
Factors Associated with the Implementation of Non-Pharmaceutical Interventions for Reducing Coronavirus Disease 2019 (COVID-19): A Systematic Review


Abstract
:1. Introduction
Research Question (RQ)
2. Materials and Methods
2.1. Criteria for Considering Studies for the Study
- Types of participants: all studies that involve human subjects of any age or gender, including ethnic (Black, Asian, White) and healthcare worker (medical doctors, nurses, allied healthcare professions) groups.
- Types of intervention: research describing three major NPIs, e.g., social distance, isolation and quarantine, focusing only on COVID-19/SARS-CoV-2.
- Types of outcome measure: primary outcomes include: COVID-19; reducing the risk of transmission/infection of COVID-19; secondary outcomes include changes in social behaviour, for example, SD by avoiding crowds, restricting movements, isolating ill patients and quarantine of exposed people.
- Types of studies: no study design filter is added. To measure the impact of NPIs, this review considered all studies evaluating the effectiveness of NPIs relating to reducing the risk of transmission/infection of COVID-19. We included both RCTs and non-RCTs, for example, cross-sectional, survey, case-control, RCTs and observational studies (retrospective or prospective) including preprint engines such as medRxiv, bioRxiv, Litcovid and SSRN for unpublished studies on COVID-19, given the lags in publication.
- Study period: December 2019 to March 2021.
- Articles published in narrative review, modelling studies, opinions, letters, news, editorials, perspectives, commentaries and any other publications lacking primary data, including grey literature.
- Studies containing duplicate datasets.
2.2. Search Strategy
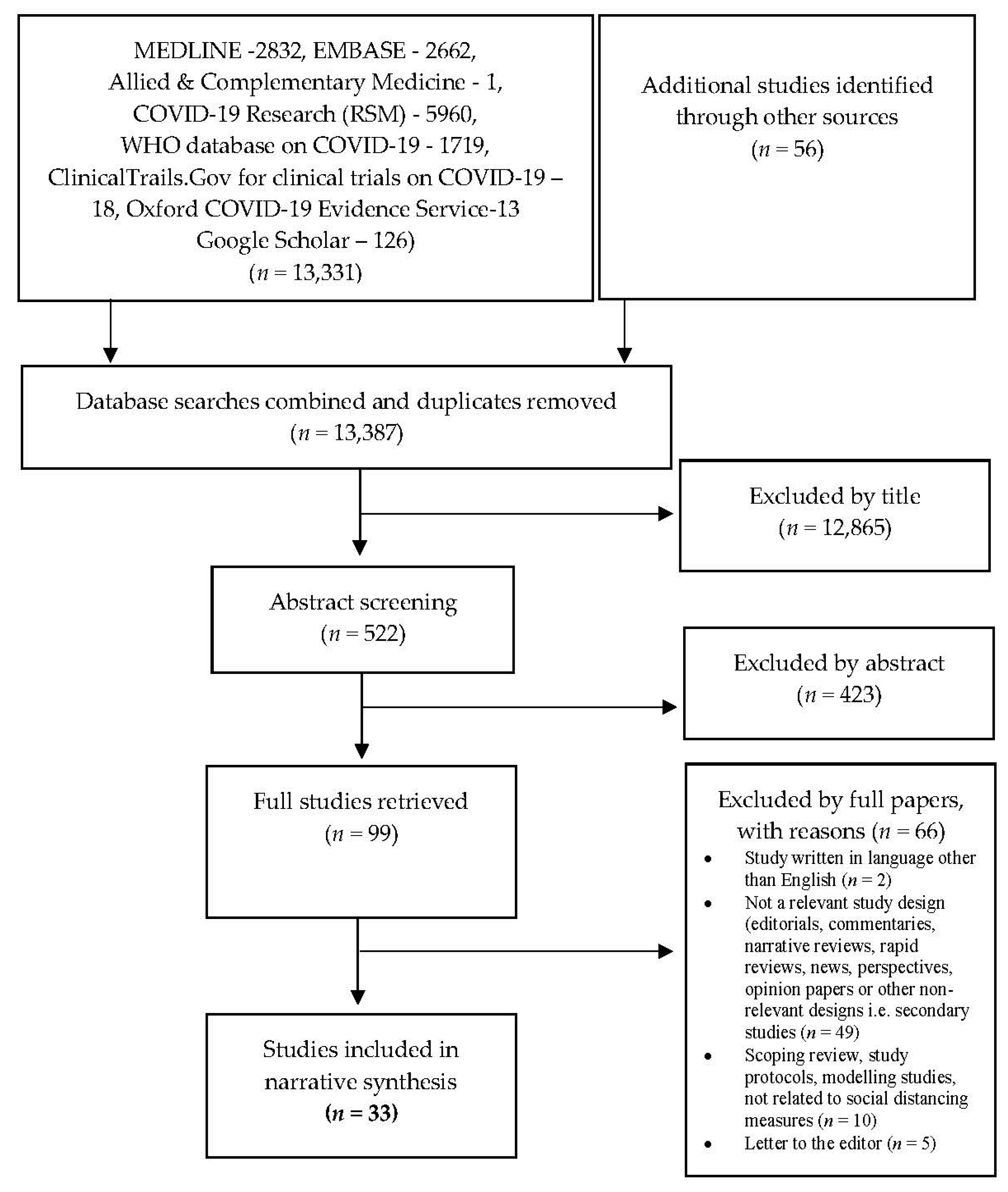
2.3. Selection of Studies
2.4. Data Extraction, Analysis and Synthesis
2.5. Quality Appraisal (Risk of Bias)
3. Results
3.1. Study Characteristics
3.2. Risk of Bias
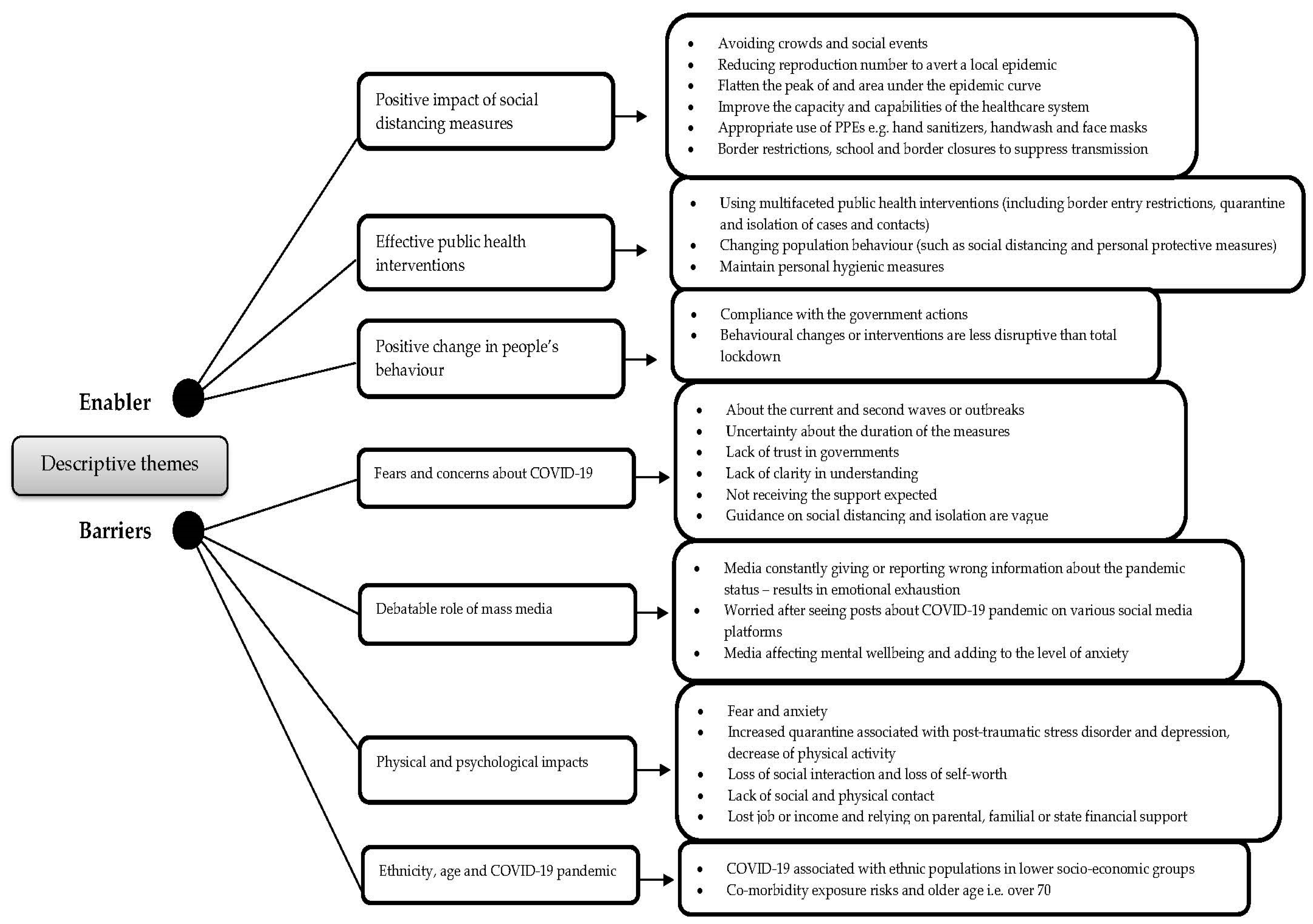
3.3. Synthesis of Results
- Theme 1. Positive impact of SD measures.
- Theme 2. Effective public health interventions.
- Theme 3. Positive changes in people’s behaviour.
- Theme 4. Fears and concerns about COVID-19.
- Theme 5. Debatable role of mass media.
- Theme 6. Physical and psychological impacts.
- Theme 7. Ethnicity, age and COVID-19 pandemic.
3.4. Enablers
3.4.1. Theme 1. Positive Impact of SD Measures
- Without strengthening SDMs, local infections are likely to continue occurring, given that the effective reproduction number (R0) is approximately 1 or slightly higher. Travel measures and testing, tracing, and treating efforts are particularly important in maintaining suppression, although these measures will be increasingly difficult to implement as case numbers increase [66].
3.4.2. Theme 2. Effective Public Health Interventions
- The package of public health interventions (including border entry restrictions, quarantine and isolation of cases and contacts, and population behaviour changes, such as social distancing and personal protective measures) that Hong Kong has implemented since late January 2020, is associated with reduced spread of COVID-19 [66].
- The study participants reported frequent use of sanitisers, hand wash, and masks during the past week. This indicates participants’ increasing concern towards personal hygienic measures. Awareness about COVID-19 is reflected in behaviour and attitude as most participants agreed with social distancing, avoiding travel, self-quarantine and adequate hygiene [68].
3.4.3. Theme 3. Positive Changes in People’s Behaviour
- Social distancing and population behavioural changes with social and economic impacts less disruptive than total lockdown can meaningfully control COVID-19. Control measures and changes in population behaviour coincided with a substantial reduction in influenza transmission in early February 2020. This observation suggests the same measures would also have affected COVID-19 transmission in the community, because of some similarities, as well as differences, in the modes of transmission of influenza and COVID-19 [66].
- Avoiding close contact, washing hands and wearing facial masks were considered the most protective measures [77].
- Hand hygiene is a major element in the prevention of COVID-19 and other infectious disease [90].
3.5. Barriers
3.5.1. Theme 4. Fears and Concerns about COVID-19
- Overall, 77.4% (1640/2108) of respondents reported being worried about COVID-19 in the UK. For those not previously testing positive for COVID-19, 47.5% (979/2108) believed it was likely they would be infected at some point in the future under the UK Government’s preventive measures. If infected, just over half (56.9%) would expect to be moderately/severely affected (e.g., may need self-care and rest in bed) [65].
- People are very worried and are not willing to go to health facilities even if they have general problems. They used to contact health personnel through phone calls, but they were not willing to visit any health centres due to fear of getting COVID-19 from health workers. Fear of transmission was pervasive among health workers as well [90].
- The analysis of contact characteristics showed that the incidence rate of close contacts who lived in the same residence was 17.9%, significantly higher than those of other groups with different forms of contact. The incidence rate of relatives was 10.7%, with the highest risk of infection among all relationship groups. The results showed that the closer the contact distance and the higher the frequency of contact, the greater the risk of infection [72].
- Most participants felt that guidance on social distancing and isolation had been generally unclear, although some described how it had “become clearer”. Many participants exhibited lack of trust in government or in the media [88].
- One study has highlighted the implication of health systems:
- The weak infrastructure, under-resourced health system, widespread of the illiteracy and social practices will negatively influence the spread of the COVID-19 and response towards its prevention [89].
3.5.2. Theme 5. Debatable Role of Mass Media
- Approximately 28% of people report sleep difficulties. More than two-thirds of participants reported themselves worried after seeing posts about COVID-19 on social media [69].
- Approximately 46% of participants reported worry regarding discussion of COVID-19 in news channels and print media. This indicates a significant proportion of survey participants, despite having adequate awareness about coronavirus infection, are largely influenced by media information. Media influences mental wellbeing and adds to anxiety levels [69].
3.5.3. Theme 6. Physical and Psychological Impacts
- The mandated lack of social and, especially, physical contact with family members were identified as particularly difficult. Confinement at home and work, being unable to see friends, being unable to shop for basic necessities of everyday life, and being unable to purchase thermometers and prescribed medications enhanced their feeling of distance from the outside world [71].
- All participants felt that the social distancing and isolation policies had had significant social and psychological impacts on their lives and the central theme was loss […]. These emotional and psychological losses were particularly acute for those living in more urban, densely populated cities like London or Birmingham. They were also especially evident amongst those in low-paid or precarious occupations, who had either lost their job or income or were now relying on parental, familial or state financial support as a result of the pandemic [88].
- During the COVID-19 pandemic parents emerged with various type of emotional problems, to the extent that some parents experienced symptoms of anxiety (6.6%) and depression (21.7%) which included washing their hands frequently and findings themselves preoccupied with physical discomfort [91].
3.5.4. Theme 7. Ethnicity, Age and COVID-19 Pandemic
- More disadvantaged backgrounds were less likely to be able to work from home or self-isolate if needed, suggesting structural barriers to adopting preventive behaviours in these groups. The most economically disadvantaged in society are less able to comply with certain NPIs, likely partly due to their financial situation [65].
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 10 April 2021).
- Chen, H.; Shi, L.; Zhang, Y.; Wang, X.; Sun, G. A cross-country core strategy comparison in China, Japan, Singapore and South Korea during the early COVID-19 pandemic. Glob. Health 2021, 17, 22. [Google Scholar] [CrossRef]
- Alanezi, F.; Aljahdali, A.; Alyousef, S.M.; Alrashed, H.; Mushcab, H.; AlThani, B.; Alghamedy, F.; Alotaibi, H.; Saadah, A.; Alanzi, T. A Comparative Study on the Strategies Adopted by the United Kingdom, India, China, Italy, and Saudi Arabia to Contain the Spread of the COVID-19 Pandemic. J. Healthc. Leadersh. 2020, 12, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Ferguson, N.; Laydon, D.; Nedjati-Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunubá, Z.; Cuomo-Dannenburg, G.; et al. Report 9-Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand. Available online: https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-9-impact-of-npis-on-covid-19/ (accessed on 10 April 2021).
- Li, Z.; Chen, Q.; Feng, L.; Rodewald, L.; Xia, Y.; Yu, H.; Zhang, R.; An, Z.; Yin, W.; Chen, W.; et al. Active case finding with case management: The key to tackling the COVID-19 pandemic. Lancet 2020, 396, 63–70. [Google Scholar] [CrossRef]
- World Health Organization. Overview of Public Health and Social Measures in the Context of COVID-19: Interim Guidance. Available online: https://apps.who.int/iris/handle/10665/332115 (accessed on 10 April 2021).
- Ferguson, N.M.; Cummings, D.A.T.; Fraser, C.; Cajka, J.C.; Cooley, P.C.; Burke, D.S. Strategies for mitigating an influenza pandemic. Nature 2006, 442, 7101. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Nonpharmaceutical Interventions (NPIs). 2020. Available online: https://www.cdc.gov/nonpharmaceutical-interventions/index.html (accessed on 3 April 2021).
- European Centre for Disease Prevention and Control. Coronavirus Disease 2019 (COVID-19) in the EU/EEA and the UK. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-rapid-risk-assessment-coronavirus-disease-2019-eighth-update-8-april-2020.pdf (accessed on 3 April 2021).
- Mal, P.; Suneel, P.; Shomeeta, P. Social distancing: A non-pharmacological intervention for COVID-19. J. Pak. Med. Assoc. 2020, 70 (Suppl. 3), S21–S24. [Google Scholar] [CrossRef]
- Johnson, C.Y.; SLFA. Social Distancing Could Buy U.S. Valuable Time against Coronavirus. 2020. Available online: https://www.washingtonpost.com/health/2020/03/10/social-distancing-coronavirus/ (accessed on 3 April 2021).
- Kähler, C.J.; Hain, R. Fundamental protective mechanisms of face masks against droplet infections. J. Aerosol Sci. 2020, 148, 105617. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19. Available online: https://web.archive.org/web/20200325084602/https://www.who.int/docs/default-source/coronaviruse/transcripts/who-audio-emergencies-coronavirus-press-conference-full-20mar2020.pdf?sfvrsn=1eafbff_0 (accessed on 22 March 2021).
- Rocklöv, J.; Sjödin, H.; Wilder-Smith, A. COVID-19 outbreak on the Diamond Princess cruise ship: Estimating the epidemic potential and effectiveness of public health countermeasure. J. Travel Med. 2020, 27, taaa030. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Basic Protective Measures against the New Coronavirus. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 22 March 2021).
- Holmes, R. Is COVID-19 Social Media’s Levelling Up Moment? 2020. Available online: https://www.forbes.com/sites/ryanholmes/2020/04/24/is-covid-19-social-medias-levelling-up-moment/#32e022256c60 (accessed on 22 March 2021).
- Nabity-Grover, T.; Cheung, C.M.K.; Thatcher, J.B. Inside out and outside in: How the COVID-19 pandemic affects self-disclosure on social media. Int. J. Inf. Manag. 2020, 55, 102188. [Google Scholar] [CrossRef]
- Malecki, K.M.C.; Keating, J.A.; Safdar, N. Crisis Communication and Public Perception of COVID-19 Risk in the Era of Social Media. Clin. Infect. Dis. 2021, 72, 4. [Google Scholar] [CrossRef]
- Solnick, R.E.; Chao, G.; Ross, R.D.; Kraft-Todd, G.T.; Kocher, K.E. Emergency Physicians and Personal Narratives Improve the Perceived Effectiveness of COVID-19 Public Health Recommendations on Social Media: A Randomized Experiment. Acad. Emerg. Med. 2021, 28, 2. [Google Scholar] [CrossRef]
- Liu, Z.; Geng, H.; Chen, H.; Zhu, M.; Zhu, T. Exploring the Mechanisms of Influence on COVID-19 Preventive Behaviors in China’s Social Media Users. Int. J. Environ. Res. Public Health 2020, 17, 23. [Google Scholar]
- Oh, S.-H.; Lee, S.Y.; Han, C. The Effects of Social Media Use on Preventive Behaviors during Infectious Disease Outbreaks: The Mediating Role of Self-relevant Emotions and Public Risk Perception. Health Commun. 2020, 1–10. [Google Scholar] [CrossRef]
- World Health Organization. Social Media & COVID-19: A Global Study of Digital Crisis Interaction among Gen Z and Millennials. 2020. Available online: https://www.who.int/news-room/feature-stories/detail/social-media-covid-19-a-global-study-of-digital-crisis-interaction-among-gen-z-and-millennials (accessed on 2 April 2021).
- Chatwin, J.; Butler, D.; Jones, J.; James, L.; Choucri, L.; McCarthy, R. Experiences of pregnant mothers using a social media based antenatal support service during the COVID-19 lockdown in the UK: Findings from a user survey. BMJ Open 2021, 11, 1. [Google Scholar] [CrossRef]
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 434–436. [Google Scholar] [CrossRef]
- Razaq, A.; Harrison, D.; Karunanithi, S.; Barr, B.; Asaria, M.; Khunti, K. BAME COVID-19 Deaths-What Do We Know? Rapid Data & Evidence Review: “Hidden in Plain Sight”. Available online: https://www.cebm.net/wp-content/uploads/2020/05/BAME-COVID-Rapid-Data-Evidence-Review-Final-Hidden-in-Plain-Sight-compressed.pdf (accessed on 28 January 2021).
- Baena-Díez, J.M.; Barroso, M.; Cordeiro-Coelho, S.I.; Díaz, J.L.; Grau, M. Impact of COVID-19 outbreak by income: Hitting hardest the most deprived. J. Public Health 2020, 42, 698–703. [Google Scholar] [CrossRef]
- Public Health England. Disparities in the Risk and Outcomes from COVID-19. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/889195/disparities_review.pdf (accessed on 12 March 2021).
- van Elsland, S.L.; O’Hare, R. Coronavirus Pandemic Could Have Caused 40 Million Deaths if Left Unchecked. Available online: https://www.imperial.ac.uk/news/196496/coronavirus-pandemic-could-have-caused-40/ (accessed on 22 March 2021).
- Lewnard, J.A.; Lo, N.C. Scientific and ethical basis for social-distancing interventions against COVID-19. Lancet Infect. Dis. 2020, 20, 631–633. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M.; Allen, J.; Goldblatt, P.; Herd, E.; Morrison, J. Build. Back Fairer: The COVID-19 Marmot Review. The Pandemic, Socioeconomic and Health Inequalities in England; Institute of Health Equity: London, UK, 2020. [Google Scholar]
- Haque, Z.; Becares, L.; Treloar, N. Over-Exposed and Under-Protected: The Devastating Impact of Covid-19 on Black and Minority Ethnic Communities in Great Britain. 2020. Available online: https://www.gmcvo.org.uk/news/over-exposed-and-under-protected-devastating-impact-covid-19-black-and-minority-ethnic (accessed on 1 April 2021).
- Baker, N. The Housing Pandemic: Four Graphs Showing the Link between COVID-19 Deaths and the Housing Crisis. 2020. Available online: https://www.insidehousing.co.uk/insight/insight/the-housing-pandemic-four-graphs-showing-the-link-between-covid-19-deaths-and-the-housing-crisis-66562 (accessed on 1 April 2021).
- Judge, L.; Rahman, F. Lockdown Living: Housing Quality Across the Generations. 2020. Available online: https://www.resolutionfoundation.org/publications/lockdown-living/ (accessed on 1 April 2021).
- Ministry of Housing C & LG. Overcrowded Households. 2020. Available online: https://www.ethnicity-facts-figures.service.gov.uk/housing/housing-conditions/overcrowded-households/latest (accessed on 1 April 2021).
- Butler, P. Poor Housing Linked to High Covid-19 Death Rate in London Borough. 2020. Available online: https://www.theguardian.com/world/2020/aug/17/poor-housing-linked-high-covid-19-death-rate-london-borough-brent (accessed on 1 April 2021).
- Khunti, K.; Singh, A.; Pareek, M.; Hanif, W. Is ethnicity linked to incidence or outcomes of covid-19? BMJ 2020, 369, m1548. [Google Scholar] [CrossRef] [Green Version]
- Vandenberg, O.; Martiny, D.; Rochas, O.; van Belkum, A.; Kozlakidis, Z. Considerations for diagnostic COVID-19 tests. Nat. Rev. Microbiol. 2021, 19, 171–183. [Google Scholar] [CrossRef]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 7820. [Google Scholar] [CrossRef]
- Peplow, M. Developing Countries Face Diagnostic Challenges as the COVID-19 Pandemic Surges. 2020. Available online: https://0-cen-acs-org.brum.beds.ac.uk/analytical-chemistry/diagnostics/Developing-countries-face-diagnostic-challenges/98/i27 (accessed on 1 April 2021).
- Park, M.; Cook, A.; Lim, J.; Sun, Y.; Dickens, B. A Systematic Review of COVID-19 Epidemiology Based on Current Evidence. J. Clin. Med. 2020, 9, 967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. The COVID-19 pandemic calls for spatial distancing and social closeness: Not for social distancing! J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Russell, S.; Croker, H.; Packer, J.; Ward, J.; Stansfield, C.; Mytton, O.; Bonell, C.; Booy, R. School closure and management practices during coronavirus outbreaks including COVID-19: A rapid systematic review. Lancet Child. Adolesc. Health 2020, 4, 397–404. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Webster, R.; Brooks, S.; Smith, L.; Woodland, L.; Wessely, S.; James, R. How to improve adherence with quarantine: Rapid review of the evidence. medRxiv 2020. [Google Scholar] [CrossRef]
- Bayham, J.; Fenichel, E. Impact of school closures for COVID-19 on the US health-care workforce and net mortality: A modelling study. Lancet Public Health 2020, 5, e271–e278. [Google Scholar] [CrossRef]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.; Russell, T.; Munday, J.; Kucharski, A.; Edmunds, W.; Sun, F. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef] [Green Version]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Jit, M.; Klepac, P.; Flasche, S.; Clifford, S.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Tang, B.; Xia, F.; Tang, S.; Bragazzi, N.; Li, Q.; Sun, X.; Liang, J.; Xiao, Y.; Wu, J. The effectiveness of quarantine and isolation determine the trend of the COVID-19 epidemics in the final phase of the current outbreak in China. Int. J. Infect. Dis. 2020, 95, 288–293. [Google Scholar] [CrossRef]
- Zeb, A.; Alzahrani, E.; Erturk, V.S.; Zaman, G. Mathematical Model for Coronavirus Disease 2019 (COVID-19) Containing Isolation Class. Biomed. Res. Int. 2020, 2020, 3452402. [Google Scholar] [CrossRef]
- Mahtani, K.R.; Heneghan, C.; Aronson, J.K. What Is the Evidence for social Distancing during Global Pandemics? A Rapid Summary of Current Knowledge. Available online: https://www.phc.ox.ac.uk/files/covid-19-evidence-service/what-is-the-evidence-for-social-distancing-during-global-pandemics-final-1.pdf/view (accessed on 22 March 2021).
- Rashid, H.; Ridda, I.; King, C.; Begun, M.; Tekin, H.; Wood, J.G.; Booy, R. Evidence compendium and advice on social distancing and other related measures for response to an influenza pandemic. Paediatr. Respir. Rev. 2015, 16, 119–126. [Google Scholar] [CrossRef]
- Fong, M.; Gao, H.; Wong, J.; Xiao, J.; Shiu, E.; Ryu, S.; Cowling, B. Nonpharmaceutical measures for pandemic influenza in nonhealthcare settings-social distancing measures. Emerg. Infect. Dis. 2020, 26, 976–984. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- University of Michigan. Michigan Medicine Projections Show Aggressive Social Distancing Will Dramatically Reduce the Peak Number of Hospitalized COVID-19 Patients. Available online: https://www.uofmhealth.org/news/archive/202003/michigan-medicine-projections-show-aggressive-social (accessed on 22 March 2021).
- Regmi, K.; Lwin, C.M. Impact of non-pharmaceutical interventions for reducing transmission of COVID-19: A systematic review and meta-analysis protocol. BMJ Open 2020, 10, e041383. [Google Scholar] [CrossRef]
- Gough, D.; Oliver, S.; Thomas, J. An Introduction to Systematic Reviews; Sage: London, UK, 2017. [Google Scholar]
- Guyatt, G.; Rennie, D. Users’ Guides to the Medical Literature: A Manual for Evidenced-Based Clinical Practice; AMA Press: Chicago, IL, USA, 2007. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: West Sussex, UK, 2009. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K. Chapter 7: Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global/ (accessed on 16 April 2021).
- Lockwood, C.; Munn, Z.; Porritt, K. Qualitative research synthesis: Methodological guidance for systematic reviewers utilizing meta-aggregation. Int. J. Evid. Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef]
- Atchison, C.; Bowman, L.; Vrinten, C.; Redd, R.; Pristerà, P.; Eaton, J.; Ward, H. Early perceptions and behavioural responses during the COVID-19 pandemic: A cross-sectional survey of UK adults. BMJ Open. 2021, 11, e043577. [Google Scholar] [CrossRef]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.Y.; Tsang, T.K.; Li, J.C.M.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S.; et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of Public Health Interventions With the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA 2020, 323, 1915. [Google Scholar] [CrossRef] [Green Version]
- Rios-González, C.M. Knowledge, attitudes and practices towards COVID-19 in Paraguayans during outbreaks: A quick online survey. Rev. Salud Publica Parag. 2020, 10, 17–22. [Google Scholar] [CrossRef]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatr. 2020, 51, 102083. [Google Scholar]
- Al-Hanawi, M.K.; Angawi, K.; Alshareef, N.; Qattan, A.M.N.; Helmy, H.Z.; Abudawood, Y.; Alqurashi, M.; Kattan, W.M.; Kadasah, N.A.; Chirwa, G.C.; et al. Knowledge, Attitude and Practice Toward COVID-19 Among the Public in the Kingdom of Saudi Arabia: A Cross-Sectional Study. Front. Public Health 2020, 8, 217. [Google Scholar] [CrossRef]
- Liu, M.; Cheng, S.-Z.; Xu, K.-W.; Yang, Y.; Zhu, Q.-T.; Zhang, H.; Yang, D.-Y.; Cheng, S.-Y.; Xiao, H.; Wang, J.-W.; et al. Use of personal protective equipment against coronavirus disease 2019 by healthcare professionals in Wuhan, China: Cross sectional study. BMJ 2020, 369, m2195. [Google Scholar] [CrossRef]
- Wu, Y.; Song, S.; Kao, Q.; Kong, Q.; Sun, Z.; Wang, B. Risk of SARS-CoV-2 infection among contacts of individuals with COVID-19 in Hangzhou, China. Public Health 2020, 185, 57–59. [Google Scholar] [CrossRef]
- Alobuia, W.M.; Dalva-Baird, N.P.; Forrester, J.D.; Bendavid, E.; Bhattacharya, J.; Kebebew, E. Racial disparities in knowledge, attitudes and practices related to COVID-19 in the USA. J. Public Health 2020, 42, 470–478. [Google Scholar] [CrossRef]
- Feng, Y.; Zong, M.; Yang, Z.; Gu, W.; Dong, D.; Qiao, Z. When altruists cannot help: The influence of altruism on the mental health of university students during the COVID-19 pandemic. Global. Health 2020, 16, 61. [Google Scholar] [CrossRef]
- Shorey, S.; Ang, E.; Yamina, A.; Tam, C. Perceptions of public on the COVID-19 outbreak in Singapore: A qualitative content analysis. J. Public Health 2020, 42, 665–671. [Google Scholar] [CrossRef]
- Sikkema, R.S.; Pas, S.D.; Nieuwenhuijse, D.F.; O’Toole, Á.; Verweij, J.; van der Linden, A.; Chestakova, I.; Schapendonk, C.; Pronk, M.; Lexmond, P.; et al. COVID-19 in health-care workers in three hospitals in the south of the Netherlands: A cross-sectional study. Lancet Infect. Dis. 2020, 20, 1273–1280. [Google Scholar] [CrossRef]
- Rugarabamu, S.; Ibrahim, M.; Byanaku, A. Knowledge, attitudes, and practices (KAP) towards COVID-19: A quick online cross-sectional survey among Tanzanian residents. medRxiv 2020. [Google Scholar] [CrossRef]
- Grannell, A.; Roux, C.W.; McGillicuddy, D. “I am terrified of something happening to me” The lived experience of people with obesity during pandemic. Clin. Obes. 2020, 10, e12406. [Google Scholar] [CrossRef]
- Moorthy, A.; Sankar, T.K. Emerging public health challenge in UK: Perception and belief on increased COVID19 death among BAME healthcare workers. J. Public Health 2020, 42, 486–492. [Google Scholar] [CrossRef]
- Solerte, S.B.; D’Addio, F.; Trevisan, R.; Lovati, E.; Rossi, A.; Pastore, I.; Dell’Acqua, M.; Ippolito, E.; Scaranna, C.; Bellante, R.; et al. Sitagliptin Treatment at the Time of Hospitalization Was Associated With Reduced Mortality in Patients With Type 2 Diabetes and COVID-19: A Multicenter, Case-Control, Retrospective, Observational Study. Diabetes Care 2020, 43, 2999–3006. [Google Scholar] [CrossRef]
- Vally, Z. Public perceptions, anxiety and the perceived efficacy of health-protective behaviours to mitigate the spread of the SARS-Cov-2/ COVID-19 pandemic. Public Health 2020, 187, 67–73. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlȏt, R.; Lambert, H.; Oliver, I.; Robin, C.; Yardley, L.; Rubin, G.J. Factors associated with adherence to self-isolation and lockdown measures in the UK: A cross-sectional survey. Public Health 2020, 187, 41–52. [Google Scholar] [CrossRef]
- Jing, Q.-L.; Liu, M.-J.; Zhang, Z.-B.; Fang, L.-Q.; Yuan, J.; Zhang, A.-R.; Dean, N.E.; Luo, L.; Ma, M.-M.; Longini, I.; et al. Household secondary attack rate of COVID-19 and associated determinants in Guangzhou, China: A retrospective cohort study. Lancet Infect. Dis. 2020, 20, 1141–1150. [Google Scholar] [CrossRef]
- Islam, S.; Emran, G.I.; Rahman, E.; Banik, R.; Sikder, T.; Smith, L.; Hossain, S. Knowledge, attitudes and practices associated with the COVID-19 among slum dwellers resided in Dhaka City: A Bangladeshi interview-based survey. J. Public Health 2020. [Google Scholar] [CrossRef]
- Makhashvili, N.; Javakhishvili, J.D.; Sturua, L.; Pilauri, K.; Fuhr, D.C.; Roberts, B. The influence of concern about COVID-19 on mental health in the Republic of Georgia: A cross-sectional study. Glob. Health 2020, 16, 111. [Google Scholar] [CrossRef]
- Bäuerle, A.; Teufel, M.; Musche, V.; Weismüller, B.; Kohler, H.; Hetkamp, M.; Dörrie, N.; Schweda, A.; Skoda, E.-M. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: A cross-sectional study in Germany. J. Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef]
- Skoda, E.-M.; Teufel, M.; Stang, A.; Jöckel, K.-H.; Junne, F.; Weismüller, B.; Hetkamp, M.; Musche, V.; Kohler, H.; Dörrie, N.; et al. Psychological burden of healthcare professionals in Germany during the acute phase of the COVID-19 pandemic: Differences and similarities in the international context. J. Public Health 2020, 42, 688–695. [Google Scholar] [CrossRef]
- Williams, S.; Armitage, C.; Tampe, T.; Dienes, K. Public perceptions and experiences of social distancing and social isolation during the COVID-19 pandemic: A UK-based focus group study. BMJ Open 2020, 10, e039334. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.A.O.; Elhassan, E.A.M.; Mohamed, A.O.; Mohammed, A.A.; Edris, H.A.; Mahgoop, M.A.; Sharif, M.E.; Bashir, M.I.; Abdelrahim, R.B.; Idriss, W.I.; et al. Knowledge, attitude and practice of the Sudanese people towards COVID-19: An online survey. BMC Public Health 2021, 21, 274. [Google Scholar] [CrossRef]
- Singh, D.R.; Sunuwar, D.R.; Shah, S.K.; Karki, K.; Sah, L.K.; Adhikari, B.; Sah, R.K. Impact of COVID-19 on health services utilization in Province-2 of Nepal: A qualitative study among community members and stakeholders. BMC Health Serv. Res. 2021, 21, 174. [Google Scholar] [CrossRef]
- Wang, L.; Li, D.; Pan, S.; Zhai, J.; Xia, W.; Sun, C.; Zou, M. The relationship between 2019-nCoV and psychological distress among parents of children with autism spectrum disorder. Glob. Health 2021, 17, 23. [Google Scholar] [CrossRef]
- Wolf, M.S.; Serper, M.; Opsasnick, L.; O’Conor, R.M.; Curtis, L.M.; Benavente, J.; Wismer, G.; Batio, S.; Eifler, M. Awareness, Attitudes, and Actions Related to COVID-19 Among Adults With Chronic Conditions at the Onset of the U.S. Outbreak. Ann. Intern. Med. 2020, 173, 100–109. [Google Scholar] [CrossRef] [Green Version]
- Zhong, B.L.; Luo, W.; Li, H.; Zhang, Q.; Liu, X.; Li, W.T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.; Da Molin, G.; De Giglio, O.; Caggiano, G.; Di Onofrio, V.; Ferracuti, S.; Montagna, M.; Liguori, G.; Orsi, G. understanding knowledge and behaviors related to CoViD–19 epidemic in Italian undergraduate students: The EPICO Study. Int. J. Environ. Res. Public Health 2020, 17, 3481. [Google Scholar] [CrossRef]
- Geldsetzer, P. Knowledge and perceptions of covid-19 among the general public in the United States and the United Kingdom: A cross-sectional Online Survey. Ann. Intern. Med. 2020, 173, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Katz, R.; Vaught, A.; Simmens, S. Local decision making for implementing social distancing in response to outbreaks. Public Health Rep. 2019, 134, 150–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, K.; Glatz, T.; Guijt, M.C.; Piccininni, M.; van der Meulen, M.; Atmar, K.; Jolink, A.T.; Kurth, T.; Rohmann, J.L. Public perspectives on social distancing and other protective measures in Europe: A cross-sectional 1 survey study during the COVID-19 pandemic. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Sandro, G.; Rima, S. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Milne, G.J.; Xie, S. The effectiveness of social distancing in mitigating COVID-19 spread: A modelling analysis. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- The Lancet Child & Adolescent Health. Pandemic school closures: Risks and opportunities. Lancet Child. Adolesc. Health 2020, 4, 341. [Google Scholar] [CrossRef]
- Sjödin, H.; Wilder-Smith, A.; Osman, S.; Farooq, Z.; Rocklöv, J. Only strict quarantine measures can curb the coronavirus disease (COVID-19) outbreak in Italy, 2020. Eurosurveillance 2020, 25, 2000280. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Considerations Relating to Social Distancing Measures in Response to COVID-19–Second Update. Available online: https://www.ecdc.europa.eu/en/publications-data/considerations-relating-social-distancing-measures-response-covid-19-second (accessed on 22 March 2021).
- Azman, A.; Luquero, F. From China: Hope and Lessons for COVID-19 Control. Lancet Infect. Dis. 2020. Available online: https://0-linkinghub-elsevier-com.brum.beds.ac.uk/retrieve/pii/S1473309920302644 (accessed on 10 April 2021). [CrossRef]
- Challen, R.; Brooks-Pollock, E.; Read, J.; Dyson, L.; Tsaneva-Atanasova, K.; Danon, L. Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1: Matched cohort study. BMJ 2021, 372, n579. [Google Scholar] [CrossRef]
- Martin, A.; Gravelle, T.B.; Baekkeskov, E.; Lewis, J.; Kashima, Y. Enlisting the support of trusted sources to tackle policy problems: The case of antimicrobial resistance. PLoS ONE 2019, 14, e0212993. [Google Scholar] [CrossRef]
- Gerber, A.S.; Patashnik, E.M.; Doherty, D.; Dowling, C.M. Doctor Knows Best: Physician Endorsements, Public Opinion, and the Politics of Comparative Effectiveness Research. J. Health Polit Policy Law 2014, 39, 171–208. [Google Scholar] [CrossRef] [Green Version]
- Nicol, G.E.; Piccirillo, J.F.; Mulsant, B.H.; Lenze, E.J. Action at a Distance: Geriatric Research during a Pandemic. J. Am. Geriatr. Soc. 2020, 68, 922–925. [Google Scholar] [CrossRef] [Green Version]
- Hiremath, P.; Suhas, K.; Manjunath, M.; Shettar, M. COVID 19: Impact of lock-down on mental health and tips to overcome. Asian J. Psychiatr. 2020, 51, 102088. [Google Scholar] [CrossRef] [PubMed]
- Rose, T.C.; Mason, K.; Pennington, A.; Mchale, P.; Taylor-Robinson, D.; Barr, B. Inequalities in COVID19 mortality related to ethnicity and socioeconomic deprivation. medRxiv 2020. [Google Scholar] [CrossRef]
- Pollock, A.M.; Roderick, P.; Cheng, K.; Pankhania, B. Covid-19: Why is the UK government ignoring WHO’s advice? Br. Med. J. 2020, 368, m1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regmi, K.; Gilbert, R.; Thunhurst, C. How can health systems be strengthened to control and prevent an Ebola outbreak? A narrative review. Infect. Ecol. Epidemiol. 2015, 5, 28877. [Google Scholar] [CrossRef] [PubMed]
- Wolkewitz, M.; Puljak, L. Methodological challenges of analysing COVID-19 data during the pandemic. BMC Med. Res. Methodol. 2020, 20, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shokraneh, F. Keeping up with studies on covid-19: Systematic search strategies and resources. Br. Med. J. 2020, 369, m1601. [Google Scholar] [CrossRef]
- Glasziou, P. Waste in covid-19 research. Br. Med. J. 2020, 369, m1847. [Google Scholar]
- Randhawa, G.; Griffin, S. Covid-19 Must Be a Tipping Point for Tackling Inequalities. Available online: https://0-blogs-bmj-com.brum.beds.ac.uk/bmj/2021/02/12/covid-19-must-be-a-tipping-point-for-tackling-inequalities/ (accessed on 16 April 2021).



{kind=link}
{kind=link}
| Search Terms | Search Date | Reviewers |
|---|---|---|
| #1: “COVID 19”(MeSH Terms) OR “COVID 19”(All Fields) OR “sars cov 2”(All Fields) OR “sars cov 2”(MeSH Terms) OR “severe acute respiratory syndrome coronavirus 2”(All Fields) OR “ncov”(All Fields) OR “2019 ncov”(All Fields) OR “coronavirus infections”(MeSH Terms) OR “coronavirus”(MeSH Terms) OR “coronavirus”(All Fields) OR “coronaviruses”(All Fields) OR “betacoronavirus”(MeSH Terms) OR “betacoronavirus”(All Fields) OR “betacoronaviruses”(All Fields) OR “wuhan coronavirus”(All Fields) | 12 March 2021 | K.R., C.M.L. |
| #2: “social distance”(All Fields) OR “social distancing”(All Fields) OR “cohorting”(All Fields) OR “community containment”(All Fields) OR “isolation strategy”(All Fields) OR “isolation”(All Fields) OR “patient isolation”(All Fields) OR “patient isolation”(MeSH Terms) OR “patient isolators”(All Fields) OR “patient isolators”(MeSH Terms) OR “physical contact”(All Fields) OR “physical distancing”(All Fields) OR “quarantine”(All Fields) OR “quarantines”(All Fields) OR “quarantine”(MeSH Terms) OR OR “quarantined”(All Fields) OR “quarantining”(All Fields) OR “Banning”(All Fields) OR “distancing”(All Fields) | ||
| #3: “reduce”(All Fields) OR “reduced”(All Fields) OR “reduces”(All Fields) OR “reducing”(All Fields) OR “transmission”(MeSH Subheading) OR “transmission”(All Fields) OR “transmissions”(All Fields) OR “prevention and control”(MeSH Subheading) OR “prevention and control”(All Fields) OR “prevention”(All Fields) OR “reduce infection”(All Fields) | ||
| #4: #1 AND #2 AND #3 | ||
| Study ID | Aims/Study Question | Country | Type of Study | Samples | JBI Appraisal Tools * | Reviewer Comments | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Questioned Answered | JBI | |||||||||
| Yes | No | Unclear | NA | |||||||
| Atchison et al. [65] | To examine risk perceptions and behavioural responses of the UK adult population during the early phase of the COVID-19 epidemic. | UK | Cross-sectional survey | 2108 | 1, 2, 4, 7, 8 | 3, 5, 8 | 0 | 0 | Quant. 5/8 | Lack of methodological details but plausible analysis. |
| Cowling et al. [66] | To examine the effect of these interventions and behavioural changes of the public on the incidence of COVID-19, as well as on influenza virus infections, which might share some aspects of transmission dynamics with COVID-19. | Hong Kong | Cross-sectional telephone survey | 3013 | 1, 2, 4, 7, 8 | 3, 5, 6 | 0 | 0 | Quant. 5/8 | Lack of methodological details but plausible analysis. |
| Pan et al. [67] | To evaluate the association of public health interventions with the epidemiological features of the COVID-19 outbreak in Wuhan by 5 periods according to key events and interventions. | China | Quantitative survey | 32,583 | 2, 4, 7, 8 | 1, 3, 5, 6 | 0 | 0 | Quant. 4/8 | Poor methodological details. |
| Rios-González [68] | To examine the knowledge, attitudes and practices of the population about COVID-19. | Paraguay | Cross-sectional study | 3141 | 2, 3, 7, 8 | 1, 4, 5, 6 | 0 | 0 | Quant. 4/8 | Poor methodological details. |
| Roy et al. [69] | To assess the knowledge, attitude, anxiety experience, and perceived mental healthcare need among the adult Indian population during the COVID-19 pandemic. | India | Cross-sectional, observational study | 662 | 1, 2, 7, 8 | 3, 4, 5, 6 | 0 | 0 | Quant. 4/8 | Poor methodological details. |
| Al-Hanawi et al. [70] | To investigate COVID-19 knowledge, attitudes and practices (KAP), and associated sociodemographic characteristics among the general population. | Saudi Arabia | Cross-sectional study | 3388 | 1, 2, 3, 4, 6, 7, 8 | 5 | 0 | 0 | Quant. 7/8 | Few gaps in methodological details but plausible analysis. |
| Liu et al. [71] | To examine the protective effects of appropriate personal protective equipment for frontline healthcare professionals who provided care for patients with coronavirus disease 2019 (COVID-19). | China | Cross-sectional study | 420 | 1, 2, 3, 4, 6, 7, 8 | 5 | 0 | 0 | Quant. 7/8 | Few gaps in methodological details but plausible analysis. |
| Wu et al. [72] | To determine the rate of secondary infection among contacts of individuals with confirmed COVID-19 in Hangzhou according to the type of contact, the intensity of the contact, and their relationship with the index patient. | China | Retrospective cohort study | 2994 | 1, 2, 3, 6, 7, 11 | 4, 5, 8, 9, 10 | 0 | 0 | Cohor.7/11 | Some gaps in the methodology. |
| Alobuia et al. [73] | To determine whether disparities exist in the levels of knowledge, attitudes and practices (KAPs) related to COVID-19. | USA | Cross-sectional study | 1216 | 1, 2, 4, 8 | 3, 5, 6, 7 | 0 | 0 | Quant. 4/8 | Poor methodological details; some gaps in the methodology. |
| Feng et al. [74] | To explore the influence of altruism on negative affect and mental health (anxiety and depressive symptoms) during the COVID-19 pandemic while people self-isolated at home in China. | China | Cross-sectional study | 1346 | 1, 2, 4, 7, 8 | 3, 5, 6 | 0 | 0 | Quant. 5/8 | Some gaps in methodology but overall convincing. |
| Shorey et al. [75] | To analyse the comments left on local media news outlets to find common concerns and discuss potential new measures that can be developed to reduce panic and support for Singapore’s public during and beyond COVID-19. | Singapore | Qualitative study | Not provided (NP) | 3, 4, 5, 8, 9, 10 | 1, 2, 6, 7 | 0 | 0 | Quali. 6/10 | Some gaps in methodology. |
| Sikkema et al. [76] | To understand sources and modes of transmission of SARS-CoV-2 in healthcare workers and patients. | Netherlands | Cross-sectional study | 96 | 1, 2, 3, 4, 7 | 5, 6, 8 | 0 | 0 | Quant. 5/8 | Some gaps in methodology but overall convincing. |
| Rugarabamu et al. [77] | To investigate KAP towards COVID-19 KAP among residents in Tanzania during the April–May 2020 period of the epidemic. | Tanzania | Cross-sectional study | 400 | 2, 4, 7, 8 | 1, 3, 5, 6 | 0 | 0 | Quant. 4/8 | Some gaps in the methodology. |
| Grannell et al. [78] | To examine the impact of the pandemic on their lived experience from a treatment and psychosocial standpoint and additionally explore their awareness of obesity as a risk factor for COVID-19 disease severity. | Ireland | Qualitative study | 23 | 1, 2, 3, 4, 5, 8, 9, 10 | 6, 7 | 0 | 0 | Quali. 8/10 | Some gaps in methodology but overall convincing. |
| Moorthy and Sankar [79] | To explore the beliefs and perception about the reported worrying issue among the BAME health workforce in the diverse city of Leicester. | UK | Cross-sectional study | 200 | 1, 2, 3, 4, 5, 7, 8 | 6 | 0 | 0 | Quant. 7/8 | Some gaps in methodological details but plausible analysis. |
| Solerte et al. [80] | To report several clinical and biochemical outcomes in patients with type 2 diabetes hospitalized for COVID-19. | Italy | Case-control, retrospective study | 338 | 1, 2, 3, 4, 5, 8, 10 | 6, 7, 9 | 0 | 0 | Case-Contr. 7/10 | Appropriate methodological details and plausible analysis. |
| Vally [81] | To examine the public’s perceptions of the pandemic, assesses the extent to which participants have adhered to a range of recommended health-protective behaviours to prevent infection and evaluates whether anxiety about COVID-19 or perceptions related to the pandemic are associated with greater adherence to these behaviours. | United Arab Emirates, Abu Dhabi and Dubai | Cross-sectional study | 634 | 1, 2, 3, 4, 7, 8 | 5, 6 | 0 | 0 | Quant. 6/8 | Some gaps in methodological details but plausible analysis. |
| Smith et al. [82] | To investigate factors associated with adherence to self-isolation and lockdown measures due to COVID-19 in the UK. | UK | Cross-sectional survey | 217 | 1, 2, 3, 4, 6, 7, 8 | 5 | 0 | 0 | Quant. 7/8 | Appropriate methodological details and plausible analysis. |
| Jing et al. [83] | To estimate the secondary attack rate of SARS-CoV-2 among household and non-household close contacts in Guangzhou, China. | China | Retrospective cohort study | 349 | 1, 2, 3, 6, 7, 11 | 4, 5, 8, 9, 10 | 0 | 0 | Cohort. 6/11 | Some gaps in methodological details but plausible analysis. |
| Islam et al. [84] | To investigate the KAP toward COVID-19 among slum dwellers resided in Dhaka City, Bangladesh. | Bangladesh | Cross-sectional study | 406 | 1, 2, 3, 4, 7, 8 | 5, 6 | 0 | 0 | Quant. 6/8 | Some gaps in methodological details but plausible analysis. |
| Makhashvili et al. [85] | To examine concern about COVID-19 and its association with symptoms of mental disorders in the Republic of Georgia. | Georgia | Cross-sectional study | 2088 | 1, 2, 3, 4, 6, 7, 8 | 5 | 0 | 0 | Quant. 7/8 | Appropriate methodological details and plausible analysis. |
| Bäuerle et al. [86] | To assess initial data on the mental health burden of the German public during the COVID-19 pandemic. | Germany | Cross-sectional study | 15,037 | 1, 2, 3, 4, 7, 8 | 5, 6 | 0 | 0 | Quant. 6/8 | Some gaps in methodology but overall convincing. |
| Skoda et al. [87] | To close the research gap and provide initial findings on the psychological burden of German healthcare professionals after the COVID-19 outbreak. | Germany | Cross-sectional study | 12,863 | 1, 2, 3, 7, 8 | 4, 5, 6 | 0 | 0 | Quant. 5/8 | Poor methodological details; some gaps in the methodologies but overall convincing. |
| Williams et al. [88] | To explore the perceptions and experiences of the UK public of social distancing and social isolation measures related to the COVID-19 pandemic. | UK | Qualitative—focus group study | 27 | 1, 2, 3, 4, 5, 8, 9, 10 | 6, 7 | 0 | 0 | Quali. 8/10 | Some gaps in methodology but overall convincing. |
| Mohamed et al. [89] | To assess the knowledge, attitude, and practices of the Sudanese population towards COVID-19. | Sudan | Descriptive cross-sectional | 987 | 1, 2, 3, 4, 7, 8 | 5, 6 | 0 | 0 | Quant. 6/8 | Some gaps in methodology but overall convincing. |
| Singh et al. [90] | To explore community perceptions of COVID-19 and their experiences towards health services utilization during the pandemic in Province-2 of Nepal. | Nepal | Qualitative study | 41 | 2, 3, 4, 5, 6, 8, 9, 10 | 1, 7 | 0 | 0 | Quali. 8/10 | Few gaps in methodological details but plausible analysis. |
| Wang et al. [91] | To investigate psychological distress among parents of children with ASD during the COVID-19 pandemic. | China | Cross-sectional study | 6726 | 1, 2, 3, 4, 7, 8 | 5, 6 | 0 | 0 | Quant. 6/8 | Some gaps in methodology but overall convincing. |
| Wolf et al. [92] | To determine COVID-19 awareness, knowledge, attitudes, and related behaviours among U.S. adults who are more vulnerable to complications of infection because of age and comorbid conditions. | USA | Cross-sectional survey | 630 | 1, 2, 3, 4, 7, 8 | 5, 6 | 0 | 0 | Quant. 6/8 | Few gaps in methodological details but plausible analysis. |
| Zhong et al. [93] | To investigate Chinese residents’ KAP towards COVID-19 during the rapid rise period of the outbreak. | China | Cross-sectional survey | 6919 | 1, 2, 3, 4, 7, 8 | 5.6 | 0 | 0 | Quant. 6/8 | Some gaps in methodology but overall convincing. |
| Gallè et al. [94] | To (i) evaluate the level of knowledge about the 2019-nCoV, it’s spread and the control measures adopted; (ii) analyse health-related behaviours during lockdown, in order to estimate its possible impact on personal habits; (iii) understand if the study field may influence the level of knowledge and lifestyle habits during the pandemic. | Italy | Quantitative survey | 2125 | 1, 3, 7, 8 | 2, 4, 5, 6 | 0 | 0 | Quant. 4/8 | Poor methodological details. |
| Geldsetzer [95] | To assess knowledge and perceptions about COVID-19 among a convenience sample of the general public in the United States and the United Kingdom. | UK and USA | Cross-sectional survey | 5974 | 2, 3, 4, 7, 8 | 1, 5, 6 | 0 | 0 | Quant. 5/8 | Poor methodological details. |
| Katz et al. [96] | To identify key features of preparedness and the primary concerns of local public health officials in deciding to implement social distancing measures, and determine whether any particular factor could explain the widespread variation among health departments in responses to past outbreaks. | USA | Cross-sectional online survey | 150 | 1, 2, 4, 7, 8 | 3, 5, 6 | 0 | 0 | Quant. 5/8 | Lack of methodological details but plausible analysis. |
| Meier et al. [97] | To evaluate public belief in the effectiveness of protective measures, to what extent individuals have implemented these measures in their daily lives, and to identify key communication channels used to acquire information on COVID-19 in European countries. | Netherlands, Germany and Italy | Cross-sectional survey study | 9796 | 1, 2, 3, 4, 7, 8 | 5, 6 | 0 | 0 | Quant. 6/8 | Some gaps in methodological details but plausible analysis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Regmi, K.; Lwin, C.M. Factors Associated with the Implementation of Non-Pharmaceutical Interventions for Reducing Coronavirus Disease 2019 (COVID-19): A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4274. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084274
Regmi K, Lwin CM. Factors Associated with the Implementation of Non-Pharmaceutical Interventions for Reducing Coronavirus Disease 2019 (COVID-19): A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(8):4274. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084274
Chicago/Turabian StyleRegmi, Krishna, and Cho Mar Lwin. 2021. "Factors Associated with the Implementation of Non-Pharmaceutical Interventions for Reducing Coronavirus Disease 2019 (COVID-19): A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 8: 4274. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084274