
Chronic Pain among Individuals Experiencing Homelessness and Its Interdependence with Opioid and Other Substance Use and Mental Illness

 ,
,
Abstract
:1. Introduction
2. Methods
Statistical Analysis
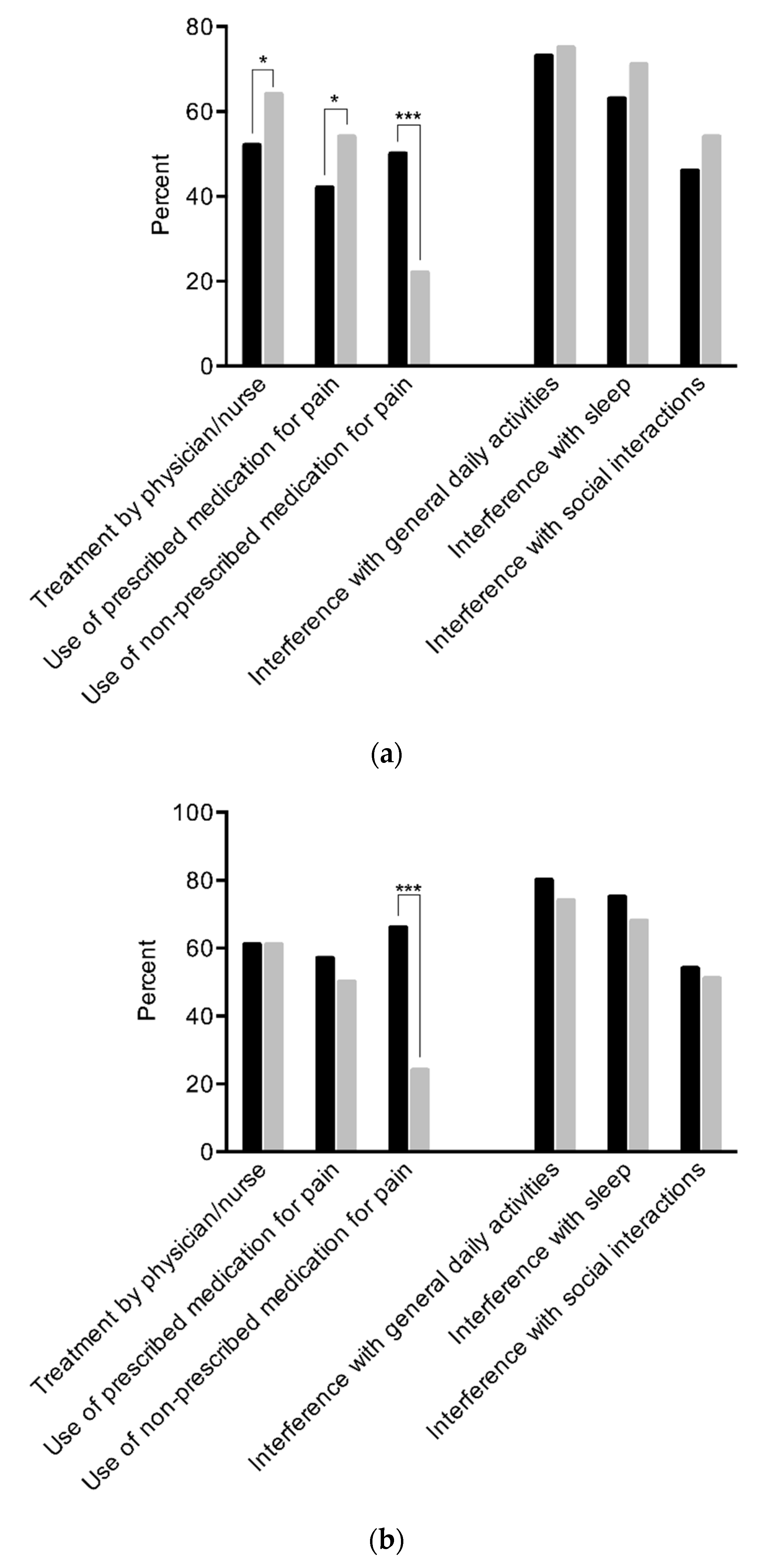
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The U.S. Department of Housing and Urban Development. The 2020 Annual Homeless Assessment Report (AHAR) to Congress—PART 1: Point-in-Time Estimates of Homelessness; The U.S. Department of Housing and Urban Development: Washington, DC, USA, 2021.
- Gaetz, S.; Dej, E.; Richter, T.; Redman, M. The State of Homelessness in Canada: 2016; Canadian Homelessness Research Network: Toronto, ON, Canada, 2016. [Google Scholar]
- Fazel, S.; Geddes, J.R.; Kushel, M. The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet 2014, 384, 1529–1540. [Google Scholar] [CrossRef] [Green Version]
- Raoult, D. Infections in the homeless. Lancet Infect. Dis. 2001, 1, 77–84. [Google Scholar] [CrossRef]
- Stratigos, A.J.; Stern, R.; Gonzalez, E.; Johnson, R.A.; O’Connell, J.; Dover, J.S. Prevalence of skin disease in a cohort of shelter-based homeless men. J. Am. Acad. Dermatol. 1999, 41, 197–202. [Google Scholar] [CrossRef]
- Gelberg, L.; Linn, L.S.; Usatine, R.P.; Smith, M.H. Health, homelessness, and poverty. A study of clinic users. Arch. Intern. Med. 1990, 150, 2325–2330. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.D. Poor people, poor health: The health status of the homeless. J. Soc. Issues 1990, 46, 49–64. [Google Scholar] [CrossRef]
- Fazel, S.; Khosla, V.; Doll, H.; Geddes, J. The prevalence of mental disorders among the homeless in western countries: Systematic review and meta-regression analysis. PLoS Med. 2008, 5, e225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torchalla, I.; Strehlau, V.; Li, K.; Krausz, M. Substance use and predictors of substance dependence in homeless women. Drug Alcohol Depend. 2011, 118, 173–179. [Google Scholar] [CrossRef]
- Schütz, C.; Choi, F.; Jae Song, M.; Wesarg, C.; Li, K.; Krausz, M. Living with dual diagnosis and homelessness: Marginalized within a marginalized group. J. Dual Diagn. 2019, 15, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.W.; Wilkins, E.; Chambers, C.; Estrabillo, E.; Berends, J.; MacDonald, A. Chronic pain among homeless persons: Characteristics, treatment, and barriers to management. BMC Fam. Pract. 2011, 12, 73. [Google Scholar] [CrossRef] [Green Version]
- Krausz, R.M.; Clarkson, A.F.; Strehlau, V.; Torchalla, I.; Li, K.; Schuetz, C.G. Mental disorder, service use, and barriers to care among 500 homeless people in 3 different urban settings. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1235–1243. [Google Scholar] [CrossRef]
- Zhang, L.; Norena, M.; Gadermann, A.; Hubley, A.; Russell, L.; Aubry, T.; To, M.J.; Farrell, S.; Hwang, S.; Palepu, A. Concurrent disorders and health care utilization among homeless and vulnerably housed persons in Canada. J. Dual Diagn. 2018, 14, 21–31. [Google Scholar] [CrossRef]
- Hwang, S.W.; Burns, T. Health interventions for people who are homeless. Lancet 2014, 384, 1541–1547. [Google Scholar] [CrossRef]
- Bauer, L.K.; Brody, J.K.; León, C.; Baggett, T.P. Characteristics of homeless adults who died of drug overdose: A retrospective record review. J. Health Care Poor Underserved 2016, 27, 846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, R.; Ewing, J.J.J.; Garrett, A.; Harrison, E.K.; Lwin, K.K.; Wheeler, D.W. The Nature and Prevalence of Chronic Pain in Homeless Persons: An Observational Study. F1000Research 2013, 2, 2–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogel, M.; Frank, A.; Choi, F.; Strehlau, V.; Nikoo, N.; Nikoo, M.; Hwang, S.W.; Somers, J.; Krausz, M.R.; Schütz, C.G. Chronic pain among homeless persons with mental illness. Pain Med. 2017, 18, 2280–2288. [Google Scholar] [CrossRef] [PubMed]
- Krashin, D.; Murinova, N.; Ballantyne, J. Management of pain with comorbid substance abuse. Curr. Psychiatry Rep. 2012, 14, 462–468. [Google Scholar] [CrossRef]
- Voon, P.; Callon, C.; Nguyen, P.; Dobrer, S.; Montaner, J.; Wood, E.; Kerr, T. Self-management of pain among people who inject drugs in Vancouver. Pain Manag. 2014, 4, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voon, P.; Callon, C.; Nguyen, P.; Dobrer, S.; Montaner, J.S.G.; Wood, E.; Kerr, T. Denial of prescription analgesia among people who inject drugs in a Canadian setting. Drug Alcohol Rev. 2015, 34, 221–228. [Google Scholar] [CrossRef] [Green Version]
- Feodor Nilsson, S.; Hjorthøj, C.R.; Erlangsen, A.; Nordentoft, M. Suicide and unintentional injury mortality among homeless people: A Danish nationwide register-based cohort study. Eur. J. Public Health 2013, 24, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miaskowski, C.; Penko, J.M.; Guzman, D.; Mattson, J.E.; Bangsberg, D.R.; Kushel, M.B. Occurrence and characteristics of chronic pain in a community-based cohort of indigent adults living with HIV infection. J. Pain 2011, 12, 1004–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stergiopoulos, V.; Hwang, S.W.; Gozdzik, A.; Nisenbaum, R.; Latimer, E.; Rabouin, D.; Adair, C.E.; Bourque, J.; Connelly, J.; Frankish, J. Effect of scattered-site housing using rent supplements and intensive case management on housing stability among homeless adults with mental illness: A randomized trial. JAMA 2015, 313, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Janavs, J.; Weiller, E.; Keskiner, A.; Schinka, J.; Knapp, E.; Sheehan, M.F.; Dunbar, G.C. The validity of the Mini International Neuropsychiatric Interview (MINI) according to the SCID-P and its reliability. Eur. Psychiatry 1997, 12, 232–241. [Google Scholar] [CrossRef]
- Cunningham, J.; Craner, J.; Evans, M.; Hooten, W.M. Benzodiazepine use in patients with chronic pain in an interdisciplinary pain rehabilitation program. J. Pain Res. 2017, 10, 311–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goering, P.N.; Streiner, D.L.; Adair, C.; Aubry, T.; Barker, J.; Distasio, J.; Hwang, S.W.; Komaroff, J.; Latimer, E.; Somers, J.; et al. The at Home/Chez Soi trial protocol: A pragmatic, multi-site, randomised controlled trial of a Housing First intervention for homeless individuals with mental illness in five Canadian cities. BMJ Open 2011, 1, e000323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsden, J.; Gossop, M.; Stewart, D.; Best, D.; Farrell, M.; Lehmann, P.; Edwards, C.; Strang, J. The Maudsley Addiction Profile (MAP): A brief instrument for assessing treatment outcome. Addiction 1998, 93, 1857–1867. [Google Scholar] [CrossRef]
- Khantzian, E.J.; Treece, C. DSM-III psychiatric diagnosis of narcotic addicts: Recent findings. Arch. Gen. Psychiatry 1985, 42, 1067–1071. [Google Scholar] [CrossRef]
- Krausz, M.; Verthein, U.; Degkwitz, P. Psychiatric comorbidity in opiate addicts. Eur. Addict. Res. 1999, 5, 55–62. [Google Scholar] [CrossRef]
- Ballantyne, J.C.; LaForge, S.K. Opioid dependence and addiction during opioid treatment of chronic pain. Pain 2007, 129, 235–255. [Google Scholar] [CrossRef]
- Nielsen, S.; Lintzeris, N.; Bruno, R.; Campbell, G.; Larance, B.; Hall, W.; Hoban, B.; Cohen, M.L.; Degenhardt, L. Benzodiazepine Use among Chronic Pain Patients Prescribed Opioids: Associations with Pain, Physical and Mental Health, and Health Service Utilization. Pain Med. 2015, 16, 356–366. [Google Scholar] [CrossRef] [Green Version]
- Compton, M.A. Cold-pressor pain tolerance in opiate and cocaine abusers: Correlates of drug type and use status. J. Pain Symptom Manag. 1994, 9, 462–473. [Google Scholar] [CrossRef]
- Beliveau, C.M.; McMahan, V.M.; Arenander, J.; Angst, M.S.; Kushel, M.; Torres, A.; Santos, G.-M.; Coffin, P.O. Stimulant use for self-management of pain among safety-net patients with chronic non-cancer pain. Subst. Abus. 2021, 1–8. [Google Scholar] [CrossRef]
- Larney, S.; Peacock, A.; Mathers, B.M.; Hickman, M.; Degenhardt, L. A systematic review of injecting-related injury and disease among people who inject drugs. Drug Alcohol Depend. 2017, 171, 39–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, J.S.; Prather, K.; Weiss, R.D. Physical Pain and Associated Clinical Characteristics in Treatment-Seeking Patients in Four Substance Use Disorder Treatment Modalities. Am. J. Addict. 2008, 17, 121–125. [Google Scholar] [CrossRef]
- Atkinson, J.H.; Slater, M.A.; Patterson, T.L.; Grant, I.; Garfin, S.R. Prevalence, onset, and risk of psychiatric disorders in men with chronic low back pain: A controlled study. Pain 1991, 45, 111–121. [Google Scholar] [CrossRef]
- Kroenke, K.; Wu, J.; Bair, M.J.; Krebs, E.E.; Damush, T.M.; Tu, W. Reciprocal Relationship Between Pain and Depression: A 12-Month Longitudinal Analysis in Primary Care. J. Pain 2011, 12, 964–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooten, W.M. Chronic Pain and Mental Health Disorders: Shared Neural Mechanisms, Epidemiology, and Treatment. Mayo Clin. Proc. 2016, 91, 955–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total (N = 828) N (%) | Participants with Chronic Pain N (%) | Participants without Chronic Pain N (%) | p a | |
|---|---|---|---|---|
| Gender | 0.682 | |||
| Male | 572 (69) | 310 (69) | 262 (69) | |
| Female | 244 (30) | 133 (30) | 111 (29) | |
| Other | 12 (1) | 5 (1) | 7 (2) | |
| Study Site | ||||
| Toronto | 414 (50) | 225 (50) | 189 (50) | 0.889 |
| Vancouver | 414 (50) | 223 (50) | 191 (50) | |
| Country of Birth (N = 826) | 0.609 | |||
| Canada | 595 (72) | 326 (73) | 269 (71) | |
| Outside Canada | 231 (28) | 122 (27) | 109 (29) | |
| Race/Ethnicity | 0.079 | |||
| Aboriginal | 89 (11) | 43 (10) | 46 (12) | |
| Ethnoracial b | 345 (42) | 176 (39) | 169 (45) | |
| White | 394 (48) | 229 (51) | 165 (43) | |
| Education (N = 824) | 0.746 | |||
| Incomplete high school | 429 (52) | 234 (53) | 195 (52) | |
| Completed high school | 395 (48) | 211 (47) | 184 (49) | |
| Marital status (N = 825) | 0.001 | |||
| Married/partnered | 37 (5) | 25 (6) | 12 (3) | |
| Divorced/separated/widowed | 216 (26) | 137 (31) | 97 (21) | |
| Single/never married | 572 (69) | 284 (64) | 288 (76) | |
| Primary employment status (N = 825) | 0.827 | |||
| Unemployed | 770 (93) | 415 (93) | 355 (94) | |
| Employed or self-employed | 31 (4) | 18 (4) | 13 (3) | |
| Other | 24 (3) | 14 (3) | 10 (3) | |
| Intervention arm | 0.423 | |||
| Treatment as usual | 326 (39) | 182 (41) | 144 (38) | |
| Housing first | 502 (61) | 266 (59) | 236 (62) | |
| Wartime service (N = 819) | 39 (5) | 27 (6) | 12 (3) | 0.058 |
| Total (N = 828) N (%) | Participants with Chronic Pain N (%) | Participants without Chronic Pain N (%) | p a | |
|---|---|---|---|---|
| Major Depressive Episode b | 319 (39) | 205 (46) | 114 (30) | <0.001 |
| Manic or Hypomanic Episode b | 131 (16) | 82 (18) | 49 (13) | 0.034 |
| Post-traumatic Stress Disorder b (N = 827) | 214 (26) | 139 (31) | 75 (20) | <0.001 |
| Panic Disorder b | 148 (18) | 104 (23) | 44 (12) | <0.001 |
| Mood Disorder with Psychotic Features b (N = 827) | 158 (19) | 96 (22) | 62 (16) | 0.060 |
| Psychotic Disorder b | 365 (44) | 174 (39) | 191 (50) | 0.001 |
| Any substance use (N = 806) | 535 (66) | 301 (69) | 234 (63) | 0.067 |
| Alcohol use | 367 (44) | 204 (46) | 163 (43) | 0.446 |
| Opioid c use (N = 818) | 89 (11) | 57 (13) | 32 (9) | 0.047 |
| Sedative use (N = 823) | 13 (2) | 8 (2) | 5 (1) | 0.580 |
| Stimulant use d (N = 817) | 234 (29) | 141 (32) | 93 (25) | 0.025 |
| THC use (N = 827) | 290 (35) | 163 (36) | 127 (34) | 0.388 |
| Daily use of any substance (N = 819) | 200 (24) | 127 (29) | 73 (19) | 0.002 |
| Polysubstance (≥3) use (N = 806) | 118 (15) | 77 (18) | 41 (11) | 0.008 |
| Injection use (N = 818) | 82 (10) | 56 (13) | 26 (7) | 0.007 |
| Odds Ratio | 95% CI | p-Value | S.E. | Wald | Df | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Age | 1.038 | 1.023 | 1.052 | <0.001 | 0.007 | 27.924 | 1 |
| Major depressive episode | 1.545 | 1.125 | 2.122 | 0.007 | 0.162 | 7.225 | 1 |
| Post-Traumatic Stress Disorder | 1.623 | 1.132 | 2.325 | 0.008 | 0.183 | 6.957 | 1 |
| Panic disorder | 1.756 | 1.161 | 2.656 | 0.008 | 0.211 | 7.108 | 1 |
| Daily substance use | 1.458 | 1.020 | 2.085 | 0.039 | 0.182 | 4.274 | 1 |
| Injection use | 1.810 | 1.076 | 3.047 | 0.025 | 0.266 | 4.994 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vogel, M.; Choi, F.; Westenberg, J.N.; Cabanis, M.; Nikoo, N.; Nikoo, M.; Hwang, S.W.; Somers, J.; Schütz, C.G.; Krausz, M. Chronic Pain among Individuals Experiencing Homelessness and Its Interdependence with Opioid and Other Substance Use and Mental Illness. Int. J. Environ. Res. Public Health 2022, 19, 5. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010005
Vogel M, Choi F, Westenberg JN, Cabanis M, Nikoo N, Nikoo M, Hwang SW, Somers J, Schütz CG, Krausz M. Chronic Pain among Individuals Experiencing Homelessness and Its Interdependence with Opioid and Other Substance Use and Mental Illness. International Journal of Environmental Research and Public Health. 2022; 19(1):5. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010005
Chicago/Turabian StyleVogel, Marc, Fiona Choi, Jean N. Westenberg, Maurice Cabanis, Nooshin Nikoo, Mohammadali Nikoo, Stephen W. Hwang, Julian Somers, Christian G. Schütz, and Michael Krausz. 2022. "Chronic Pain among Individuals Experiencing Homelessness and Its Interdependence with Opioid and Other Substance Use and Mental Illness" International Journal of Environmental Research and Public Health 19, no. 1: 5. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010005