
Influence of Childhood Adversity and Infection on Timing of Menarche in a Multiethnic Sample of Women

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Characteristics | Excluded (N = 122) 1 | Included (N = 400) 1 | p-Value |
|---|---|---|---|
| Menarche (years), M (SD) | 12.85 (1.85) | 12.62 (1.94) | 0.2313 |
| Education, N (%) | |||
| Less than HS HS Graduate Some College Bachelor’s degree or higher | 32 (26.23) 27 (22.13) 27 (22.13) 36 (29.51) | 74 (18.50) 97 (24.25) 100 (25.00) 129 (32.25) | 0.325 |
| Race/Ethnicity, N (%) | |||
| Hispanic NH White NH Black NH Other | 89 (72.95) 14 (11.48) 13 (10.66) 6 (4.92) | 294 (73.50) 43 (10.75) 56 (14.00) 7 (1.75) | 0.203 |
| Nativity, N (%) | |||
| U.S.-born Foreign-born | 35 (28.69) 87 (71.31) | 135 (33.75) 265 (66.25) | 0.296 |
| Language dominance, N (%) | |||
| English Spanish | 52 (42.62) 70 (57.38) | 188 (47.00) 212 (53.00) | 0.396 |
| Childhood Adversity, Domains | β | 95% CI | Adjusted Mean Age |
|---|---|---|---|
| Neither | ref. | 13.3 | |
| Childhood maltreatment only | 0.13 | −0.69, 0.72 | 13.3 |
| Parental maladjustment only | −0.41 | −1.05, 0.23 | 12.9 |
| Both | −0.40 | −0.90, 0.11 | 12.9 |
| Childhood Adversity, Domains | RR | 95% CI |
|---|---|---|
| Neither | ref. | |
| Childhood maltreatment only | 0.78 | 0.42, 1.48 |
| Parental maladjustment only | 1.07 | 0.66, 1.74 |
| Both | 1.10 | 0.76, 1.60 |
References
- Ellis, B.J. Timing of pubertal maturation in girls: An integrated life history approach. Psychol. Bull. 2004, 130, 920–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herman-Giddens, M.E. The decline in the age of menarche in the United States: Should we be concerned? J. Adolesc. Health 2007, 40, 201–203. [Google Scholar] [CrossRef]
- McDonald, J.A.; Eng, S.M.; Dina, O.O.; Schooling, C.M.; Terry, M.B. Infection and pubertal timing: A systematic review. J. Dev. Orig. Health Dis. 2016, 7, 636–651. [Google Scholar] [CrossRef] [PubMed]
- Parent, A.S.; Teilmann, G.; Juul, A.; Skakkebaek, N.E.; Toppari, J.; Bourguignon, J.P. The timing of normal puberty and the age limits of sexual precocity: Variations around the world, secular trends, and changes after migration. Endocr. Rev. 2003, 24, 668–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, K.; Mouritsen, A.; Aksglaede, L.; Hagen, C.P.; Mogensen, S.S.; Juul, A. Recent secular trends in pubertal timing: Implications for evaluation and diagnosis of precocious puberty. Horm. Res. Paediatr. 2012, 77, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Biro, F.M.; Pajak, A.; Wolff, M.S.; Pinney, S.M.; Windham, G.C.; Galvez, M.P.; Greenspan, L.C.; Kushi, L.H.; Teitelbaum, S.L. Age of Menarche in a Longitudinal US Cohort. J. Pediatr. Adolesc. Gynecol. 2018, 31, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Beltz, A.M.; Corley, R.P.; Bricker, J.B.; Wadsworth, S.J.; Berenbaum, S.A. Modeling pubertal timing and tempo and examining links to behavior problems. Dev. Psychol. 2014, 50, 2715–2726. [Google Scholar] [CrossRef] [Green Version]
- Kaltiala-Heino, R.; Marttunen, M.; Rantanen, P.; Rimpela, M. Early puberty is associated with mental health problems in middle adolescence. Soc. Sci. Med. 2003, 57, 1055–1064. [Google Scholar] [CrossRef]
- Gallicchio, L.; Flaws, J.A.; Smith, R.L. Age at menarche, androgen concentrations, and midlife obesity: Findings from the Midlife Women’s Health Study. Menopause 2016, 23, 1182–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Li, L.; Millwood, I.Y.; Peters, S.A.E.; Chen, Y.; Guo, Y.; Bian, Z.; Chen, X.; Chen, L.; Feng, S.; et al. Age at menarche and risk of major cardiovascular diseases: Evidence of birth cohort effects from a prospective study of 300,000 Chinese women. Int. J. Cardiol. 2017, 227, 497–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertrand, K.A.; Gerlovin, H.; Bethea, T.N.; Palmer, J.R. Pubertal growth and adult height in relation to breast cancer risk in African American women. Int.J. Cancer 2017, 141, 2462–2470. [Google Scholar] [CrossRef]
- Ellis, B.J.; McFadyen-Ketchum, S.; Dodge, K.A.; Pettit, G.S.; Bates, J.E. Quality of early family relationships and individual differences in the timing of pubertal maturation in girls: A longitudinal test of an evolutionary model. J. Pers. Soc. Psychol. 1999, 77, 387–401. [Google Scholar] [CrossRef] [PubMed]
- Yermachenko, A.; Dvornyk, V. Nongenetic determinants of age at menarche: A systematic review. Biomed. Res. Int. 2014, 2014, 371583. [Google Scholar] [CrossRef]
- Webster, G.D.; Graber, J.A.; Gesselman, A.N.; Crosier, B.S.; Schember, T.O. A life history theory of father absence and menarche: A meta-analysis. Evol. Psychol. 2014, 12, 273–294. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Hussain, M.A.; Islam, S.; Mahumud, R.A.; Biswas, T.; Islam, S.M.S. Age at menarche and its socioeconomic determinants among female students in an urban area in Bangladesh. Sex. Reprod Healthc 2017, 12, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Houghton, L.C.; Cooper, G.D.; Booth, M.; Chowdhury, O.A.; Troisi, R.; Ziegler, R.G.; Katki, H.A.; Hoover, R.N.; Bentley, G.R. Childhood environment influences adrenarcheal timing among first-generation Bangladeshi migrant girls to the UK. PLoS ONE 2014, 9, e109200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slopen, N.; McLaughlin, K.A.; Dunn, E.C.; Koenen, K.C. Childhood adversity and cell-mediated immunity in young adulthood: Does type and timing matter? Brain Behav. Immun. 2013, 28, 63–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalmakis, K.A.; Chandler, G.E. Adverse childhood experiences: Towards a clear conceptual meaning. J. Adv. Nurs 2014, 70, 1489–1501. [Google Scholar] [CrossRef]
- Midei, A.J.; Matthews, K.A.; Chang, Y.F.; Bromberger, J.T. Childhood physical abuse is associated with incident metabolic syndrome in mid-life women. Health Psychol. 2013, 32, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Slopen, N.; Koenen, K.C.; Kubzansky, L.D. Cumulative adversity in childhood and emergent risk factors for long-term health. J. Pediatr. 2014, 164, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Suglia, S.F.; Koenen, K.C.; Boynton-Jarrett, R.; Chan, P.S.; Clark, C.J.; Danese, A.; Faith, M.S.; Goldstein, B.I.; Hayman, L.L.; Isasi, C.R.; et al. Childhood and Adolescent Adversity and Cardiometabolic Outcomes: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e15–e28. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.L.; Jerman, P.; Silverio Marques, S.; Koita, K.; Purewal Boparai, S.K.; Burke Harris, N.; Bucci, M. Systematic review of pediatric health outcomes associated with childhood adversity. BMC Pediatr. 2018, 18, 83. [Google Scholar] [CrossRef] [PubMed]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, D.; Sun, Y. Adverse Childhood Experiences and Early Pubertal Timing Among Girls: A Meta-Analysis. Int.J. Env. Res. Public Health 2019, 16, 2887. [Google Scholar] [CrossRef] [Green Version]
- Suglia, S.F.; Chen, C.; Wang, S.; Cammack, A.L.; April-Sanders, A.K.; McGlinchey, E.L.; Kubo, A.; Bird, H.; Canino, G.; Duarte, C.S. Childhood Adversity and Pubertal Development Among Puerto Rican Boys and Girls. Psychosom Med. 2020, 82, 487–494. [Google Scholar] [CrossRef]
- Biro, F.M.; McMahon, R.P.; Striegel-Moore, R.; Crawford, P.B.; Obarzanek, E.; Morrison, J.A.; Barton, B.A.; Falkner, F. Impact of timing of pubertal maturation on growth in black and white female adolescents: The National Heart, Lung, and Blood Institute Growth and Health Study. J. Pediatr. 2001, 138, 636–643. [Google Scholar] [CrossRef]
- Kaplowitz, P.B. Link between body fat and the timing of puberty. Pediatrics 2008, 121, S208–S217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y. Is obesity associated with early sexual maturation? A comparison of the association in American boys versus girls. Pediatrics 2002, 110, 903–910. [Google Scholar] [CrossRef] [Green Version]
- Kwok, M.K.; Leung, G.M.; Lam, T.H.; Schooling, C.M. Early life infections and onset of puberty: Evidence from Hong Kong’s children of 1997 birth cohort. Am. J. Epidemiol. 2011, 173, 1440–1452. [Google Scholar] [CrossRef]
- Carvalho-Queiroz, C.; Johansson, M.A.; Persson, J.O.; Jortso, E.; Kjerstadius, T.; Nilsson, C.; Saghafian-Hedengren, S.; Sverremark-Ekstrom, E. Associations between EBV and CMV Seropositivity, Early Exposures, and Gut Microbiota in a Prospective Birth Cohort: A 10-Year Follow-up. Front. Pediatr. 2016, 4, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochberg, Z.; Belsky, J. Evo-devo of human adolescence: Beyond disease models of early puberty. BMC Med. 2013, 11, 113. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, R.L.; Lee, I.; Shin, H.J.; He, J. Human adenovirus-36 antibody status is associated with obesity in children. Int.J. Pediatr. Obes. 2010, 5, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Sabin, M.A.; Burgner, D.; Atkinson, R.L.; Pei-Lun Lee, Z.; Magnussen, C.G.; Cheung, M.; Kahonen, M.; Lehtimaki, T.; Jokinen, E.; Laitinen, T.; et al. Longitudinal investigation of adenovirus 36 seropositivity and human obesity: The Cardiovascular Risk in Young Finns Study. Int.J. Obes. 2015, 39, 1644–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schooling, C.M.; Jones, H.E.; Leung, G.M. Lifecourse infectious origins of sexual inequalities in central adiposity. Int.J. Epidemiol. 2011, 40, 1556–1564. [Google Scholar] [CrossRef] [Green Version]
- Ferrand, R.A.; Bandason, T.; Musvaire, P.; Larke, N.; Nathoo, K.; Mujuru, H.; Ndhlovu, C.E.; Munyati, S.; Cowan, F.M.; Gibb, D.M.; et al. Causes of acute hospitalization in adolescence: Burden and spectrum of HIV-related morbidity in a country with an early-onset and severe HIV epidemic: A prospective survey. PLoS Med. 2010, 7, e1000178. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.F.; Tsai, W.Y.; Tung, Y.C.; Chen, H.L.; Ni, Y.H.; Hsu, H.Y.; Chang, M.H. Effect of menarche onset on the clinical course in females with chronic hepatitis B virus infection. J. Pediatr. 2014, 165, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.I. Vaccine Development for Epstein-Barr Virus. Adv. Exp. Med. Biol. 2018, 1045, 477–493. [Google Scholar] [CrossRef] [PubMed]
- Balfour, H.H., Jr.; Odumade, O.A.; Schmeling, D.O.; Mullan, B.D.; Ed, J.A.; Knight, J.A.; Vezina, H.E.; Thomas, W.; Hogquist, K.A. Behavioral, virologic, and immunologic factors associated with acquisition and severity of primary Epstein-Barr virus infection in university students. J. Infect. Dis. 2013, 207, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balfour, H.H., Jr. Epstein-Barr virus vaccine for the prevention of infectious mononucleosis--and what else? J. Infect. Dis. 2007, 196, 1724–1726. [Google Scholar] [CrossRef]
- Farahmand, M.; Monavari, S.H.; Shoja, Z.; Ghaffari, H.; Tavakoli, M.; Tavakoli, A. Epstein-Barr virus and risk of breast cancer: A systematic review and meta-analysis. Future Oncol. 2019, 15, 2873–2885. [Google Scholar] [CrossRef] [PubMed]
- Glaser, S.L.; Hsu, J.L.; Gulley, M.L. Epstein-Barr virus and breast cancer: State of the evidence for viral carcinogenesis. Cancer Epidemiol. Biomark. Prev. 2004, 13, 688–697. [Google Scholar]
- Richardson, A.K.; Currie, M.J.; Robinson, B.A.; Morrin, H.; Phung, Y.; Pearson, J.F.; Anderson, T.P.; Potter, J.D.; Walker, L.C. Cytomegalovirus and Epstein-Barr virus in breast cancer. PLoS ONE 2015, 10, e0118989. [Google Scholar] [CrossRef] [Green Version]
- Abbott, R.J.; Pachnio, A.; Pedroza-Pacheco, I.; Leese, A.M.; Begum, J.; Long, H.M.; Croom-Carter, D.; Stacey, A.; Moss, P.A.H.; Hislop, A.D.; et al. Asymptomatic Primary Infection with Epstein-Barr Virus: Observations on Young Adult Cases. J. Virol. 2017, 91, e00382-17. [Google Scholar] [CrossRef] [Green Version]
- Vestergaard, H.; Westergaard, T.; Wohlfahrt, J.; Hjalgrim, H.; Melbye, M. Tonsillitis, tonsillectomy and Hodgkin’s lymphoma. Int.J. Cancer 2010, 127, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Yasui, Y.; Potter, J.D.; Stanford, J.L.; Rossing, M.A.; Winget, M.D.; Bronner, M.; Daling, J. Breast cancer risk and "delayed" primary Epstein-Barr virus infection. Cancer Epidemiol. Biomark. Prev. 2001, 10, 9–16. [Google Scholar]
- Rostgaard, K.; Balfour, H.H., Jr.; Jarrett, R.; Erikstrup, C.; Pedersen, O.; Ullum, H.; Nielsen, L.P.; Voldstedlund, M.; Hjalgrim, H. Primary Epstein-Barr virus infection with and without infectious mononucleosis. PLoS ONE 2019, 14, e0226436. [Google Scholar] [CrossRef] [PubMed]
- Mersky, J.P.; Topitzes, J.; Reynolds, A.J. Impacts of adverse childhood experiences on health, mental health, and substance use in early adulthood: A cohort study of an urban, minority sample in the U.S. Child. Abus. Negl. 2013, 37, 917–925. [Google Scholar] [CrossRef] [Green Version]
- Sameroff, A.J.; Bartko, W.T.; Baldwin, A.; Baldwin, C.; Seifer, R. Family and social influences on the development of child competence. In Families, Risk, and Competence; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1998; pp. 161–185. [Google Scholar]
- Urayama, K.Y.; Ma, X.; Selvin, S.; Metayer, C.; Chokkalingam, A.P.; Wiemels, J.L.; Does, M.; Chang, J.; Wong, A.; Trachtenberg, E.; et al. Early life exposure to infections and risk of childhood acute lymphoblastic leukemia. Int.J. Cancer 2011, 128, 1632–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akinbami, L.J.; Moorman, J.E.; Garbe, P.L.; Sondik, E.J. Status of childhood asthma in the United States, 1980–2007. Pediatrics 2009, 123, S131–S145. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, S.H.; Shrestha, S.; Bjerregaard, L.G.; Angquist, L.H.; Baker, J.L.; Jess, T.; Allin, K.H. Antibiotic exposure in early life and childhood overweight and obesity: A systematic review and meta-analysis. Diabetes Obes. Metab. 2018, 20, 1508–1514. [Google Scholar] [CrossRef]
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int.J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef]
- Rodriguez, C.B.; Wei, Y.; Terry, M.B.; Wyka, K.; Athilat, S.; Albrecht, S.S.; Tehranifar, P. Associations of Nativity, Age at Migration, and Percent of Life in the U.S. with Midlife Body Mass Index and Waist Size in New York City Latinas. Int.J. Environ. Res. Public Health 2020, 17, 2436. [Google Scholar] [CrossRef] [Green Version]
- Tehranifar, P.; Rodriguez, C.B.; April-Sanders, A.K.; Desperito, E.; Schmitt, K.M. Migration History, Language Acculturation, and Mammographic Breast Density. Cancer Epidemiol. Biomark. Prev. 2018, 27, 566–574. [Google Scholar] [CrossRef] [Green Version]
- Appleton, A.A.; Holdsworth, E.; Ryan, M.; Tracy, M. Measuring Childhood Adversity in Life Course Cardiovascular Research: A Systematic Review. Psychosom Med. 2017, 79, 434–440. [Google Scholar] [CrossRef]
- Dias, E.P.; Rocha, M.L.; Carvalho, M.O.; Amorim, L.M. Detection of Epstein-Barr virus in recurrent tonsillitis. Braz. J. Otorhinolaryngol. 2009, 75, 30–34. [Google Scholar] [CrossRef] [Green Version]
- Hislop, A.D.; Kuo, M.; Drake-Lee, A.B.; Akbar, A.N.; Bergler, W.; Hammerschmitt, N.; Khan, N.; Palendira, U.; Leese, A.M.; Timms, J.M.; et al. Tonsillar homing of Epstein-Barr virus-specific CD8+ T cells and the virus-host balance. J. Clin. Investig. 2005, 115, 2546–2555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, N.; Kiang, M.V.; Kosheleva, A.; Waterman, P.D.; Chen, J.T.; Beckfield, J. Age at menarche: 50-year socioeconomic trends among US-born black and white women. Am. J. Public Health 2015, 105, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Belsky, J.; Steinberg, L.D.; Houts, R.M.; Friedman, S.L.; DeHart, G.; Cauffman, E.; Roisman, G.I.; Halpern-Felsher, B.L.; Susman, E.; NICHD Early Child Care Research Network. Family rearing antecedents of pubertal timing. Child. Dev. 2007, 78, 1302–1321. [Google Scholar] [CrossRef]
- Chisholm, J.S.; Quinlivan, J.A.; Petersen, R.W.; Coall, D.A. Early stress predicts age at menarche and first birth, adult attachment, and expected lifespan. Hum. Nat. 2005, 16, 233–265. [Google Scholar] [CrossRef] [PubMed]
- Epel, E.S. Psychological and metabolic stress: A recipe for accelerated cellular aging? Hormones 2009, 8, 7–22. [Google Scholar] [CrossRef]
- Carpenter, L.L.; Carvalho, J.P.; Tyrka, A.R.; Wier, L.M.; Mello, A.F.; Mello, M.F.; Anderson, G.M.; Wilkinson, C.W.; Price, L.H. Decreased adrenocorticotropic hormone and cortisol responses to stress in healthy adults reporting significant childhood maltreatment. Biol. Psychiatry 2007, 62, 1080–1087. [Google Scholar] [CrossRef] [Green Version]
- Elzinga, B.M.; Roelofs, K.; Tollenaar, M.S.; Bakvis, P.; van Pelt, J.; Spinhoven, P. Diminished cortisol responses to psychosocial stress associated with lifetime adverse events a study among healthy young subjects. Psychoneuroendocrinology 2008, 33, 227–237. [Google Scholar] [CrossRef]
- Negriff, S.; Saxbe, D.E.; Trickett, P.K. Childhood maltreatment, pubertal development, HPA axis functioning, and psychosocial outcomes: An integrative biopsychosocial model. Dev. Psychobiol. 2015, 57, 984–993. [Google Scholar] [CrossRef] [PubMed]
- Culpin, I.; Heron, J.; Araya, R.; Melotti, R.; Lewis, G.; Joinson, C. Father absence and timing of menarche in adolescent girls from a UK cohort: The mediating role of maternal depression and major financial problems. J. Adolesc. 2014, 37, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Ellis, B.J.; Garber, J. Psychosocial antecedents of variation in girls’ pubertal timing: Maternal depression, stepfather presence, and marital and family stress. Child. Dev. 2000, 71, 485–501. [Google Scholar] [CrossRef]
- Henrichs, K.L.; McCauley, H.L.; Miller, E.; Styne, D.M.; Saito, N.; Breslau, J. Early menarche and childhood adversities in a nationally representative sample. Int.J. Pediatr. Endocrinol. 2014, 2014, 14. [Google Scholar] [CrossRef] [Green Version]
- Toromanovic, A.; Tahirovic, H.; Collaborators from pediatric centers in Federation of Bosnia and Herzegovina. Effect of family disintegration on age at menarche. Acta Med. Acad. 2015, 44, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Bleil, M.E.; Adler, N.E.; Appelhans, B.M.; Gregorich, S.E.; Sternfeld, B.; Cedars, M.I. Childhood adversity and pubertal timing: Understanding the origins of adulthood cardiovascular risk. Biol. Psychol. 2013, 93, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henrich, J.; Heine, S.J.; Norenzayan, A. The weirdest people in the world? Behav. Brain Sci. 2010, 33, 61–83, discussion 83–135. [Google Scholar] [CrossRef] [PubMed]
- Magnus, M.C.; Anderson, E.L.; Howe, L.D.; Joinson, C.J.; Penton-Voak, I.S.; Fraser, A. Childhood psychosocial adversity and female reproductive timing: A cohort study of the ALSPAC mothers. J. Epidemiol. Community Health 2018, 72, 34–40. [Google Scholar] [CrossRef]
- Mendle, J.; Turkheimer, E.; D’Onofrio, B.M.; Lynch, S.K.; Emery, R.E.; Slutske, W.S.; Martin, N.G. Family structure and age at menarche: A children-of-twins approach. Dev. Psychol. 2006, 42, 533–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moffitt, T.E.; Caspi, A.; Belsky, J.; Silva, P.A. Childhood experience and the onset of menarche: A test of a sociobiological model. Child. Dev. 1992, 63, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Boynton-Jarrett, R.; Harville, E.W. A prospective study of childhood social hardships and age at menarche. Ann. Epidemiol. 2012, 22, 731–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boynton-Jarrett, R.; Wright, R.J.; Putnam, F.W.; Lividoti Hibert, E.; Michels, K.B.; Forman, M.R.; Rich-Edwards, J. Childhood abuse and age at menarche. J. Adolesc. Health 2013, 52, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Merrick, M.T.; Ford, D.C.; Ports, K.A.; Guinn, A.S. Prevalence of Adverse Childhood Experiences From the 2011-2014 Behavioral Risk Factor Surveillance System in 23 States. JAMA Pediatr. 2018, 172, 1038–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okasha, M.; McCarron, P.; Smith, G.D.; McEwen, J. Age at menarche: Secular trends and association with adult anthropometric measures. Ann. Hum. Biol. 2001, 28, 68–78. [Google Scholar] [PubMed]
- Hauspie, R.C.; Vercauteren, M.; Susanne, C. Secular changes in growth and maturation: An update. Acta Paediatr. Suppl. 1997, 423, 20–27. [Google Scholar] [CrossRef]
- Hokken-Koelega, A.C. Timing of puberty and fetal growth. Best Pract. Res. Clin. Endocrinol. Metab. 2002, 16, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, S.J.; Jorgensen, T.; Andersen, L.P.; Bonnevie, O. Association of Helicobacter pylori infection with lifestyle, chronic disease, body-indices, and age at menarche in Danish adults. Scand. J. Public Health 2000, 28, 32–40. [Google Scholar] [CrossRef]
- McDonald, J.A.; Cherubin, S.; Goldberg, M.; Wei, Y.; Chung, W.K.; Schwartz, L.A.; Knight, J.A.; Schooling, C.M.; Santella, R.M.; Bradbury, A.R.; et al. Common Childhood Viruses and Pubertal Timing: The LEGACY Girls Study. Am. J. Epidemiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Munoz, M.E.; Fuentes-Panana, E.M. Beta and Gamma Human Herpesviruses: Agonistic and Antagonistic Interactions with the Host Immune System. Front. Microbiol. 2017, 8, 2521. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, G.C.; Krajewski, A.S.; Crawford, D.H. The ins and outs of EBV infection. Trends Microbiol. 2000, 8, 185–189. [Google Scholar] [CrossRef]
- Georgalas, C.C.; Tolley, N.S.; Narula, P.A. Tonsillitis. BMJ Clin. Evid. 2014, 2014, 0503. [Google Scholar] [PubMed]
- Must, A.; Phillips, S.M.; Naumova, E.N.; Blum, M.; Harris, S.; Dawson-Hughes, B.; Rand, W.M. Recall of early menstrual history and menarcheal body size: After 30 years, how well do women remember? Am. J. Epidemiol. 2002, 155, 672–679. [Google Scholar] [CrossRef] [PubMed]


| Characteristics | All 400 | Early Menarche 124 | Average/Late Menarche 276 | p-Value |
|---|---|---|---|---|
| Age, M (SD) | 51.5 (5.6) | 51.5 (5.4) | 51.5 (5.7) | 0.9770 |
| Race/ethnicity, N (%) | 0.2033 | |||
| Hispanic | 294 (73.5) | 96 (77.4) | 198 (71.7) | |
| Non-Hispanic White | 43 (10.8) | 8 (6.5) | 35 (12.7) | |
| Non-Hispanic Black | 56 (14.0) | 19 (15.3) | 37 (13.4) | |
| Other 2 | 7 (1.8) | 1 (0.8) | 6 (2.2) | |
| Education, N (%) | 0.0669 | |||
| Less than high school | 74 (18.5) | 15 (12.1) | 59 (21.4) | |
| High school graduate | 97 (24.3) | 35 (28.2) | 62 (22.5) | |
| Some college | 100 (25.0) | 37 (29.8) | 63 (22.8) | |
| Bachelor’s or higher degree | 129 (32.3) | 37 (29.8) | 92 (33.3) | |
| Nativity, N (%) | 0.1021 | |||
| U.S.-born | 135 (33.8) | 49 (39.5) | 86 (31.2) | |
| Foreign-born | 265 (66.3) | 75 (60.5) | 190 (68.8) | |
| Language dominance, N (%) | 0.3066 | |||
| English | 188 (47.0) | 63 (50.8) | 125 (45.3) | |
| Spanish | 212 (53.0) | 61 (49.2) | 151 (54.7) | |
| Menarche (years), M (SD) | 12.6 (1.9) | 10.4 (0.9) | 13.6 (1.4) | <0.0001 |
| Cumulative childhood adversities, N (%) | 343 (85.8) | 106 (30.9) | 237 (69.1) | 0.7301 |
| None | 176 (51.3) | 54 (50.9) | 122 (51.5) | |
| 1 | 56 (16.3) | 17 (16.0) | 39 (16.5) | |
| 2 | 47 (13.7) | 15 (14.2) | 32 (13.5) | |
| 3 | 30 (8.8) | 11 (10.4) | 19 (8.0) | |
| 4 | 16 (4.7) | 3 (2.8) | 13 (5.5) | |
| 5 | 11 (3.2) | 5 (4.7) | 6 (2.5) | |
| 6 | 7 (2.0) | 1 (0.9) | 6 (2.5) | |
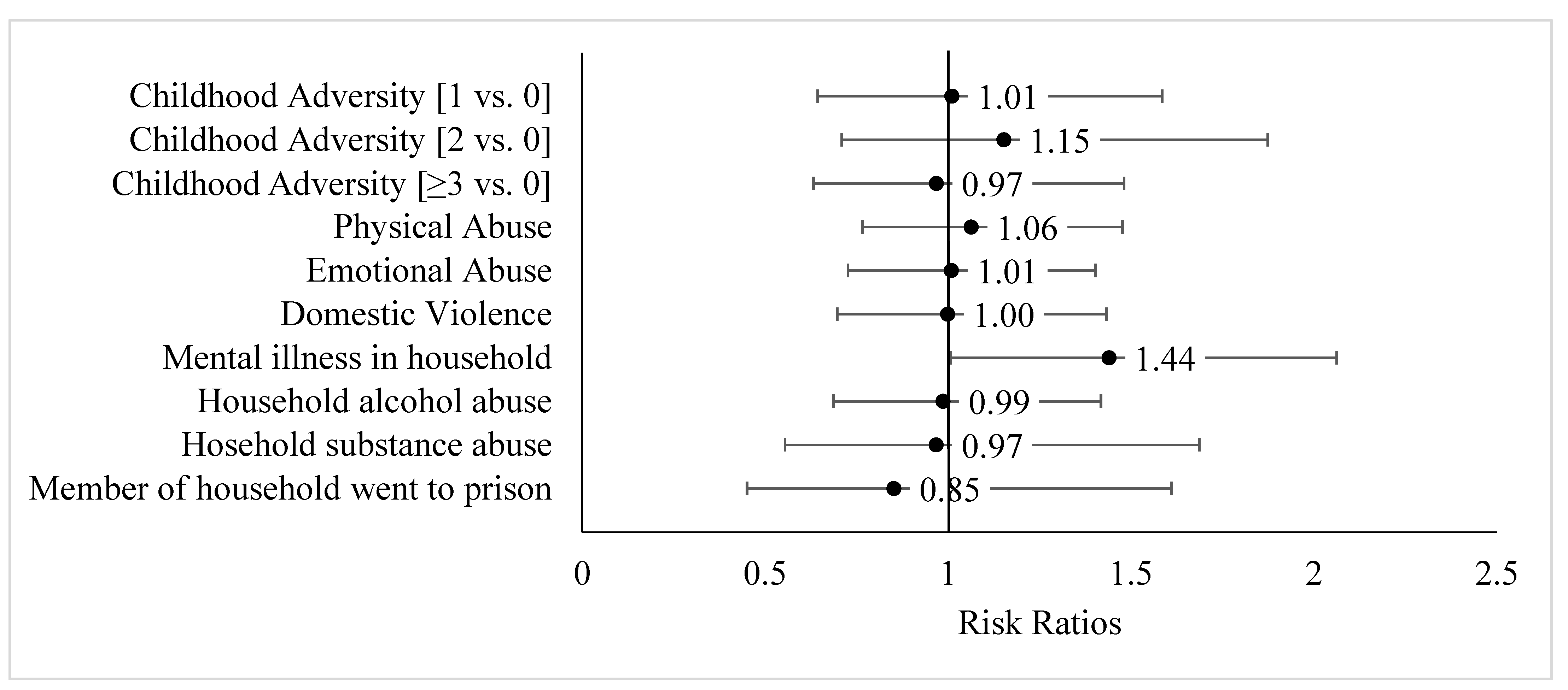
| Indicators of childhood adversity, N (%) | ||||
| Domain: Childhood maltreatment | ||||
| Physical abuse | 96 (24.0) | 31 (25.0) | 65 (23.6) | 0.7389 |
| Emotional abuse | 118 (29.3) | 36 (29.0) | 81 (29.4) | 0.9634 |
| Domain: Parental maladjustment | ||||
| Domestic violence | 76 (19.0) | 25 (20.2) | 51 (18.5) | 0.6884 |
| Mental illness in household | 57 (14.3) | 23 (18.6) | 34 (12.3) | 0.1242 |
| Household alcohol abuse | 82 (20.5) | 26 (21.0) | 56 (20.3) | 0.8914 |
| Household substance abuse | 28 (7.0) | 9 (7.3) | 19 (6.9) | 0.8243 |
| Member of household went to prison | 23 (5.8) | 7 (5.7) | 16 (5.8) | 0.9731 |
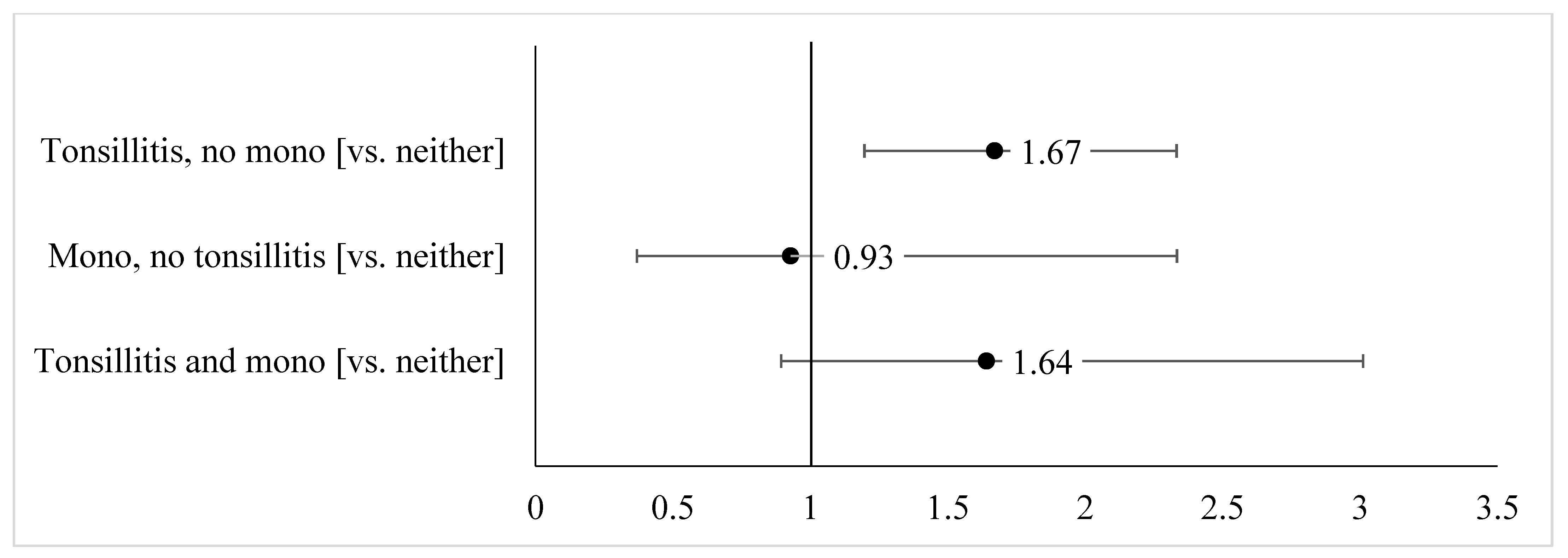
| Infection history, N (%) | 0.0283 | |||
| Tonsillitis only | 66 (16.5) | 30 (24.2) | 36 (13.0) | |
| Mono only | 19 (4.8) | 4 (3.2) | 15 (5.4) | |
| Both tonsillitis and mono | 19 (4.8) | 8 (6.5) | 11 (4.0) | |
| Neither tonsillitis nor mono | 248 (62.0) | 70 (56.5) | 178 (64.5) |
| Childhood Adversities, Cumulative | β | 95% CI | Adjusted Mean Age | |
| No childhood adversity | ref. | 13.3 | ||
| 1 childhood adversity | −0.27 | −0.85, 0.32 | 13.1 | |
| 2 childhood adversities | −0.37 | −1.01, 0.28 | 13.0 | |
| ≥3 childhood adversities | −0.33 | −0.89, 0.23 | 13.0 | |
| Childhood Adversities, Individual | β | 95% CI | Adjusted Mean Age | |
| Physical abuse | Yes | −0.29 | −0.74, 0.16 | 12.9 |
| No | ref. | 13.2 | ||
| Emotional abuse | Yes | −0.17 | −0.59, 0.25 | 13.0 |
| No | ref. | 13.2 | ||
| Domestic violence | Yes | −0.19 | −0.68, 0.30 | 13.0 |
| No | ref. | 13.2 | ||
| Mental illness in household | Yes | −0.59 | −1.15, −0.02 | 12.7 |
| No | ref. | 13.2 | ||
| Household alcohol abuse | Yes | −0.03 | −0.50, 0.45 | 13.1 |
| No | ref. | 13.1 | ||
| Household substance abuse | Yes | −0.13 | −0.87, 0.62 | 13.0 |
| No | ref. | 13.2 | ||
| Member of household went to prison | Yes | 0.25 | −0.58, 1.08 | 13.4 |
| No | ref. | 13.1 | ||
| Childhood Infections, Cumulative | β | 95% CI | Adjusted Mean Age |
|---|---|---|---|
| Neither tonsillitis nor mono | ref. | 13.2 | |
| Tonsillitis, no mono | −0.73 | −1.26, −0.20 | 12.5 |
| Mono, no tonsillitis | 0.22 | −0.69, 1.16 | 13.4 |
| Tonsillitis and mono | 0.45 | −0.44, 1.34 | 13.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
April-Sanders, A.K.; Tehranifar, P.; Argov, E.L.; Suglia, S.F.; Rodriguez, C.B.; McDonald, J.A. Influence of Childhood Adversity and Infection on Timing of Menarche in a Multiethnic Sample of Women. Int. J. Environ. Res. Public Health 2021, 18, 4080. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084080
April-Sanders AK, Tehranifar P, Argov EL, Suglia SF, Rodriguez CB, McDonald JA. Influence of Childhood Adversity and Infection on Timing of Menarche in a Multiethnic Sample of Women. International Journal of Environmental Research and Public Health. 2021; 18(8):4080. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084080
Chicago/Turabian StyleApril-Sanders, Ayana K., Parisa Tehranifar, Erica Lee Argov, Shakira F. Suglia, Carmen B. Rodriguez, and Jasmine A. McDonald. 2021. "Influence of Childhood Adversity and Infection on Timing of Menarche in a Multiethnic Sample of Women" International Journal of Environmental Research and Public Health 18, no. 8: 4080. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084080