
Dental Expenditure by Household Income in Korea over the Period 2008–2017: A Review of the National Dental Insurance Reform


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Analyses
3. Results
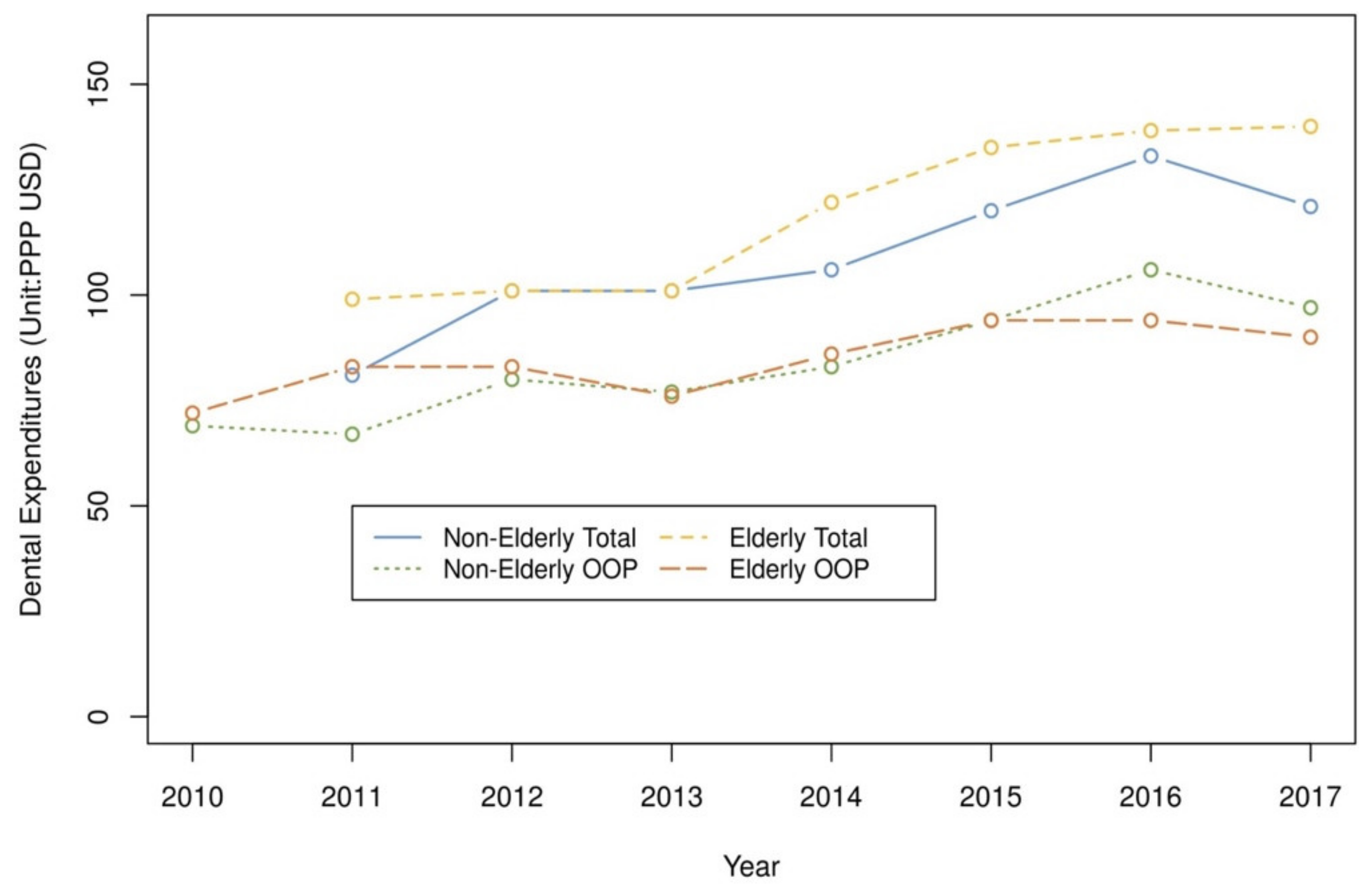
3.1. Dental Utilization and Expenditures
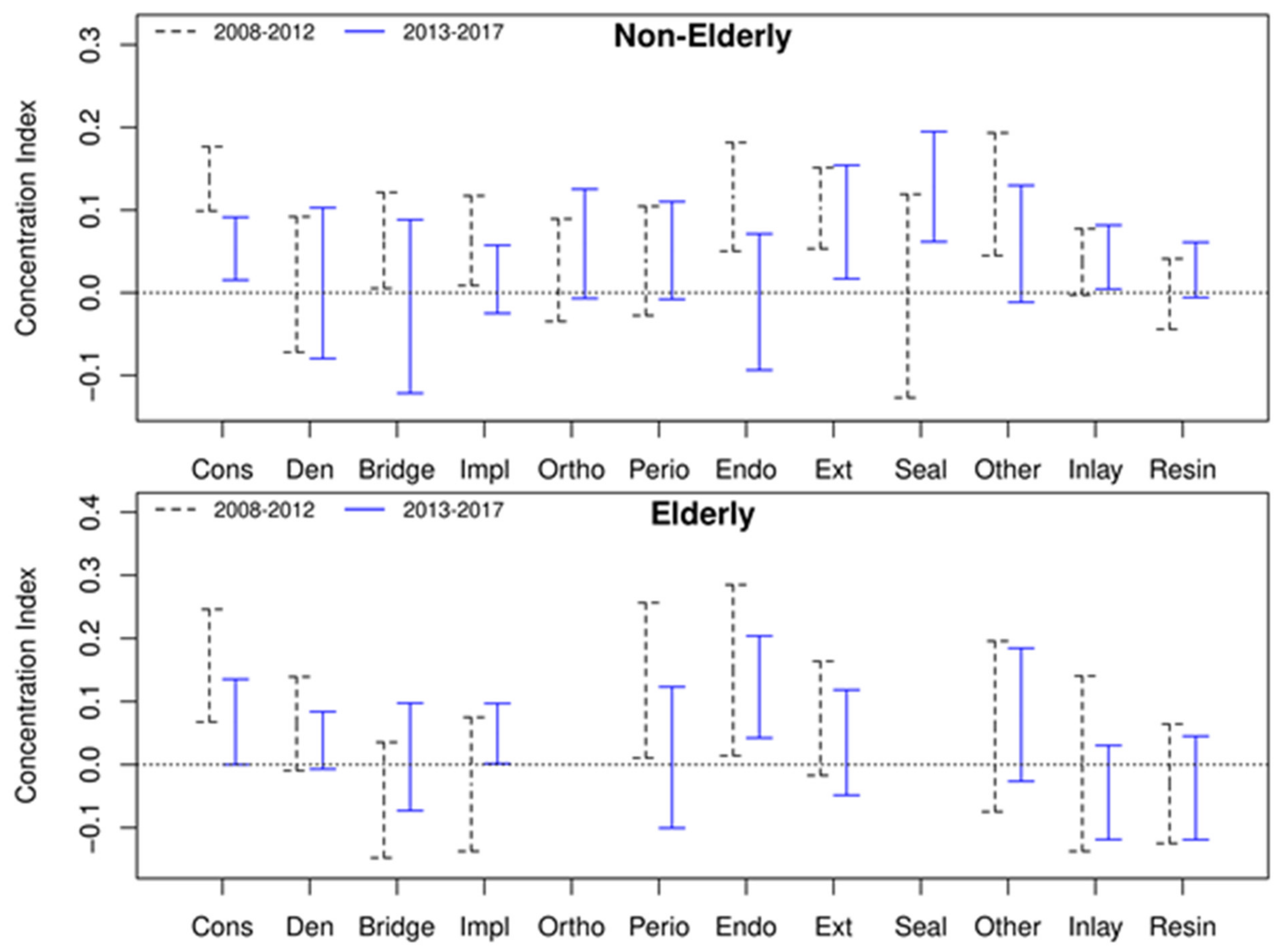
3.2. CI and Dental Inequalities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- OECD. Health at a Glance 2015: OECD Indicators; OECD Publishing: Paris, France, 2015; pp. 122–123. [Google Scholar] [CrossRef]
- Paris, V.; Hewlett, E.; Auraaen, A.; Alexa, J.; Simon, L. Health Care Coverage in OECD Countries in 2012; OECD Publishing: Paris, France, 2016; p. 69. [Google Scholar] [CrossRef]
- Insurance System in South Korea. Health Insurance Review & Assessment Serviced. Available online: https://www.hira.or.kr/dummy.do?pgmid=HIRAA020014000000 (accessed on 11 February 2020).
- Lee, H.J.; Kim, M.Y.; Yang, D.N. Recognition of dental patients in the capital area with regard to the private dental insurance. J. Korean Soc. Oral Health Sci. 2018, 6, 15–22. [Google Scholar]
- Kim, T.I.; Huh, S.I. Changes in financial burden of health expenditures by income level. Health Policy Manag. 2008, 18, 23–48. [Google Scholar]
- Duncan, L.; Bonner, A. Effects of income and dental insurance coverage on need for dental care in Canada. J. Can. Dent. Assoc. 2014, 80, 1–9. [Google Scholar]
- Schwendicke, F.; Dörfer, C.E.; Schlattmann, P.; Page, L.F.; Thomson, W.M.; Paris, S. Socioeconomic inequality and caries: A systematic review and meta-analysis. J. Dent. Res. 2015, 94, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Guessous, I.; Theler, J.M.; Izart, C.D.; Stringhini, S.; Bodenmann, P.; Gaspoz, J.M.; Wolff, H. Forgoing dental care for economic reasons in Switzerland: A six-year cross-sectional population-based study. BMC Oral Health 2014, 14, 121. [Google Scholar] [CrossRef] [Green Version]
- Armfield, J. The avoidance and delaying of dental visits in Australia. Aust. Dent. J. 2012, 57, 243–247. [Google Scholar] [CrossRef]
- Grytten, J.; Holst, D.; Skau, I. Demand for and utilization of dental services according to household income in the adult population in Norway. Community Dent. Oral Epidemiol. 2012, 40, 297–305. [Google Scholar] [CrossRef]
- Kim, H.S.; Ahn, E.; Kim, M.Y.; Kim, S.M.; Shin, H. Trends of household income and dental care spending. J. Korean Acad. Oral Health 2014, 38, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Park, E.J.; Seo, J.; Jung, Y.; Bae, J.; Lee, N.; Kim, E.; Yeom, A.; Yoon, Y.; Kim, K.; Park, H.; et al. A Report on the Korea Health Panel Survey of 2017; Korea Institute for Health and Social Affairs: Sejong, Korea, 2019; pp. 31, 36–41. [Google Scholar]
- Sanwald, A.; Theurl, E. Out-of-pocket expenditure by private households for dental services—Empirical evidence from Austria. Health Econ. Rev. 2016, 6, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’donnell, O.; van Doorslaer, E.; Wagstaff, A.; Lindelow, M. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and Their Implementation; The World Bank: Washington, DC, USA, 2008; pp. 83–84. [Google Scholar]
- Kakwani, N.C. Measurement of Tax Progressivity: An International Comparison. Econ. J. 1977, 87, 71–80. [Google Scholar] [CrossRef]
- Creedy, J.; Sleeman, C. Adult equivalence scales, inequality and poverty. N. Z. Econ. Pap. 2005, 39, 51–81. [Google Scholar] [CrossRef]
- Rao, C.R. Linear Statistical Inference and Its Applications, 2nd ed.; Wiley: New York, NY, USA, 1973; pp. 388–389. [Google Scholar]
- Kakwani, N.; Wagstaff, A.; Van Doorslaer, E. Socioeconomic inequalities in health: Measurement, computation, and statistical inference. J. Econ. 1997, 77, 87–103. [Google Scholar] [CrossRef] [Green Version]
- Koolman, X.; Van Doorslaer, E. On the interpretation of a concentration index of inequality. Health Econ. 2004, 13, 649–656. [Google Scholar] [CrossRef]
- World Bank. PPP Conversion Factor, GDP (LCU per International $)—Korea, Rep. Available online: https://data.worldbank.org/indicator/PA.NUS.PPP?locations=KR (accessed on 17 February 2020).
- Jiménez, J.; Perdiguero, J. Difference-in-Difference; Springer: New York, NY, USA, 2019; pp. 551–555. [Google Scholar] [CrossRef]
- Bailit, H.; Beazoglou, T. Financing dental care: Trends in public and private expenditures for dental services. Dent. Clin. N. Am. 2008, 52, 281–295. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2013: OECD Indicators; OECD Publishing: Paris, France, 2013; p. 147. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.T.; Lee, J.H.; Kweon, H.H.I.; Lee, J.S.; Choi, J.K.; Kim, D.W.; Choi, S.H. Evaluation of national health insurance coverage of periodontal scaling: A nationwide cohort study in Korea. J. Korean Dent. Assoc. 2016, 54, 604–612. [Google Scholar]
- Huh, J.; Nam, S.; Lee, B.; Hu, K.S.; Jung, I.Y.; Choi, S.H.; Lee, J.Y. Improvement of Accessibility to Dental Care due to Expansion of National Health Insurance Coverage for Scaling in South Korea. J. Korean Dent. Assoc. 2019, 57, 644–653. [Google Scholar]
- Park, H.J.; Lee, J.H.; Park, S.; Kim, T.I. Changes in dental care access upon health care benefit expansion to include scaling. J Periodontal. Implant. Sci. 2016, 46, 405–414. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Amar, S. Periodontal disease and systemic conditions: A bidirectional relationship. Odontology 2006, 94, 10–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.S.; Jung, S.H. The impact of expanded national health insurance coverage of dentures and dental implants on dental care utilization among older adults in South Korea: A study based on the Korean Health Panel Survey. Int. J. Environ. Res. Public Health 2020, 17, 6417. [Google Scholar] [CrossRef]
- Oh, M.A. Policy issues of elderly welfare spending for alleviating the elderly poverty rate. Public Health Forum 2013, 196, 25–35. [Google Scholar]
- Kim, J.; Bae, H. A Study of the Experience of Unmet Dental Care Needs among Older Adults. Health Soc. Welf. Rev. 2019, 39, 365–389. [Google Scholar]
- Listl, S. Income-related inequalities in dental service utilization by Europeans aged 50+. J. Dent. Res. 2011, 90, 717–723. [Google Scholar] [CrossRef]
- Geyer, S.; Schneller, T.; Micheelis, W. Social gradients and cumulative effects of income and education on dental health in the Fourth German Oral Health Study. Community Dent. Oral Epidemiol. 2010, 38, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Nakao, H.; Imai, H. Different income information as an indicator for health inequality among Japanese adults. J. Epidemiol. 2007, 17, 93–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molarius, A.; Engström, S.; Flink, H.; Simonsson, B.; Tegelberg, Å. Socioeconomic differences in self-rated oral health and dental care utilisation after the dental care reform in 2008 in Sweden. BMC Oral Health 2014, 14, 134. [Google Scholar] [CrossRef] [Green Version]
- Bertoldi, C.; Lalla, M.; Pradelli, J.M.; Cortellini, P.; Lucchi, A.; Zaffe, D. Risk factors and socioeconomic condition effects on periodontal and dental health: A pilot study among adults over fifty years of age. Eur. J. Dent. 2013, 7, 336. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Larsson, M.; Berglundh, T. Effectiveness of implant therapy analyzed in a Swedish population: Early and late implant loss. J. Dent. Res. 2015, 94, 44S–51S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kravitz, A.; Treasure, E.T. EU Manual of Dental Practice 2015; Council of European Dentists: Brussels, Belgium, 2015; p. 186. [Google Scholar]
- Kim, C.S.; Han, S.Y.; Lee, S.E.; Kang, J.H.; Kim, C.W. Dental care utilization for examination and regional deprivation. J. Prev. Med. Public Health 2015, 48, 195. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, A.N.; Everitt, B.; Newton, T.; Steele, J.; Sherriff, M.; Bower, E. The effects of social class and dental attendance on oral health. J. Dent. Res. 2008, 87, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Anikeeva, O.; Brennan, D.S.; Teusner, D.N. Household income modifies the association of insurance and dental visiting. BMC Health Serv. Res. 2013, 13, 432. [Google Scholar] [CrossRef] [Green Version]
- Thompson, B.; Cooney, P.; Lawrence, H.; Ravaghi, V.; Quiñonez, C. The potential oral health impact of cost barriers to dental care: Findings from a Canadian population-based study. BMC Oral Health 2014, 14, 78. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Time | Newly Added Dental Benefits |
|---|---|
| December 2009 | Sealant (6 to 14 years old) in the 1st molar (sound teeth not affected by caries) |
| December 2010 | Sealant (6 to 14 years old) in the 1st molar (sound tooth with occlusal surface not affected by caries) |
| July 2012 | Complete denture (CD) for people aged 75 or older |
| October 2012 | Sealant in the 1st and 2nd molar teeth of children under 14 years old (sound teeth with occlusal surface not affected by caries) |
| April 2013 | Sealant (under 18 years old) in the 1st and 2nd molar teeth in children/adolescents (sound teeth with occlusal surface not affected by caries) |
| July 2013 | Scaling for all ages (full mouth scaling for prevention, once a year for people over 20 years old) |
| Removable partial denture (RPD) for people aged 75 or older | |
| July 2014 | Dental implant for people aged 75 or older |
| July 2015 | CD, RPD, and dental implants for people aged 70 or older |
| July 2016 | CD, RPD, and dental implants for people aged 65 or older |
| August 2017 | The co-payment for implants and dentures for people aged 65 and over was reduced from 50% to 30% |
| October 2017 | Sealant’s co-payment rate cut to 10% |
| Items | Categories | Elderly (n = 3650) | Non-Elderly (n = 12,843) | p-Value 3 |
|---|---|---|---|---|
| Age (mean) | 73.6 | 38.2 | <0.001 | |
| Gender (%) | Male | 46.5 | 43.8 | <0.001 |
| Female | 53.5 | 56.2 | ||
| Marital status (%) | Single | 30 | 56.3 | <0.001 |
| Married | 70 | 43.7 | ||
| Education (%) | ≤Elementary | 50.8 | 24.1 | <0.001 |
| Middle/High | 39.6 | 45.3 | ||
| ≥College | 9.6 | 30.6 | ||
| Medical aid (%) | 6.5 | 3.0 | <0.001 | |
| Job (%) | Unemployed | 85.2 | 45.2 | <0.001 |
| Equivalence Income 1 | 17,620 | 30,326 | <0.001 | |
| Number of annual dental visits | 2008–2012 | 5.00 | 3.99 | <0.001 |
| 2013–2017 | 5.32 | 3.81 | ||
| Ratio of dental expenditure 2 (%) | 2008–2012 | 30.7 | 46.5 | <0.001 |
| 2013–2017 | 31.1 | 42.5 |
| Items | Equivalence Scale | Gross Household Income | |||||
|---|---|---|---|---|---|---|---|
| CI 1 | 95% CI 2 | CI 1 | 95% CI 2 | ||||
| Total | 0.0859 | 0.0725 | 0.0993 | 0.0728 | 0.0593 | 0.0864 | |
| Age | Non-elderly | 0.1011 | 0.0853 | 0.1170 | 0.0903 | 0.0742 | 0.1065 |
| Elderly | 0.0802 | 0.0555 | 0.1050 | 0.0728 | 0.0486 | 0.0970 | |
| Year | 2008–2012 (P1) | 0.1118 | 0.0911 | 0.1326 | 0.0977 | 0.0768 | 0.1185 |
| 2013–2017 (P2) | 0.0562 | 0.0386 | 0.0738 | 0.0471 | 0.0294 | 0.0648 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, H.; Cho, H.-A.; Kim, B.-R. Dental Expenditure by Household Income in Korea over the Period 2008–2017: A Review of the National Dental Insurance Reform. Int. J. Environ. Res. Public Health 2021, 18, 3859. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083859
Shin H, Cho H-A, Kim B-R. Dental Expenditure by Household Income in Korea over the Period 2008–2017: A Review of the National Dental Insurance Reform. International Journal of Environmental Research and Public Health. 2021; 18(8):3859. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083859
Chicago/Turabian StyleShin, Hosung, Han-A Cho, and Bo-Ra Kim. 2021. "Dental Expenditure by Household Income in Korea over the Period 2008–2017: A Review of the National Dental Insurance Reform" International Journal of Environmental Research and Public Health 18, no. 8: 3859. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083859