
Barriers and Facilitators for Exclusive Breastfeeding in Women’s Biopsychosocial Spheres According to Primary Care Midwives in Tenerife (Canary Islands, Spain)

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Ethical Considerations
2.4. Analysis
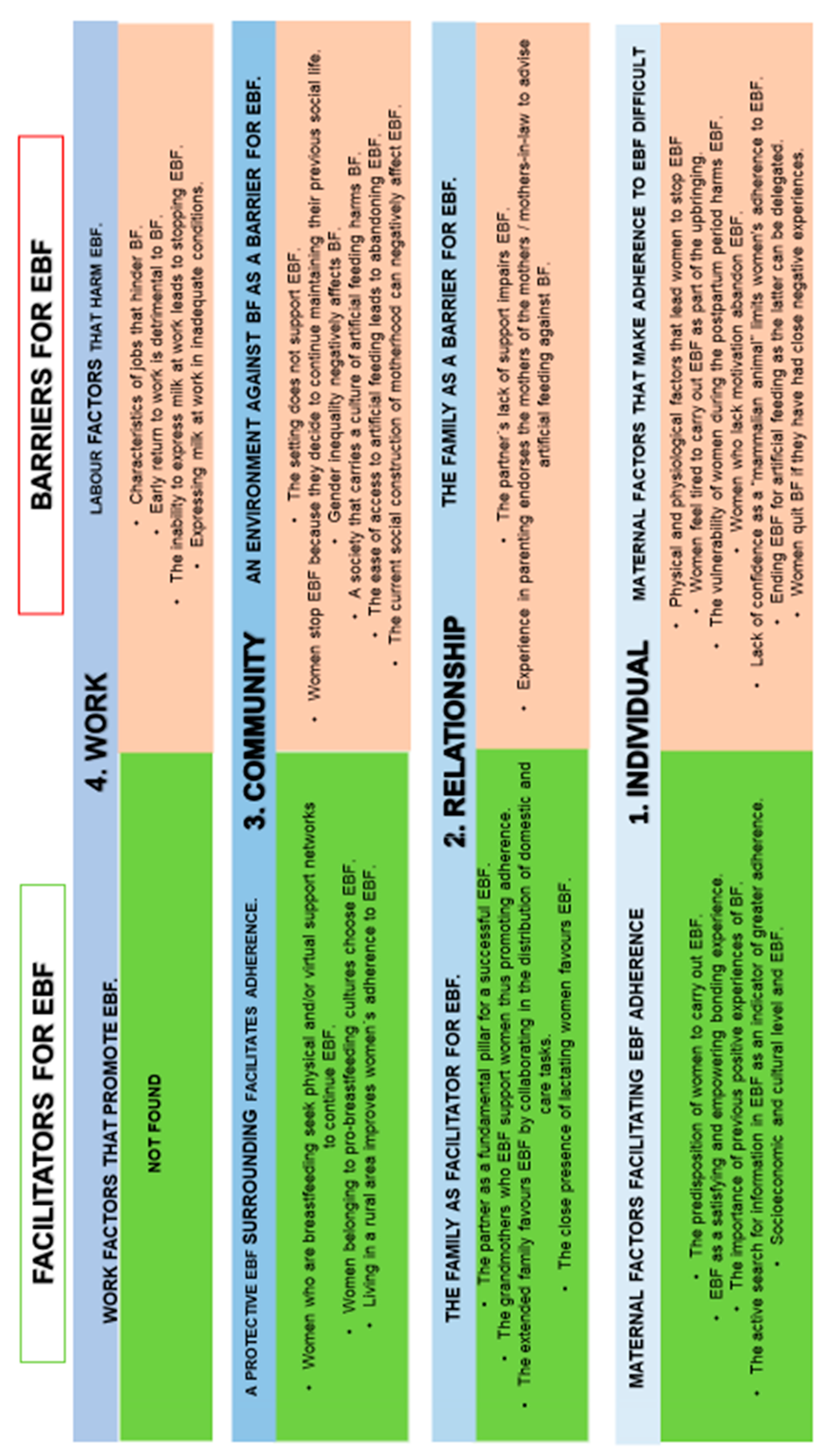
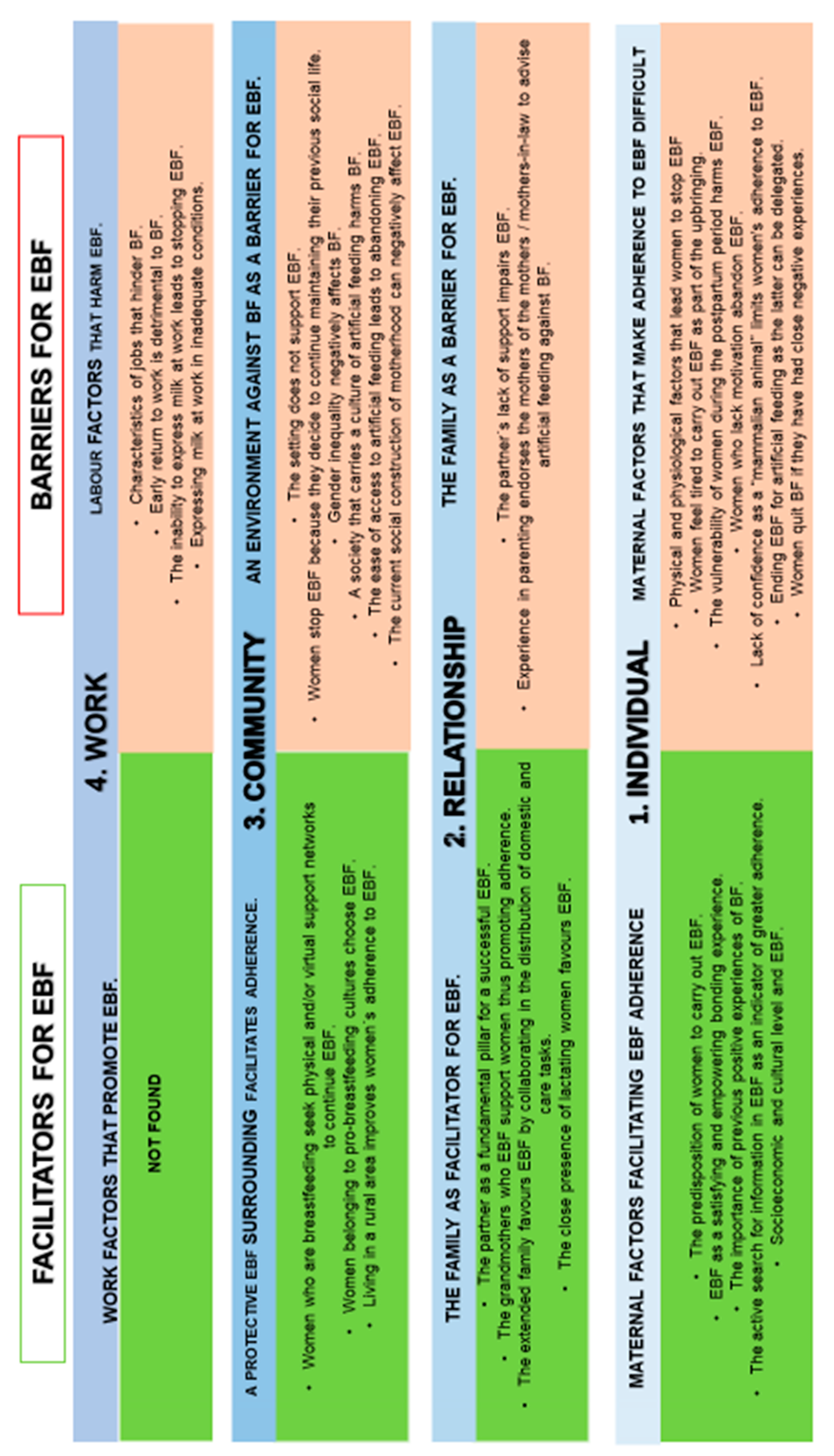
3. Results
3.1. Individual Level
3.1.1. Maternal Factors That Make Adherence to EBF Difficult
“... the first few days the problem they find the most is the latching on, which means they are already starting to have problems with cracks, a chain that can lead to significant suffering due to the pain.” (E7)
“...as a difficulty after tiredness, lack of sleep... this can be the cause of abandonment, or the lack of will to breastfeed...” (E4)
“...because postpartum is the most important period for EBF to be well established and when women are most vulnerable and need support...” (E9)
“... if the motivation is not very clear, if you are not sure, difficulties appear and you don′t try to solve them, because the logical thing is that you quit.” (E5)
“... We lack a lot of self-confidence, starting during pregnancy, to think that women have milk, they question whether they will have milk, and who doesn′t have milk? I think we have little instinct to follow the natural process...” (E8)
“...we live in a culture of social comfort, where you want things to be solved now and at this very moment, and of course breastfeeding is not from that comfort culture.” (E7)
“...there are women who may have had previous negative experiences or a friend of theirs had a horrible experience, so they are already going downhill and she says: no, I’m not going to nurse...” (E2)
3.1.2. Maternal Factors Facilitating EBF Adherence
“The motivation that each woman has to breastfeed and their conviction; that is the main positive factor for adherence to exclusive breastfeeding.” (E1)
“... the most important thing they say is that they know that breastfeeding is the best food there is, they are helping their defence system, and it is satisfying for them to be able to breastfeed their baby and also for the bond they have with the baby.” (E12)
“The first child opens the way and, more than anything, you already know how to solve difficulties and I believe that women are no longer so overwhelmed, since when the baby cries they simply put the baby to the breast without questioning themselves too much. They are more confident.” (E5)
“...the more information you have the more power you will have later, especially during labour, about your delivery and about your lactation, the more information the better...” (E14)
“…women who have a higher economic level, with a university degree, and have a job have more access to information, and they are better informed and perhaps they have more initiatives and more desire to breastfeed than others.” (E4)
3.2. Relationship Level
3.2.1. The Family as a Barrier for EBF
“... If you do not have the support of your partner and you have a person next to you who continues doing a bit their own thing, without getting involved, then even worse because you have to continue doing everything you did before plus breastfeeding…”(E14)
“…and particularly the lack of support by the mothers or mothers-in-law, who didn′t breastfeed their babies. It is what they did and what they recommend.” (E17)
3.2.2. The Family as Facilitator for EBF
“If your partner is your accomplice in that support, also as a caregiver of the baby, that influences you, it will help you in breastfeeding, because he helps you in sharing what parenting is. Mothers who have support from their partner, I think they achieve a more successful and longer lactation.” (E7)
“…When your mother, your grandmother and your great-grandmother have breastfed, it is very rare that you do not breastfeed because they will be on top of you. She feels she doesn′t want to be less than them, you know?” (E11)
“…The mother and the mother-in-law help in the postpartum providing their home-cooking in tuppers and taking care of the baby so that they can shower and stuff. The family is a very important positive factor for recovery and for maintaining lactation.” (E2)
“...it is important for breastfeeding to have someone who has breastfed in your close circle, they may be mothers, grandmothers or an important figure such as a sister...” (E1)
3.3. Community Level
3.3.1. An Environment against BF as a Barrier for EBF
“... if you want to breastfeed, but above all your environment is hindering you and they are continuously giving you a negative message, particularly at that very changing postpartum period, it is very easy to succumb.” (E14)
“Wanting to continue living the life you had before, the same trips, the same leisure, but breastfeeding puts a hold on this in many respects, because you can’t handle everything.” (E13)
“… It is still very damaging that we are still dealing with women who have suffered the pressure of not breastfeeding and using formula. We know the great pressure and the great business that existed at that time.” (E3)
3.3.2. A Protective EBF Surrounding Facilitates Adherence
“... There are many women who breastfeed and follow midwives who have webpages, or mothers who breastfeed a lot and a social network bond between these women, that perhaps didn′t exist in society, is formed.” (E8)
“... African or Arab women have very few breastfeeding problems, they have seen it with their sisters, or have several children and live in a community, they help each other.” (E9)
“...society in rural areas sees breastfeeding more normal and they do it naturally, different to what happens in city areas. In the villages they have more of a habit of breastfeeding.” (E14)
3.4. Work Level
3.4.1. Labour Factors That Harm BF
3.4.2. Work Factors That Promote EBF
4. Discussion
Limitations of Our Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
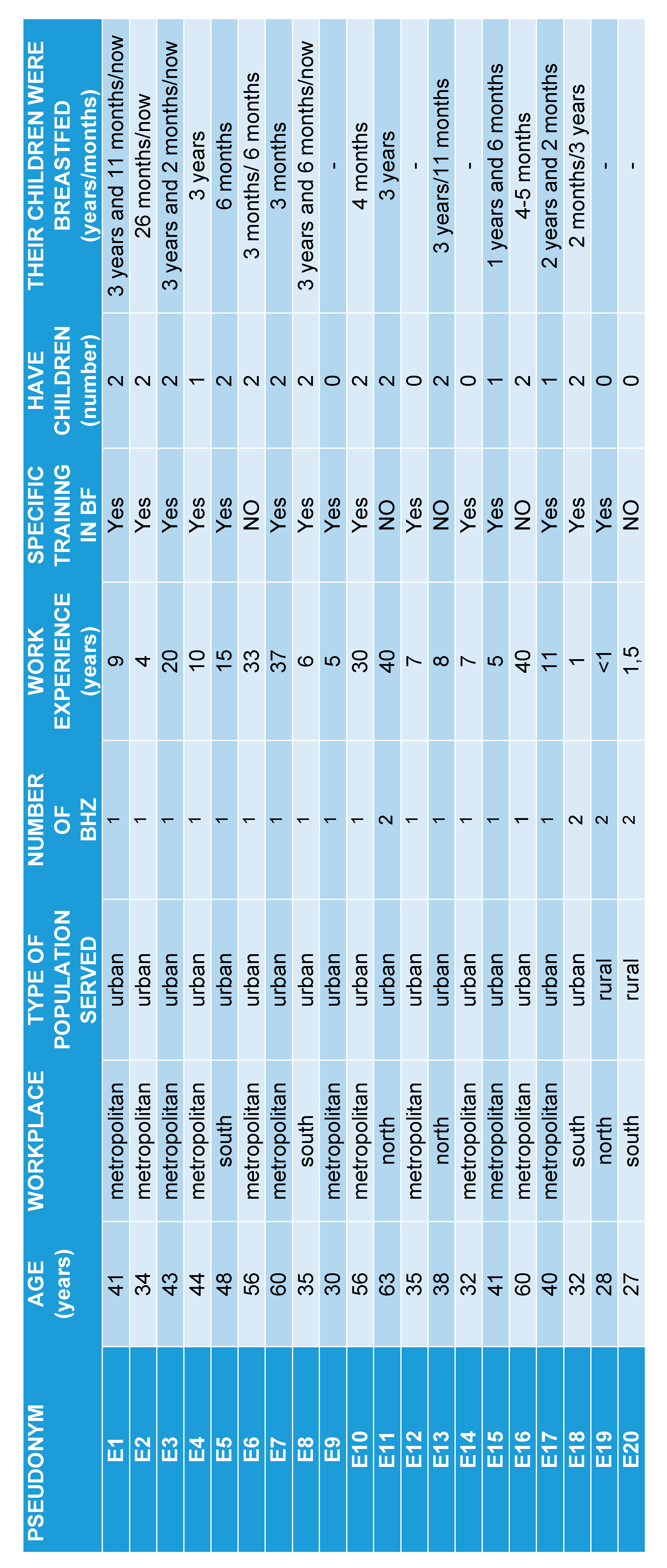
Appendix A. Profiles Primary Care Midwives

Appendix B. Interview Script for Midwives
- 1.
- Facilities for women to breastfeed.
- 2.
- Barriers or obstacles women have to breastfeed.
- 3.
- PERCEPTIONS about the causes of breastfeeding abandonment.
- 4.
- PERCEPTIONS about the causes of breastfeeding adherence.
- 5.
- Proposal to improve the encouragement and promotion of adherence to breastfeeding.
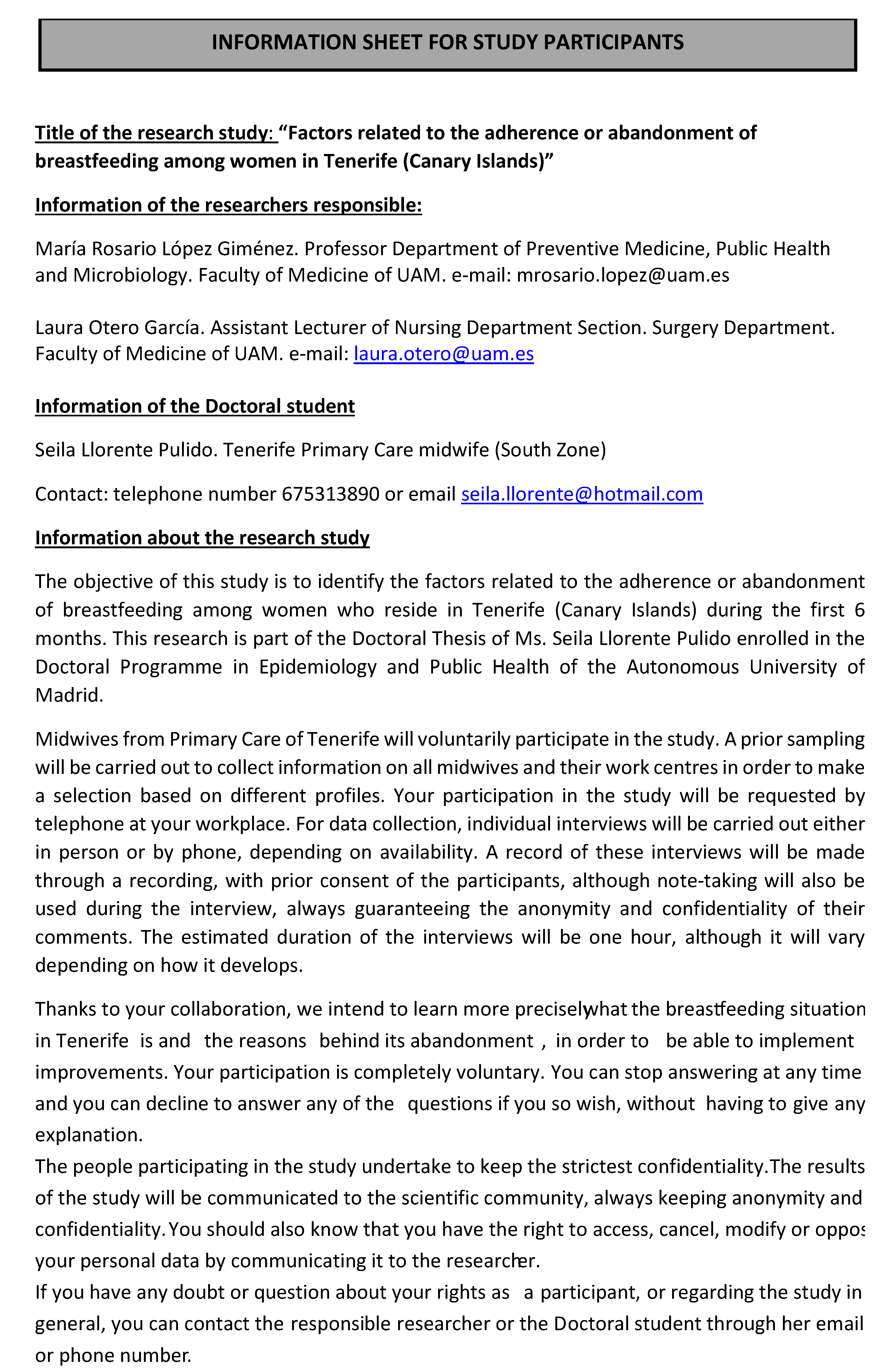
Appendix C. Information Sheet and Informed Consent


References
- WHO. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Hassiotou, F.; Geddes, D.T. Immune cell-mediated protection of the mammary gland and the infant during breastfeeding. Adv. Nut. 2015, 6, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kull, I.; Melen, E.; Alm, J.; Hallberg, J.; Svartengren, M.; van Hage, M. Breast-feeding in relation to asthma, lung function, and sensitization in young schoolchildren. J. Allergy Clin. Immunol. 2010, 125, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Duijts, L.; Jaddoe, V.W.; Hofman, A.; Moll, H.A. Prolonged and exclusive breastfeeding reduces the risk of infectious diseases in infancy. Pediatrics 2010, 126, e18–e25. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. 10 Facts on Breastfeeding. World Health Organization; World Health Organization: Geneva, Switzerland, 2014; Available online: http://www.who.int/features/factfiles/breastfeeding/en/ (accessed on 23 March 2021).
- Hörnell, A.; Lagström, H.; Lande, B.; Thorsdottir, I. Breastfeeding, introduction of other foods and effects on health: A systematic literature review for the 5th Nordic Nutrition Recommendations. Food Nutr. Res. 2013, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yorifuji, T.; Kubo, T.; Yamakawa, M.; Kato, T.; Inoue, S.; Tokinobu, A.; Doi, H. Breastfeeding and behavioral development: A nationwide longitudinal Survey in Japan. J. Pediatr. 2014, 164, 1019–1025.e3. [Google Scholar] [CrossRef] [PubMed]
- Mosca, F.; Giannì, M.L. Human milk: Composition and health benefits. Pediatr. Medica Chir. 2017, 39, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Ciampo, L.A.; Lopes Del Ciampo, I.R. Breastfeeding and the Benefits of Lactation for Women’s Health. Rev. Bras. Ginecol. Obstet. 2018, 40, 354–359. [Google Scholar] [CrossRef] [Green Version]
- Hamdan, A.; Tamim, H. The relationship between postpartum depression and breastfeeding. Int. J. Psychiatry Med. 2012, 43, 243–259. [Google Scholar] [CrossRef]
- Brown, A.; Rance, J.; Bennett, P. Understanding the relationship between breastfeeding and postnatal depression: The role of pain and physical difficulties. J. Adv. Nurs. 2016, 72, 273–282. [Google Scholar] [CrossRef] [Green Version]
- Heinrichs, M.; NeumannI, D.; Ehlert, U. Lactation and stress: Protective effects of breast-feeding in humans. Stress 2002, 5, 165–203. [Google Scholar] [CrossRef]
- Groër, M.W. Differences between exclusive breastfeeders, formula-feeders, and controls: A study of stress, mood, and endocrine variables. Biol. Res. Nurs. 2005, 7, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Krol, K.M.; Grossmann, T. Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsbl 2018, 61, 977–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doan, T.; Gardiner, A.; Gay, C.L.; Lee, K.A. Breastfeeding increases sleep duration of new parents. J. Perinat. Neonat. Nurs. 2007, 21, 200–206. [Google Scholar] [CrossRef]
- Kramer, M.S.; Kakuma, R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2012, 2012, CD003517. [Google Scholar] [CrossRef]
- Global Nutrition Report 2015: Actions and Accountability to Advance Nutrition and Sustainable Development; International Food Policy Research Institute: Washington, WA, USA, 2015.
- Sítuación de Salud Informe de Salud Informe Anual del Sistema Nacional de Salud 2018. Informes, Estudios e Investigación 2020 Ministerio de Sanidad. Secretaría General Técnica Pº del Prado, 18–20. 28014 Madrid NIPO: 133-20-031-6. Available online: https://cpage.mpr.gob.es/ (accessed on 29 July 2020).
- Encuesta Nacional de Salud 2012. Instituto Nacional de Estadística. Ministerio de Sanidad, Servicios Sociales e Igualdad. Available online: http://www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/ (accessed on 4 May 2020).
- World Health Organization. Global Nutrition Targets 2025 Breastfeeding Policy Brief. WHO/NMH/NHD/14.7; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Oribe, M.; Lertxundia, A.; Basterrechea, M.; Begiristain, H.; Santa Marina, L.; Villar, M.; Dorronsoro, M.; Amiano, P.; Ibarluzea, J. Prevalencia y factores asociados con la duración de la lactancia materna exclusiva durante los 6 primeros meses en la cohorte INMA de Guipúzcoa. Gac. Sanit. 2015, 29, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Medina, F.I.M.; Fernández, G.C.T. Breastfeeding problems prevention in early breast feeding through effective technique. Enfermería Global Nº 31. Rev. Electr. Trimest. Enfermería 2013, 12, 443–444. [Google Scholar]
- Abou-Dakn, M.; Fluhr, J.W.; Gensch, M.; Woeckel, A. Positive Effect of HPA Lanolin versus Expressed Breastmilk on Painful and Damaged Nipples during Lactation. 2011. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/20720454 (accessed on 4 May 2020).
- Díaz-Gómez, N.M.; Ruzafa-Martínez, M.; Ares, S.; Espiga, I.; De Alba, C. Motivaciones y barreras percibidas por las mujeres españolas en relación a la lactancia materna. Rev. Esp. Salud Pública 2016, 90, e1–e18. [Google Scholar]
- Thomson, G.; Dykes, F.; Hurley, M.A.; Hoddinott, P. Incentives as connectors: Insights into a breastfeeding incentive intervention in a disadvantaged area of North-West England. BMC Pregnancy Childbirth 2012, 12, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rius, J.M.; Ortuno, J.; Rivas, C.; Maravall, M.; Calzado, M.A.; López, A.; Aguar, M.; Vento, M. Factores asociados al abandono precoz de la lactancia materna en una región del este de España. Anales Pediatr. 2014, 80, 6–15. [Google Scholar] [CrossRef] [PubMed]
- González, I.A.; Huespe Auchter, M.S.; Auchter, M.C. Lactancia materna exclusiva factores de éxito y/o fracaso. Rev. Posgrado VIa Cátedra Med. 2008, 177, 2. [Google Scholar]
- Vila-Candel, R.; Soriano-Vidal, F.J.; Murillo-Llorente, M.; Pérez-Bermejo, M.; Castro-Sánchez, E. Mantenimiento de la lactancia materna exclusiva a los 3 meses posparto: Experiencia en un departamento de salud de la Comunidad Valenciana. Aten Primaria 2019, 51, 91–98. [Google Scholar] [CrossRef]
- Haiek, L.N.; Gauthier, D.L.; Brosseau, D.; Rocheleau, L. Understanding breastfeeding behavior: Rates and shifts in patterns in Quebec. J. Hum. Lact. 2007, 23, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Almeida, C.P.; Cunha, F.F.; Pires, E.P.; SÁ, E. Common mental disorders in pregnancy in the context of interpartner violence. J. Psychiatr. Ment. Health Nurs. 2013, 20, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Gubler, T.; Krähenmann, F.; Roos, M.; Zimmermann, R.; Ochsenbein-Kölble, N. Determinants of successful breastfeeding initiation in healthy term singletons: A Swiss university hospital observational study. J. Perinat. Med. 2013, 41, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dozier, A.M.; Howard, C.R.; Brownell, E.A.; Wissler, R.N.; Glantz, J.C.; Ternullo, S.R.; Thevenet-Morrison, K.N.; Childs, C.K.; Lawrence, R.A. Labor Epidural Anesthesia, Obstetric Factors and Breastfeeding Cessation. 2013. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/22696104 (accessed on 4 May 2020).
- Bellù, R.; Condò, M. Breastfeeding promotion: Evidence and problems. Pediatr. Med. Chir. 2017, 39, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frías, R.L.; Bello, H.M.J.; Fernández, R.A.A. La función de las matronas en la Edad Media. Primer Semest. 2019, 13, 17–25. [Google Scholar]
- Pol-Pons, A.; Aubanell-Serra, M.; Vidal, M.; Martí-Lluch, R.; Ponjoan, A. Lactancia materna: Competencia básica de los profesionales sanitarios de atención primaria. Aten Primar. 2019, 51, 47–51. [Google Scholar] [CrossRef]
- Pol-Pons, A.; Aubanell-Serra, M.; Vidal, M.; Ojeda-Ciurana, I.; Martí-Lluch, R.; Ponjoan, A. Breast feeding basic competence in primary care: Development and validation of the CAPA questionnaire. Midwifery 2016, 42, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Muñiz, L.C.; Sánchez, C.J.L.; Castanedo, H.S.; del Río, C.E.; Sota, M.S.; de Adana Herrero, S.M. ECoLaE: Validación de un cuestionario sobre conocimientos y habilidades en lactancia materna para enfermería. Aten Primar. 2020, 52, 373–380. [Google Scholar] [CrossRef]
- Martínez, F.E.; del Pulgar, G.M.; Martín, P.A.; Zafra, O.M.D.; Fernández, P.M.L.; Montesinos, B.J.V. Análisis de la definición de la matrona, acceso a la formación y programa formativo de este profesional de la salud a nivel internacional, europeo y español. Educ. Méd. 2018, 19 (Suppl. 3), 360–365. [Google Scholar] [CrossRef]
- Swerts, M.; Westhof, E.; Bogaerts, A.; Lemiengre, J. Supporting breast-feeding women from the perspective of the midwife: A systematic review of the literature. Midwifery 2016, 37, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Gross, S.; Resnik, A.; Nanda, J.P.; Cross-Barnet, C.; Augustyn, M.; Kelly, L.; Paige, D.M. Early Postpartum: A Critical Period in Setting the Path for Breastfeeding Success. Breastfeed. Med. 2011, 6, 407–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, H.; McLelland, G.; Gilmour, C.; Cant, R. It’s those first few weeks’: Women’s views about breastfeeding support in an Australian outer metropolitan región. Women Birth 2014, 27, 259–265. [Google Scholar] [CrossRef]
- Burns, E.; Schmied, V.; Fenwick, J.; Sheehan, A. Liquid gold from the milk bar: Constructions of breastmilk and breastfeeding women in the language and practices of midwives. Soc. Sci. Med. 2012, 75, 1737–1745. [Google Scholar] [CrossRef]
- ISTAC. Instituto Canario de Estadística de 2017, 2018, 2019 y 2020. Available online: https://www3.gobiernodecanarias.org/istac/ (accessed on 26 May 2020).
- INE (Instituto Nacional de Estadística). 2019. Available online: https://ine.es/jaxi/Datos.htm?path=/t20/e245/p04/provi/l0/&file=0ccaa002.px (accessed on 26 May 2020).
- Organización Territorial de Tenerife. Available online: https://www3.gobiernodecanarias.org/sanidad/scs/mapa (accessed on 26 May 2020).
- Brounéaus, K. In depth Intervieweing: The process, skills and ethics of interviews in peace research. In Understanding Peace Researcch: Methods and Challenges; Höglundand, K., Óberg, M., Eds.; Routledge: London, UK; New York, NY, USA, 2011. [Google Scholar]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurs. Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- ICT Services and System Development and Division of Epidemiology and Global Health; Open Code 4.02; University of Umeå: Umeå, Sweden, 2013.
- Bronfenbrenner, U. La Ecología del Desarrollo Humano; Paidós: Barcelona, Spain, 1971. [Google Scholar]
- Quirós, C.C. Factores socioeconómicos, culturales y asociados al sistema de salud que influyen en el amamantamiento. Rev. Enfermer. Actual Costa Rica Octubre 2008, 15. Available online: http://www.revenf.ucr.ac.cr/factoreslactancia.pdf (accessed on 4 May 2020).
- Navarro, Q.B.; Leal, B.S.; Villaescusa, P.R.; Castillejos, B.A. Influencia de la Fatiga Posparto Sobre el Tipo de Alimentación en el Primer Mes de Vida. 2014. Available online: http://www.nureinvestigacion.es/OJS/index.php/nure/article/view/95 (accessed on 4 May 2020).
- Garfias Barrera, A.; Márquez Cardoso, E.; Moreno Aguilera, F.; Bazán Castro, M. Maternal and family risk factors that influence the abandonment of breastfeeding. J. Med.-Surg. Spec. 2007, 12, 53–57. [Google Scholar]
- Puertas, C.E.; Herrerías, H.I.; Escalante, A.I. Creencias, Actitudes y Barreras Percibidas por las Madres Adolescentes Respecto a la Lactancia Materna. Paraninfo Digital, Monográficos de Investigación en Salud. ISSN: 1988–3439. Cualisalud 2014—XI Reunión Internacional—I Congreso Virtual de Investigación Cualitativa en Salud. Available online: http://www.index-f.com/para/n20/353.php (accessed on 4 May 2020).
- Ogbo, F.A.; Akombi, B.J.; Ahmed, K.Y.; Rwabilimbo, A.G.; Ogbo, A.O.; Uwaibi, N.E.; Agho, K.E. Breastfeeding in the community—how can partners/fathers help? A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 413. [Google Scholar] [CrossRef] [Green Version]
- Jeanjot, I.; Barlow, P.; Rozenberg, S. Domestic violence during pregnancy: Survey of patients and healthcare providers. J. Womens Health 2008, 17, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Stockl, H.; Hertlein, L.; Friese, K.; Stockl, D. Partner, workplace, and stranger abuse during pregnancy in Germany. Int. J. Gynaecol. Obstet. 2010, 111, 136–139. [Google Scholar] [CrossRef]
- Vatnar, S.K.; Bjørkly, S. Victim of and witness to violence: An interactional perspective on mothers’ perceptions of children exposed to intimate partner violence. Violence Vict. 2011, 26, 830–852. [Google Scholar] [CrossRef]
- Mariano, L.M.B.; Monteiro, J.C.S.; Stefanello, J.; Gomes-Sponholz, F.A.; Oriá, M.O.B.; Nakano, M.A.S. Exclusive breastfeeding and maternal self-efficacy among women of intimate partner violence situations. Texto Contexto Enferm. 2016, 25, e2910015. [Google Scholar] [CrossRef]
- Escriba-Aguir, V.; Royo-Marques, M.; Artazcoz, L.; Romito, P.; Ruiz-Perez, I.; Martin-Baena, D. Personal and psychosocial predictors of psychological abuse by partners during and after pregnancy: A longitudinal cohort study in a community sample. BJOG 2013, 120, 576–582. [Google Scholar] [CrossRef]
- Jasinski, J.L. Pregnancy and domestic violence: A review of the literature. Trauma Violence Abuse 2004, 5, 47–64. [Google Scholar] [CrossRef] [Green Version]
- Nesbitt, S.A.; Campbell, K.A.; Jack, S.M.; Robinson, H.; Piehl, K.; Bogdan, J.C. Canadian adolescent mothers’ perceptions of influences on breastfeeding decisions: A qualitative descriptive study. BMC Pregnancy Childbirth 2012, 12, 149. [Google Scholar] [CrossRef] [Green Version]
- Otal-Lospaus, S.; Morera-Liánez, L.; Bernal-Montañes, M.J.; Tabueña-Acin, J. El contacto precoz y su importancia en la lactancia materna frente a la cesárea. Matronas Prof. 2012, 13, 3–8. [Google Scholar]
- Muñoz, C.L. La madre que amamanta y el entorno laboral. Matronas Prof. 2008, 9, 21–26. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| North | South | Metropolitan | Total Population | |
|---|---|---|---|---|
| Number of inhabitants | 224.047 | 291.706 | 388.960 | 904.713 |
| Number of foreign inhabitants | 14.218 | 81.875 | 21.103 | 117.196 |
| Employed population (in thousands) | 93,42 | 129,78 | 172,04 | 395,24 |
| Number of BHZ | 12 | 10 | 17 | 39 |
| Subcategories | Quotes from the Midwives |
|---|---|
| The negative influence of male chauvinism on upbringing and BF. Midwives perceive the negative influence of male chauvinism on upbringing and BF. Socially, there are many cases in which sexualisation of women occurs where women are valued more for their physical appearance than for other qualities or capacities. This generates an increased pressure and anxiety for them to continue staying “pretty or beautiful” in the same way as before. | “...on a social level women are valued above all for their physical appearance, so we are immediately concerned with being as we were before, beauty and consumption are the things that are valued and it is not valued that a woman breastfeeds for three years, these women are referred to as hippies or weirdos…” (E8) |
| The gender inequality in the couple relationship. The informants perceive that this gender inequality also occurs in the couple relationship, becoming compromised when they become parents. The woman focuses on caring for the child and the partner feels neglected, receiving less attention than before. | “…There are many couples who separate in the postpartum period. The couple is tested, in the change from a couple relationship to parents of a baby”. “And many times, they do not support them in breastfeeding, on the contrary, they complain that they do not have time for them.” (E4) |
| The simplistic conception of the woman’s breast. As another negative factor for BF in relation to the chauvinist society, the midwives point out the simplistic conception of the woman’s breast as an element without biological function, by not respecting BF in public. Socially, the breast of the woman in its breastfeeding function is not as accepted, despite the fact that BF in other mammals is more normalized. | “...censuring a woman who is breastfeeding, because she′s showing her tit. Many women breastfeeding in public get bad looks, there are even people who tell them to cover themselves…” (E2) |
| The loneliness that accompanies motherhood. Midwives highlight the feeling of loneliness that characterises motherhood today. They explain that before, women lived with the family and had the opportunity to face this stage together, while currently many women do not have the support of their partner or family, because they are not physically close or because their presence and involvement in parenting is non-existent. In these cases, women feel alone in seeing to the needs of a newborn 24 h a day, where additionally BF requires more time and exclusive dedication, without the possibility to delegate and be able to do other things. | “...the feeling of loneliness I think is an important factor, which is ascribed to motherhood, we women have it now in the postnatal period and it is seen more or less intensely depending on the support you have.” (E1) |
| Being a mother: a clash between expectations and reality as a negative factor for EBF. Midwives point out that the social idealisation of motherhood makes it difficult for women to adapt to the new situation. The lack of close references and true information on postpartum and motherhood causes women, after childbirth, to find themselves in a situation they did not expect, and without any tools to face it. | “...the differences between fiction and reality. The imaginary idea they had of what it is to be a mother, what they′ve seen in movies, what they′ve seen with their friends, a couple of hours is not the same as 24 h in the leading role of a nursing mother.” (E15) |
| The current individualistic society: loss of the “tribe” sense, key to EBF. Midwives highlight the influence of the general functioning of today’s society, much more individualistic in upbringing and especially in BF. The informants perceive that it can be a negative factor for new mothers to not have any close lactating women as a reference and as an example for them. | “We are in an individualistic society, raising our child alone, so you spend a lot of time alone with your baby in your house taking care of it without other women who support you, we are not surrounded by our relatives who support us with breastfeeding as they used to.” (E4) |
| Characteristics of jobs that hinder BF. Midwives indicate that women find it difficult to maintain EBF due to the lack of support at work in reconciling it with family life, related to the characteristics of the position they occupy. | “...women with important positions do not even have half an hour of rest, but must always be available. This is causing them a lot of anxiety in returning to work, so they decide to bottle-feed.” (E15) |
| Early return to work is detrimental to BF. Midwives perceive that insecure working conditions determine an early return, hindering EBF and upbringing. | “…The population that I attended had very difficult work contracts, if they did not come back within 6 weeks, they no longer had a job. The commitment to their job and job insecurity, had a great influence on that too...” (E3) |
| The inability to express milk at work leads to stopping EBF. The informants point out that the inability to express milk during the working day causes discomfort and problems that force women to abandon BF. | “...especially the main problem is that not all jobs allow you to go and express your milk. Some mothers have told me: ′Look, I have to stop this because throughout the day I could not go at any time to express milk and my breasts hurt, I could not stand it.” (E14) |
| Expressing milk at work, but in inadequate conditions. Midwives indicate that women manage to express milk at work in order to continue their BF, but in inadequate conditions, using their resting time for it, as in many jobs it is not even contemplated. They do not even have a dedicated space for it, and milk is usually expressed in bathrooms or remote places, where women feel uncomfortable. | “...There are women who use the half hour they have for breakfast to express milk or there are times when they feel strange or are embarrassed. Sometimes they cry in the bathroom.” (E17) |
| Maternal motivation is a protective factor to continue breastfeeding after returning to work. The informants point out that the return to work is a moment of important crisis in EBF. Many women highlight that the degree of involvement and motivation for EBF is more important than the return to work itself. | “...in the end, those who really believe in breastfeeding, the fact that they work or not, is not decisive.” (E15) |
| Working woman and mother, conflict of interest. Midwives emphasise that the return to work with a small baby implies a conflict of interest for women, where in one way or another it is a resignation, either at a professional level or at the level of more present parenting. | “Well, many times you give up breastfeeding or maternity or a more present upbringing you would like, the neuropsychology supports it or you have to leave your job a bit. Sometimes they are forced to leave even their job or a job promotion…” (E1) |
| Women seek ways to reconcile EBF and work at the cost of pay cuts. Midwives find that women are looking for a way to reconcile EBF but many times that implies a reduction in income or an increase in expenses if they decide to take the baby to a nursery. | “And if I reduce the working hours, on the days that I do have to work, I have to pay for childcare, then I earn less and on top of that I am paying for care...” (E3) |
| Need to plan ahead and get used to it previously. Midwives perceive that women are very concerned with going back to work and the care of their child in their absence, so many prepare for that moment. Women decide to plan and start bottle-feeding or anticipate the introduction of complementary foods so someone else can feed their child while they are at work. | “… If my child is going to stay with my mother or is going to go to kindergarten, I start giving him a bottle when he′s two months old so he can get used to it, it is like planning ahead…” (E8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llorente-Pulido, S.; Custodio, E.; López-Giménez, M.R.; Sanz-Barbero, B.; Otero-García, L. Barriers and Facilitators for Exclusive Breastfeeding in Women’s Biopsychosocial Spheres According to Primary Care Midwives in Tenerife (Canary Islands, Spain). Int. J. Environ. Res. Public Health 2021, 18, 3819. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073819
Llorente-Pulido S, Custodio E, López-Giménez MR, Sanz-Barbero B, Otero-García L. Barriers and Facilitators for Exclusive Breastfeeding in Women’s Biopsychosocial Spheres According to Primary Care Midwives in Tenerife (Canary Islands, Spain). International Journal of Environmental Research and Public Health. 2021; 18(7):3819. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073819
Chicago/Turabian StyleLlorente-Pulido, Seila, Estefanía Custodio, Maria Rosario López-Giménez, Belén Sanz-Barbero, and Laura Otero-García. 2021. "Barriers and Facilitators for Exclusive Breastfeeding in Women’s Biopsychosocial Spheres According to Primary Care Midwives in Tenerife (Canary Islands, Spain)" International Journal of Environmental Research and Public Health 18, no. 7: 3819. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073819