
Evaluations of Muscular Strength, Ability to Balance and Health Status in Prisoners during COVID-19

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Subjects
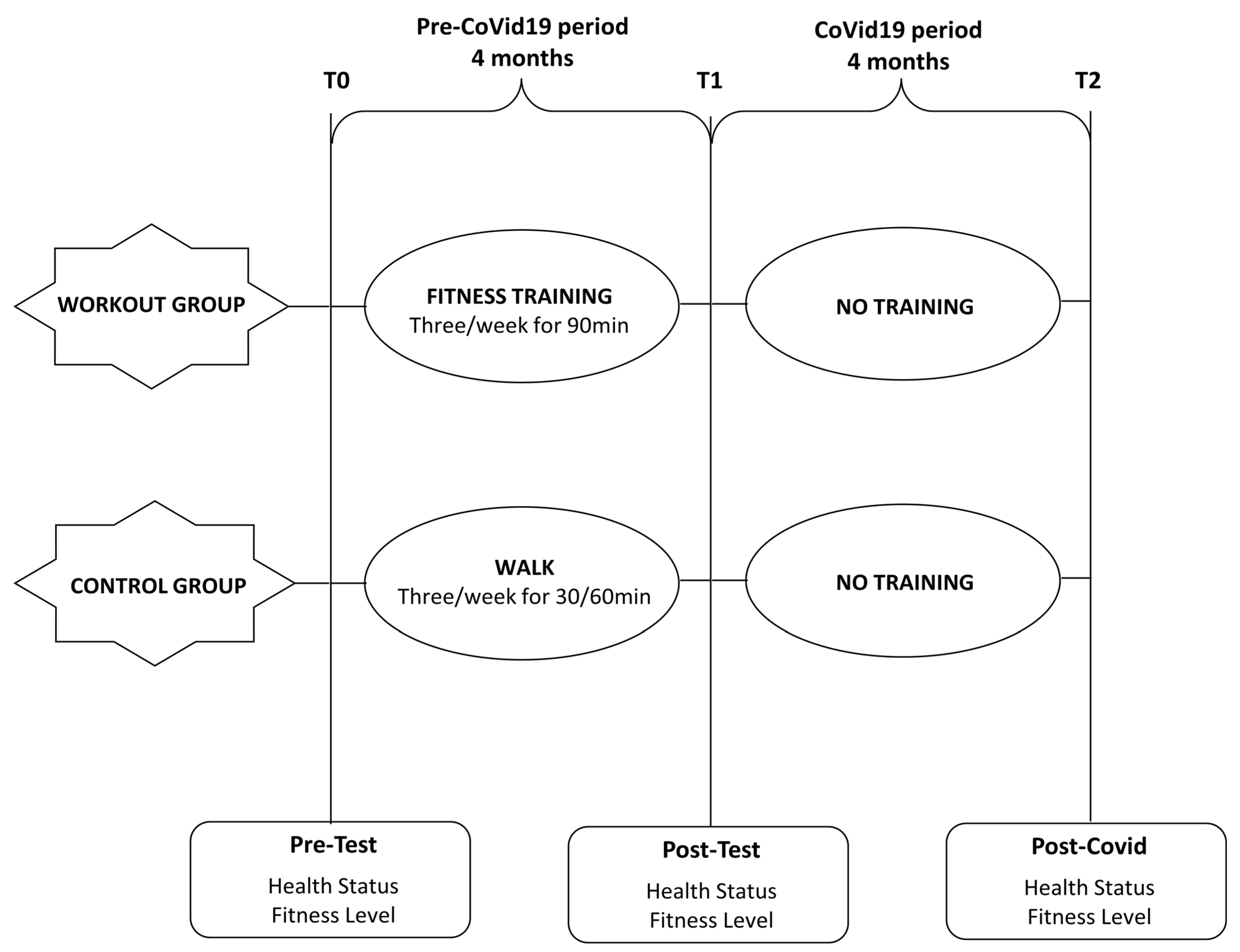
2.2. Study Design
2.3. Testing Procedures
2.4. Testing Procedures before and after the 4-Month Period and after the Post COVID Period
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Caputo, F.; Gratteri, S.; Sacco, M.A.; Scalise, C.; Cacciatore, G.; Bonetta, F.; Zibetti, A.; Aloe, L.; Sicilia, F.; Cordasco, F.; et al. Covid-19 emergency in prison: Current management and forensic perspectives. Med. Leg. J. 2020, 88, 185–186. [Google Scholar] [CrossRef] [PubMed]
- Hawks, L.; Woolhandler, S.; McCormick, D. COVID-19 in Prisons and Jails in the United States. JAMA Intern. Med. 2020, 180, 1041–1042. [Google Scholar] [CrossRef]
- Simpson, P.L.; Butler, T.G. Covid-19, prison crowding, and release policies. BMJ 2020, 20, 369:m1551. [Google Scholar] [CrossRef] [Green Version]
- Fovet, T.; Lancelevée, C.; Eck, M.; Scouflaire, T.; Bécache, E.; Dandelot, D.; Giravalli, P.; Guillard, A.; Horrach, P.; Lacambre, M.; et al. Mental health care in French correctional facilities during the Covid-19 pandemic. Encephale 2020, 46, S60–S65. [Google Scholar] [CrossRef] [PubMed]
- Cingolani, M.; Caraceni, L.; Cannovo, N.; Fedeli, P. The COVID-19 Epidemic and the Prison System in Italy. J. Correct Health Care 2021, 27, 1–7. [Google Scholar] [CrossRef]
- Lennon, R.P.; Claussen, K.A.; Kuersteiner, K.A. State of the heart: An overview of the disease burden of cardiovascular disease from an epidemiologic perspective. Prim. Care 2018, 45, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Perry, B.D.; Caldow, M.K.; Brennan-Speranza, T.C.; Sbaraglia, M.; Jerums, G.; Garnham, A.; Wong, C.; Levinger, P.; Asrar Ul Haq, M.; Hare, D.L.; et al. Muscle atrophy in patients with Type 2 Diabetes Mellitus: Roles of inflammatory pathways, physical activity and exercise. Exerc. Immunol. Rev. 2016, 22, 94–109. [Google Scholar] [PubMed]
- Choudhry, K.; Armstrong, D.; Dregan, A. Nurses’ Perceptions of Weight Gain and Obesity in the Prison Environment. J. Correct Health Care 2017, 23, 173–183. [Google Scholar] [CrossRef]
- Simeni Njonnou, S.R.; Boombhi, J.; Etoa Etoga, M.C.; Tiodoung Timnou, A.; Jingi, A.M.; Nkem Efon, K.; Mbono Samba Eloumba, E.A.; Ntsama Essomba, M.J.; Kengni Kebiwo, O.; Tsitsol Meke, A.N.; et al. Prevalence of Diabetes and Associated Risk Factors among a Group of Prisoners in the Yaounde Central Prison. J. Diabetes Res. 2020, 2020. [Google Scholar] [CrossRef] [Green Version]
- Esposito, M. The health of Italian prison inmates today: A critical approach. J. Correct. Health Care 2010, 16, 230–238. [Google Scholar] [CrossRef]
- Jin, X.; Kinner, S.A.; Hopkins, R.; Stockings, E.; Courtney, R.J.; Shakeshaft, A.; Petrie, D.; Dobbins, T.; Dolan, K. Brief intervention on Smoking, Nutrition, Alcohol and Physical (SNAP) inactivity for smoking relapse prevention after release from smoke-free prisons: A study protocol for a multicentre, investigator-blinded, randomised controlled trial. BMJ Open 2018, 8, e021326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, G.P.D.; Morais, S.C.R.V.; Frazão, C.M.F.Q.; Lopes, C.T.; Mangueira, S.O.; Linhares, F.M.P. Cardiovascular risk factors in people deprived of their liberty: An integrative review. Rev. Gaucha. Enferm. 2020, 41, e20190357. [Google Scholar] [CrossRef]
- Arries, E.J.; Maposa, S. Cardiovascular risk factors among prisoners: An integrative review. J. Forensic. Nurs. 2013, 9, 52–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannocci, A.; Mipatrini, D.; D’Egidio, V.; Rizzo, J.; Meggiolaro, S.; Firenze, A.; Boccia, G.; Santangelo, O.E.; Villari, P.; La Torre, G.; et al. Health related quality of life and physical activity in prison: A multicenter observational study in Italy. Eur. J. Public Health 2018, 28, 570–576. [Google Scholar] [CrossRef]
- Gallé, F.; Maida, P.; Cirella, A.; Giuliano, E.; Belfiore, P.; Liguori, G. Does post-operative psychotherapy contribute to improved comorbidities in bariatric patients with borderline personality disorder traits and bulimia tendencies? A prospective study. Obes. Surg. 2017, 27, 1872–1878. [Google Scholar] [CrossRef] [PubMed]
- Sim, J. The future of prison health care: A critical analysis. Crit. Soc. Policy 2002, 22, 300–323. [Google Scholar] [CrossRef]
- Moeller, L.; Stöver, H.; Jürgens, R.; Gatherer, A.; Nikogosian, H. Health in Prisons: A WHO Guide to the Essential in Prison Health, World Health Organisation, Copehnagen; Enggist, S., Møller, L., Galea, G., Udesen, C., Eds.; WHO Regional Office for Europe: Copenhagen, Denmark, 2007. [Google Scholar]
- Meek, R.; Champion, N.; Klier, S. Fit for Release: How Sports-Based Learning Can Help Prisoners Engage in Education, Gain Employment and Desist from Crime; Prisoners Education Trust: London, UK, 2012. [Google Scholar]
- Buckaloo, B.; Krug, K.; Nelson, K. Exercise and the low-security inmate: Changes in depression, stress, and anxiety. Prison J. 2009, 89, 328–343. [Google Scholar] [CrossRef]
- Meek, R.; Lewis, G. The Impact of a Sports Initiative for Young Men in Prison: Staff and Participant Perspectives. J. Sport Soc. Issues 2014, 38, 95–123. [Google Scholar] [CrossRef]
- Frank, P.; Dahn, J. Exercise and wellbeing: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–192. [Google Scholar]
- Olaitan, S.; Shmaila, H.; Sikiru, L.; Lawal, I. Correlates of selected indices of physical fitness and duration of incarceration among inmates in some selected Nigeria Prisons. Ethiop. J. Health Sci. 2010, 20, 65–69. [Google Scholar] [CrossRef] [Green Version]
- Ginn, S. Prison environment and health. BMJ 2012, 345, e5921. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Adams, K.; Cafarelli, E.; Dudey, G.; Dody, C.; Faigenbaum, M.S.; Fleck, S.J.; Franklin, B.; Fry, A.C.; Newton, R.U.; et al. American College of Sports Medicine position stand: Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2002, 34, 36–380. [Google Scholar]
- Pérez-Moreno, F.; Cámara-Sánchez, M.; Tremblay, J.F.; Riera-Rubio, V.J.; Gil-Paisán, L.; Lucia, A. Benefits of exercise training in Spanish prison inmates. Clinical Sciences. Int. J. Sports Med. 2007, 28, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.G.; Roche, A.F.; Matorell, L.R. Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 1988. [Google Scholar]
- Parameswaran, G.I.; Brand, K.; Dolan, J. Pulse oximetry as a potential screening tool for lowerextremity arterial disease in asymptomatic patients with diabetes mellitus. Arch. Intern. Med. 2005, 165, 442–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendelson, Y. Pulse oximetry: Theory and applications for noninvasive monitoring. Clin. Chem. 1992, 38, 1601–1607. [Google Scholar] [CrossRef]
- Rikli, R.; Jones, J. Functional fitness normative scores for community-residing older adults, ages 60–94. J. Aging Phys. Act. 1999, 7, 162–181. [Google Scholar] [CrossRef]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Essentials of Exercise Physiology, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2000. [Google Scholar]
- Jessie Jones, C.; Rikli, R.; Max, J.; Noffal, G. The Reliability and Validity of a Chair Sit-and-Reach Test as a Measure of Hamstring Flexibility in Older Adults. Res. Q. Exerc. Sport. 1998, 69, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Rodríguez, A.; Chinchilla-Minguet, J.L. Cardiovascular program to improve physical fitness in those over 60 years old–pilot study. Clin. Interv. Aging 2014, 13, 1269–1275. [Google Scholar]
- Diener, M.H.; Golding, L.A.; Diener, D. Validity and reliability of a one-minute sit-up test of abdominal strength and endurance. Sports Med. Train. Rehabil. 1995, 6, 105–119. [Google Scholar] [CrossRef]
- Baumgartner, T.A.; Oh, S.; Chung, H.; Hales, D. Objectivity, reliability, and validity for a revised push-up test protocol. Meas. Phys. Educ. Exerc. Sci. 2002, 6, 225–242. [Google Scholar] [CrossRef]
- Różańska-Kirschke, A.; Kocur, P.; Wilk, M.; Dylewicz, P. The Fullerton Fitness Test as an index of fitness in the elderly. Med. Rehabil. 2006, 10, 9–16. [Google Scholar]
- James, T.; Rikli, R.E.; Jones, C.J. The reliability and validity of a 30-s arm curl as a measure of upper body strength in older adults. Southwest Chapter Am. Coll. Sports Med. 1998, 27, 113–120. [Google Scholar]
- Moffa, S.; Perna, A.; Candela, G.; Cattolico, A.; Sellitto, C.; De Blasiis, P.; Guerra, G.; Tafuri, D.; Lucariello, A. Effects of Hoverboard on Balance in Young Soccer Athletes. J. Funct. Morphol. Kinesiol. 2020, 5, 60. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, L.; Lefevre, J.; Philippaerts, R.; Martens, M.; Huygens, W.; Troosters, T.; Beunen, G. How to assess physical activity? How to assess physical fitness? Eur. J. Cardiovasc. Prev. Rehabil. 2005, 12, 102–114. [Google Scholar] [CrossRef]
- Stewart, I.B.; Pickering, R.L. Effect of prolonged exercise on arterial oxygen saturation in athletes susceptible to exercise-induced hypoxemia. Scand. J. Med. Sci. Sports 2007, 17, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Attili, A.K.; Kazerooni, E.A.; Gross, B.H.; Flaherty, K.R.; Myers, J.L.; Martinez, F.J. Smoking-related interstitial lung disease: Radiologic-clinical-pathologic correlation. Radiographics 2008, 28, 1383–1396. [Google Scholar] [CrossRef] [PubMed]
- Siconolfi, S.F.; Garber, C.E.; Lasater, T.M.; Carleton, R.A. A simple, valid step test for estimating maximal oxygen uptake in epidemiologic studies. Am. J. Epidemiol. 1985, 121, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise capacity and mortality among men referred for exercise testing. N. Engl. J. Med. 2002, 4, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Lauer, M.S.; Okin, P.M.; Larson, M.G.; Evans, J.C.; Levy, D. Prognostic implications of chronotropic incompetence in the Framingham heart study. Circulation 1996, 93, 1520–1526. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Cashin, A.; Potter, E.; Stevens, W.; Davidson, K.; Muldoon, D. Fit for prison: Special population health and fitness programme evaluation. Int. J. Prison. Health 2008, 4, 208–216. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| WORKOUT GROUP | CONTROL GROUP | |||||
|---|---|---|---|---|---|---|
| November 2019 | February 2020 | July 2020 (Post Covid-19 Stop) | November 2019 | February 2020 | July 2020 (Post Covid-19 Stop) | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| BMI (kg/m²) | 28.1 * ± 1.71 | 27.75 † ± 1.94 | 28.25 ± 1.68 | 27.9 ± 2.19 | 27.6 †† ± 1.98 | 28.1 ± 2.04 |
| SBP (mmHg) | 123.75 ** ± 9.43 | 116.15 †† ± 8.73 | 123.05 ± 8.03 | 123.6 ** ± 8.72 | 122.1 ± 8.49 | 122.9 ± 8.87 |
| DBP (mmHg) | 81.8 ** ± 6.97 | 76.65 †† ± 6.42 | 81 ± 6.92 | 79.85 * ± 10.81 | 79 ± 10.17 | 79.6 ± 10.53 |
| SpO2(%) | 97.2 * ± 1.64 | 98.05 † ± 1.19 | 97.55 ± 1.46 | 97.1 ± 1.51 | 97.2 ± 1.5 | 97.3 ± 1.52 |
| CVF (L) | 4.59 ** ± 0.29 | 4.66 †† ± 0.29 | 4.54 ± 0.3 | 4.73 ± 0.37 | 4.74 †† ± 0.37 | 4.68 ± 0.36 |
| FEV1 (L) | 3.9 ** ± 0.28 | 3.97 ± 0.28 | 3.91 ± 0.27 | 4.04 ** ± 0.43 | 4.09 † ± 0.04 | 4.04 ± 0.41 |
| TIFFENAU INDEX (%) | 0.84 ± 0.02 | 0.85 ± 0.02 | 0.86 ± 0.02 | 0.85 ** ± 0.04 | 0.86 ± 0.04 | 0.86 ± 0.04 |
| WORKOUT GROUP | CONTROL GROUP | |||||
|---|---|---|---|---|---|---|
| November 2019 | February 2020 | July 2020 (Post Covid-19 Stop) | November 2019 | February 2020 | July 2020 (Post Covid-19 Stop) | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| 2 Minutes Step Test (n) | 38.85 ** ± 6.01 | 42.45 †† ± 5.96 | 39.6 ± 5.66 | 39.35 ± 5.72 | 40.15 ± 5.57 | 39.2 ± 5.48 |
| HR 30-60 | 45.25 ** ± 4.1 | 41.95 †† ± 3.97 | 45.1 ± 4.26 | 44.35 ± 4.27 | 45.05 ± 4.71 | 4.55 ± 5.48 |
| Sit and reach (cm) | 0.8 ** ± 4.17 | 2.85 †† ± 3.82 | 1.7 ± 3.86 | 0.65 ± 4.95 | 0.71 ± 4.8 | 0.63 ± 4.63 |
| Half sit up test (n) | 24.3 ** ± 5.54 | 28.9 ††± 5.26 | 24.6 ± 6.01 | 25.25 ± 6.52 | 25.4 ± 6.32 | 24.7 ± 6.13 |
| Push up test (n) | 28.45 ** ± 6.15 | 35.55††± 5.35 | 29.7 ± 5.43 | 29.55 ± 8.11 | 29.15 ± 7.85 | 29.1 ± 8.01 |
| Armcurl test (n) | 26.85 ** ± 4.39 | 31.9 †† ± 4.5 | 28 ± 4.1 | 24.9 ± 5.09 | 25.15 ± 5.26 | 24.8 ± 4.67 |
| Stork test (s) | 30.3 ** ± 6.36 | 34.35 †† ± 6.26 | 30.45 ± 6.24 | 30.3 ± 6.36 | 31.1 ± 5.97 | 30.8 ± 6.14 |
| 10 × 5 shuttle test (s) | 25.5 ** ± 3.84 | 22.8 ††± 2.89 | 7.25 ± 3.38 | 25.5 ± 3.84 | 25.2 ± 3.67 | 25.3 ± 3.84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moffa, S.; Perna, A.; Cattolico, A.; Sellitto, C.; Ascione, A.; Tafuri, D.; Guerra, G.; Lucariello, A. Evaluations of Muscular Strength, Ability to Balance and Health Status in Prisoners during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 4316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084316
Moffa S, Perna A, Cattolico A, Sellitto C, Ascione A, Tafuri D, Guerra G, Lucariello A. Evaluations of Muscular Strength, Ability to Balance and Health Status in Prisoners during COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(8):4316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084316
Chicago/Turabian StyleMoffa, Stefano, Angelica Perna, Alessandro Cattolico, Carmine Sellitto, Antonio Ascione, Domenico Tafuri, Germano Guerra, and Angela Lucariello. 2021. "Evaluations of Muscular Strength, Ability to Balance and Health Status in Prisoners during COVID-19" International Journal of Environmental Research and Public Health 18, no. 8: 4316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084316