
Psychiatric Comorbidity in Mexican Adolescents with a Diagnosis of Eating Disorders Its Relationship with the Body Mass Index


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Statement
2.3. Measurements
2.3.1. Sociodemographic and Anthropometric Measurements
2.3.2. Clinical Measurements
Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-Kid)
Questionnaire on Eating and Weight Pattern-Revised (QEWP-R)
2.4. Statistical Analysis
2.4.1. Comparison with Reference Sample
2.4.2. Comparison between ED Diagnoses
2.4.3. Comparison of BMI between ED Diagnosis and Comorbidities
3. Results
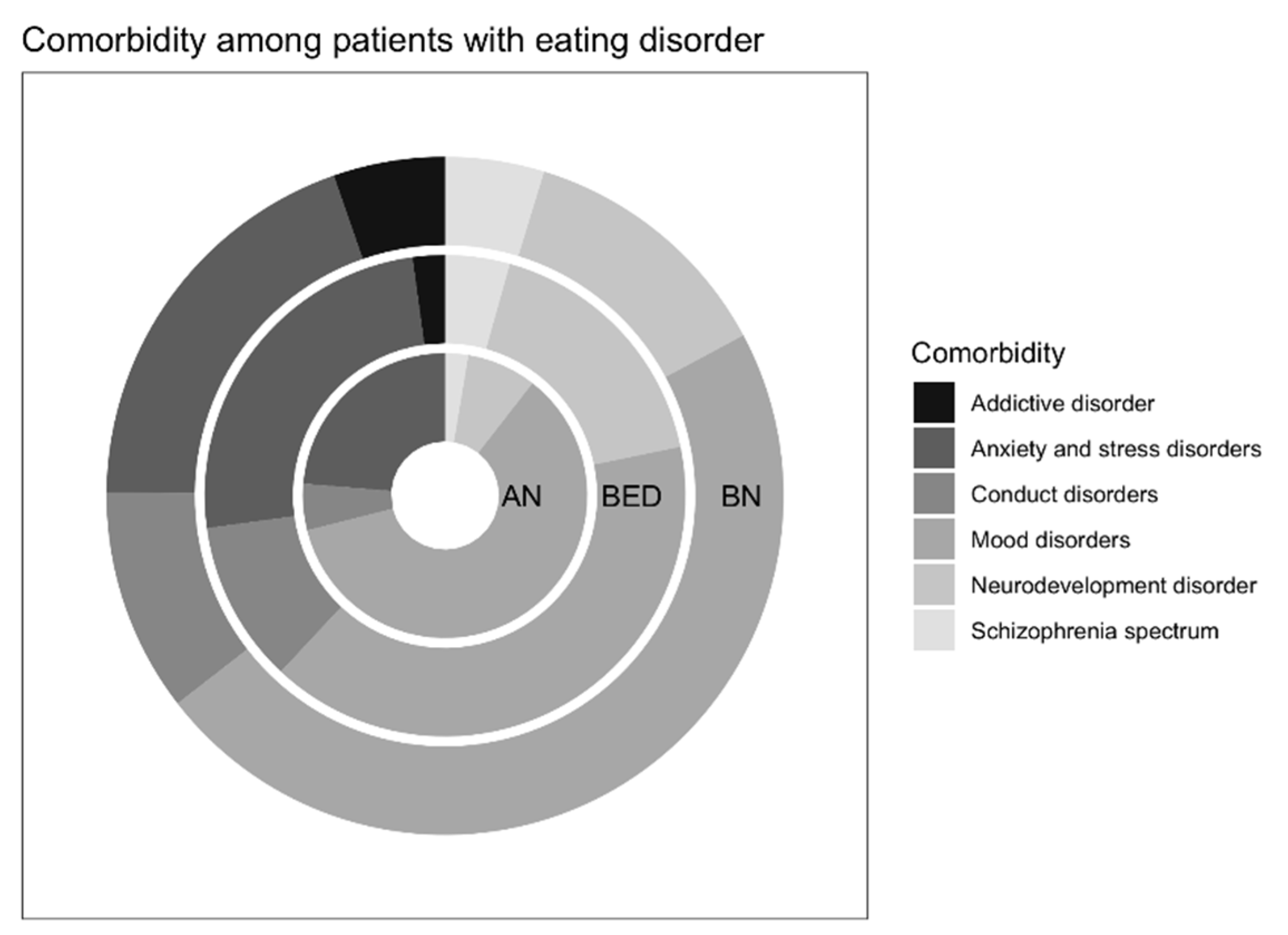
3.1. Major Depressive Disorder Was the Most Frequent Psychiatric Comorbidity
3.2. Prevalence of Psychiatric Disorders among Patients with EDs Is Higher Than the Reference Sample
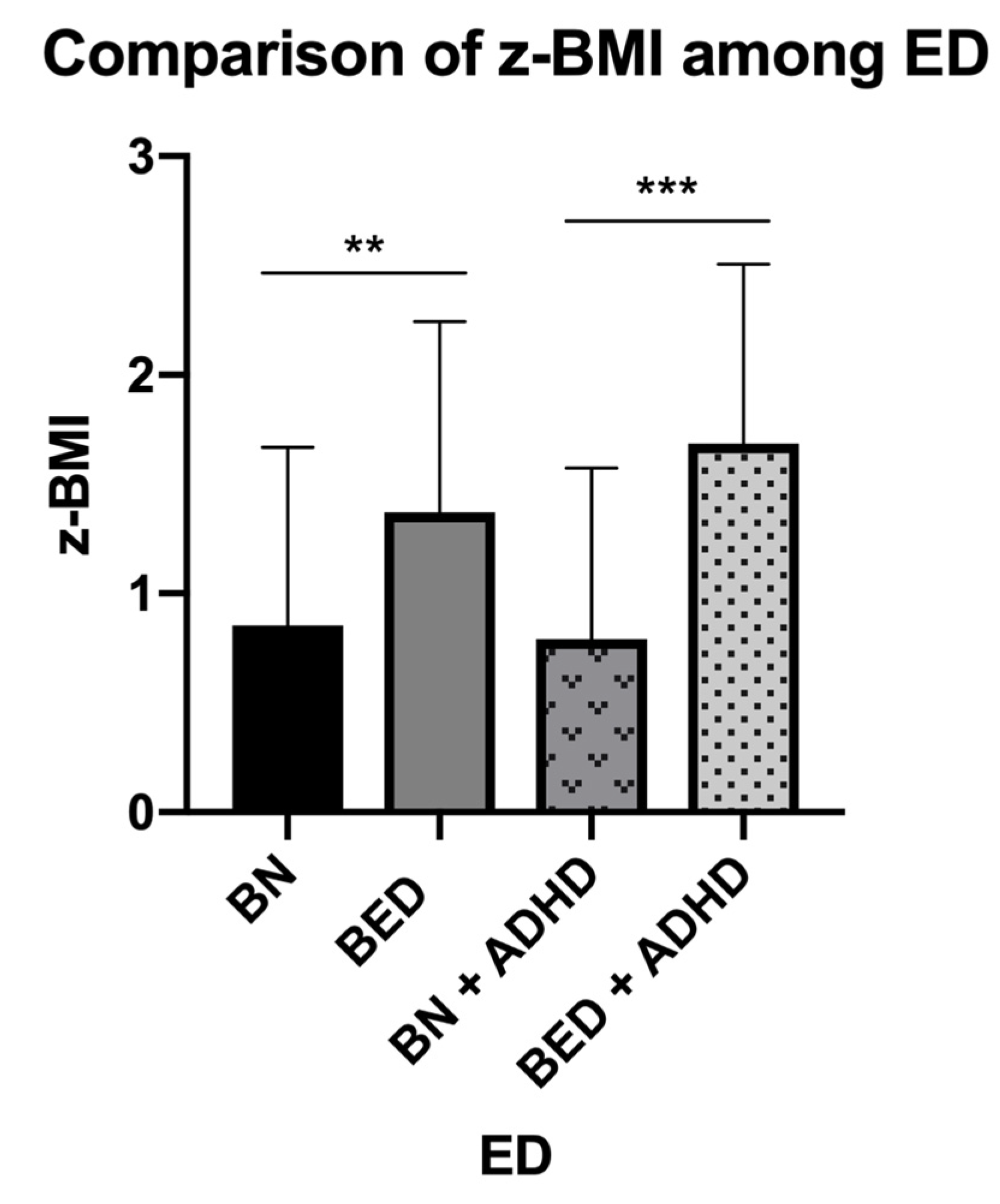
3.3. Attention-Deficit/Hyperactivity Disorder Prevalence Was Different between the Diagnosis of ED and It Is Associated with an Increased BMI in BED
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Brien, K.M.; Vincent, N.K. Psychiatric comorbidity in anorexia and bulimia nervosa: Nature, prevalence, and causal relationships. Clin. Psychol. Rev. 2003, 23, 57–74. [Google Scholar] [CrossRef]
- Hübel, C.; Marzi, S.J.; Breen, G.; Bulik, C.M. Epigenetics in eating disorders: A systematic review. Mol. Psychiatry 2019, 24, 901–915. [Google Scholar] [CrossRef]
- Herpertz-Dahlmann, B. Adolescent eating disorders: Update on definitions, symptomatology, epidemiology, and comorbidity. Child Adolesc. Psychiatr. Clin. N. Am. 2015, 24, 177–196. [Google Scholar] [CrossRef] [PubMed]
- Kolar, D.R.; Rodriguez, D.L.M.; Chams, M.M.; Hoek, H.W. Epidemiology of eating disorders in Latin America: A systematic review and meta-analysis. Curr. Opin. Psychiatry 2016, 29, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Himmerich, H.; Hotopf, M.; Shetty, H.; Schmidt, U.; Treasure, J.; Hayes, R.D.; Stewart, R.; Chang, C.-K. Psychiatric comorbidity as a risk factor for mortality in people with anorexia nervosa. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Smink, F.R.E.; van Hoeken, D.; Hoek, H.W. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Unikel, C.; Bojorquez, I. A review of eating disorders research in Mexico. Int. J. Psychol. 2007, 42, 59–68. [Google Scholar] [CrossRef]
- Villarejo, C.; Fernández-Aranda, F.; Jiménez-Murcia, S.; Peñas-Lledó, E.; Granero, R.; Penelo, E.; Tinahones, F.J.; Sancho, C.; Vilarrasa, N.; Montserrat-Gil de Bernabé, M.; et al. Lifetime obesity in patients with eating disorders: Increasing prevalence, clinical and personality correlates. Eur. Eat. Disord. Rev. 2012, 20, 250–254. [Google Scholar] [CrossRef] [Green Version]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Cigliobianco, M.; Paoli, R.A.; Caletti, E.; Mansur, R.; Zugno, E.; Prunas, C.; McIntyre, R.S. Possible association between social cognition and metabolic dysfunctions in Bipolar Disorder and Schizophrenia: Preliminary results. J. Affect. Disord. 2019, 246, 828–835. [Google Scholar] [CrossRef]
- Solmi, F.; Mascarell, M.C.; Zammit, S.; Kirkbride, J.B.; Lewis, G. Polygenic risk for schizophrenia, disordered eating behaviours and body mass index in adolescents. Braz. J. Psychiatry 2019, 215, 428–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vainik, U.; García-García, I.; Dagher, A. Uncontrolled eating: A unifying heritable trait linked with obesity, overeating, personality and the brain. Eur. J. Neuroscencei 2019, 50, 2430–2445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 68, 714–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alegria, M.; Woo, M.; Cao, Z.; Torres, M.; Meng, X.; Striegel-Moore, R. Prevalence and correlates of eating disorders in Latinos in the United States. Int. J. Eat. Disord. 2007, 40, S15–S21. [Google Scholar] [CrossRef]
- Unikel, C.; Root, T.; Vonholle, A.; Ocampo, R.; Bulik, C.M. Disordered eating and substance use among a female sample of Mexican adolescents. Subst. Use Misuse 2011, 46, 523–534. [Google Scholar] [CrossRef]
- Benjet, C.; Borges, G.; Medina-Mora, M.E.; Zambrano, J.; Aguilar-Gaxiola, S. Youth mental health in a populous city of the developing world: Results from the mexican adolescent mental health survey. J. Child Psychol. Psychiatry Allied Discip. 2009, 50, 386–395. [Google Scholar] [CrossRef]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®), 5th ed.; American Psychiatric Pub: Washigton, DC, USA, 2013. [Google Scholar]
- Sheehan, D.V.; Sheehan, K.H.; Shytle, R.D.; Janavs, J.; Bannon, Y.; Rogers, J.E.; Milo, K.M.; Stock, S.L.; Wilkinson, B. Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J. Clin. Psychiatry 2010, 71, 313–326. [Google Scholar] [CrossRef]
- Mestre, J.I.; Rossi, P.C.; Torrens, M. The Assessment Interview: A Review of Structured and Semi-structured Clinical Interviews Available for Use Among Hispanic Clients. In Guide to Psychological Assessment with Hispanics; Benuto, L.T., Ed.; Springer: Boston, MA, USA, 2013; pp. 33–48. [Google Scholar]
- Yanovski, S.Z.; Marcus, M.D.; Wadden, T.A.; Walsh, B.T. The Questionnaire on Eating and Weight Patterns-5: An updated screening instrument for binge eating disorder. Int. J. Eat. Disord. 2015, 48, 259–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tovilla-Zárate, C.; Juárez-Rojop, I.; Peralta Jimenez, Y.; Jiménez, M.A.; Vázquez, S.; Bermúdez-Ocaña, D.; Ramón-Frías, T.; Genis Mendoza, A.D.; García, S.P.; Narváez, L.L. Prevalence of anxiety and depression among outpatients with type 2 diabetes in the Mexican population. PLoS ONE 2012, 7, e36887. [Google Scholar] [CrossRef]
- Flegal, K.M.; Cole, T.J. Construction of LMS parameters for the Centers for Disease Control and Prevention 2000 growth charts. Natl. Health Stat. Rep. 2013, 63, 1–3. [Google Scholar]
- Hernández-Cordero, S.; Cuevas-Nasu, L.; Morán-Ruán, M.C.; Méndez-Gómez Humarán, I.; Ávila-Arcos, M.A.; Rivera-Dommarco, J.A. Overweight and obesity in Mexican children and adolescents during the last 25 years. Nutr. Diabetes 2017, 7, e247. [Google Scholar] [CrossRef] [Green Version]
- Högberg, C.; Billstedt, E.; Björck, C.; Björck, P.-O.; Ehlers, S.; Gustle, L.-H.; Hellner, C.; Höök, H.; Serlachius, E.; Svensson, M.A.; et al. Diagnostic validity of the MINI-KID disorder classifications in specialized child and adolescent psychiatric outpatient clinics in Sweden. BMC Psychiatry 2019, 19, 142. [Google Scholar] [CrossRef] [Green Version]
- De la Peña, O.; Esquivel, A.; Pérez, G.; Palacios, C. Validación Concurrente para Trastornos Externalizados del MINI-Kid y la Entrevista Se-miestructurada para Adolescentes. Revista Chilena de Psiquiatria y Neurologia de la Infancia y Adolescencia 2009, 20, 8–12. [Google Scholar]
- Spitzer, R.L.; Devlin, M.; Walsh, B.T.; Hasin, D.; Wing, R.; Marcus, M.; Stunkard, A.; Wadden, T.; Yanovski, S.; Agras, S.; et al. Binge eating disorder: A multisite field trial of the diagnostic criteria. Int. J. Eat. Disord. 1992, 11, 191–203. [Google Scholar] [CrossRef]
- Borges, M.B.F.; Morgan, C.M.; Claudino, A.M.; Silveira, D.X. da Validation of the portuguese version of the Questionnaire on Eating and Weight Patterns: Revised (QEWP-R) for the screening of binge eating disorder. Braz. J. Psychiatry 2005, 27, 319–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García Díaz, E.; Martín Folgueras, T.; Morcillo Herrera, L.; Jiménez Sosa, A. Diagnostic and psychopathologic evaluation of binge eating disorder in gastric bypass patients. Nutr. Hosp. 2012, 27, 553–557. [Google Scholar] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; 3.5.1; R Core Team: Vienna, Austria, 2018. [Google Scholar]
- Tsai, M.-C.; Gan, S.-T.; Lee, C.-T.; Liang, Y.-L.; Lee, L.-T.; Lin, S.-H. National population-based data on the incidence, prevalence, and psychiatric comorbidity of eating disorders in Taiwanese adolescents and young adults. Int. J. Eat. Disord. 2018, 51, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Ulfvebrand, S.; Birgegård, A.; Norring, C.; Högdahl, L.; von Hausswolff-Juhlin, Y. Psychiatric comorbidity in women and men with eating disorders results from a large clinical database. Psychiatry Res. 2015, 230, 294–299. [Google Scholar] [CrossRef]
- Lindstedt, K.; Kjellin, L.; Gustafsson, S.A. Adolescents with full or subthreshold anorexia nervosa in a naturalistic sample–characteristics and treatment outcome. J. Eat. Disord. 2017, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- Kostro, K.; Lerman, J.B.; Attia, E. The current status of suicide and self-injury in eating disorders: A narrative review. J. Eat. Disord. 2014, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Koutek, J.; Kocourkova, J.; Dudova, I. Suicidal behavior and self-harm in girls with eating disorders. Neuropsychiatr. Dis. Treat. 2016, 12, 787–793. [Google Scholar] [PubMed] [Green Version]
- Portzky, G.; van Heeringen, K.; Vervaet, M. Attempted suicide in patients with eating disorders. Crisis 2014, 35, 378–387. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Bruffaerts, R.; Demyttenaere, K.; Hwang, I.; Chiu, W.T.; Sampson, N.; Kessler, R.C.; Alonso, J.; Borges, G.; de Girolamo, G.; de Graaf, R.; et al. Treatment of suicidal people around the world. Braz. J. Psychiatry 2011, 199, 64–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Ramirez, S.; Mundo-Rosas, V.; Garcia-Guerra, A.; Shamah-Levy, T. Dietary patterns are associated with overweight and obesity in Mexican school-age children. Arch. Latinoam. Nutr. 2011, 61, 270–278. [Google Scholar] [PubMed]
- Santos, N.H.; Fiaccone, R.L.; Barreto, M.L.; Silva, L.A.; Silva Rde, C. Association between eating patterns and body mass index in a sample of children and adolescents in Northeastern Brazil. Cadernos de Saude Publica 2014, 30, 2235–2245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthoud, H.R.; Munzberg, H.; Morrison, C.D. Blaming the Brain for Obesity: Integration of Hedonic and Homeostatic Mechanisms. Gastroenterology 2017, 152, 1728–1738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steward, T.; Mestre-Bach, G.; Vintro-Alcaraz, C.; Aguera, Z.; Jimenez-Murcia, S.; Granero, R.; Fernandez-Aranda, F. Delay Discounting of Reward and Impulsivity in Eating Disorders: From Anorexia Nervosa to Binge Eating Disorder. Eur. Eat. Disord. Rev. 2017, 25, 601–606. [Google Scholar] [CrossRef]
- Kahnt, T. A decade of decoding reward-related fMRI signals and where we go from here. NeuroImage 2018, 180, 324–333. [Google Scholar] [CrossRef]
- Mitchell, M.R.; Potenza, M.N. Recent Insights into the Neurobiology of Impulsivity. Curr. Addict. Rep. 2014, 1, 309–319. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, B.; Touyz, S.; Hay, P.; Burton, A.; Russell, J.; Caterson, I. Neuroimaging in bulimia nervosa and binge eating disorder: A systematic review. J. Eat. Disord. 2018, 6, 3. [Google Scholar] [CrossRef]
- Frank, G.K. Advances from neuroimaging studies in eating disorders. CNS Spectr. 2015, 20, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Uhl, G.R.; Koob, G.F.; Cable, J. The neurobiology of addiction. Ann. N. Y. Acad. Sci. 2019, 1451, 5–28. [Google Scholar] [CrossRef]
- Brunault, P.; Frammery, J.; Montaudon, P.; De Luca, A.; Hankard, R.; Ducluzeau, P.H.; Cortese, S.; Ballon, N. Adulthood and childhood ADHD in patients consulting for obesity is associated with food addiction and binge eating, but not sleep apnea syndrome. Appetite 2019, 136, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Frayling, T.M.; Timpson, N.J.; Weedon, M.N.; Zeggini, E.; Freathy, R.M.; Lindgren, C.M.; Perry, J.R.; Elliott, K.S.; Lango, H.; Rayner, N.W.; et al. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science 2007, 316, 889–894. [Google Scholar] [CrossRef] [Green Version]
- Velders, F.P.; De Wit, J.E.; Jansen, P.W.; Jaddoe, V.W.; Hofman, A.; Verhulst, F.C.; Tiemeier, H. FTO at rs9939609, food responsiveness, emotional control and symptoms of ADHD in preschool children. PLoS ONE 2012, 7, e49131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, T.D.; Greene, B.H.; Bellodi, L.; Cavallini, M.C.; Cellini, E.; Di Bella, D.; Ehrlich, S.; Erzegovesi, S.; Estivill, X.; Fernandez-Aranda, F.; et al. Fat mass and obesity-associated gene (FTO) in eating disorders: Evidence for association of the rs9939609 obesity risk allele with bulimia nervosa and anorexia nervosa. Obes. Facts 2012, 5, 408–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellini, G.; Franzago, M.; Bagnoli, S.; Lelli, L.; Balsamo, M.; Mancini, M.; Nacmias, B.; Ricca, V.; Sorbi, S.; Antonucci, I.; et al. Fat mass and obesity-associated gene (FTO) is associated to eating disorders susceptibility and moderates the expression of psychopathological traits. PLoS ONE 2017, 12, e0173560. [Google Scholar] [CrossRef]
- Chuang, Y.F.; Tanaka, T.; Beason-Held, L.L.; An, Y.; Terracciano, A.; Sutin, A.R.; Kraut, M.; Singleton, A.B.; Resnick, S.M.; Thambisetty, M. FTO genotype and aging: Pleiotropic longitudinal effects on adiposity, brain function, impulsivity and diet. Mol. Psychiatry 2015, 20, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Sobczyk-Kopciol, A.; Broda, G.; Wojnar, M.; Kurjata, P.; Jakubczyk, A.; Klimkiewicz, A.; Ploski, R. Inverse association of the obesity predisposing FTO rs9939609 genotype with alcohol consumption and risk for alcohol dependence. Addiction 2011, 106, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Hanc, T.; Cortese, S. Attention deficit/hyperactivity-disorder and obesity: A review and model of current hypotheses explaining their comorbidity. Neurosci. Biobehav. Rev. 2018, 92, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Nazar, B.P.; Bernardes, C.; Peachey, G.; Sergeant, J.; Mattos, P.; Treasure, J. The risk of eating disorders comorbid with attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Int. J. Eat. Disord. 2016, 49, 1045–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymour, K.E.; Reinblatt, S.P.; Benson, L.; Carnell, S. Overlapping neurobehavioral circuits in ADHD, obesity, and binge eating: Evidence from neuroimaging research. CNS Spectr. 2015, 20, 401–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landau, Z.; Pinhas-Hamiel, O. Attention Deficit/Hyperactivity, the Metabolic Syndrome, and Type 2 Diabetes. Curr. Diabetes Rep. 2019, 19, 46. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Psychiatric Comorbidity | EDs n (%) | Reported Prevalence n (%) a | X2 | p-Value |
|---|---|---|---|---|
| Major depressive disorder | 98 (52.40) | 144 (4.79) | 562.85 | <0.001 |
| Dysthymic disorder | 42 (22.45) | 15 (0.49) | 484.09 | <0.001 |
| Hypomanic disorder | 3 (1.60) | 75 (2.49) | 0.58 | 0.620 |
| Suicide risk | 76 (40.64) | 214 (8.75) | 176.84 | <0.001 |
| Panic disorder | 9 (4.81) | 48 (1.59) | 10.37 | 0.004 |
| Agoraphobia | 9 (4.81) | 108 (3.59) | 0.43 | 0.500 |
| Separation anxiety disorder | 2 (1.06) | 78 (2.59) | 1.67 | 0.320 |
| Social phobia | 12 (6.41) | 336 (11.18) | 3.63 | 0.056 |
| Specific phobia | 19 (10.16) | 628 (20.89) | 11.90 | <0.001 |
| Generalized anxiety disorder | 33 (17.64) | 15 (0.49) | 349.50 | <0.001 |
| Obsessive-compulsive disorder | 3 (1.60) | - | - | - |
| Post-traumatic stress disorder | 6 (3.20) | 30 (0.99) | 7.71 | 0.010 |
| Adjustment disorder | 7 (3.74) | - | - | - |
| Alcohol use disorder | 3 (1.60) | 96 (3.19) | 1.48 | 0.200 |
| Substance use disorder (non-alcohol) | 10 (5.34) | 39 (1.29) | 19.10 | <0.001 |
| Conduct disorder | 11 (5.88) | 90 (2.99) | 3.89 | 0.040 |
| Oppositional defiant disorder | 26 (13.90) | 150 (4.99) | 25.15 | < 0.001 |
| TIC disorder | 4 (2.13) | - | - | - |
| Attention–deficit/hyperactivity disorder | 39 (20.85) b | 48 (1.59) | 239.05 | <0.001 |
| Psychotic disorder | 13 (6.95) | - | - | - |
| Psychiatric Comorbidity | AN n = 32 n (%) | BN n = 104 n (%) | BED n = 51 n (%) | X2 | p-Value |
|---|---|---|---|---|---|
| Mood disorders | 23 (71.88) | 80 (76.92) | 37 (72.55) | 0.53 | 0.767 |
| Major depressive disorder | 14 (43.75) | 55 (52.88) | 29 (56.86) | 1.37 | 0.502 |
| Dysthymic disorder | 8 (25.00) | 21 (20.19) | 13 (25.49) | 0.69 | 0.706 |
| Hypomanic disorder | 0 | 3 (2.88) | 0 | 2.43 | 0.745 |
| Suicide risk | 9 (28.13) | 47 (45.19) | 20 (39.22) | 3.01 | 0.221 |
| Anxiety and stressor related disorders | 9 (28.23) | 33 (31.73) | 23 (45.10) | 3.44 | 0.178 |
| Panic disorder | 1 (3.13) | 4 (3.85) | 4 (7.84) | 1.43 | 0.578 |
| Agoraphobia | 1 (3.13) | 4 (3.85) | 4 (7.84) | 1.43 | 0.578 |
| Separation anxiety disorder | 1 (3.13) | 1 (0.96) | 0 | 1.84 | 0.387 |
| Social phobia | 2 (6.25) | 6 (5.77) | 4 (7.84) | 0.24 | 0.917 |
| Specific phobia | 3 (9.38) | 13 (12.50) | 3 (5.88) | 1.66 | 0.452 |
| Generalized anxiety disorder | 4 (12.50) | 17 (16.35) | 12 (23.53) | 1.91 | 0.411 |
| Obsessive-compulsive disorder | 1 (3.13) | 2 (1.92) | 0 | 1.36 | 0.575 |
| Post-traumatic stress disorder | 1 (3.13) | 2 (1.92) | 3 (5.88) | 1.72 | 0.381 |
| Adjustment disorder | 0 | 2 (1.92) | 5 (9.80) | 7.39 | 0.042 |
| Substance-related and addictive disorders | 0 | 9 (8.65) | 2 (3.92) | 3.79 | 0.178 |
| Alcohol use disorder | 0 | 3 (2.88) | 0 | 2.43 | 0.745 |
| Substance use disorder (non-alcohol) | 0 | 8 (7.69) | 2 (3.92) | 3.14 | 0.232 |
| Disruptive, Impulse-control and conduct disorders | 2 (6.25) | 18 (17.31) | 10 (19.61) | 2.88 | 0.228 |
| Conduct disorder | 1 (3.13) | 7 (6.73) | 3 (5.88) | 0.57 | 0.913 |
| Oppositional defiant disorder | 2 (6.25) | 16 (15.38) | 8 (15.69) | 1.89 | 0.454 |
| Neurodevelopment disorders | 3 (9.38) | 21 (20.19) | 16 (31.37) | 5.85 | 0.058 |
| TIC disorder | 1 (3.13) | 1 (0.96) | 2 (3.92) | 1.61 | 0.284 |
| Attention–Deficit/hyperactivity disorder | 3 (9.38) | 20 (19.23) | 16 (31.37) | 6.13 | 0.046 |
| Psychotic disorder | 1 (3.13) | 8 (7.69) | 4 (7.84) | 0.87 | 0.791 |
| Bulimia Nervosa | Binge Eating Disorder | |||||
|---|---|---|---|---|---|---|
| BMI Diagnoses | No ADHD (n = 83) | ADHD (n = 20) | X2; p-Value | No ADHD (n = 35) | ADHD (n = 16) | X2; p-Value |
| Normal weight | 45 (54.22) | 13 (65.00) | 1.07; 0.586 | 8 (22.86) | 2 (12.50) | 6.00; 0.048 |
| Overweight | 17 (20.48) | 4 (20.00) | 11 (31.43) | 1 (6.25) | ||
| Obesity | 21 (25.30) | 3 (15.00) | 16 (45.71) | 13 (81.25) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Ramos, D.; Martínez-Magaña, J.J.; García, A.R.; Juarez-Rojop, I.E.; Gonzalez-Castro, T.B.; Tovilla-Zarate, C.A.; Sarmiento, E.; López-Narvaez, M.L.; Nicolini, H.; Genis-Mendoza, A.D. Psychiatric Comorbidity in Mexican Adolescents with a Diagnosis of Eating Disorders Its Relationship with the Body Mass Index. Int. J. Environ. Res. Public Health 2021, 18, 3900. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083900
Ruiz-Ramos D, Martínez-Magaña JJ, García AR, Juarez-Rojop IE, Gonzalez-Castro TB, Tovilla-Zarate CA, Sarmiento E, López-Narvaez ML, Nicolini H, Genis-Mendoza AD. Psychiatric Comorbidity in Mexican Adolescents with a Diagnosis of Eating Disorders Its Relationship with the Body Mass Index. International Journal of Environmental Research and Public Health. 2021; 18(8):3900. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083900
Chicago/Turabian StyleRuiz-Ramos, David, José Jaime Martínez-Magaña, Ana Rosa García, Isela Esther Juarez-Rojop, Thelma Beatriz Gonzalez-Castro, Carlos Alfonso Tovilla-Zarate, Emmanuel Sarmiento, María Lilia López-Narvaez, Humberto Nicolini, and Alma Delia Genis-Mendoza. 2021. "Psychiatric Comorbidity in Mexican Adolescents with a Diagnosis of Eating Disorders Its Relationship with the Body Mass Index" International Journal of Environmental Research and Public Health 18, no. 8: 3900. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083900