
Healthcare Costs Associated with Complications in Patients with Type 2 Diabetes among 1.85 Million Adults in Beijing, China

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Sample
2.3. Statistical Analysis
3. Results
3.1. Demographics
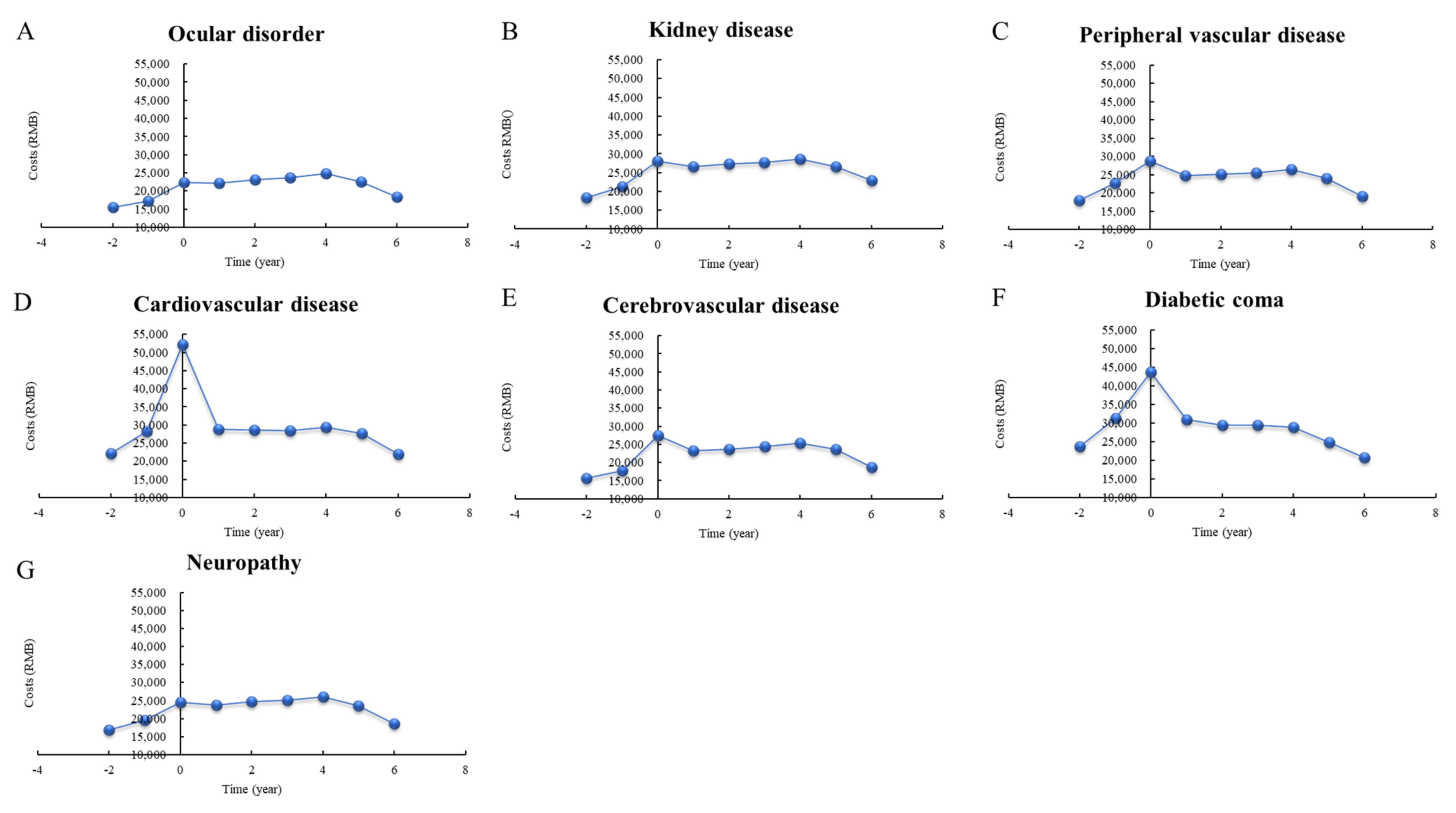
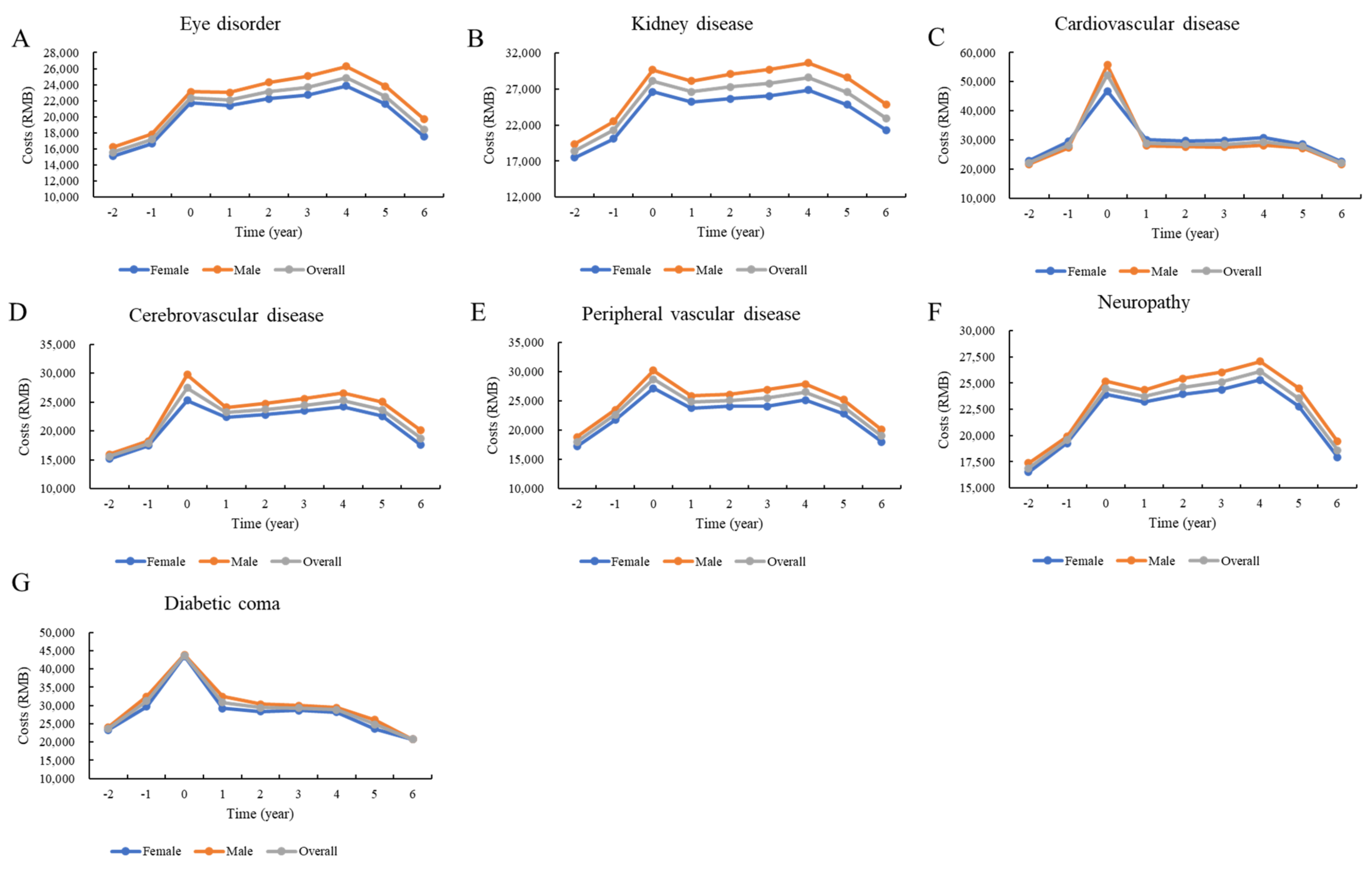
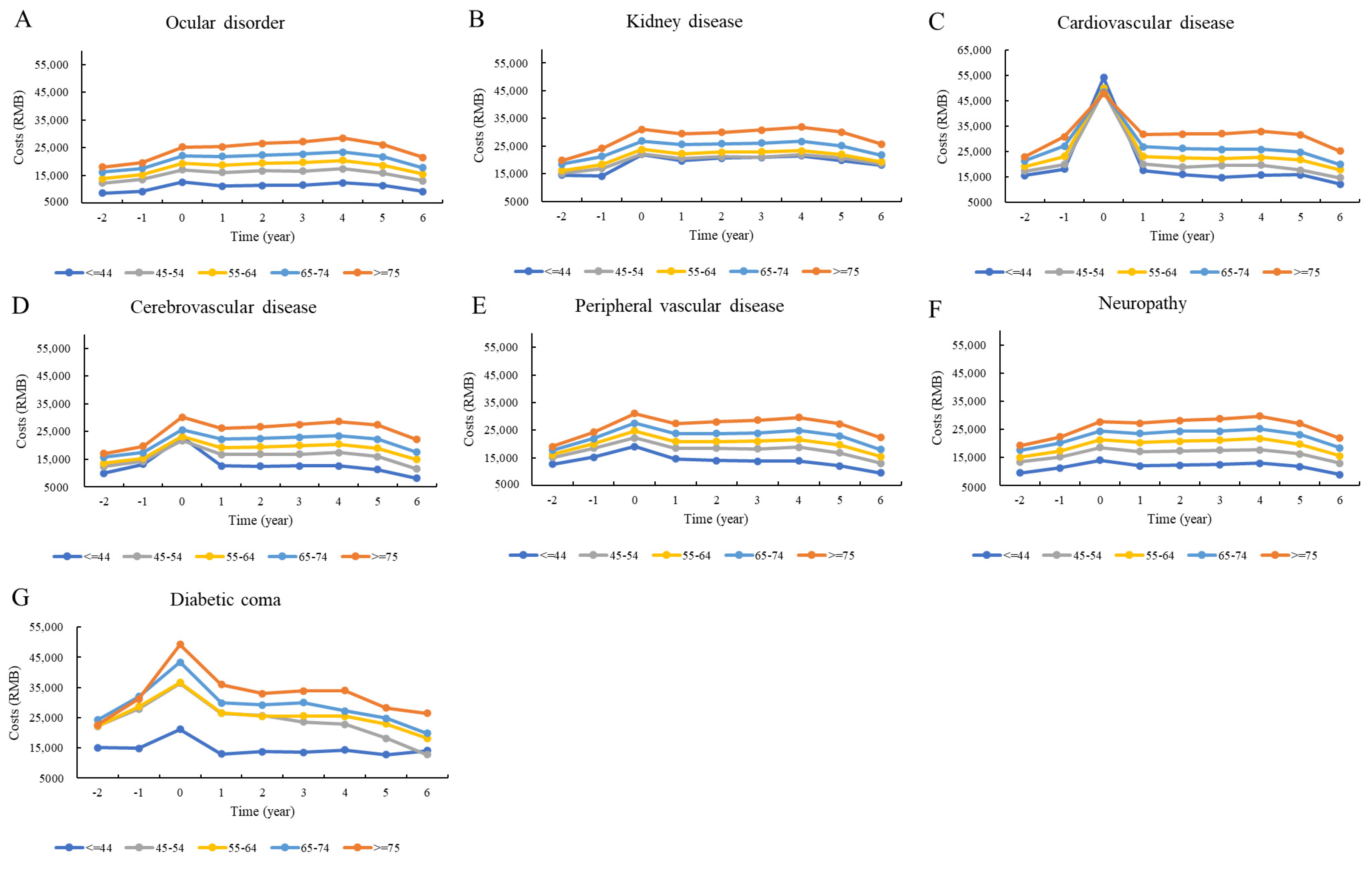
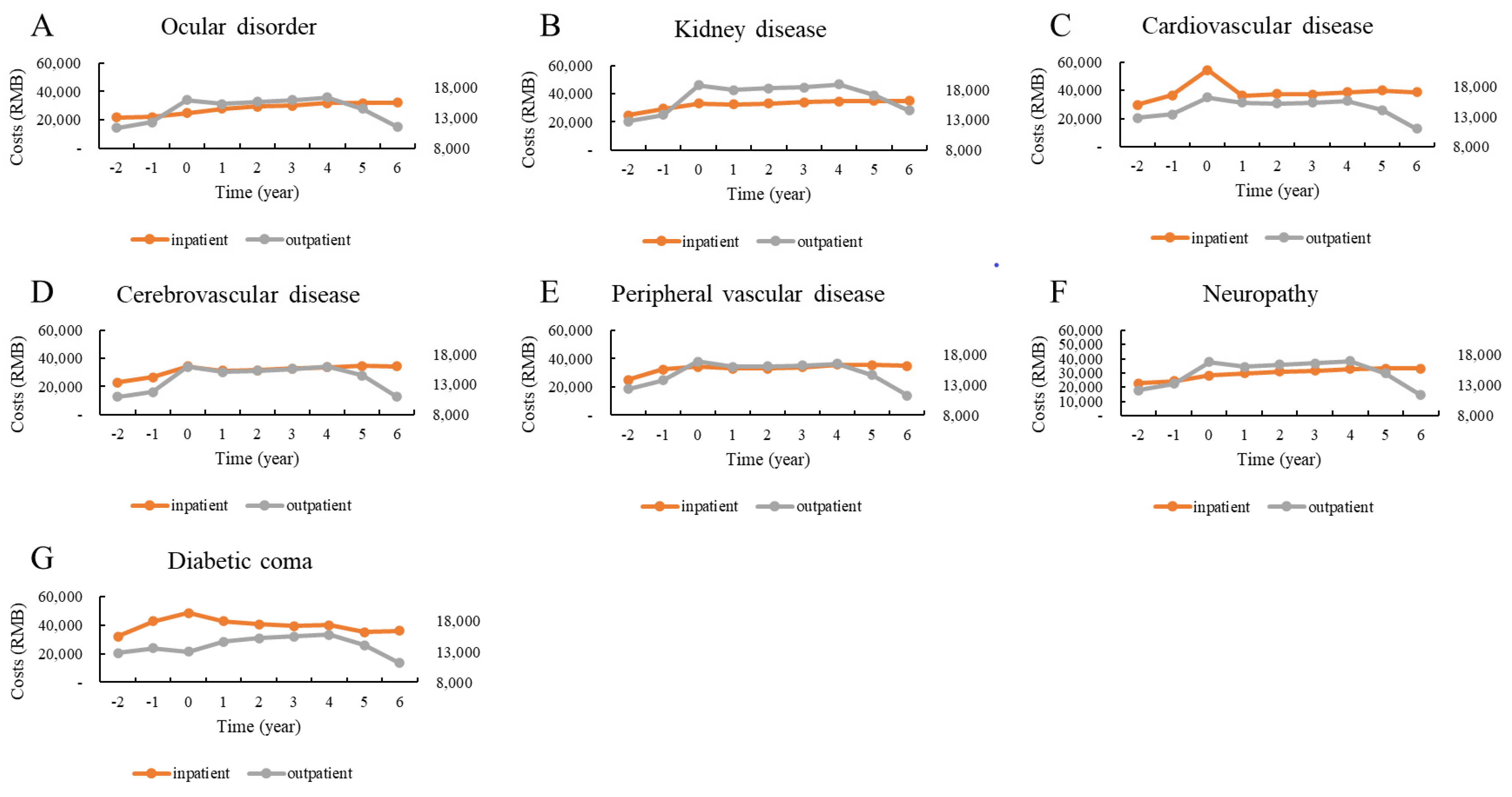
3.2. Descriptive Analysis
3.3. Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Misra, A.; Gopalan, H.; Jayawardena, R.; Hills, A.P.; Soares, M.; Reza-Albarrán, A.; Ramaiya, K.L. Diabetes in developing countries. J. Diabetes 2019, 11, 522–539. [Google Scholar] [CrossRef]
- Misra, A.; Sattar, N.; Tandon, N.; Shrivastava, U.; Hills, A.P. Clinical management of type 2 diabetes in south Asia. Lancet Diabetes Endocrinol. 2018, 6, 979–991. [Google Scholar] [CrossRef]
- Unnikrishnan, R.; Anjana, R.M.; Mohan, V. Diabetes mellitus and its complications in India. Nat. Rev. Endocrinol. 2016, 12, 357–370. [Google Scholar] [CrossRef] [Green Version]
- Pham, H.T.K.; Kieu, T.T.M.; Duong, T.D.; van Nguyen, K.D.; Tran, N.Q.; Tran, T.H.; Ng, J.Y.S. Direct medical costs of diabetes and its complications in Vietnam: A national health insurance database study—ScienceDirect. Diabetes Res. Clin. Pract. 2020, 162, 108051. [Google Scholar] [CrossRef]
- Wang, L.; Gao, P.; Zhang, M.; Huang, Z.; Zhang, D.; Deng, Q.; Li, Y.; Zhao, Z.; Qin, X.; Jin, D.; et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. Jama 2017, 317, 2515–2523. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.; Yang, C.; Fang, K.; Shi, M.; Yu, G.; Hu, Y. Hospitalization costs and complications in hospitalized patients with type 2 diabetes mellitus in Beijing, China. J. Diabetes 2017, 9, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Shuai, L.; Tan, X.; Zhao, Q. Assessment of hospital length of stay and direct costs of type 2 diabetes in Hubei Province, China. BMC Health Serv. Res. 2017, 17, 199. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Chen, B.; Shah, N.; Wang, Z.; Eggleston, K. Socioeconomic correlates of inpatient spending for patients with type 2 diabetes mellitus in China: Evidence from Hangzhou. Exp. Clin. Endocrinol. Diabetes 2012, 120, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Clarke, P.M.; Gray, A.M.; Briggs, A.; Farmer, A.J.; Fenn, P.; Stevens, R.J.; Matthews, D.R.; Stratton, I.M.; Holman, R.R. A model to estimate the lifetime health outcomes of patients with type 2 diabetes: The United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 2004, 47, 1747–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC Diabetes Cost-effectiveness Group. Cost-effectiveness of intensive glycemic control, intensified hypertension control, and serum cholesterol level reduction for type 2 diabetes. Jama 2002, 287, 2542–2551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahm, K.; Laxy, M.; Schneider, U.; Rogowski, W.H.; Lhachimi, S.K.; Holle, R. Health care costs associated with incident complications in patients With Type 2 diabetes in Germany. Diabetes Care 2018, 41, 971–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Fu, C.W.; Pan, C.Y.; Chen, W.; Zhan, S.; Luan, R.; Tan, A.; Liu, Z.; Xu, B. How do Type 2 diabetes mellitus-related chronic complications impact direct medical cost in four major cities of urban China? Value Health 2009, 12, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Liu, H.; Wu, Y.; Si, Y.; Song, J.; Cao, Y.; Li, M.; Wu, Y.; Wang, X.; Chen, L.; et al. Association between ambient fine particulate pollution and hospital admissions for cause specific cardiovascular disease: Time series study in 184 major Chinese cities. BMJ 2019, 367, I6572. [Google Scholar] [CrossRef] [Green Version]
- Swart, E.; Gothe, H.; Geyer, S.; Jaunzeme, J.; Maier, B.; Grobe, T.G.; Ihle, P. Good Practice of Secondary Data Analysis (GPS): Guidelines and recommendations. Gesundh. (Bundesverb. Arzte Offentlichen Gesundh. (Ger.)) 2015, 77, 120–126. [Google Scholar] [CrossRef]
- Alva, M.L.; Gray, A.; Mihaylova, B.; Leal, J.; Holman, R.R. The impact of diabetes-related complications on healthcare costs: New results from the UKPDS (UKPDS 84). Diabetic Med. 2015, 32, 459–466. [Google Scholar] [CrossRef]
- Nixon, R.M.; Thompson, S.G. Parametric modelling of cost data in medical studies. Stats Med. 2004, 23, 1311–1331. [Google Scholar] [CrossRef]
- Mihaylova, B.; Briggs, A.; O’Hagan, A.; Thompson, S.G. Review of statistical methods for analysing healthcare resources and costs. Health Econ. 2011, 20, 897–916. [Google Scholar] [CrossRef]
- Wu, H.; Eggleston, K.N.; Zhong, J.; Hu, R.; Wang, C.; Xie, K.; Chen, Y.; Chen, X.; Yu, M. How do type 2 diabetes mellitus (T2DM)-related complications and socioeconomic factors impact direct medical costs? A cross-sectional study in rural Southeast China. BMJ Open 2018, 8, e020647. [Google Scholar] [CrossRef]
- Caro, J.J.; Ward, A.J.; O’Brien, J.A. Lifetime costs of complications resulting from type 2 diabetes in the U.S. Diabetes Care 2002, 25, 476–481. [Google Scholar] [CrossRef] [Green Version]
- Cavan, D.; Makaroff, L.E.; Da, R.; Karuranga, S.; Sylvanowicz, M.; Conlon, J.; Chaney, D.; Malhi, A.; Barratt, J. Global perspectives on the provision of diabetic retinopathy screening and treatment: Survey of health care professionals in 41 countries. Diabetes Res. Clin. Pract. 2018, 143, 170–178. [Google Scholar] [CrossRef]
- Wong, T.Y.; Sun, J.; Kawasaki, R.; Ruamviboonsuk, P.; Gupta, N.; Lansingh, V.C.; Maia, M.; Mathenge, W.; Moreker, S.; Muqit, M.M.K.; et al. Guidelines on diabetic eye care: The international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology 2018, 125, 1608–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regitz-Zagrosek, V. Sex and gender differences in health. Science & Society Series on Sex and Science. EMBO Rep. 2012, 13, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaberg, M.L.; Burch, D.M.; Hud, Z.R.; Zacharias, M.P. Gender differences in the onset of diabetic neuropathy. J. Diabetes Complicat. 2008, 22, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Peek, M.E. Gender differences in diabetes-related lower extremity amputations. Clin. Orthop. Relat. Res. 2011, 469, 1951–1955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.B.; Pedula, K.L.; Bakst, A.W. The progressive cost of complications in Type 2 diabetes mellitus. Arch. Intern. Med. 1999, 159, 1873–1880. [Google Scholar] [CrossRef]
- Cannon, A.; Handelsman, Y.; Heile, M.; Shannon, M. Burden of illness in Type 2 diabetes mellitus. J. Manag. Care Spec. Pharm. 2018, 24, S5–S13. [Google Scholar] [CrossRef]
- Fisher, K.; Griffith, L.; Gruneir, A.; Panjwani, D.; Gandhi, S.; Sheng, L.; Gafni, A.; Chris, P.; Markle-Reid, M.; Ploeg, J. Comorbidity and its relationship with health service use and cost in community-living older adults with diabetes: A population-based study in Ontario, Canada. Diabetes Res. Clin. Pract. 2016, 122, 113–123. [Google Scholar] [CrossRef]
- Rodríguez-Sánchez, B.; Angelini, V.; Feenstra, T.; Alessie, R. Diabetes-Associated factors as predictors of nursing home admission and costs in the elderly across Europe. J. Am. Med. Dir. Assoc. 2017, 18, 74–82. [Google Scholar] [CrossRef]
- Basaraba, J.E.; Picard, M.; George-Phillips, K.; Mysak, T. Pharmacists as care providers for stroke patients: A systematic review. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2018, 45, 49–55. [Google Scholar] [CrossRef]
- Tran, D.T.; Welsh, R.C.; Ohinmaa, A.; Thanh, N.X.; Kaul, P. Resource use and burden of hospitalization, outpatient, physician, and drug costs in short- and long-term care after acute myocardial infarction. Can. J. Cardiol. 2018, 34, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Xie, P. Outpatient workload in China. Lancet 2013, 381, 1983–1984. [Google Scholar] [CrossRef]
- Xu, X.; Li, B.; Huang, H. Air pollution and unscheduled hospital outpatient and emergency room visits. Environ. Health Perspect. 1995, 103, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Layden, J.; Michaels, J.; Bermingham, S.; Higgins, B. Diagnosis and management of lower limb peripheral arterial disease: Summary of NICE guidance. BMJ 2012, 345, e4947. [Google Scholar] [CrossRef] [Green Version]
- Rhee, S.Y.; Kim, Y.S.J.D.; Journal, M. Peripheral arterial disease in patients with Type 2 diabetes mellitus. Diabetes Metab. J. 2015, 39, 283–290. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | Female | Male |
|---|---|---|---|
| (n = 1,859,039) | (n = 985,797) | (n = 873,242) | |
| Sex (%) | 53.03 | 46.97 | |
| Age, years, mean | 65.01 | 64.40 | 65.70 |
| Age group, number (%) | |||
| ≤44 | 79,407 (4.27) | 36,606 (3.71) | 42,801 (4.90) |
| 45–54 | 335,158 (18.03) | 197,010 (19.98) | 138,148 (15.82) |
| 55–64 | 568,559 (30.58) | 313,664 (31.82) | 254,895 (29.19) |
| 65–74 | 510,500 (27.46) | 258,333 (26.21) | 252,167 (28.88) |
| ≥75 | 365,415 (19.66) | 180,184 (18.28) | 185,231 (21.21) |
| Number of complications | |||
| 1 | 762,130 (41.00) | 385,273 (39.08) | 376,857 (43.16) |
| 2 | 561,424 (30.20) | 305,143 (30.95) | 256,281 (29.35) |
| 3 | 327,087 (17.59) | 180,665 (18.33) | 146,422 (16.77) |
| ≥4 | 208,398 (11.21) | 114,716 (11.64) | 93,682 (10.73) |
| Variables | No. (%) |
|---|---|
| Type of complications | |
| Cardiovascular disease | 738,589 (39.73) |
| Cerebrovascular disease | 571,915 (30.76) |
| Kidney disease | 345,728 (18.60) |
| Eye disorder | 230,866 (12.42) |
| Neuropathy | 191,710 (10.31) |
| Peripheral vascular disease | 186,780 (10.05) |
| Diabetic coma | 9221 (0.50) |
| Variable | Coefficient Estimate (Standard Error) | |
| Sex: female (Ref: male) | −2236.33 *** (28.66) | |
| Age group (Ref: ≤44 years), years | ||
| 45–54 | 2173.74 *** (56.14) | |
| 55–64 | 3715.05 *** (54.52) | |
| 65–74 | 5582.47 *** (58.31) | |
| ≥75 | 6333.84 *** (59.20) | |
| Coefficient Estimate (Standard Error) | ||
| Event/condition (Ref: n) | <1 year after the event | >1 year after the event |
| Neuropathy | −16.14 (115.09) | 883.90 *** (91.01) |
| Ocular disorders | −503.66 *** (106.65) | 1423.16 *** (93.39) |
| Kidney disease | 304.14 ** (108.43) | 624.00 *** (83.08) |
| Cardiovascular disease | 10,631.16 *** (125.74) | 1150.71 *** (86.10) |
| Peripheral vascular disease | −748.48 *** (129.33) | −1033.74 *** (114.89) |
| Cerebrovascular disease | 1017.62 ** (74.56) | 653.82 *** (70.28) |
| Diabetic coma | 3135.64 *** (492.21) | −1031.60 ** (436.63) |
| Variable | Coefficient Estimate (Standard Error) | |
| Sex: female (Ref: male) | −29.78 *** (0.39) | |
| Age group (Ref: ≤44 years), years | ||
| 45–54 | 46.02 *** (0.80) | |
| 55–64 | 57.73 *** (0.80) | |
| 65–74 | 75.86 *** (0.85) | |
| ≥75 | 73.24 *** (0.88) | |
| Coefficient Estimate (Standard Error) | ||
| Event/condition (Ref: n) | <1 year after the event | >1 year after the event |
| Neuropathy | −6.28 *** (0.64) | 51.89 *** (0.76) |
| Ocular disorders | −11.70 *** (2.30) | 89.07 *** (3.31) |
| Kidney disease | −23.53 *** (0.76) | 52.18 *** (0.97) |
| Cardiovascular disease | −3.34 ** (1.20) | 29.79 *** (1.51) |
| Peripheral vascular disease | −14.07 *** (0.77) | 27.02 *** (0.90) |
| Cerebrovascular disease | −11.28 ** (0.40) | 31.84 *** (0.48) |
| Diabetic coma | −30.39 *** (4.36) | 25.54 *** (5.59) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, J.-H.; Wu, Y.; Wang, Z.-J.; Wu, Y.-Q.; Wu, T.; Wang, M.-Y.; Wang, X.-W.; Wang, S.-Y.; Wang, J.-T.; Yu, H.; et al. Healthcare Costs Associated with Complications in Patients with Type 2 Diabetes among 1.85 Million Adults in Beijing, China. Int. J. Environ. Res. Public Health 2021, 18, 3693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073693
Wu J-H, Wu Y, Wang Z-J, Wu Y-Q, Wu T, Wang M-Y, Wang X-W, Wang S-Y, Wang J-T, Yu H, et al. Healthcare Costs Associated with Complications in Patients with Type 2 Diabetes among 1.85 Million Adults in Beijing, China. International Journal of Environmental Research and Public Health. 2021; 18(7):3693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073693
Chicago/Turabian StyleWu, Jun-Hui, Yao Wu, Zi-Jing Wang, Yi-Qun Wu, Tao Wu, Meng-Ying Wang, Xiao-Wen Wang, Si-Yue Wang, Jia-Ting Wang, Huan Yu, and et al. 2021. "Healthcare Costs Associated with Complications in Patients with Type 2 Diabetes among 1.85 Million Adults in Beijing, China" International Journal of Environmental Research and Public Health 18, no. 7: 3693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073693