; Ji, X.; Ma, C.; Wang, X.; Li, K.; Li, J. Extended afternoon naps are associated with hypertension in women but not in men. Heart Lung 2020, 49, 2–9. [Google Scholar] [CrossRef]
- Zhao, H.; Gui, W.; Huang, H.; Liu, Y.; Ding, H.; Fan, W.; Huang, S.; Yang, W.; Wang, X.; Chen, G. Association of long-term sleep habits and hypertension: A cross-sectional study in Chinese adults. J. Hum. Hypertens. 2019, 34, 378–387. [Google Scholar] [CrossRef]
- Cao, Y.M.; Li, D.; Li, K.B.; Yu, H.; Xin, W.; Miao, D.J.; An, Y. Epidemiological study on the relationship between the siesta and blood pressure. Zhonghua yi Xue Za Zhi 2016, 96, 1699–1701. [Google Scholar] [PubMed]
- Cai, M.; Huang, Y.; Sun, X.; He, Y.; Sun, C. Siesta is associated with reduced systolic blood pressure level and decreased prevalence of hypertension in older adults. J. Hum. Hypertens. 2015, 30, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Yang, Y.; Huang, Z.; Yuan, H.; Lu, Y. The association of nighttime sleep duration and daytime napping duration with hypertension in Chinese rural areas: A population-based study. J. Hum. Hypertens. 2020, 1–7. [Google Scholar] [CrossRef]
- Wu, L.; He, Y.; Jiang, B.; Liu, M.; Wang, J.; Zhang, D.; Wang, Y.; Zeng, J.; Yao, Y. Association between sleep duration and the prevalence of hypertension in an elderly rural population of China. Sleep Med. 2016, 27–28, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Zomers, M.L.; Hulsegge, G.; Van Oostrom, S.H.; Proper, K.I.; Verschuren, W.M.M.; Picavet, H.S.J. Characterizing Adult Sleep Behavior Over 20 Years—The Population-Based Doetinchem Cohort Study. Sleep 2017, 40, 40. [Google Scholar] [CrossRef] [PubMed]
- Gangwisch, J.E. A Review of Evidence for the Link between Sleep Duration and Hypertension. Am. J. Hypertens. 2014, 27, 1235–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort Profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2014, 43, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Wu, Y.; Zhai, L.; Wang, T.; Sun, Y.; Zhang, D. Longitudinal Association of Sleep Duration with Depressive Symptoms among Middle-aged and Older Chinese. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef]
- Li, J.; Cacchione, P.Z.; Hodgson, N.; Riegel, B.; Ms, B.T.K.; Scharf, M.T.; Richards, K.C.; Gooneratne, N.S. Afternoon Napping and Cognition in Chinese Older Adults: Findings from the China Health and Retirement Longitudinal Study Baseline Assessment. J. Am. Geriatr. Soc. 2017, 65, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension. J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for Depression in Well Older Adults: Evaluation of a Short Form of the CES-D. Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Head, G.; Lukoshkova, E.V. Understanding the Morning Rise in Blood Pressure. Clin. Exp. Pharmacol. Physiol. 2008, 35, 516–521. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Mastorantonakis, S.E.; Roussias, L.G. Intraindividual Reproducibility of Blood Pressure Surge upon Rising after Nighttime Sleep and Siesta. Hypertens. Res. 2008, 31, 1859–1864. [Google Scholar] [CrossRef] [Green Version]
- Woods, D.L.; Kim, H.; Yefimova, M. To Nap or Not to Nap. Biol. Res. Nurs. 2011, 15, 185–190. [Google Scholar] [CrossRef]
- Wang, Y.; Mei, H.; Jiang, Y.-R.; Sun, W.-Q.; Song, Y.-J.; Liu, S.-J.; Jiang, F. Relationship between Duration of Sleep and Hypertension in Adults: A Meta-Analysis. J. Clin. Sleep Med. 2015, 11, 1047–1056. [Google Scholar] [CrossRef]
- Floras, J.S. Hypertension and Sleep Apnea. Can. J. Cardiol. 2015, 31, 889–897. [Google Scholar] [CrossRef] [PubMed]
- Masa, J.F.; Rubio, M.; Pérez, P.; Mota, M.; De Cos, J.S.; Montserrat, J.M. Association between Habitual Naps and Sleep Apnea. Sleep 2006, 29, 1463–1468. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R.; Osteoporotic Fractures in Men for the Osteoporotic Fractures in Men (MrOS) and the Study of Osteoporotic Fractures (SOF) Research Groups; Hayes, A.L.; Blackwell, T.; Evans, D.S.; Ancoli-Israel, S.; Wing, Y.K.; Stone, K.L. The association between sleep patterns and obesity in older adults. Int. J. Obes. 2014, 38, 1159–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, W.; Li, Z.; Wu, L.; Cao, Z.; Liang, Y.; Yang, H.; Wang, Y.; Wu, T. Longer habitual afternoon napping is associated with a higher risk for impaired fasting plasma glucose and diabetes mellitus in older adults: Results from the Dongfeng–Tongji cohort of retired workers. Sleep Med. 2013, 14, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E.; Cushman, W.C. Diabetes and hypertension: The bad companions. Lancet 2012, 380, 601–610. [Google Scholar] [CrossRef]
- Eckel, N.; Meidtner, K.; Kalle-Uhlmann, T.; Stefan, N.; Schulze, M.B. Metabolically healthy obesity and cardiovascular events: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2016, 23, 956–966. [Google Scholar] [CrossRef]
- Lauderdale, D.S.; Knutson, K.L.; Yan, L.L.; Liu, K.; Rathouz, P.J. Self-Reported and Measured Sleep Duration. Epidemiology 2008, 19, 838–845. [Google Scholar] [CrossRef] [Green Version]
- St-Onge, M.-P.; Grandner, M.A.; Brown, D.; Conroy, M.B.; Jean-Louis, G.; Coons, M.; Bhatt, D.L. Sleep Duration and Quality: Impact on Lifestyle Behaviors and Cardiometabolic Health: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e367–e386. [Google Scholar] [CrossRef] [Green Version]
- Loredo, J.S.; Ancoli-Israel, S.; Dimsdale, J.E. Sleep quality and blood pressure dipping in obstructive sleep apnea. Am. J. Hypertens. 2001, 14, 887–892. [Google Scholar] [CrossRef]

| Variables | 0 min (N = 2839) | 1–29 min (N = 495) | 30–59 min (N = 485) | 60–89 min (N = 1210) | ≥90 min (N = 700) | p Value 3 |
|---|---|---|---|---|---|---|
| Age (years) 1 | 56.50 (13.00) | 57.50 (12.00) | 56.50 (12.00) | 56.50 (14.00) | 57.50 (15.00) | 0.027 |
| Gender 2 | 0.175 | |||||
| Male | 1372 (48.33) | 251 (50.71) | 219 (45.15) | 595 (49.17) | 315 (45.00) | |
| Female | 1467 (51.67) | 244 (49.29) | 266 (54.85) | 615 (50.83) | 385 (55.00) | |
| BMI (kg/m2) 1 | 22.32 (4.22) | 22.92 (4.60) | 22.49 (4.49) | 22.84 (4.57) | 22.74(4.76) | <0.001 |
| Smoking status 2 | <0.001 | |||||
| Current | 815 (28.71) | 158 (31.92) | 130 (26.80) | 421 (34.79) | 276 (39.43) | |
| Former | 162 (5.71) | 40 (8.08) | 33 (6.80) | 126 (10.41) | 67 (9.57) | |
| Never | 1862 (65.59) | 297 (60.00) | 322 (66.39) | 663 (54.79) | 357 (51.00) | |
| Drinking status 2 | <0.001 | |||||
| Current | 828 (29.17) | 178 (35.96) | 158 (32.58) | 473 (39.09) | 289 (41.29) | |
| Former | 171 (6.02) | 25 (5.05) | 38 (7.84) | 84 (6.94) | 55 (7.86) | |
| Never | 1840 (64.81) | 292 (58.99) | 289 (59.59) | 653 (53.97) | 356 (50.86) | |
| SBP (mmHg) 1 | 118.33 (17.67) | 119.33 (17.00) | 118.00 (18.00) | 117.67 (17.00) | 119.00 (17.67) | 0.229 |
| DBP (mmHg) 1 | 70.33 (12.33) | 71.33 (12.00) | 70.67 (13.33) | 69.67 (12.67) | 71.00 (12.33) | 0.039 |
| Sleep duration (h) 1 | 6.00 (3.00) | 7.00 (3.00) | 6.00 (3.00) | 7.00 (2.00) | 7.00 (2.00) | <0.001 |
| Depression 2 | 1380 (48.61) | 220 (44.44) | 233 (48.04) | 540 (44.63) | 317 (45.29) | 0.091 |
| Comorbidities 2 | ||||||
| Hyperlipidemia | 109 (3.84) | 31 (6.26) | 27 (5.57) | 62 (5.12) | 48 (6.86) | 0.004 |
| Diabetes | 80 (2.82) | 13 (2.63) | 26 (5.36) | 49 (4.05) | 28 (4.00) | 0.019 |
| Midday Napping, Minutes | Cases/N | Person-Years | Unadjusted HR (95% CI) 1 | p Value | Adjusted HR (95% CI) 2 | p Value |
|---|---|---|---|---|---|---|
| 0 min | 600/2839 | 10,716 | 1.00 (ref.) | 1.00 (ref.) | ||
| 1–29 min | 121/495 | 1834 | 1.18 (0.97–1.43) | 0.101 | 1.12 (0.92–1.36) | 0.260 |
| 30–59 min | 113/485 | 1818 | 1.11 (0.91–1.36) | 0.309 | 1.10 (0.90–1.34) | 0.366 |
| 60–89 min | 244/1210 | 4592 | 0.95 (0.82–1.10) | 0.492 | 0.89 (0.77–1.04) | 0.133 |
| ≥90 min | 185/700 | 2570 | 1.28 (1.09–1.51) | 0.003 | 1.18 (1.01–1.40) | 0.048 |
| Midday Napping, Minutes | Cases/N | Person- Years | Unadjusted HR (95% CI) | p Value | Adjusted HR (95% CI) 1 | p Value | |
|---|---|---|---|---|---|---|---|
| 2011 | 2013 | ||||||
| 0 min | 0 min | 389/1752 | 6576 | 1.00 (ref.) 2 | 1.00 (ref.) 6 | ||
| 1–59 min | 61/287 | 1080 | 0.95 (0.73–1.25) | 0.738 | 0.95 (0.72–1.24) | 0.701 | |
| 60–89 min | 81/341 | 1274 | 1.07 (0.85–1.37) | 0.556 | 1.00 (0.79–1.28) | 0.973 | |
| ≥90 min | 36/215 | 820 | 0.74 (0.53–1.05) | 0.088 | 0.73 (0.52–1.03) | 0.073 | |
| 1–59 min | 0 min | 60/245 | 902 | 1.04 (0.73–1.47) | 0.828 | 1.08 (0.76–1.53) | 0.673 |
| 1–59 min | 68/285 | 1064 | 1.00 (ref.) 3 | 1.00 (ref.) 7 | |||
| 60–89 min | 56/220 | 826 | 1.06 (0.75–1.51) | 0.741 | 0.98 (0.69–1.40) | 0.920 | |
| ≥90 min | 39/140 | 506 | 1.20 (0.81–1.78) | 0.36 | 1.13 (0.76–1.68) | 0.551 | |
| 60–89 min | 0 min | 56/256 | 962 | 1.11 (0.79–1.57) | 0.544 | 1.18 (0.83–1.67) | 0.359 |
| 1–59 min | 42/229 | 874 | 0.92 (0.63–1.34) | 0.66 | 0.97 (0.66–1.42) | 0.867 | |
| 60–89 min | 75/380 | 1434 | 1.00 (ref.) 4 | 1.00 (ref.) 8 | |||
| ≥90 min | 58/240 | 906 | 1.22 (0.87–1.72) | 0.248 | 1.14 (0.80–1.61) | 0.470 | |
| ≥90 min | 0 min | 25/108 | 396 | 0.72 (0.46–1.12) | 0.145 | 0.77 (0.49–1.20) | 0.251 |
| 1–59 min | 19/102 | 384 | 0.57 (0.35–0.93) | 0.025 | 0.59 (0.36–0.97) | 0.037 | |
| 60–89 min | 40/184 | 690 | 0.66 (0.46–0.96) | 0.031 | 0.68 (0.47–0.99) | 0.044 | |
| ≥90 min | 89/281 | 1010 | 1.00 (ref.) 5 | 1.00 (ref.) 9 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, J.; Zhang, X.; Moore, J.B.; Wang, B.; Li, R. Midday Nap Duration and Hypertension among Middle-Aged and Older Chinese Adults: A Nationwide Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 3680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073680
Fu J, Zhang X, Moore JB, Wang B, Li R. Midday Nap Duration and Hypertension among Middle-Aged and Older Chinese Adults: A Nationwide Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(7):3680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073680
Chicago/Turabian StyleFu, Jialin, Xinge Zhang, Justin B. Moore, Bowen Wang, and Rui Li. 2021. "Midday Nap Duration and Hypertension among Middle-Aged and Older Chinese Adults: A Nationwide Retrospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 7: 3680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073680