
Sex and Limb Differences in Lower Extremity Alignment and Kinematics during Drop Vertical Jumps


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anthropometric Measurements
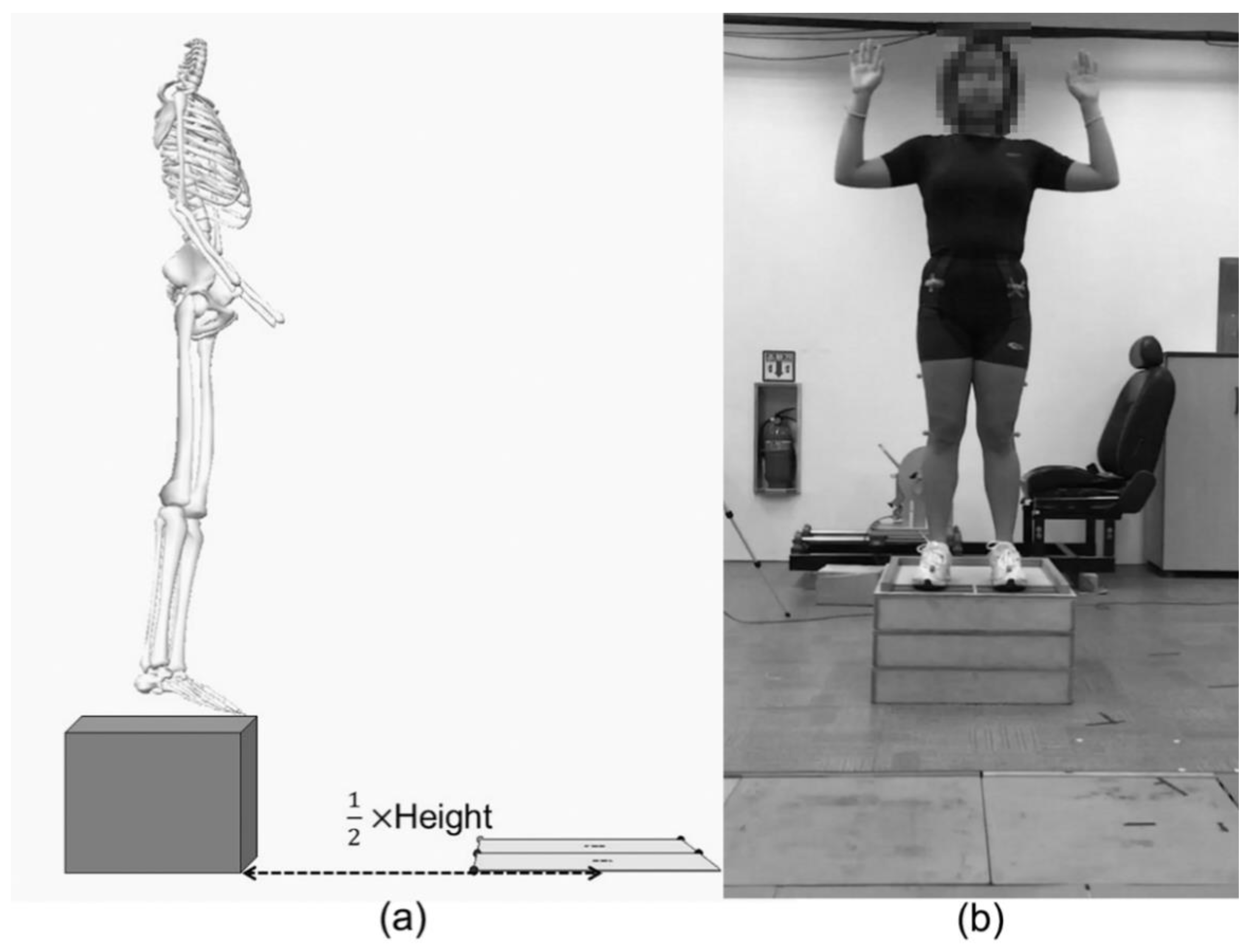
2.3. Dynamic Measurements
2.4. Statistical Analysis
3. Results
3.1. Anthropometric Measurements
3.2. Dynamic Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hootman, J.M.; Dick, R.; Agel, J. Epidemiology of collegiate injuries for 15 sports: Summary and recommendations for injury prevention initiatives. J. Athl. Train. 2007, 42, 311–319. [Google Scholar] [PubMed]
- Messina, D.F.; Farney, W.C.; DeLee, J.C. The Incidence of Injury in Texas High School Basketball. Am. J. Sports Med. 1999, 27, 294–299. [Google Scholar] [CrossRef]
- Arendt, E.; Dick, R. Knee Injury Patterns Among Men and Women in Collegiate Basketball and Soccer. Am. J. Sports Med. 1995, 23, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Waldén, M.; Hägglund, M.; Werner, J.; Ekstrand, J. The epidemiology of anterior cruciate ligament injury in football (soccer): A review of the literature from a gender-related perspective. Knee Surg. Sport. Traumatol. Arthrosc. 2011, 19, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Sigward, S.M.; Cesar, G.M.; Havens, K.L. Predictors of Frontal Plane Knee Moments During Side-Step Cutting to 45 and 110 Degrees in Men and Women. Clin. J. Sport Med. 2015, 25, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agel, J.; Arendt, E.A.; Bershadsky, B. Anterior Cruciate Ligament Injury in National Collegiate Athletic Association Basketball and Soccer: A 13-Year Review. Am. J. Sports Med. 2005, 33, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Medina McKeon, J.M.; Hertel, J. Sex Differences and Representative Values for 6 Lower Extremity Alignment Measures. J. Athl. Train. 2009, 44, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.-D.; Shultz, S.J. Sex Differences in Clinical Measures of Lower Extremity Alignment. J. Orthop. Sport. Phys. Ther. 2007, 37, 389–398. [Google Scholar] [CrossRef]
- Decker, M.J.; Torry, M.R.; Wyland, D.J.; Sterett, W.I.; Richard Steadman, J. Gender differences in lower extremity kinematics, kinetics and energy absorption during landing. Clin. Biomech. 2003, 18, 662–669. [Google Scholar] [CrossRef]
- Nguyen, A.-D.; Shultz, S.J.; Schmitz, R.J. Landing Biomechanics in Participants With Different Static Lower Extremity Alignment Profiles. J. Athl. Train. 2015, 50, 498–507. [Google Scholar] [CrossRef] [Green Version]
- Kernozek, T.W.; Torry, M.R.; VAN Hoof, H.; Cowley, H.; Tanner, S. Gender differences in frontal and sagittal plane biomechanics during drop landings. Med. Sci. Sports Exerc. 2005, 37, 1003–1012, discussion 1013. [Google Scholar] [PubMed]
- Norcross, M.F.; Shultz, S.J.; Weinhold, P.S.; Lewek, M.D.; Padua, D.A.; Blackburn, J.T. The influences of sex and posture on joint energetics during drop landings. Scand. J. Med. Sci. Sports 2015, 25, e166–e175. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.P.; Sizer, P.S.; James, C.R. Effects of fatigue on frontal plane knee motion, muscle activity, and ground reaction forces in men and women during landing. J. Sports Sci. Med. 2009, 8, 419–427. [Google Scholar] [PubMed]
- Gehring, D.; Melnyk, M.; Gollhofer, A. Gender and fatigue have influence on knee joint control strategies during landing. Clin. Biomech. 2009, 24, 82–87. [Google Scholar] [CrossRef]
- McLean, S.G.; Felin, R.E.; Suedekum, N.; Calabrese, G.; Passerallo, A.; Joy, S. Impact of Fatigue on Gender-Based High-Risk Landing Strategies. Med. Sci. Sport. Exerc. 2007, 39, 502–514. [Google Scholar] [CrossRef]
- Cortes, N.; Onate, J.; Abrantes, J.; Gagen, L.; Dowling, E.; Van Lunen, B. Effects of gender and foot-landing techniques on lower extremity kinematics during drop-jump landings. J. Appl. Biomech. 2007, 23, 289–299. [Google Scholar] [CrossRef]
- Bruton, M.R.; Adams, R.D.; O’Dwyer, N.J. Sex Differences in Drop Landing. Percept. Mot. Skills 2017, 124, 992–1008. [Google Scholar] [CrossRef]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G.; Crosby, R.W.; Andrews, P.J.; Krause, C. Muscles, Testing and Function: With Posture and Pain, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1993; ISBN 0683045768. [Google Scholar]
- Heiderscheit, B.C.; Hamill, J.; Caldwell, G.E. Influence of Q-angle on Lower-Extremity Running Kinematics. J. Orthop. Sport. Phys. Ther. 2000, 30, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Pantano, K.J.; White, S.C.; Gilchrist, L.A.; Leddy, J. Differences in peak knee valgus angles between individuals with high and low Q-angles during a single limb squat. Clin. Biomech. 2005, 20, 966–972. [Google Scholar] [CrossRef]
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebretsen, L.; Bahr, R.; Krosshaug, T. Mechanisms for Noncontact Anterior Cruciate Ligament Injuries. Am. J. Sports Med. 2010, 38, 2218–2225. [Google Scholar] [CrossRef]
- Brophy, R.; Silvers, H.J.; Gonzales, T.; Mandelbaum, B.R. Gender influences: The role of leg dominance in ACL injury among soccer players. Br. J. Sports Med. 2010, 44, 694–697. [Google Scholar] [CrossRef]
- Brown, T.N.; Palmieri-Smith, R.M.; McLean, S.G. Sex and limb differences in hip and knee kinematics and kinetics during anticipated and unanticipated jump landings: Implications for anterior cruciate ligament injury. Br. J. Sports Med. 2009, 43, 1049–1056. [Google Scholar] [CrossRef]
- Pollard, C.D.; Norcross, M.F.; Johnson, S.T.; Stone, A.E.; Chang, E.; Hoffman, M.A. A biomechanical comparison of dominant and non-dominant limbs during a side-step cutting task. Sport. Biomech. 2018, 1–9. [Google Scholar] [CrossRef]
- Ford, K.R.; Myer, G.D.; Hewett, T.E. Valgus knee motion during landing in high school female and male basketball players. Med. Sci. Sport. Exerc. 2003, 35, 1745–1750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magee, D.J. Orthopedic Physical Assessment, 6th ed.; Elsevier Saunders: St. Louis, MO, USA, 2014; ISBN 978-1-4557-0977-9. [Google Scholar]
- Livingston, L.A.; Mandigo, J.L. Bilateral within-subject Q angle asymmetry in young adult females and males. Biomed. Sci. Instrum. 1997, 33, 112–117. [Google Scholar]
- Stuberg, W.; Temme, J.; Kaplan, P.; Clarke, A.; Fuchs, R. Measurement of tibial torsion and thigh-foot angle using goniometry and computed tomography. Clin. Orthop. Relat. Res. 1991, 272, 208–212. [Google Scholar] [CrossRef]
- Elliott, A.; Woodward, W. Statistical Analysis Quick Reference Guidebook: With SPSS Examples; Sage: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Alviso, D.J.; Dong, G.T.; Lentell, G.L. Intertester Reliability for Measuring Pelvic Tilt in Standing. Phys. Ther. 1988, 68, 1347–1351. [Google Scholar] [CrossRef] [PubMed]
- Day, J.W.; Smidt, G.L.; Lehmann, T. Effect of Pelvic Tilt on Standing Posture. Phys. Ther. 1984, 64, 510–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajdosik, R.; Simpson, R.; Smith, R.; DonTigny, R.L. Pelvic Tilt. Phys. Ther. 1985, 65, 169–174. [Google Scholar] [CrossRef]
- Gilliam, J.; Brunt, D.; MacMillan, M.; Kinard, R.E.; Montgomery, W.J. Relationship of the Pelvic Angle to the Sacral Angle: Measurement of Clinical Reliability and Validity. J. Orthop. Sport. Phys. Ther. 1994, 20, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Endo, K.; Suzuki, H.; Nishimura, H.; Tanaka, H.; Shishido, T.; Yamamoto, K. Sagittal lumbar and pelvic alignment in the standing and sitting positions. J. Orthop. Sci. 2012, 17, 682–686. [Google Scholar] [CrossRef]
- Bråten, M.; Terjesen, T.; Rossvoll, I. Femoral anteversion in normal adults. Acta Orthop. Scand. 1992, 63, 29–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laible, C.; Sherman, O.H. Risk factors and prevention strategies of non-contact anterior cruciate ligament injuries. Bull. Hosp. Jt. Dis. 2014, 72, 70–75. [Google Scholar]
- Hsu, R.W.; Himeno, S.; Coventry, M.B.; Chao, E.Y. Normal axial alignment of the lower extremity and load-bearing distribution at the knee. Clin. Orthop. Relat. Res. 1990, 255, 215–227. [Google Scholar] [CrossRef]
- Woodland, L.H.; Francis, R.S. Parameters and comparisons of the quadriceps angle of college-aged men and women in the supine and standing positions. Am. J. Sports Med. 1992, 20, 208–211. [Google Scholar] [CrossRef]
- Moul, J.L. Differences in Selected Predictors of Anterior Cruciate Ligament Tears Between Male and Female NCAA Division I Collegiate Basketball Players. J. Athl. Train. 1998, 33, 118–121. [Google Scholar]
- Tillman, M.D.; Bauer, J.A.; Cauraugh, J.H.; Trimble, M.H. Differences in lower extremity alignment between males and females. Potential predisposing factors for knee injury. J. Sports Med. Phys. Fitness 2005, 45, 355–359. [Google Scholar]
- Hvid, I.; Andersen, L.I.; Schmidt, H. Chondromalacia Patellae: The Relation to Abnormal Patellofemoral Joint Mechanics. Acta Orthop. Scand. 1981, 52, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Omololu, B.B.; Ogunlade, O.S.; Gopaldasani, V.K. Normal Q-angle in an Adult Nigerian Population. Clin. Orthop. Relat. Res. 2009, 467, 2073–2076. [Google Scholar] [CrossRef] [Green Version]
- Shultz, S.J.; Nguyen, A.-D. Bilateral Asymmetries in Clinical Measures of Lower-Extremity Anatomic Characteristics. Clin. J. Sport Med. 2007, 17, 357–361. [Google Scholar] [CrossRef]
- Tamari, K.; Tinley, P.; Briffa, K.; Aoyagi, K. Ethnic-, gender-, and age-related differences in femorotibial angle, femoral antetorsion, and tibiofibular torsion: Cross-sectional study among healthy Japanese and Australian Caucasians. Clin. Anat. 2005, 19, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, L.P.; Gunderson, R.B.; Steen, H.; Reikerås, O. The normal development of tibial torsion. Skelet. Radiol. 2001, 30, 519–522. [Google Scholar] [CrossRef]
- Pandy, M.G.; Shelburne, K.B. Dependence of cruciate-ligament loading on muscle forces and external load. J. Biomech. 1997, 30, 1015–1024. [Google Scholar] [CrossRef]
- Nagano, Y.; Ida, H.; Akai, M.; Fukubayashi, T. Gender differences in knee kinematics and muscle activity during single limb drop landing. Knee 2007, 14, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Hvid, I.; Andersen, L.I. The Quadriceps Angle and its Relation to Femoral Torsion. Acta Orthop. Scand. 1982, 53, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-C.; Lai, W.-H.; Shih, Y.-F.; Chang, C.-M.; Lo, C.-Y.; Hsu, H.-C. Physiological anterior laxity in healthy young females: The effect of knee hyperextension and dominance. Knee Surg. Sport. Traumatol. Arthrosc. 2009, 17, 1083–1088. [Google Scholar] [CrossRef]
- Shultz, S.J.; Nguyen, A.-D.; Levine, B.J. The Relationship Between Lower Extremity Alignment Characteristics and Anterior Knee Joint Laxity. Sport. Heal. A Multidiscip. Approach 2009, 1, 54–60. [Google Scholar] [CrossRef]
- Mondal, S.; Chhangte, Z.; Gayen, A.; Chatterjee, S. Dominant and Non-Dominant Leg Muscle Electrical Activity Of Soccer Players: A Preliminary Study. Int. Ref. J. Eng. Sci. 2014, 3, 65–69. [Google Scholar]
- Ball, N.B.; Stock, C.G.; Scurr, J.C. Bilateral Contact Ground Reaction Forces and Contact Times During Plyometric Drop Jumping. J. Strength Cond. Res. 2010, 24, 2762–2769. [Google Scholar] [CrossRef]
- Reinschmidt, C.; van den Bogert, A.J.; Nigg, B.M.; Lundberg, A.; Murphy, N. Effect of skin movement on the analysis of skeletal knee joint motion during running. J. Biomech. 1997, 30, 729–732. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement | ICC | SEM |
|---|---|---|
| Pelvic tilt | 0.88 | 1.35 |
| Femoral anteversion | 0.94 | 0.91 |
| Q-angle | 0.93 | 0.94 |
| Genu recurvatum | 0.90 | 1.09 |
| Tibial torsion | 0.93 | 1.97 |
| Navicular drop | 0.95 | 0.53 |
| Male | Female | |||
|---|---|---|---|---|
| Dominant | Non-Dominant | Dominant | Non-Dominant | |
| Pelvic tilt * | 8.6 (3.3) | 9.0 (3.9) | 10.8 (3.5) | 10.8 (3.7) |
| Femoral anteversion * | 7.1 (6.9) | 7.7 (6.1) | 10.1 (6.3) | 9.6 (6.7) |
| Q-angle * | 14.6 (4.7) | 14.1 (4.7) | 21.8 (5.4) | 21.4 (4.7) |
| Genu recurvatum † | 2.1 (4.1) | 1.3 (3.9) | 3.1 (2.9) | 2.3 (3.3) |
| Tibial torsion * | 20.0 (7.4) | 20.1 (6.3) | 16.6 (6.2) | 17.2 (5.7) |
| Navicular drop | 7.9 (3.8) | 8.4 (4.0) | 7.5 (3.8) | 8.0 (3.4) |
| Male | Female | |||
|---|---|---|---|---|
| Dominant | Non-Dominant | Dominant | Non-Dominant | |
| Hip flexion/extension † | 36.3 (7.3) | 37.0 (8.5) | 37.1 (5.8) | 38.7 (5.2) |
| Hip adduction/abduction *† | −10.8 (3.9) | −13.0 (4.1) | −7.6 (3.7) | −10.9 (3.9) |
| Hip internal/external rotation † | −6.2 (9.8) | −8.9 (11.4) | −6.1 (10.4) | −9.8 (10.2) |
| Knee flexion/extension *† | 25.3 (7.1) | 27.1 (7.6) | 20.7 (5.9) | 23.9 (6.0) |
| Knee adduction /abduction * | 4.9 (4.6) | 4.6 (4.6) | 1.7 (4.3) | 0.5 (5.1) |
| Knee internal/external rotation † | 4.4 (9.4) | 6.5 (9.0) | 1.1 (8.1) | 7.1 (8.5) |
| Ankle dorsiflexion/plantarflexion * | −10.6 (11.6) | −11.0 (10.6) | −16.8 (10.9) | −14.8 (11.3) |
| Ankle inversion/eversion † | −3.5 (8.7) | −0.1 (8.9) | 0.6 (8.4) | 1.3 (8.6) |
| Ankle internal/external rotation * | 0.3 (1.9) | 0.1 (2.0) | −0.7 (2.0) | −0.6 (1.8) |
| Male | Female | |||
|---|---|---|---|---|
| Dominant | Non-Dominant | Dominant | Non-Dominant | |
| Hip flexion † | 75.5 (15.1) | 79.9 (12.1) | 78.6 (15.3) | 81.6 (11.6) |
| Hip adduction *,†,§ | −6.8 (4.7) | −9.7 (3.9) | −3.1 (4.1) | −5.9 (4.3) |
| Hip internal rotation | 6.1 (10.2) | 4.9 (12.5) | 5.9 (9.6) | 2.5 (10.5) |
| Knee flexion † | 100.4 (15.7) | 101.7 (15.7) | 97.8 (12.9) | 100.3 (14.7) |
| Knee abduction *,†,§ | −2.3 (7.9) | −5.4 (9.0) | −9.8 (9.0) | −14.9 (11.6) |
| Knee internal rotation *,† | 23.9 (9.9) | 27.4 (9.6) | 18.7 (9.3) | 24.4 (9.6) |
| Ankle dorsiflexion ‡ | 34.2 (5.0) | 33.7 (5.0) | 34.3 (4.5) | 35.7 (6.1) |
| Ankle eversion *,§ | −1.1 (1.9) | −1.5 (1.8) | −2.0 (2.0) | −1.9 (1.9) |
| Ankle external rotation ‡,§ | −25.4 (7.9) | −23.0 (6.1) | −24.2 (7.7) | −26.0 (6.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chun, Y.; Bailey, J.P.; Kim, J.; Lee, S.-C.; Lee, S.Y. Sex and Limb Differences in Lower Extremity Alignment and Kinematics during Drop Vertical Jumps. Int. J. Environ. Res. Public Health 2021, 18, 3748. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073748
Chun Y, Bailey JP, Kim J, Lee S-C, Lee SY. Sex and Limb Differences in Lower Extremity Alignment and Kinematics during Drop Vertical Jumps. International Journal of Environmental Research and Public Health. 2021; 18(7):3748. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073748
Chicago/Turabian StyleChun, Youngmin, Joshua P. Bailey, Jinah Kim, Sung-Cheol Lee, and Sae Yong Lee. 2021. "Sex and Limb Differences in Lower Extremity Alignment and Kinematics during Drop Vertical Jumps" International Journal of Environmental Research and Public Health 18, no. 7: 3748. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073748