
Individual-Level Determinants of Lifestyle Behavioral Changes during COVID-19 Lockdown in the United States: Results of an Online Survey

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Setting
2.2. Procedures
2.2.1. Lifestyle Behavioral Change Variables
2.2.2. Individual-Level Determinants
Sociodemographics
Mental Health
Behavioral Determinants
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Changes in Healthy Lifestyle Behaviors
3.2.1. Univariate Analyses: Healthy Lifestyle Behavioral Change
3.2.2. Univariate Analyses: Healthy Behavioral Change Index
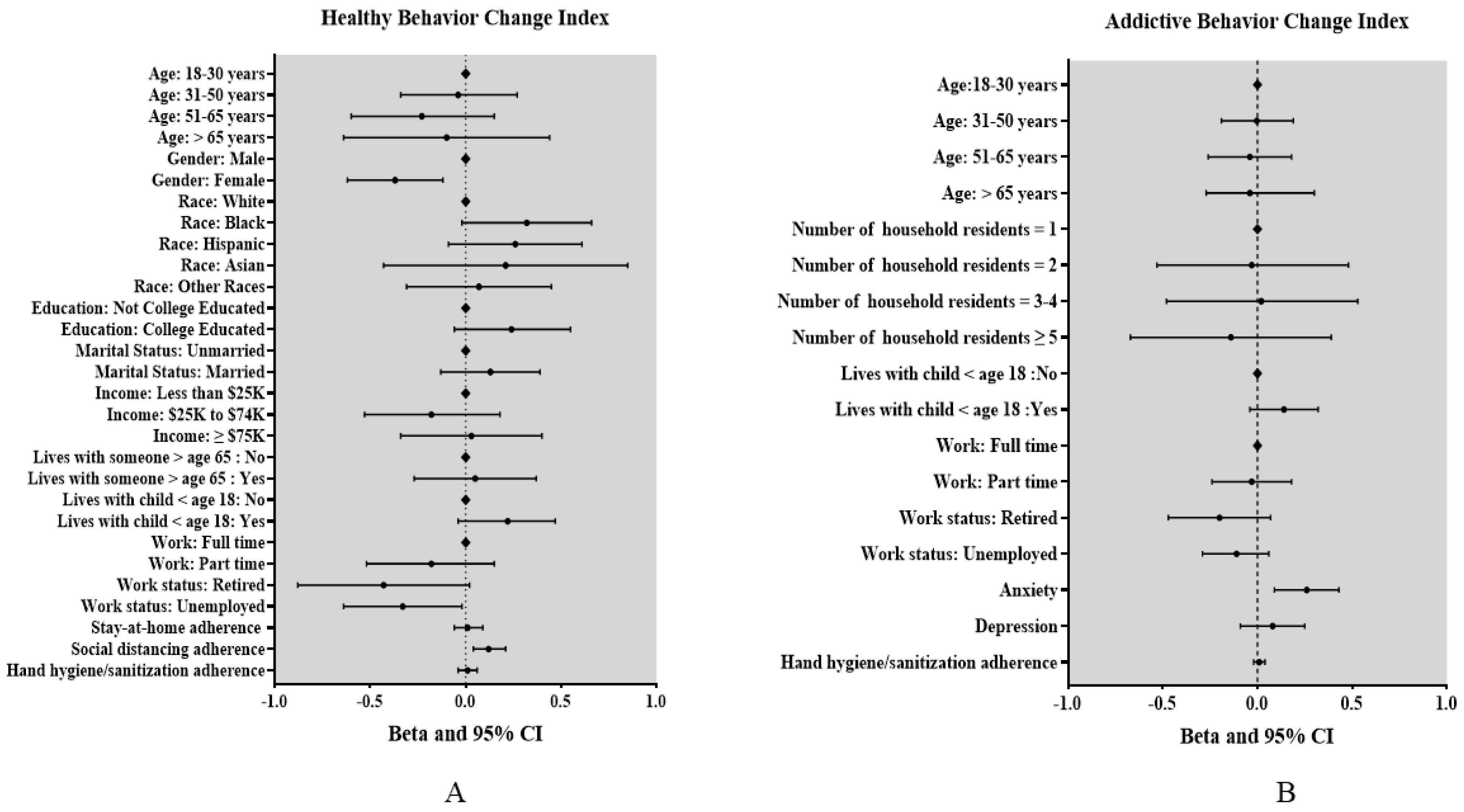
3.2.3. Multivariable Analysis: Healthy Behavioral Change Index
3.3. Changes in Addictive Lifestyle Behaviors
3.3.1. Univariate Analyses: Addictive Lifestyle Behavioral Change
3.3.2. Univariate Analyses: Addictive Behavioral Change Index
3.3.3. Multivariable Analysis: Addictive Behavioral Change Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Construct | Measure |
|---|---|
| Sociodemographics (19 items) | Age, gender, race/ethnicity, education, marital status, annual household income, work status, current living arrangement (alone, or with a spouse/partner, family member, or non-family member), number of household residents, whether they lived with someone over age 65 or younger than age 18, zip code, and cross street. |
| Mental Health Impacts | |
| General Depression (4 items) | PROMIS Depression 4-item Short form [32] |
| General Anxiety (4 items) | PROMIS Anxiety 4-item Short Form [33] |
| Health Behavioral Impacts: COVID-19 Preventive Measures | |
| Adherence to Stay-at-Home Orders | “Does the area where you live have a stay-at-home Orders?” (1 = yes, 2 = no, 3 = I don’t know) “To what extent do you currently follow the stay at home order?” (0 = not at all to 10 = completely) |
| Social Distancing | “What amount of social distancing do you currently practice?” (0 = no social distancing to 10 = complete social distancing) |
| Hand Hygiene | “How often do you practice protective measures like hand washing, use of hand sanitizer, or disinfection of household surfaces to keep yourself and others you live with from contracting COVID-19?” (0 = never to 10 = every few hours) |
| Health Behavioral Impacts: Lifestyle Behaviors | |
| Alcohol Use | “Has your drinking increased/decreased/stayed the same since COVID-19?” |
| Tobacco Use | Two items on current smoking status and type and number of tobacco products smoked per day, taken from the Global Adult Tobacco Survey [31] |
| Exercise | “Since COVID-19 I am exercising more.” (1 = strongly disagree to 5 = strongly agree) |
| Diet | “Since COVID-19 I am eating more healthy foods.” (1 = strongly disagree to 5 = strongly agree) |
References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Balanzá–Martínez, V.; Atienza–Carbonell, B.; Kapczinski, F.; De Boni, R.B. Lifestyle behaviours during the COVID-19—Time to connect. Acta Psychiatr. Scand. 2020, 141, 399–400. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Hu, Z.; Lin, X.; Chiwanda Kaminga, A.; Xu, H. Impact of the COVID-19 Epidemic on Lifestyle Behaviors and Their Association With Subjective Well-Being Among the General Population in Mainland China: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e21176. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Kaluza, J.; Wolk, A. Combined impact of healthy lifestyle factors on lifespan: Two prospective cohorts. J. Intern. Med. 2017, 282, 209–219. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Pan, A.; Wang, D.D.; Liu, X.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C. Impact of healthy lifestyle factors on life expectancies in the US population. Circulation 2018, 138, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; del Pozo Cruz, B.; Green, M.A.; Bauman, A.E. Is the COVID-19 lockdown nudging people to be more active: A big data analysis. Br. J. Sports Med. 2020, 54, 1183. [Google Scholar] [CrossRef] [PubMed]
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obes Res. Clin. Pr. 2020, 14, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Allès, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and physical activity during the COVID-19 lockdown period (March-May 2020): Results from the French NutriNet-Santé cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Pelucchi, C.; Gallus, S.; Garavello, W.; Bosetti, C.; La Vecchia, C. Cancer risk associated with alcohol and tobacco use: Focus on upper aero-digestive tract and liver. Alcohol Res. Health 2006, 29, 193. [Google Scholar]
- Tran, T.D.; Hammarberg, K.; Kirkman, M.; Nguyen, H.T.M.; Fisher, J. Alcohol use and mental health status during the first months of COVID-19 pandemic in Australia. J. Affect. Disord 2020, 277, 810–813. [Google Scholar] [CrossRef]
- Yach, D. Tobacco Use Patterns in Five Countries During the COVID-19 Lockdown. Nicotine Tob Res. 2020, 22, 1671–1672. [Google Scholar] [CrossRef] [PubMed]
- Vanderbruggen, N.; Matthys, F.; Van Laere, S.; Zeeuws, D.; Santermans, L.; Van den Ameele, S.; Crunelle, C.L. Self-reported alcohol, tobacco, and Cannabis use during COVID-19 lockdown measures: Results from a web-based survey. Eur. Addict. Res. 2020, 26, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Avery, A.R.; Tsang, S.; Seto, E.Y.W.; Duncan, G.E. Stress, Anxiety, and Change in Alcohol Use During the COVID-19 Pandemic: Findings Among Adult Twin Pairs. Front. Psychiatry 2020, 11, 571084. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and Stress during COVID-19: Associations with Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian Adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Ingram, J.; Maciejewski, G.; Hand, C.J. Changes in Diet, Sleep, and Physical Activity Are Associated With Differences in Negative Mood During COVID-19 Lockdown. Front. Psychol. 2020, 11, 2328. [Google Scholar] [CrossRef]
- Bremner, J. US Alcohol Sales Increase 55 Percent in One Week Amid Coronavirus Pandemic. 2020. Available online: https://www.newsweek.com/us-alcohol-sales-increase-55-percent-one-week-amid-coronavirus-pandemic-1495510 (accessed on 13 November 2020).
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef]
- Klemperer, E.M.; West, J.C.; Peasley-Miklus, C.; Villanti, A.C. Change in Tobacco and Electronic Cigarette Use and Motivation to Quit in Response to COVID-19. Nicotine Tob. Res. 2020, 22, 1662–1663. [Google Scholar] [CrossRef] [PubMed]
- Khantzian, E.J. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv. Rev. Psychiatry 1997, 4, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.H.; Grant, V.V.; Mackie, C.J.; Conrod, P.J. Comorbidity of Anxiety and Depression with Substance Use Disorders; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Yang, G.Y.; Lin, X.L.; Fang, A.P.; Zhu, H.L. Eating Habits and Lifestyles during the Initial Stage of the COVID-19 Lockdown in China: A Cross-Sectional Study. Nutrients 2021, 13, 970. [Google Scholar] [CrossRef] [PubMed]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.E.; Garnett, C.; Shahab, L.; Oldham, M.; Brown, J. Association of the Covid-19 lockdown with smoking, drinking, and attempts to quit in England: An analysis of 2019–2020 data. medRxiv 2020. [Google Scholar] [CrossRef]
- Badr, H.; Oluyomi, A.; Adel Fahmideh, M.; Raza, S.A.; Zhang, X.; El-Mubasher, O.; Amos, C. Psychosocial and health behavioural impacts of COVID-19 pandemic on adults in the USA: Protocol for a longitudinal cohort study. BMJ Open 2020, 10, e044642. [Google Scholar] [CrossRef] [PubMed]
- Mervosh, S.; Lee, J.; Gamio, L.; Popovich, N. See How All 50 States Are Reopening. Available online: https://www.nytimes.com/interactive/2020/us/states-reopen-map-coronavirus.html (accessed on 8 June 2020).
- Qualtrics [Software]; Oxford University Press: Oxford, UK, 2020.
- Global Adult Tobacco Survey Collaborative Group. Tobacco Questions for Surveys: A Subset of Key Questions from the Global Adult Tobacco Survey (GATS); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2011.
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J. Clin. Epidemiol 2010, 63, 1179–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schalet, B.D.; Pilkonis, P.A.; Yu, L.; Dodds, N.; Johnston, K.L.; Yount, S.; Riley, W.; Cella, D. Clinical validity of PROMIS Depression, Anxiety, and Anger across diverse clinical samples. J. Clin. Epidemiol. 2016, 73, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Tearnan, B.H.; Lewandowski, M. The Behavioral Assessment of Pain Questionnaire: The development and validation of a comprehensive self-report instrument. Am. J. Pain Manag. 1992, 2, 181–191. [Google Scholar]
- Bourassa, K.J.; Sbarra, D.A.; Caspi, A.; Moffitt, T.E. Social Distancing as a Health Behavior: County-Level Movement in the United States During the COVID-19 Pandemic Is Associated with Conventional Health Behaviors. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2020, 54, 548–556. [Google Scholar] [CrossRef]
- Martinez, E.Z.; Silva, F.M.; Morigi, T.Z.; Zucoloto, M.L.; Silva, T.L.; Joaquim, A.G.; Dall Agnol, G.; Galdino, G.; Martinez, M.O.Z.; Silva, W.R.d. Physical activity in periods of social distancing due to COVID-19: A cross-sectional survey. Ciência Saúde Coletiva 2020, 25, 4157–4168. [Google Scholar] [CrossRef] [PubMed]
- Power, K. The COVID-19 pandemic has increased the care burden of women and families. Sustain. Sci. Pract. Policy 2020, 16, 67–73. [Google Scholar] [CrossRef]
- Reichelt, M.; Makovi, K.; Sargsyan, A. The impact of COVID-19 on gender inequality in the labor market and gender-role attitudes. Eur. Soc. 2020, 23, 1–18. [Google Scholar] [CrossRef]
- Smed, S.; Tetens, I.; Bøker Lund, T.; Holm, L.; Ljungdalh Nielsen, A. The consequences of unemployment on diet composition and purchase behaviour: A longitudinal study from Denmark. Public Health Nutr. 2018, 21, 580–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Domelen, D.R.; Koster, A.; Caserotti, P.; Brychta, R.J.; Chen, K.Y.; McClain, J.J.; Troiano, R.P.; Berrigan, D.; Harris, T.B. Employment and physical activity in the U.S. Am. J. Prev. Med. 2011, 41, 136–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.T.-H. The psychosocial impact of the COVID-19 pandemic on changes in smoking behavior: Evidence from a nationwide survey in the UK. Tob. Prev. Cessat. 2020, 6, 1–5. [Google Scholar] [CrossRef]
- National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/covid19/pulse/mental-health.htm (accessed on 13 November 2020).
- Clay, J.M.; Parker, M.O. Alcohol use and misuse during the COVID-19 pandemic: A potential public health crisis? Lancet Public Health 2020, 5, e259002E. [Google Scholar] [CrossRef]
- Ekman, A.; Dickman, P.W.; Klint, A.; Weiderpass, E.; Litton, J.E. Feasibility of using web-based questionnaires in large population-based epidemiological studies. Eur. J. Epidemiol 2006, 21, 103–111. [Google Scholar] [CrossRef] [Green Version]
- van Gelder, M.M.; Bretveld, R.W.; Roeleveld, N. Web-based questionnaires: The future in epidemiology? Am. J. Epidemiol. 2010, 172, 1292–1298. [Google Scholar] [CrossRef]
- Werneck, A.O.; Silva, D.R.d.; Malta, D.C.; Souza-Júnior, P.R.B.d.; Azevedo, L.O.; Barros, M.B.d.A.; Szwarcwald, C.L. Lifestyle behaviors changes during the COVID-19 pandemic quarantine among 6,881 Brazilian adults with depression and 35,143 without depression. Ciência Saúde Coletiva 2020, 25, 4151–4156. [Google Scholar] [CrossRef]
- Ruíz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Rangel Bousquet Carrilho, T.; de Oliveira Cardoso, L. Changes of physical activity and ultra-processed food consumption in adolescents from different countries during Covid-19 pandemic: An observational study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef] [PubMed]

| Sociodemographic Characteristics | n (%) a | Lifestyle Behaviors and Self-Reported Changes Since the Pandemic | n (%) a |
|---|---|---|---|
| Age, Mean (SD), years | 45.0 (17.0) | Drinks alcohol | |
| 18–30 | 324 (25.4) | Yes | 562 (58.2) |
| 31–50 | 489 (38.3) | No | 404 (41.8) |
| 51–65 | 264 (20.7) | Reported change in alcohol use | |
| >65 | 199 (15.6) | Increased | 218 (39.5) |
| Gender | Decreased | 87 (15.8) | |
| Male | 724 (57.5) | Stayed the same | 247 (44.8) |
| Female | 517 (41.0) | Vaping frequency | |
| Race/Ethnicity | Daily | 108 (11.3) | |
| White | 623 (50.2) | Less than Daily | 64 (6.7) |
| Black | 238 (19.2) | Not at all | 788 (82.0) |
| Hispanic | 181 (14.6) | Reported change in vaping frequency | |
| Asian | 35 (2.8) | Increased | 78 (45.9) |
| Other | 165 (13.3) | Decreased | 31 (18.2) |
| Education | Stayed the same | 61 (35.9) | |
| Not college educated | 263 (21.0) | Tobacco smoking frequency | |
| College educated | 988 (79.0) | Daily | 181 (19.0) |
| Marital status | Less than daily | 61 (6.4) | |
| Unmarried | 613 (48.8) | Not at all | 713 (74.7) |
| Married | 644 (51.2) | Reported change in tobacco smoking frequency | |
| Annual household income | Increased | 98 (41.0) | |
| Less than $25 K | 185 (19.0) | Decreased | 48 (20.1) |
| $25 K to $74 K | 382 (39.3) | Stayed the same | 93 (38.9) |
| $75 K or more | 406 (41.7) | Increase in PA frequency | |
| Number of household residents | 1 = Strongly Disagree | 718 (18.6) | |
| 1 | 251 (20.1) | 2 = Disagree | 224 (23.4) |
| 2 | 408 (32.6) | 3 = Neutral | 237 (24.8) |
| 3–4 | 433 (34.6) | 4 = Agree | 205 (21.4) |
| 5 or more | 158 (12.6) | 5 = Strongly Agree | 113 (11.8) |
| Lives with someone > age 65 | Increase in healthy eating | ||
| Yes | 281 (28.1) | 1 = Strongly disagree | 75 (7.8) |
| No | 720 (71.9) | 2 = Disagree | 213 (22.3) |
| Lives with someone < age 18 | 3 = Neutral | 324 (33.9) | |
| Yes | 452 (45.3) | 4 = Agree | 243 (25.4) |
| No | 546 (54.7) | 5 = Strongly agree | 102 (10.7) |
| Work status | Mental Health | ||
| Working full-time | 460 (47.2) | Anxiety b | |
| Working part-time | 128 (13.1) | T-score, mean (SE) | 58.9 (10.6) |
| Retired | 165 (16.9) | Case | 423 (47.7) |
| Unemployed | 221 (22.7) | Not a case | 464 (52.3) |
| Living arrangement | Depression b | ||
| Lives alone | 229 (18.6) | T-score, mean (SE) | 56.1 (10.1) |
| Lives with spouse/partner | 679 (55.3) | Case | 347 (39.1) |
| Lives with a family member | 274 (22.3) | Not a case | 541 (60.9) |
| Lives with a non-family member | 47 (3.8) | ||
| US region of residence | COVID-19 mitigation behaviors | ||
| Northeast | 205 (21.5) | Area of residence under stay-at-home order | |
| Midwest | 200 (21.0) | Yes | 803 (82.8) |
| South | 365 (38.3) | No | 143 (14.7) |
| West | 184 (19.3) | Stay-at-home adherence c | |
| Continuing life as normal | 10 (1.3) | ||
| Stay at home besides essential trips | 269 (33.5) | ||
| Social distancing adherence d | |||
| No social distancing | 14 (1.5) | ||
| Complete social distancing | 299 (31.9) | ||
| Hand hygiene/sanitization adherence e | |||
| Never | 12 (1.3) | ||
| Every few hours | 327 (34.9) | ||
| Factors | Healthy Behavioral Change Index a | |||||
|---|---|---|---|---|---|---|
| Crude Regression Coefficients | 95% CI | p-Value | Adjusted Regression Coefficients b | 95% CI | p-Value | |
| Age | ||||||
| One unit increase | −0.11 | −0.02, −0.01 | <0.001 | |||
| 18–30 | Ref | <0.001 | Ref | 0.63 | ||
| 31–50 | 0.10 | −0.13, 0.33 | −0.04 | −0.34, 0.27 | ||
| 51–65 | −0.36 | −0.62, −0.11 | −0.23 | −0.60, 0.15 | ||
| >65 | −0.40 | −0.68, −0.12 | −0.10 | −0.64, 0.44 | ||
| Gender | <0.001 | |||||
| Male | Ref | Ref | ||||
| Female | −0.90 | −0.57, −0.22 | −0.37 | −0.62, −0.12 | 0.003 | |
| Race | <0.001 | 0.35 | ||||
| White | Ref | Ref | ||||
| Black | 0.54 | 0.31, 0.76 | 0.32 | −0.02, 0.66 | ||
| Hispanic | 0.33 | 0.06, 0.60 | 0.26 | −0.09, 0.61 | ||
| Asian | 0.45 | −0.02, 0.93 | 0.21 | −0.43, 0.85 | ||
| Other | 0.27 | −0.04, 0.59 | 0.07 | −0.31, 0.45 | ||
| Education | 0.02 | 0.12 | ||||
| Not college educated | Ref | Ref | ||||
| College educated | 0.27 | 0.05, 0.49 | 0.24 | −0.06, 0.55 | ||
| Marital status | 0.006 | 0.34 | ||||
| Unmarried | Ref | Ref | ||||
| Married | 0.24 | 0.07, 0.42 | 0.13 | −0.13, 0.39 | ||
| Annual household income | 0.002 | 0.24 | ||||
| Less than $25,000 | Ref | Ref | ||||
| $25,000 to $74,000 | 0.14 | −0.11, 0.38 | −0.18 | −0.53, 0.18 | ||
| $75,000 or more | 0.41 | 0.16, 0.65 | 0.03 | −0.34, 0.40 | ||
| Living arrangement | 0.08 | |||||
| Lives alone | Ref | |||||
| Lives with spouse/partner | 0.27 | 0.03, 0.50 | ||||
| Lives with family member | 0.22 | −0.05, 0.50 | ||||
| Lives with non-family member | −0.07 | −0.53, 0.38 | ||||
| Number of household residents | 0.22 | |||||
| 1 | Ref | |||||
| 2 | 0.10 | −0.14, 0.35 | ||||
| 3–4 | 0.22 | −0.02, 0.47 | ||||
| 5 or more | 0.26 | −0.06, 0.59 | ||||
| Lives with someone > age 65 | 0.01 | 0.75 | ||||
| Yes | −0.29 | −0.51, −0.06 | 0.05 | −0.27, 0.37 | ||
| No | Ref | Ref | ||||
| Lives with child < age 18 | <0.001 | 0.10 | ||||
| Yes | 0.41 | 0.21, 0.60 | 0.22 | −0.04, 0.47 | ||
| No | Ref | Ref | ||||
| Work status | <0.001 | |||||
| Working full-time | Ref | 0.10 | ||||
| Working part-time | −0.25 | −0.51, −0.02 | −0.18 | −0.52, 0.15 | ||
| Retired | −0.71 | −0.95, −0.47 | −0.43 | −0.88, 0.02 | ||
| Unemployed | −0.58 | −0.79, −0.36 | −0.33 | −0.64, −0.02 | ||
| Anxietyc | ||||||
| Case | −0.03 | −0.21, 0.15 | ||||
| Not a case | Ref | |||||
| Depressionc | 0.30 | |||||
| Case | −0.10 | −0.28, 0.09 | ||||
| Not a case | Ref | |||||
| Stay-at-home adherence | 0.01 | 0.77 | ||||
| One unit increase | 0.06 | 0.01, 0.11 | 0.01 | −0.06, 0.09 | ||
| Social distancing adherence | <0.001 | 0.004 | ||||
| One unit increase | 0.09 | 0.04, 0.13 | 0.12 | 0.04, 0.21 | ||
| Hand hygiene/sanitization adherence | 0.79 | |||||
| One unit increase | 0.07 | 0.03, 0.11 | 0.001 | 0.01 | −0.04, 0.06 | |
| Factors | Addictive Behavioral Change Index a | |||||
|---|---|---|---|---|---|---|
| Crude Regression Coefficients | 95% CI | p-Value | Adjusted Regression Coefficients c | 95% CI | p-Value | |
| Age | ||||||
| One unit increase | −0.005 | −0.008, −0.001 | 0.005 | |||
| 18–30 | Ref | 0.002 | 0.98 | |||
| 31–50 | 0.07 | −0.08, 0.23 | −0.003 | −0.19, 0.19 | ||
| 51–65 | −0.08 | −0.25, 0.09 | −0.04 | −0.26, 0.18 | ||
| >65 | −0.19 | −0.38, −0.01 | 0.01 | −0.27, 0.30 | ||
| Gender | 0.68 | |||||
| Male | Ref | |||||
| Female | −0.024 | −0.14, 0.09 | ||||
| Race | ||||||
| White | Ref | |||||
| Black | 0.13 | −0.03, 0.28 | ||||
| Hispanic | −0.09 | −0.28, 0.09 | ||||
| Asian | −0.19 | −0.51, 0.13 | ||||
| Other | 0.09 | −0.12, 0.30 | ||||
| Education | 0.43 | |||||
| Not college educated | Ref | |||||
| College Educated | 0.06 | −0.09, 0.21 | ||||
| Marital status | 0.59 | |||||
| Unmarried | Ref | |||||
| Married | 0.03 | −0.08, 0.15 | ||||
| Annual household income | 0.74 | |||||
| Less than $25,000 | Ref | |||||
| $25,000 to $74,999 | 0.06 | −0.10, 0.23 | ||||
| $75,000 or more | 0.04 | −0.13, 0.20 | ||||
| Living arrangement | 0.04 | |||||
| Lives alone | Ref | |||||
| Lives with spouse/partner | 0.17 | 0.01, 0.32 | ||||
| Lives with family member | 0.11 | −0.07, 0.29 | ||||
| Lives with non-family member | 0.40 | 0.10, 0.71 | ||||
| Number of household residents | 0.008 | 0.5 | ||||
| 1 | Ref | Ref | ||||
| 2 | 0.08 | −0.08, 0.24 | −0.03 | −0.53, 0.48 | ||
| 3–4 | 0.26 | 0.10, 0.42 | 0.02 | −0.48, 0.53 | ||
| 5 or more | 0.13 | −0.08, 0.35 | −0.14 | −0.67, 0.39 | ||
| Lives with someone > age 65 | 0.28 | |||||
| Yes | −0.08 | −0.23, 0.06 | ||||
| No | Ref | |||||
| Lives with child < age 18 | 0.004 | 0.12 | ||||
| Yes | 0.19 | 0.06, 0.32 | 0.14 | −0.04, 0.32 | ||
| No | Ref | Ref | ||||
| Work status | 0.38 | |||||
| Working full-time | Ref | 0.01 | Ref | |||
| Working part-time | −0.01 | −0.19, 0.17 | −0.03 | −0.24, 0.18 | ||
| Retired | −0.27 | −0.43, −0.10 | −0.20 | −0.47, 0.07 | ||
| Unemployed | −0.11 | −0.26, 0.04 | −0.11 | −0.29, 0.06 | ||
| Anxietyd | <0.0001 | 0.002 | ||||
| Case | 0.35 | 0.23, 0.47 | 0.26 | 0.09, 0.43 | ||
| Not a case | Ref | Ref | ||||
| Depressiond | <0.0001 | 0.36 | ||||
| Case | 0.28 | 0.16, 0.40 | 0.08 | −0.09, 0.25 | ||
| Not a case | Ref | Ref | ||||
| Stay-at-home adherence | ||||||
| One unit increase | −0.002 | −0.037, 0.033 | 0.90 | |||
| Social distancing adherence | ||||||
| One unit increase | 0.02 | −0.01, 0.05 | 0.19 | |||
| Hand hygiene/sanitization adherence | 0.47 | |||||
| One unit increase | 0.02 | −0.16, 0.27 | 0.09 | 0.01 | −0.02, 0.04 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Oluyomi, A.; Woodard, L.; Raza, S.A.; Adel Fahmideh, M.; El-Mubasher, O.; Byun, J.; Han, Y.; Amos, C.I.; Badr, H. Individual-Level Determinants of Lifestyle Behavioral Changes during COVID-19 Lockdown in the United States: Results of an Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 4364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084364
Zhang X, Oluyomi A, Woodard L, Raza SA, Adel Fahmideh M, El-Mubasher O, Byun J, Han Y, Amos CI, Badr H. Individual-Level Determinants of Lifestyle Behavioral Changes during COVID-19 Lockdown in the United States: Results of an Online Survey. International Journal of Environmental Research and Public Health. 2021; 18(8):4364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084364
Chicago/Turabian StyleZhang, Xiaotao, Abiodun Oluyomi, LeChauncy Woodard, Syed Ahsan Raza, Maral Adel Fahmideh, Ola El-Mubasher, Jinyoung Byun, Younghun Han, Christopher I. Amos, and Hoda Badr. 2021. "Individual-Level Determinants of Lifestyle Behavioral Changes during COVID-19 Lockdown in the United States: Results of an Online Survey" International Journal of Environmental Research and Public Health 18, no. 8: 4364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084364