
Adapting Traditional Healing Values and Beliefs into Therapeutic Cultural Environments for Health and Well-Being



Abstract
:1. Introduction
2. Rongoā Māori
3. Materials and Methods
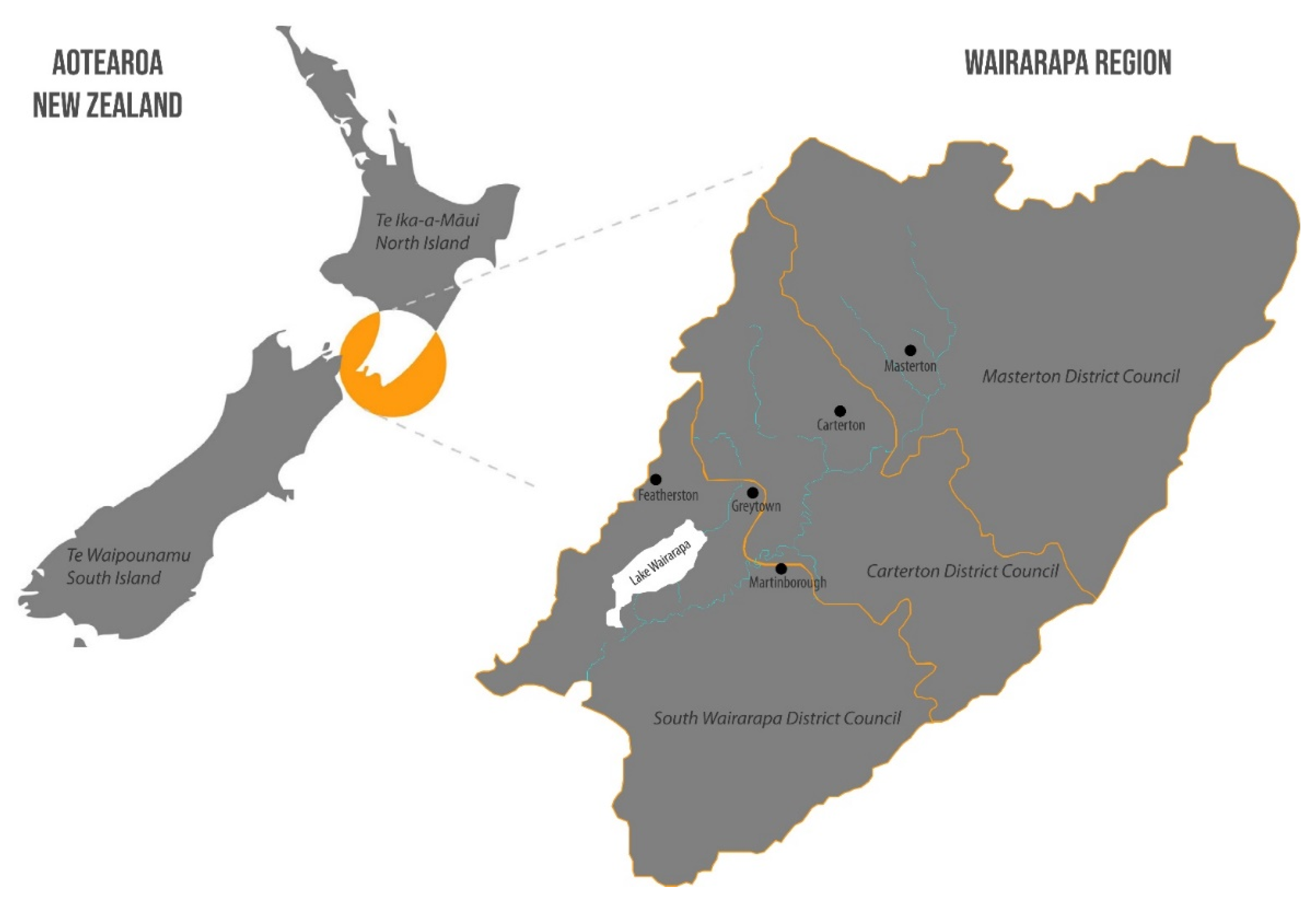
3.1. Process
3.2. Recruitment
3.3. Interviews
3.4. Data Analysis
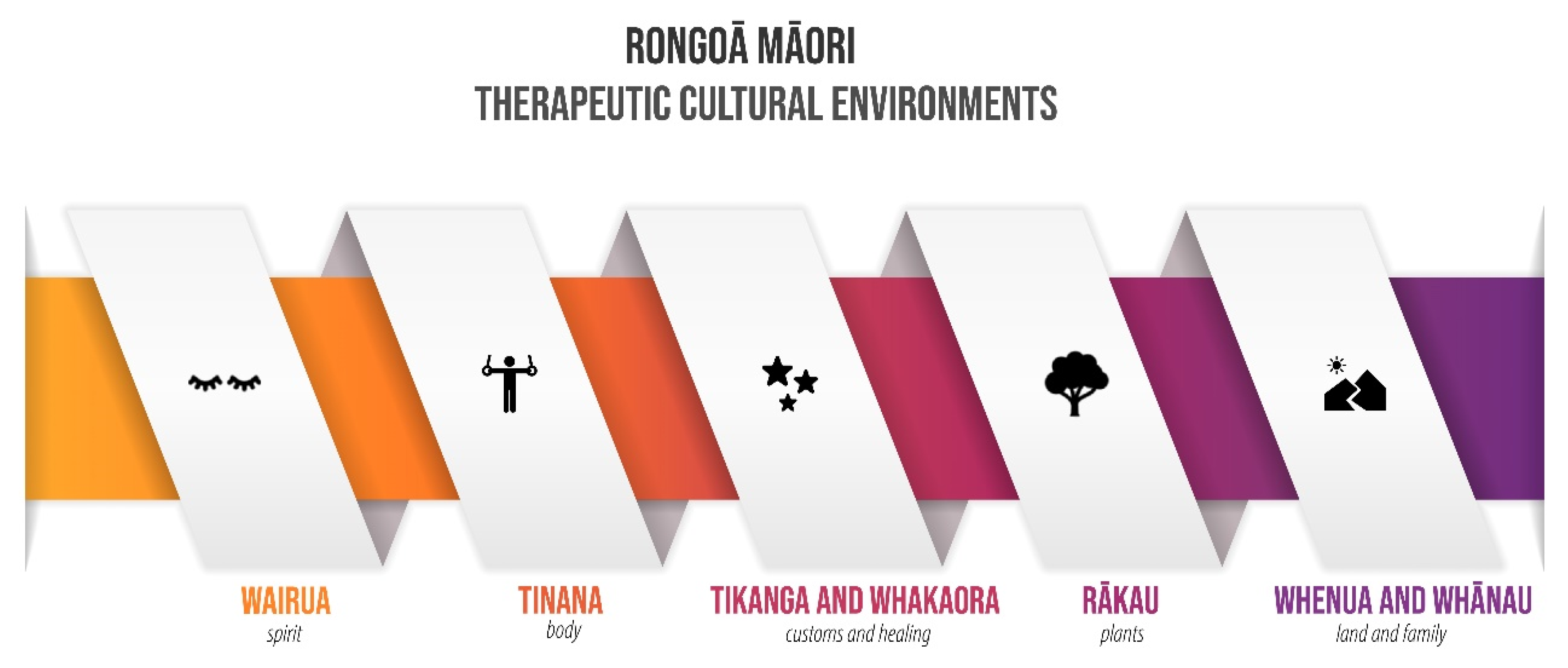
4. Results
4.1. Wairua (Spirit)
“It’s our tīpuna [ancestors] that do all the work…. we are just the vessel.”(participant 4, female)
“When healing, we connect to the whaiora’s [patient’s] ancestors to do the mahi [work].”(participant 1, male)
“If the balance is uneven, and you don’t have that out there in the environment, then you bring that balance back. You must do one thing before you even attempt to go in and start doing.”(participant 7, female)
“Go into the ngāhere [forests] to get rongoā, you must first ask Tānē Mahuta [god of the forests and birds]. You must go through all those Atua [gods], like Tangaroa [god of the ocean], Tūmatauenga [god of war], Rūaumoko [god of earthquakes, volcanoes and seasons]. You go through the whole lot where ever it is that you have to go....”(participant 2, male)
“Rongoā is like a journey… it involves opening up to the mauri [life force] around you and allow that to come through you…. if your surrounding taiao [environment] is polluted, the healing is not going to work.”(participant 5, female)
4.2. Tinana (Body)
“If those bad emotions and thoughts are trapped in your body, they can cause damage… it’s all to do with the connection of mind, body and spirit.”(participant 1, male)
“It is when our hinengaro [mind], tinana [body] and wairua [spirit] are separated that disharmony and illness appear in our lives. That can take many forms, from unhappiness to physical malfunction.”(participant 3, female)
“Our tinana [body] is stronger than you think, it has the power to heal itself.”(participant 6, female)
“And with the karakia [chants], you put in that karakia what you need to be done for the tinana [body], for the mauri [life force], for the mana [authority or prestige] of your people. If the balance is uneven, then you must bring that balance back.”(participant 4, female)
4.3. Tikanga (Customs) and Whakaora (Healing)
“Often, when somebody is unwell, I would feel whatever they have first in my own skin, you know… the quick I can make sense of it, better I can offer assistance.”(participant 8, female)
“The first thing is to put the person at ease and get to know them…. so I can connect in with that whenua [land] and whakapapa [genealogy].”(participant 2, male)
“Aroha [love and respect] is the most critical part of the healing process… oh yes, it needs to be with your patient...it is that love that helps with the healing.”(participant 3, female)
“So, I came here first, I stopped there dropped him off some rongoā pain relief, so by the time I got back there after here, he hadn’t chopped his leg off. We gauged it from Monday, by Wednesday he was fine, by Thursday it was still a bit tender, but he pushed it and by Friday he was running around. Saturday, he was going nightclubbing.”(participant 5, female)
“I’ve got a two-year-old mokopuna [grandchild] that has had eczema since, I don’t know, the word goes, of which we actually have to use rongoā on him. Our children and their generation, they’re actually turning towards rongoā because they’ve studied to find out that mainstream medicine doesn’t work, and it isn’t fixing them, and they don’t trust it.”(participant 3, female)
4.4. Rākau (Plants)
“Rongoā is a different world, you know, it has its own process and generally takes a day… it starts with a karakia [chants] at home and… there’s more karakia [chants] while you walk the bush while you connect with the atua [gods] and with the rākau [trees, plants, herbs].”(participant 6, female)
“It is about the exchange of mauri [life force] and whatumanawa [emotional] stuff… there’s a lot of hongi [pressing noses] with the rākau [plants] as they’ve their own stories, you know, they’re individuals like us.”(participant 8, female)
“We get to know their [plants] whakapapa [genealogy], that’s the connection we want to have…cause everyone can boil stuff but it’s becoming tuned with the rākau [plants] that releases the full potential of it.”(participant 7, female)
“Depending on how connected with the taiao [environment] you are, you know which leaves to pick first…even from which tree…doesn’t matter the illness, the tuākana [elder siblings, referring to plants] always have the right answers.”(participant 1, male)
“Even though the mauri [life force] of the rākau [plants] is being taken, you know, it returns to become one with people… helping them [people] in their journey.”(participant 4, female)
“We make our own pani [spread] for our own rongoā and we utilise our native plants. For the pani, we use beeswax mainly. But, some whānau [extended family] are allergic to honey, therefore, they are allergic to beeswax. So, we use coconut oil as another source.”(participant 7, female)
“We’ve got marae clinics and kaumātua [eldery] days. We do mirimiri [soft tissue massage], whitiwhiti kōrero [advice/support] and honohono [deep tissue massage]. We also use native plants of our lands to make rongoā, ah, for different ailments.”(participant 5, female)
“We do honohono, you know, energy work, so we don’t have to touch people at all… and whitiwhiti kōrero, which is about holistic well-being.”(participant 8, female)
“We also do whānau mirimiri. We only touch the hands, the feet, and work the wairua [spirit].”(participant 2, male)
“Mahi wheua, which is a realignment of the bones, but also gets rid of the uric acid in whānau [extended family], especially kaumātua [elders]. Um, it makes the blood flow so those crystals that crystallise around the bone don’t get to stay there.”(participant 6, female)
4.5. Whenua (Land) and Whānau (Family)
“Healing is a holistic thing, you’re working with and for the whenua [land], once the whenua [land] is healed, then our people will feel better.”(participant 2, male)
“The whenua [land] grounds our whānau [extended family], all whānau. You know, ‘cause some whānau [family] float around up in the sky. There’s a time for that, aye. I’m not saying that, you know, that’s not done, but there’s time for that, we need to anchor, and we anchor in our tipuna [ancestors] and whenua [land]. Especially us when we go to do mahi [work].”(participant 3, female)
“It’s amazing what water can do in the spiritual realm for us as iwi. We have a true belief in this awa [river]... that keeps us safe, within that tapu [sacred] realm of our Māori tikanga [customs and traditions].”(participant 1, male)
“You know, if you were feeling not so good, you went back to your land... You took yourself and your troubles back to the land.”(participant 4, female)
“Our children are actually a bit more close to rongoā than we are. I do find that it’s taken time.”(participant 8, female)
“Cause the kids go, ‘aunty, we’ve seen that stuff work.’ It ain’t my stuff, it’s our stuff. And as long as I’m picking those leaves from your whenua [land], it’s your stuff.”(participant 5, female)
“So, really, these things that we have learned, to reach a young person, you’ve got to come down to their level, not expect them to come up to you. You want to reach your mokopuna [grandchildren] or whoever and put it across and make it exciting. Who the hell wants to listen to an old person? Oh, please.”(participant 6, female)
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdollahi Fard, M.; Shojaii, A. Efficacy of Iranian Traditional Medicine in the Treatment of Epilepsy. BioMed Res. Int. 2013, 2013, 692751. [Google Scholar] [CrossRef] [Green Version]
- Alves, R.R.; Rosa, I.M. Biodiversity, Traditional Medicine and Public Health: Where Do They Meet? J. Ethnobiol. Ethnomed. 2007, 3, 14. [Google Scholar] [CrossRef] [Green Version]
- Nyika, A. Ethical and Regulatory Issues Surrounding African Traditional Medicine in the Context of HIV/AIDS. Dev. World Bio 2007, 7, 25–34. [Google Scholar] [CrossRef]
- Young, C.; Koopsen, C. Spirituality, Health, and Healing: An Integrative Approach, 2nd ed.; G-Reference, Information and Interdisciplinary Subjects Series; Jones & Bartlett Learning: Burlington, MA, USA, 2010; ISBN 978-0-7637-7942-9. [Google Scholar]
- World Health Organization. Traditional Medicine: Growing Needs and Potential; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Leaming, N.; Willis, G.M. The Good Lives Model: New Avenues for Maori Rehabilitation? Sex. Abus. Aust. N. Z. 2016, 7, 59–69. [Google Scholar]
- Lee, C.C.; Armstrong, K.L. Indigenous Models of Mental Health Intervention: Lessons from Traditional Healers. In Handbook of Multicultural Counseling; Casas, J.M., Suzuki, L.A., Alexander, C.M., Jackson, M.A., Eds.; SAGE Publications: Singapore, 2016; pp. 441–456. ISBN 978-1-4833-2332-9. [Google Scholar]
- Chaklader, M.A. Rethinking Medicalization through the Lens of Cultural Hegemony: Traditional Healing and Societal Wellbeing of Chakma Ethnic Community in Bangladesh. Singap. J. Soc. Sci. 2018, 1, 35–46. [Google Scholar]
- Fijal, D.; Beagan, B.L. Indigenous Perspectives on Health: Integration with a Canadian Model of Practice. Can. J. Occup. Ther. 2019, 86, 220–231. [Google Scholar] [CrossRef]
- Gesler, W.M. Healing Places; G-Reference, Information and Interdisciplinary Subjects Series; Rowman & Littlefield Publishers Inc.: Oxford, UK, 2003; ISBN 978-0-7425-1956-5. [Google Scholar]
- Carter, L. Naming to Own Place Names as Indicators of Human Interaction with the Environment. AlterNative Int. J. Indig. Peoples 2005, 1, 6–24. [Google Scholar] [CrossRef]
- Johnson, J.T. Indigeneity’s Challenges to the White Settler-State: Creating a Thirdspace for Dynamic Citizenship. Alternatives 2008, 33, 29–52. [Google Scholar] [CrossRef]
- Pierotti, R.; Wildcat, D. Traditional Ecological Knowledge: The Third Alternative (Commentary). Ecol. Appl. 2000, 10, 1333–1340. [Google Scholar] [CrossRef]
- Tu, Y. Artemisinin-A Gift from Traditional Chinese Medicine to the World (Nobel Lecture). Angew. Chem. Int. Ed. 2016, 55, 10210–10226. [Google Scholar] [CrossRef]
- Gill, J.H. Native American Worldviews: An Introduction; Philosophy of Religion Series; Humanity Books: New York, NY, USA, 2002; ISBN 978-1-59102-051-6. [Google Scholar]
- Helsel, D.G.; Mochel, M.; Bauer, R. Shamans in a Hmong American Community. J. Altern. Complement. Med. 2004, 10, 933–938. [Google Scholar] [CrossRef]
- Kingsley, J.; Townsend, M.; Henderson-Wilson, C.; Bolam, B. Developing an Exploratory Framework Linking Australian Aboriginal Peoples’ Connection to Country and Concepts of Wellbeing. IJERPH 2013, 10, 678–698. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, R. In Sickness and Health: The Sociocultural Context of Aboriginal Wellbeing, Illness and Healing. In The Health of Aboriginal Australia; Reid, J., Trompf, P., Eds.; Harcourt Brace Jovanovich: Sydney, Australia, 1991; pp. 292–323. ISBN 978-0-7295-0385-3. [Google Scholar]
- Cram, F.; Smith, L.; Johnstone, W. Mapping the Themes of Maori Talk about Health. N. Z. Med. J. 2003, 116, 1–7. [Google Scholar]
- Durie, M. A Maori Perspective of Health. Soc. Sci. Med. 1985, 20, 483–486. [Google Scholar] [CrossRef]
- Bussmann, R.W.; Sharon, D. Traditional Medicinal Plant Use in Loja Province, Southern Ecuador. J. Ethnobiol. Ethnomed. 2006, 2, 44. [Google Scholar] [CrossRef] [Green Version]
- Tse, S.; Lloyd, C.; Petchkovsky, L.; Manaia, W. Exploration of Australian and New Zealand Indigenous People’s Spirituality and Mental Health. Aust. Occup. Ther. J. 2005, 52, 181–187. [Google Scholar] [CrossRef]
- Mark, G.; Lyons, A. Conceptualizing Mind, Body, Spirit Interconnections Through, and Beyond, Spiritual Healing Practices. Explore 2014, 10, 294–299. [Google Scholar] [CrossRef]
- Ahuriri-Driscoll, A.; Baker, V.; Hepi, M.; Hudson, M.; Mika, C.; Tiakiwai, S. The Future of Rongoa Maori: Wellbeing and Sustainability; Ministry of Health: Christchurch, New Zealand, 2008; p. 68. [Google Scholar]
- Mark, G.T.; Lyons, A.C. Maori Healers’ Views on Wellbeing: The Importance of Mind, Body, Spirit, Family and Land. Soc. Sci. Med. 2010, 70, 1756–1764. [Google Scholar] [CrossRef]
- Bodeker, G.; Kronenberg, F.; Burford, G. Policy and Public Health Perspectives on Traditional, Complementary and Alternative Medicine: An Overview. In Traditional, Complementary and Alternative Medicine; Imperial College Press: London, UK, 2006; pp. 9–40. ISBN 978-1-86094-616-5. [Google Scholar]
- Montenegro, R.A.; Stephens, C. Indigenous Health in Latin America and the Caribbean. Lancet 2006, 367, 1859–1869. [Google Scholar] [CrossRef]
- Senanayake, S.G.J.N. Indigenous Knowledge as a Key to Sustainable Development. J. Agric. Sci. 2006, 2, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Harmsworth, G.R.; Awatere, S. Indigenous Māori Knowledge and Perspectives of Ecosystems. In Ecosystem Services in New Zealand-Conditions and Trends; Dymond, J., Ed.; Manaaki Whenua Press: Lincoln, New Zealand, 2013; pp. 274–286. ISBN 978-0-478-34736-4. [Google Scholar]
- Mark, G.; Chamberlain, K.; Boulton, A. Acknowledging the Māori Cultural Values and Beliefs Embedded in Rongoā Māori Healing. IJIH 2017, 12, 75. [Google Scholar] [CrossRef] [Green Version]
- Anton, C.E.; Lawrence, C. Home Is Where the Heart Is: The Effect of Place of Residence on Place Attachment and Community Participation. J. Environ. Psychol. 2014, 40, 451–461. [Google Scholar] [CrossRef] [Green Version]
- Carter, J.; Dyer, P.; Sharma, B. Dis-Placed Voices: Sense of Place and Place-Identity on the Sunshine Coast. Soc. Cult. Geogr. 2007, 8, 755–773. [Google Scholar] [CrossRef]
- Creswell, T. Introduction: Theorizing Place. In Mobilizing Place, Placing Mobility: The Politics of Representation in a Globalised World; Verstraete, G., Cresswell, T., Eds.; Place, Sex and Race; Brill Rodopi: Amsterdam, The Netherlands, 2002; pp. 11–32. ISBN 978-90-420-1144-1. [Google Scholar]
- Rodaway, P. Sensuous Geographies: Body, Sense and Place; Taylor & Francis: London, UK, 2002; ISBN 978-1-134-88070-6. [Google Scholar]
- Scannell, L.; Gifford, R. Defining Place Attachment: A Tripartite Organizing Framework. J. Environ. Psychol. 2010, 30, 1–10. [Google Scholar] [CrossRef]
- Kidman, J. Maori Young People, Nationhood, and Land. In Space, Place, and Environment; Skelton, T., Ed.; Springer: New York, NY, USA, 2016; pp. 27–44. ISBN 978-981-287-043-8. [Google Scholar]
- Marques, B.; Freeman, C.; Carter, L.; Pedersen Zari, M. Sense of Place and Belonging in Developing Culturally Appropriate Therapeutic Environments: A Review. Societies 2020, 10, 83. [Google Scholar] [CrossRef]
- Murton, B. Being in the Place World: Toward a Māori “Geographical Self”. J. Cult. Geogr. 2012, 29, 87–104. [Google Scholar] [CrossRef]
- Kawharu, M. Ancestral Landscapes and World Heritage from a Māori Viewpoint. J. Polyn. Soc. 2009, 118, 317–338. [Google Scholar]
- Panelli, R.; Tipa, G. Placing Well-Being: A Maori Case Study of Cultural and Environmental Specificity. EcoHealth 2007, 4, 445–460. [Google Scholar] [CrossRef]
- McGowan, R. Keeping Alive the Practice of Traditional Māori Medicine in an Urbanised World. In Proceedings of the International Workshop on Colonisation, Indigenous Health and History, Stockholm, Sweden, 15–17 June 2015; pp. 15–17. [Google Scholar]
- Spiller, C.; Pio, E.; Erakovic, L.; Henare, M. Wise Up: Creating Organisational Wisdom Through an Ethic of Kaitiakitanga. J. Bus. Ethics 2011, 104, 223–235. [Google Scholar] [CrossRef]
- Riley, M. Māori Healing and Herbal: New Zealand Ethnobotanical Sourcebook; Viking Sevenseas N.Z.: Paraparaumu, New Zealand, 1994; ISBN 978-0-85467-095-6. [Google Scholar]
- Fau, T.F. Towards Human and Nature Reconciliation: A Māori Worldview Approach to Ecological Landscape Architecture. Master’s Thesis, Victoria University of Wellington, Wellington, New Zealand, 2015. [Google Scholar]
- Durie, M. Mauri Ora: The Dynamics of Maori Health; Oxford University Press: Auckland, New Zealand, 2001; ISBN 978-0-19-558418-9. [Google Scholar]
- Durie, M. Maori Knowledge and Medical Science. In Psychiatrists and Traditional Healers; Incayawar, M., Wintrob, R., Bouchard, L., Eds.; John Wiley & Sons, Ltd: Chichester, UK, 2009; pp. 237–249. ISBN 978-0-470-74105-4. [Google Scholar]
- Hatton, W.; Marques, B.; McIntosh, J. Mātauranga Māori and Therapeutic Landscapes; The International Academic Forum: Barcelona, Spain, 2017. [Google Scholar]
- Johnson, M. Adapting the Principles of Te Rongoā into Ecologically and Culturally Sustainable Farm Practice; University of Otago: Dunedin, New Zealand, 2012; p. 24. [Google Scholar]
- Chopra, A.; Doiphode, V.V. Ayurvedic Medicine: Core Concept, Therapeutic Principles, and Current Relevance. Med. Clin. N. Am. 2002, 86, 75–89. [Google Scholar] [CrossRef]
- Ahuriri-Driscoll, A.; Boulton, A.; Stewart, A.; Potaka-Osborne, G.; Hudson, M. Mā Mahi, Ka Ora: By Work, We Prosper--Traditional Healers and Workforce Development. N. Z. Med. J. 2015, 128, 34–44. [Google Scholar]
- McGowan, R. The Contemporary Use of Rongoā Māori: Traditional Māori Medicine. Master’s Thesis, University of Waikato, Hamilton, New Zealand, 2000. [Google Scholar]
- Statistics New Zealand Census of Population and Dwellings. 2013. Available online: http://archive.stats.govt.nz/Census/2013-census.aspx (accessed on 2 October 2019).
- Etikan, I.; Alkassim, R.; Abubakar, S. Comparison of Snowball Sampling and Sequential Sampling Technique. Biom. Biostat. Int. J. 2016, 3, 55. [Google Scholar]
- Haar, J.; Roche, M.; Brougham, D. Indigenous Insights into Ethical Leadership: A Study of Māori Leaders. J. Bus. Ethics 2019, 160, 621–640. [Google Scholar] [CrossRef]
- Smith, J.A.; Flowers, P.; Larkin, M. Interpretative Phenomenological Analysis: Theory, Method and Research; SAGE Publications: London, UK, 2009; ISBN 978-1-4462-4325-1. [Google Scholar]
- Barnes, H.M. Kaupapa Maori: Explaining the Ordinary. Pac. Health Dialog 2000, 7, 13–16. [Google Scholar] [PubMed]
- Smith, L.T. Decolonizing Methodologies: Research and Indigenous Peoples. In Decolonising Methodologies: Research and Indigenous Peoples; Zed Books: Dunedin, New Zealand, 1999; ISBN 978-1-85649-624-7. [Google Scholar]
- McIntosh, J.; Marques, B.; Hatton, W. Indigenous Cultural Knowledge for Therapeutic Landscape Design. In Handbook of Research on Methods and Tools for Assessing Cultural Landscape Adaptation; de Sousa Rosa, I., Lopes, J.C., Ribeiro, R., Mendes, A., Eds.; Practice, Progress, and Proficiency in Sustainability; IGI Global: Hershey, PA, USA, 2018; pp. 28–52. ISBN 978-1-5225-4186-8. [Google Scholar]
- Smith, J.A.; Jarman, M.; Osborn, M. Doing Interpretative Phenomenological Analysis. In Qualitative Health Psychology: Theories and Methods; Murray, M., Chamberlain, K., Eds.; Behaviour and Health Series; SAGE Publications: Thousand Oaks, CA, USA, 1999; pp. 218–240. ISBN 978-0-7619-5661-7. [Google Scholar]
- Lee, J. Decolonising Māori Narratives: Pūrākau as Method. MAI Rev. 2009, 2, 1–12. [Google Scholar]
- Jackson Pulver, L.; Haswell, M.; Ring, I.; Waldon, J.; Clark, W.; Whetung, V.; Graham, C.; Chino, M.; LaValley, J.; Sadana, R. Indigenous Health–Australia, Canada, Aotearoa New Zealand and the United States-Laying Claim to a Future That Embraces Health for Us All; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Rewi, T. Utilising Kaupapa Mäori Approaches to Initiate Research. MAI J. 2014, 3, 242–254. [Google Scholar]
- Mead, S.M. Tikanga Māori: Living by Māori Values; Huia Publishers: Wellington, New Zealand, 2003; ISBN 978-1-877283-88-8. [Google Scholar]
- Cram, F. Lessons on Decolonising Evaluation from Kaupapa Māori Evaluation. Can. J. Program Eval. 2015, 30, 296–312. [Google Scholar] [CrossRef]
- Attride-Stirling, J. Thematic Networks: An Analytic Tool for Qualitative Research. Qual. Res. 2001, 1, 385–405. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Salpitikorala, M. The “Other-Other” Perspective: Perceptions and Experiences of Non-Maori Ethnic-Minority Psychotherapists Practicing in the Bicultural Context of Aotearoa New Zealand. Master’s Thesis, Auckland University of Technology, Auckland, New Zealand, 2015. [Google Scholar]
- Kingi, T.K.R. “Hua Oranga”: Best Health Outcomes for Māori. Ph.D. Thesis, Massey University, Palmerston North, New Zealand, 2002. [Google Scholar]
- Holloway, I.; Todres, L. The Status of Method: Flexibility, Consistency and Coherence. Qual. Res. 2003, 3, 345–357. [Google Scholar] [CrossRef]
- Ihimaera, L. He Ara Ki Te Ao Mārama: A Pathway to Understanding the Facilitation of Taha Wairua in Mental Health Services. Master’s Thesis, Massey University, Palmerston North, New Zealand, 2004. [Google Scholar]
- Jones, B.; Ingham, T.; Davies, C.; Cram, F. Whānau Tuatahi: Māori Community Partnership Research Using a Kaupapa Māori Methodology. MAI Rev. 2010, 3, 1–14. [Google Scholar]
- Henare, M. Tapu, Mana, Mauri, Hau, Wairua: A Maori Philosophy of Vitalism and Cosmos. Indig. Tradit. Ecol. Interbeing Cosmol. Community 2001, 197–221. [Google Scholar]
- Pere, R. Te Wheke: A Celebration of Infinite Wisdom; Ao Ako Global Learning NZ: Gisborne, New Zealand, 1997; ISBN 978-0-9597994-9-1. [Google Scholar]
- Rollo, T.M.P. Ma Te Wai Ka Piki Ake Te Hauora. N. Z. J. Music Ther. 2013, 11, 51–80. [Google Scholar]
- Mark, G. Rongoā Māori (Traditional Māori Healing) through the Eyes of Māori Healers: Sharing the Healing While Keeping the Tapu. Ph.D. Thesis, Massey University, Auckland, New Zealand, 2012. [Google Scholar]
- Jones, R. Diagnosis in Traditional Maori Healing: A Contemporary Urban Clinic. Pac. Health Dialog 2000, 7, 17–24. [Google Scholar] [PubMed]
- Marques, B.; Grabasch, G.; McIntosh, J. Fostering Landscape Identity through Participatory Design with Indigenous Cultures of Australia and Aotearoa/New Zealand. Space Cult. 2018, 24, 37–52. [Google Scholar] [CrossRef]
- Durie, M. Identity, Nationhood and Implications. N. Z. J. Psychol. 1997, 26, 33. [Google Scholar]
- Royal, C. “Let the World Speak”: Towards Indigenous Epistemology; MKTA: Wellington, New Zealand, 2009; ISBN 978-0-9582955-1-2. [Google Scholar]
- Menzies, D.; Renata, A.; Whaanga-Schollum, D. Connecting Eco-Systems and Belief Systems through Regeneration and Innovation. X-Sect. J. 2016, 6, 98–105. [Google Scholar]
- Williams, A. Therapeutic Landscapes in Holistic Medicine. Soc. Sci. Med. 1998, 46, 1193–1203. [Google Scholar] [CrossRef]
- Burgess, C.P.; Johnston, F.H.; Bowman, D.M.J.S.; Whitehead, P.J. Healthy Country: Healthy People? Exploring the Health Benefits of Indigenous Natural Resource Management. Aust. N. Z. J. Public Health 2005, 29, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Datta, R. A Relational Theoretical Framework and Meanings of Land, Nature, and Sustainability for Research with Indigenous Communities. Local Environ. 2015, 20, 102–113. [Google Scholar] [CrossRef]
- Greenwood, M.; de Leeuw, S. Teachings from the Land: Indigenous People, Our Health, Our Land, and Our Children. Can. J. Nativ. Educ. 2007, 30, 48–53. [Google Scholar]
- Marques, B.; Freeman, C.; Carter, L.; Pedersen Zari, M. Conceptualising Therapeutic Environments through Culture, Indigenous Knowledge and Landscape for Health and Well-Being. Sustainability 2021, 13, 9125. [Google Scholar] [CrossRef]
- Wilson, K. Therapeutic Landscapes and First Nations Peoples: An Exploration of Culture, Health and Place. Health Place 2003, 9, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Mazuch, R. Salutogenic and Biophilic Design as Therapeutic Approaches to Sustainable Architecture. Archit. Des. 2017, 87, 42–47. [Google Scholar] [CrossRef]
- Souter-Brown, G. The Salutogenic Design Process. In Landscape and Urban Design for Health and Well-being: Using Healing, Sensory and Therapeutic Gardens; Routledge: Oxon, UK, 2015; pp. 201–213. ISBN 978-0-415-84351-5. [Google Scholar]
- Eriksson, M. Unravelling the Mystery of Salutogenesis: The Evidence Base of the Salutogenic Research as Measured by Antonovsky’s Sense of Coherence Scale. In Research Report/Folkhälsan Research Centre, Health Promotion Research Programme, 2nd ed.; Folkhälsan Research Centre: Helsinki, Finland, 2007; ISBN 978-952-5641-14-1. [Google Scholar]
- Suominen, S.; Lindstrom, B. Salutogenesis. Scand J. Public Health 2008, 36, 337–339. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Open-Ended Questions | Dichotomous Questions (Yes or No) |
|---|---|
| Can you explain what rongoā means to you? How does it work? | Do you live in your rohe (tribal boundaries)? |
| What is the relationship between healing and mātauranga (knowledge) and tikanga (customs) Māori? What is the relationship with the wider landscape/nature? | Do you live in the city? |
| How could we use the landscape to maintain our health and wellbeing? | Do whānau (family) live nearby? |
| Are there places that have special meaning for you? What are the qualities of the place/s that mean it is good to harvest from? | Do you provide help to whānau (family)? |
| What do you consider when practicing rongoā? | Do you have mokopuna (grandchildren) or tamariki (children)? |
| How do you see rongoā and other modes of traditional healing being passed on? How do you make sure that rongoā is around for future generations? | Do you have links with your local marae (Māori meeting places) or haukāinga (local people of a marae)? |
| What kind of relationship should Māori traditional healing have with mainstream health services? | Do you collect any plants, berries, other materials for rongoā? |
| What are some of the ways in which you ensure your practice is protected? | Are there ngahere (forest), rākau (plants) or awa/moana (river/lake) near you that you use? |
| Step | Description |
|---|---|
| 1. Data Familiarisation | Transcription, reading and re-reading of data, initial ideas |
| 2. Codes | Identification and organisation of the data into overarching codes |
| 3. Themes | Interpretation of data and collation of codes into potential themes based on patterns and commonalities found |
| 4. Review | Identified themes and sub-themes will be rechecked and refined in relation to the coded extracts and then the entire data set |
| 5. Define and Name | Revision and refinement of the higher themes in relation to lower themes (and vice-versa) to ensure consistency, generating clear definitions and names for each theme |
| 6. Results | Report on findings. A compelling narrative where the themes are weaved together with data extracts is required |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, B.; Freeman, C.; Carter, L. Adapting Traditional Healing Values and Beliefs into Therapeutic Cultural Environments for Health and Well-Being. Int. J. Environ. Res. Public Health 2022, 19, 426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010426
Marques B, Freeman C, Carter L. Adapting Traditional Healing Values and Beliefs into Therapeutic Cultural Environments for Health and Well-Being. International Journal of Environmental Research and Public Health. 2022; 19(1):426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010426
Chicago/Turabian StyleMarques, Bruno, Claire Freeman, and Lyn Carter. 2022. "Adapting Traditional Healing Values and Beliefs into Therapeutic Cultural Environments for Health and Well-Being" International Journal of Environmental Research and Public Health 19, no. 1: 426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010426