
Personal Exposure to Fine Particles (PM2.5) in Northwest Africa: Case of the Urban City of Bamako in Mali

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
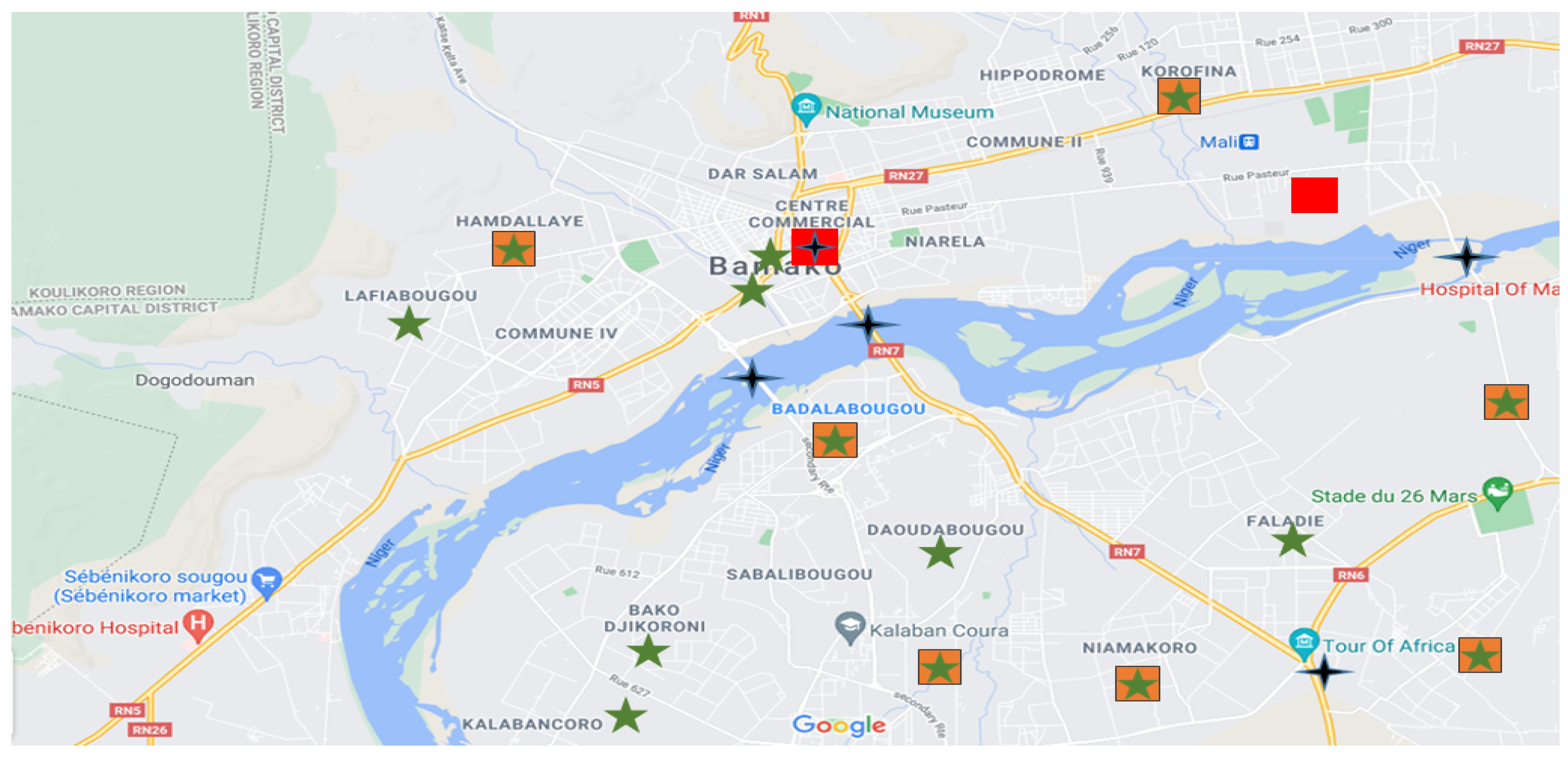
2.1. Sampling Location
2.2. Materials
2.3. Sampling Procedure
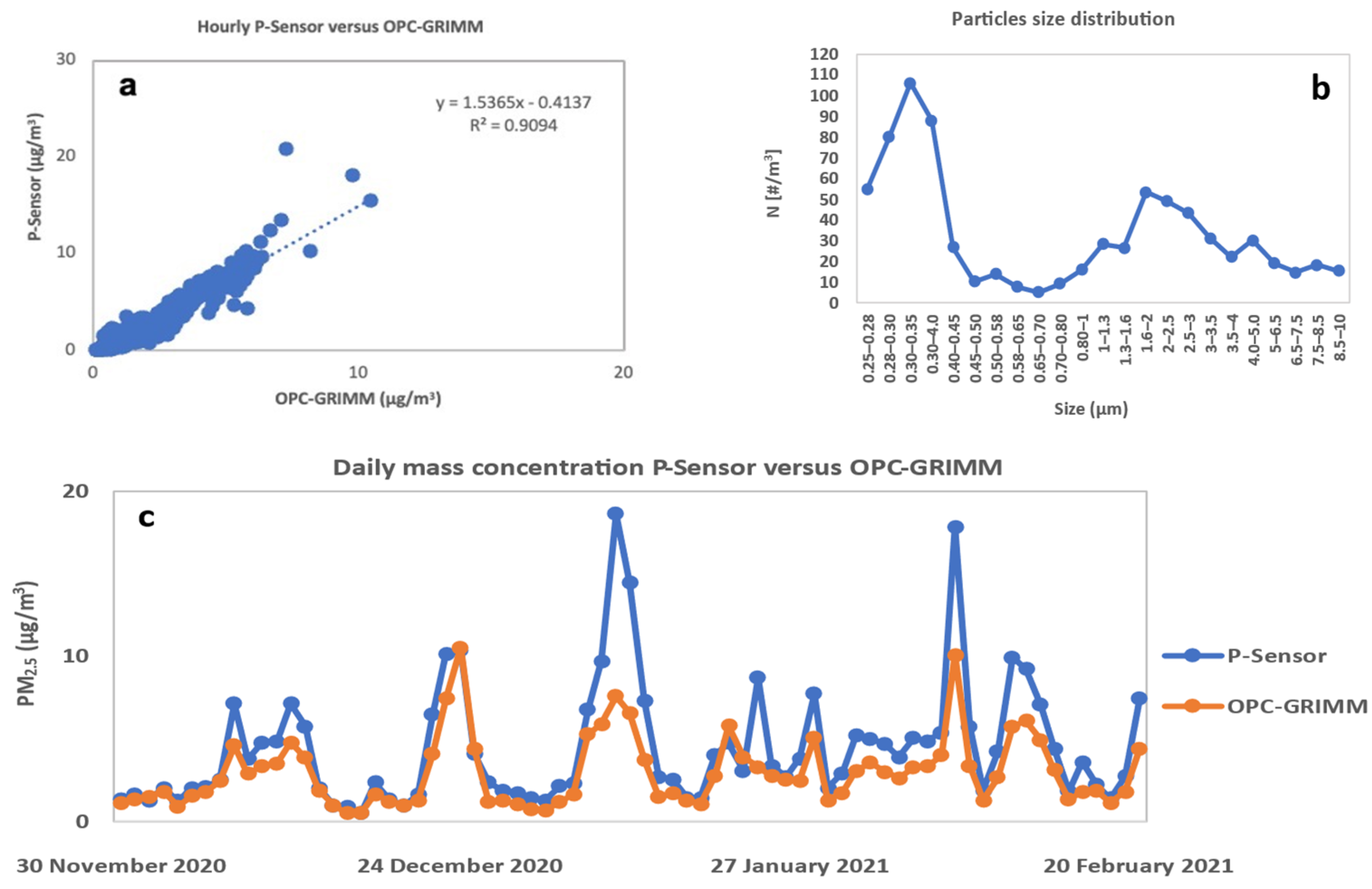
2.4. Quality Assurance and Control
2.5. Data Analysis
Personal Exposure Calculation Method: Case of the Office Workers
3. Results
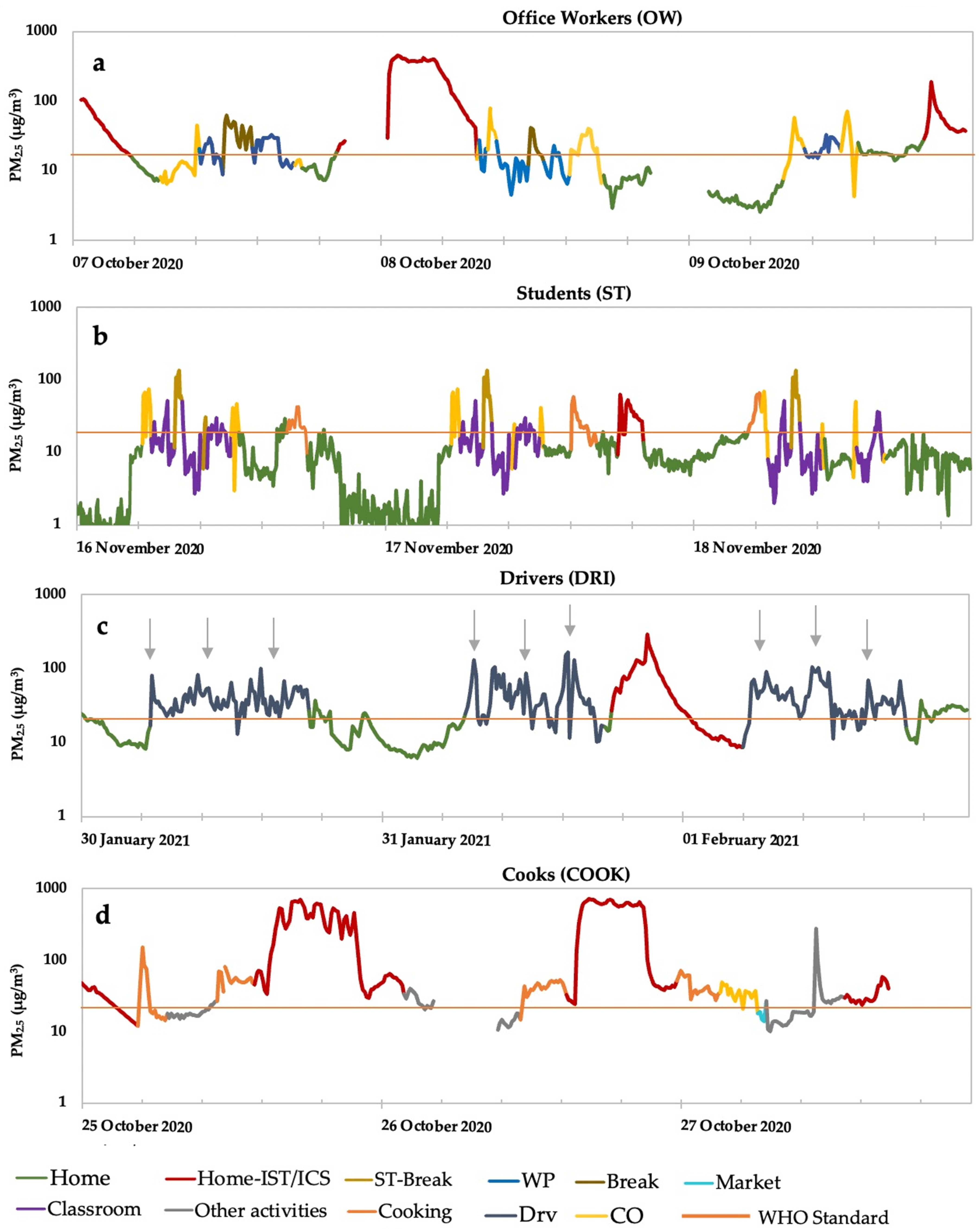
3.1. Daily Time-Series of PM2.5 Concentration
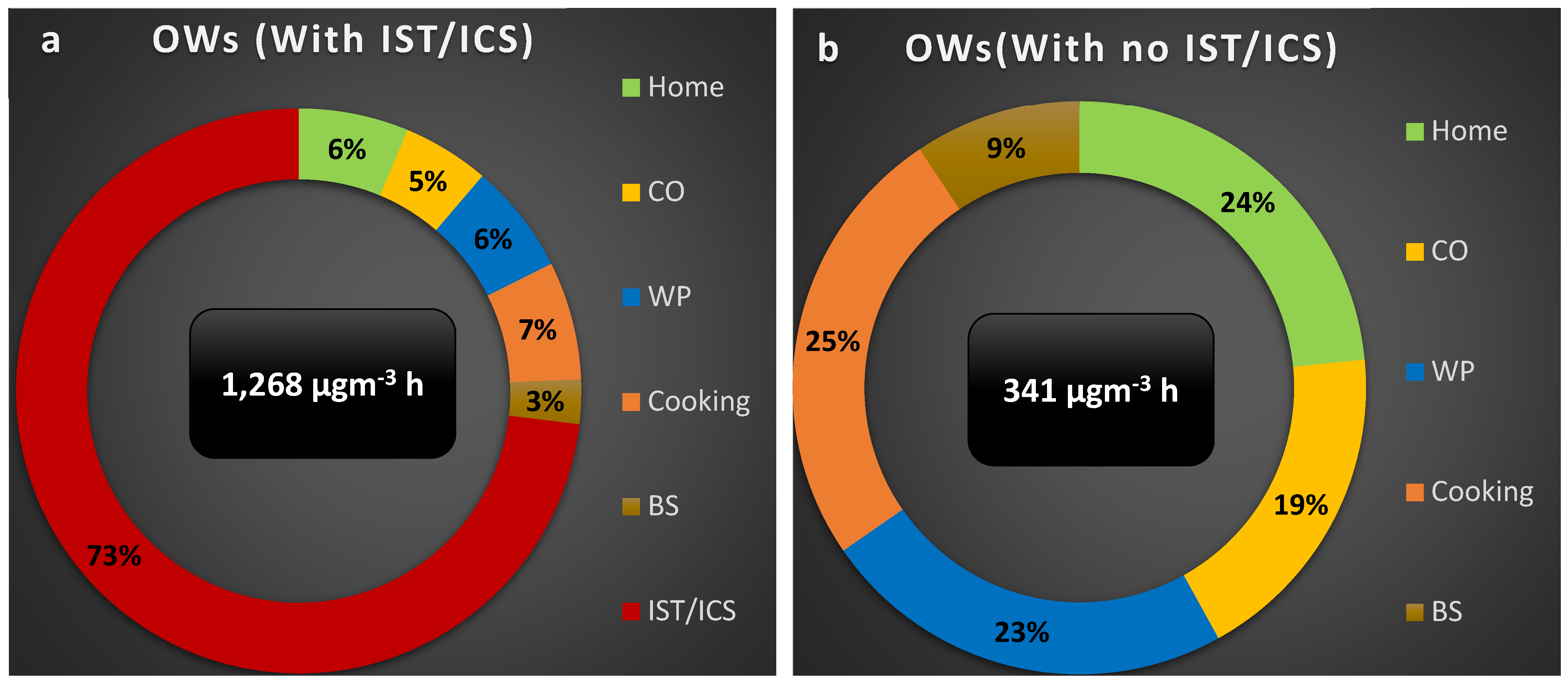
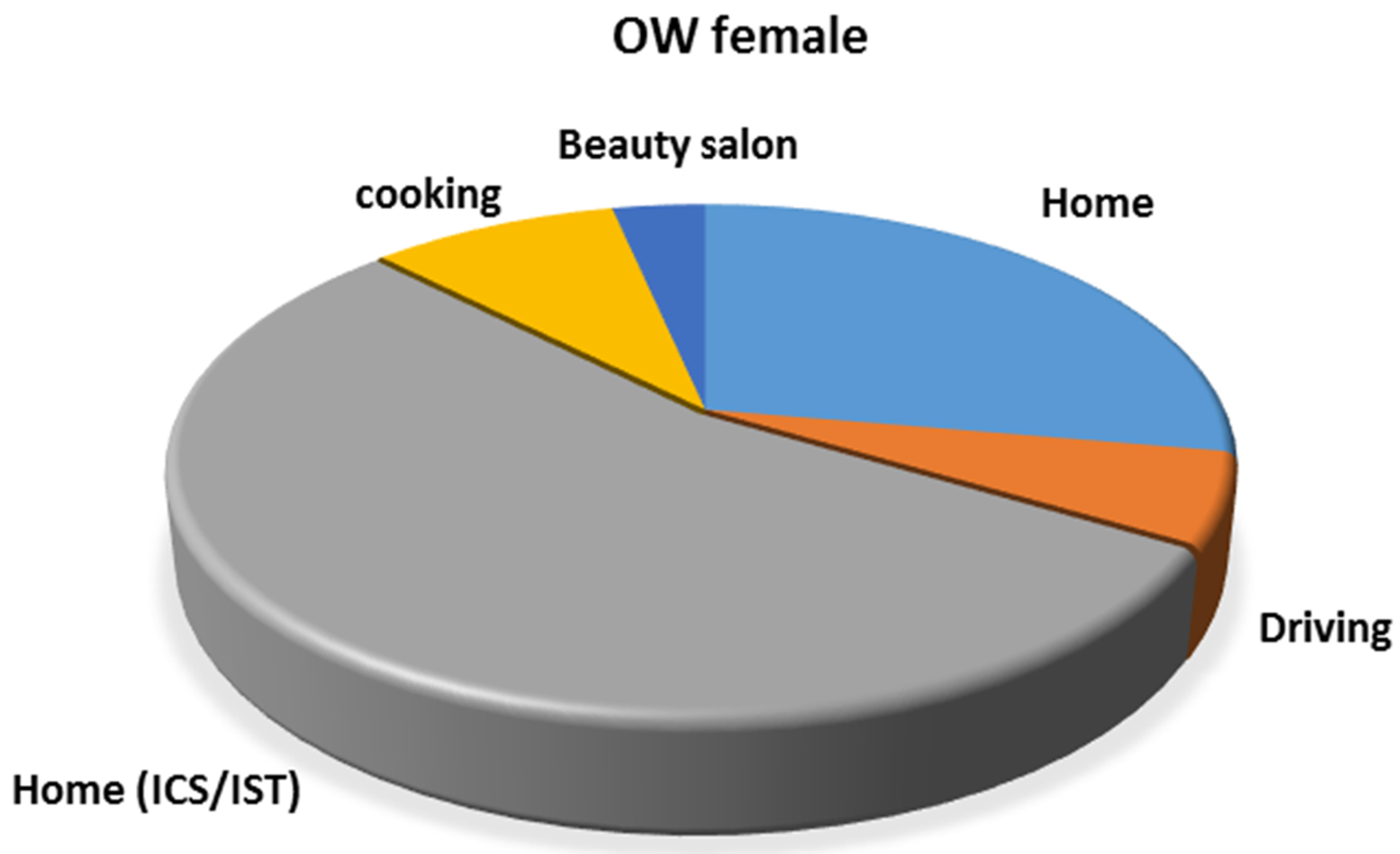
3.1.1. OW
3.1.2. ST
3.1.3. DRI
3.1.4. COOK
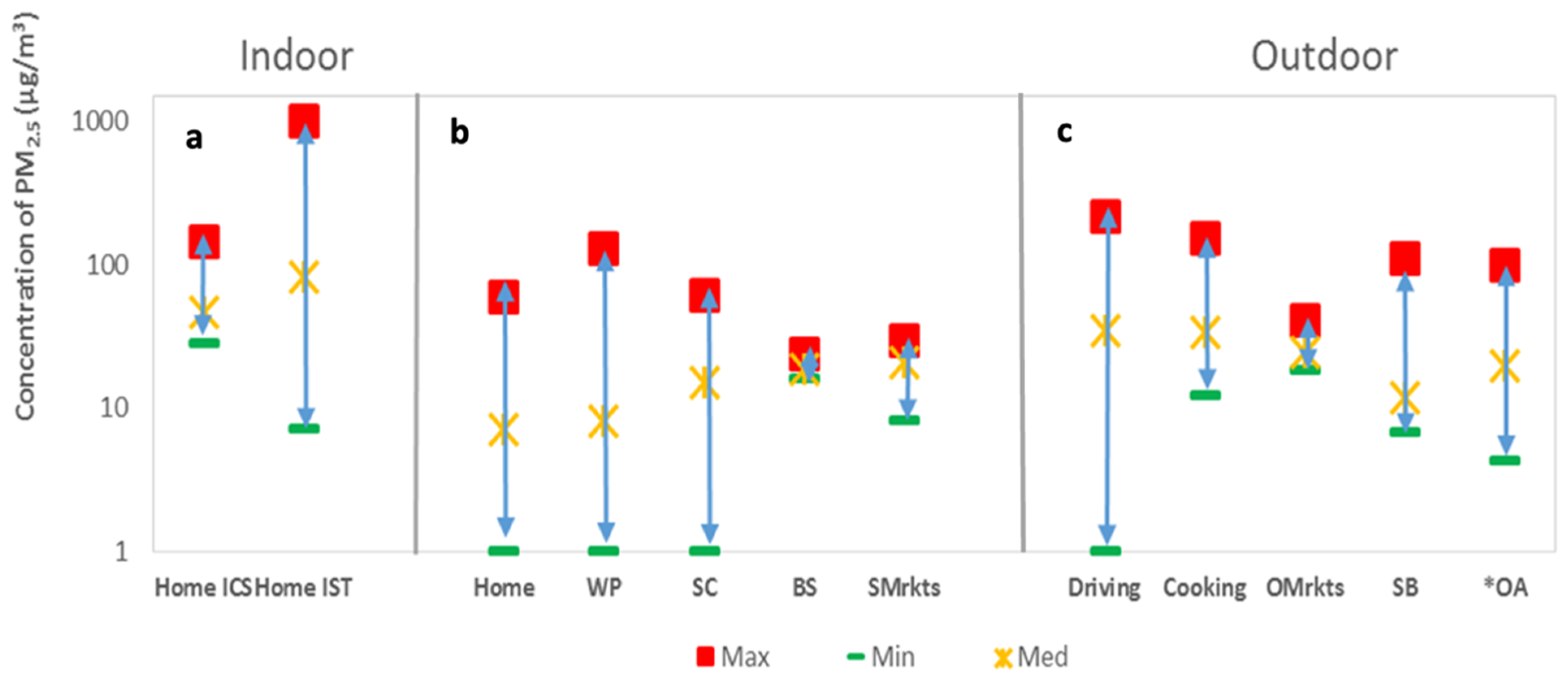
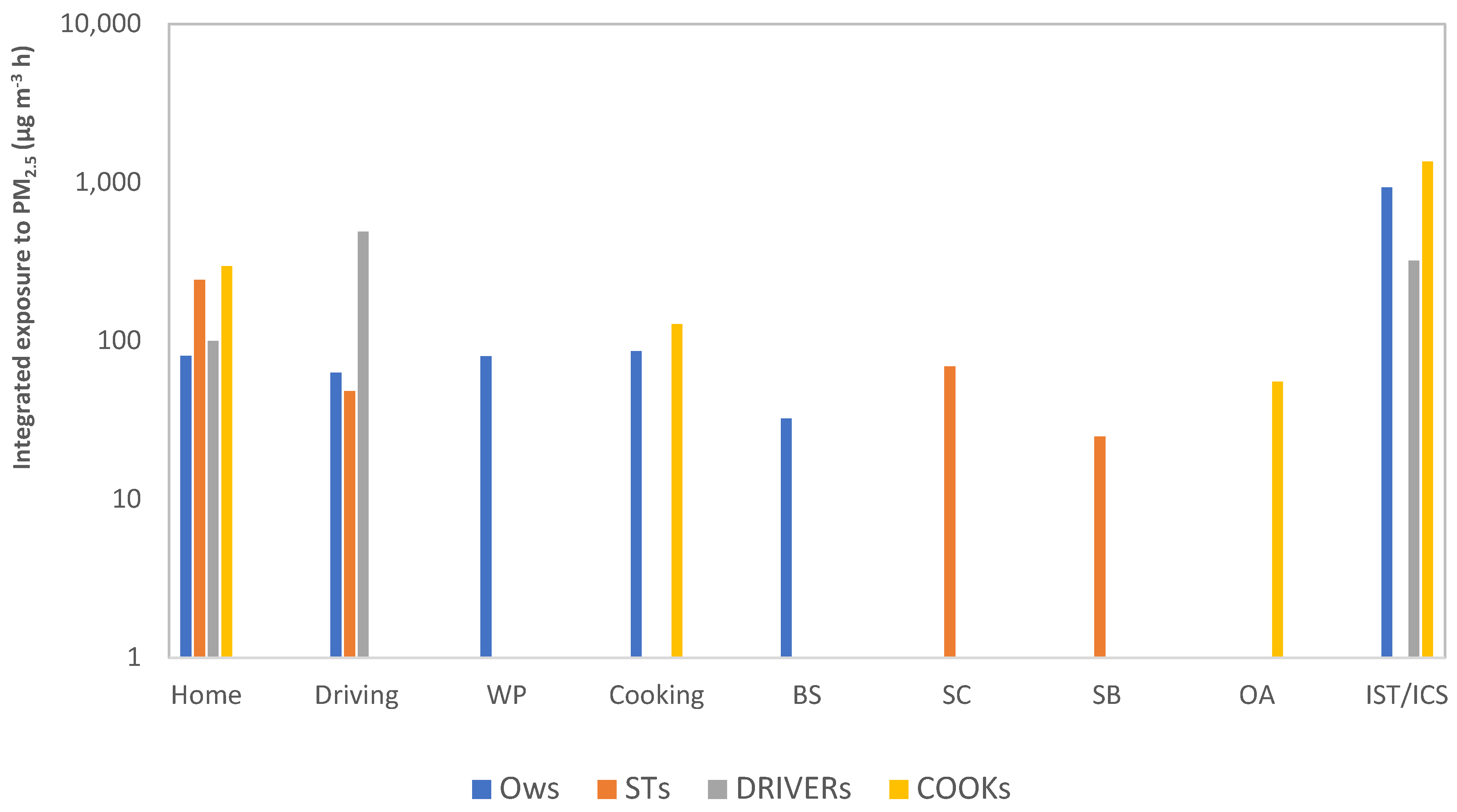
3.2. Comparison of Different Groups
4. Discussion
4.1. Identification of Activities Producing Greatest Exposure to PM2.5
4.2. Comparison of PM2.5 Concentration with WHO Standards and Health Effects
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seinfeld, J.H.; Pandis, S.N. Atmospheric Chemistry and Physics from Air Pollution to Climate Change, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2006. [Google Scholar]
- Jacob, D.J. Introduction to Atmospheric Chemistry; Princeton University Press: Chichester, UK, 1999. [Google Scholar]
- Penttinen, P.; Timonen, K.L.; Tiittanen, P.; Mirme, A.; Ruuskanen, J.; Pekkanen, J. Number Concentration and Size of Particles in Urban Air: Effects on Spirometric Lung Function in Adult Asthmatic Subjects. Environ. Health Perspect. 2001, 109, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, S.; Dey, S.; Guttikunda, S.; Pillarisetti, A.; Smith, K.R.; Di Girolamo, L. Indian annual ambient air quality standard is achievable by completely mitigating emissions from household sources. Proc. Natl. Acad. Sci. USA 2019, 116, 10711–10716. [Google Scholar] [CrossRef] [Green Version]
- Miller, L.; Xu, X. Ambient PM2.5 Human Health Effects—Findings in China and Research Directions. Atmosphere 2018, 9, 424. [Google Scholar] [CrossRef] [Green Version]
- Sicard, P.; Khaniabadi, Y.O.; Perez, S.; Gualtieri, M.; De Marco, A. Effect of O3, PM10 and PM2.5 on cardiovascular and respiratory diseases in cities of France, Iran and Italy. Environ. Sci. Pollut. Res. 2019, 26, 32645–32665. [Google Scholar] [CrossRef]
- Wang, B.; Eum, K.-D.; Kazemiparkouhi, F.; Li, C.; Manjourides, J.; Pavlu, V.; Suh, H. The impact of long-term PM2.5 exposure on specific causes of death: Exposure-response curves and effect modification among 53 million U.S. Medicare beneficiaries. Environ. Health 2020, 19, 20. [Google Scholar] [CrossRef] [Green Version]
- Agbo, K.E.; Walgraeve, C.; Eze, J.I.; Ugwoke, P.E.; Ukoha, P.O.; Van Langenhove, H. A review on ambient and indoor air pollution status in Africa. Atmos. Pollut. Res. 2020, 12, 243–260. [Google Scholar] [CrossRef]
- Katoto, P.D.; Byamungu, L.; Brand, A.S.; Mokaya, J.; Strijdom, H.; Goswami, N.; De Boever, P.; Nawrot, T.S.; Nemery, B. Ambient air pollution and health in Sub-Saharan Africa: Current evidence, perspectives and a call to action. Environ. Res. 2019, 173, 174–188. [Google Scholar] [CrossRef] [PubMed]
- Lamri, N.; Hocine, A.K.; Salah, K. Particulate matter from road traffic in Africa. J. Earth Sci. Geotech. Eng. 2017, 7, 289–304. [Google Scholar]
- Bruce, N.; Perez-Padilla, R.; Albalak, R. Indoor air pollution in developing countries: A major environmental and public health challenge. Bull. World Health Organ. 2000, 78, 1078–1092. [Google Scholar]
- Vliet, E.D.S.V.; Asante, K.; Jack, D.W.; Kinney, P.L.; Whyatt, R.M.; Chillrud, S.N.; Abokyi, L.; Zandoh, C.; Owusu-Agyei, S. Personal exposures to fine particulate matter and black carbon in households cooking with biomass fuels in rural Ghana. Environ. Res. 2013, 127, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Tefera, W.; Kumie, A.; Berhane, K.; Gilliland, F.; Lai, A.; Sricharoenvech, P.; Samet, J.; Patz, J.; Schauer, J.J. Chemical Characterization and Seasonality of Ambient Particles (PM2.5) in the City Centre of Addis Ababa. Int. J. Environ. Res. Public Health 2020, 17, 6998. [Google Scholar] [CrossRef] [PubMed]
- Togola, M. Pollution de l’air à Bamako: Un seuil (très) critique. J. Sci. Tech. Du Mali. 2017. [Google Scholar]
- Ministere De L’environnement, De L’assainissement et Du Developpement Durable (MEADD). Rapport Troisieme Commmunication Nationale Du Mali A La Convention Cadre Des Nations Unies Sur Les Changements Climatiques. 239. Mali. 2017. Available online: https://chm.cbd.int/api/v2013/documents/7DD41D1F-F5C7-60E6-3987-14624F6A9F90/attachments/RAPPORT_FINAL_TCN_09_01_18.pdf (accessed on 7 June 2021).
- Dembele, S. Dynamique Socio-Spatiale de la Ville de Bamako et Environs. Normandie Université. 2017. Available online: https://horizon.documentation.ird.fr/exl-doc/pleins_textes/divers19-04/010075426.pdf (accessed on 6 September 2021).
- Institut National de la Statistique (INSTAT). Malikunnafoni, Version 1.0.1; Mobil Application Software: Bamako, Mali, 2020. [Google Scholar]
- Nakayama, T.; Matsumi, Y.; Kawahito, K.; Watabe, Y. Development and evaluation of a palm-sized optical PM2.5 sensor. Aerosol Sci. Technol. 2018, 52, 2–12. [Google Scholar] [CrossRef] [Green Version]
- Population Data.net. 2021. Available online: https://www.populationdata.net/pays/mali/ (accessed on 25 September 2021).
- Val, S.; Liousse, C.; Doumbia, E.H.T.; Galy-Lacaux, C.; Cachier, H.; Marchand, N.; Badel, A.; Gardrat, E.; Sylvestre, A.; Baeza-Squiban, A. Physico-chemical characterization of African urban aerosols (Bamako in Mali and Dakar in Senegal) and their toxic effects in human bronchial epithelial cells: Description of a worrying situation. Part. Fibre Toxicol. 2013, 10, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panasonic Photo & Lighting Co., Ltd. n.d. Available online: https://industrial.panasonic.com/ww/products/pt/dust-sensor/pm25_led (accessed on 1 September 2021).
- Li, Z.; Wei, Y.; Zhang, Y.; Xie, Y.; Li, L.; Li, K.; Ma, Y.; Sun, X.; Zhao, W.; Gu, X. Retrieval of Atmospheric Fine Particulate Density Based on Merging Particle Size Distribution Measurements: Multi-instrument Observation and Quality Control at Shouxian. J. Geophys. Res. Atmos. 2018, 123, 12474–12488. [Google Scholar] [CrossRef]
- Lin, Y.; Bahreini, R.; Zimmerman, S.; Fofie, E.A.; Asa-Awuku, A.; Park, K.; Lee, S.-B.; Bae, G.-N.; Jung, H.S. Investigation of ambient aerosol effective density with and without using a catalytic stripper. Atmos. Environ. 2018, 187, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Rissler, J.; Nordin, E.Z.; Eriksson, A.C.; Nilsson, P.T.; Frosch, M.; Sporre, M.K.; Wierzbicka, A.; Svenningsson, B.; Löndahl, J.; Messing, M.E.; et al. Effective Density and Mixing State of Aerosol Particles in a Near-Traffic Urban Environment. Environ. Sci. Technol. 2014, 48, 6300–6308. [Google Scholar] [CrossRef]
- Atmospheric Environmental Regional Observation System: AEROS. 2021. Available online: http://soramame.taiki.go.jp/ (accessed on 26 June 2021).
- Yoon, S.; Moon, Y.; Jeong, J.; Park, C.-R.; Kang, W. A Network-Based Approach for Reducing Pedestrian Exposure to PM2.5 Induced by Road Traffic in Seoul. Land 2021, 10, 1045. [Google Scholar] [CrossRef]
- Kumar, R.; Kumar, D.; Kumar, M.; Mavi, A.K.; Singh, K.; Gupta, N. Monitoring of indoor particulate matter during burning of mosquito coil, incense sticks and dhoop. Indian J. Allergy Asthma Immunol. 2014, 28, 68. [Google Scholar] [CrossRef]
- Abera, A.; Mattisson, K.; Eriksson, A.; Ahlberg, E.; Sahilu, G.; Mengistie, B.; Bayih, A.G.; Aseffaa, A.; Malmqvist, E.; Isaxon, C. Air Pollution Measurements and Land-Use Regression in Urban Sub-Saharan Africa Using Low-Cost Sensors—Possibilities and Pitfalls. Atmosphere 2020, 11, 1357. [Google Scholar] [CrossRef]
- Belarbi, N.; Belamri, M.; Dahmani, B.; Benamar, M.A. Road Traffic and PM10, PM2.5 Emission at an Urban Area in Algeria: Identification and Statistical Analysis. Pollution 2020, 6, 651–660. [Google Scholar] [CrossRef]
- Ariunsaikhan, A.; Chonokhuu, S.; Matsumi, Y. Mobile Measurement of PM2.5 Based on an Individual in Ulaanbaatar City. Int. J. Environ. Res. Public Health 2020, 17, 2701. [Google Scholar] [CrossRef] [Green Version]
- Manigrasso, M.; Vitali, M.; Protano, C.; Avino, P. Temporal evolution of ultrafine particles and of alveolar deposited surface area from main indoor combustion and non-combustion sources in a model room. Sci. Total Environ. 2017, 598, 1015–1026. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide Global Update 2005; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Liousse, C.; Assamoi, E.; Criqui, P.; Granier, C.; Rosset, R. Explosive growth in African combustion emissions from 2005 to 2030. Environ. Res. Lett. 2014, 9, 035003. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Health Risks of Particulate Matter from Long-Range Transboundary Air Pollution.1-99. Denmark; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- International Institute for Applied Systems Analysis (IIAS). Sources of Air Pollution in Developing Countries; IIAS: Laxenburg, Austria, 2016. [Google Scholar]
- Mkoma, S.L.; Kawamura, K.; Fu, P.Q. Contributions of biomass/biofuel burning to organic aerosols and particulate matter in Tanzania, East Africa, based on analyses of ionic species, organic and elemental carbon, Levoglucosan and Mannosan. Atmos. Chem. Phys. Discuss. 2013, 13, 10325–10338. [Google Scholar] [CrossRef] [Green Version]
- Chafe, Z.A.; Brauer, M.; Klimont, Z.; Van Dingenen, R.; Mehta, S.; Rao, S.; Riahi, K.; Dentener, F.; Smith, K.R. Household Cooking with Solid Fuels Contributes to Ambient PM2.5 Air Pollution and the Burden of Disease. Environ. Health Perspect. 2014, 122, 1314–1320. [Google Scholar] [CrossRef] [Green Version]
- Dhital, S.; Rupakhet, D. Correction to: Bibliometric analysis of global research on air pollution and human health: 1998–2017. Environ. Sci. Pollut. Res. Int. 2019, 26, 25386. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Xin, J.; Wang, Y.; Wang, S.; Li, G.; Pan, X.; Liu, Z.; Wang, L. The acute effects of fine particles on respiratory mortality and morbidity in Beijing, 2004–2009. Environ. Sci. Pollut. Res. 2013, 20, 6433–6444. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhang, J.; Hashim, J.H.; Jalaludin, J.; Hashim, Z.; Goldstein, B.D. Mosquito coil emissions and health implications. Environ. Health Perspect. 2003, 111, 1454–1460. [Google Scholar] [CrossRef] [PubMed]
- Norbäcka, D.; Lu, C.; Zhang, Y.; Li, B.; Zhao, Z.; Huang, C.; Zhang, X.; Qian, H.; Sun, Y.; Wang, J.; et al. Sources of indoor particulate matter (PM) and outdoor air pollution in China in relation to asthma, wheeze, rhinitis and eczema among pre-school children: Synergistic effects between antibiotics use and PM10 and second-hand smoke. Environ. Internet 2019, 125, 252–260. [Google Scholar] [CrossRef]
- Yu, W.; Guo, Y.; Shi, L.; Li, S. The association between long-term exposure to low-level PM2.5 and mortality in the state of Queensland, Australia: A modeling study with the difference-in-differences approach. PLoS Med. 2020, 17, 1003141. [Google Scholar] [CrossRef] [PubMed]
- Apte, J.S.; Brauer, M.; Cohen, A.J.; Ezzati, M.; Pope, I.C.A. Ambient PM2.5 Reduces Global and Regional Life Expectancy. Environ. Sci. Technol. Lett. 2018, 5, 546–551. [Google Scholar] [CrossRef] [Green Version]
- Bentayeb, M.; Simoni, M.; Norbäck, D.; Baldacci, S.; Maio, S.; Viegi, G.; Annesi-Maesano, I. Indoor air pollution and respiratory health in the elderly. J. Environ. Sci. Health 2013, 48, 1783–1789. [Google Scholar] [CrossRef] [PubMed]
- Manigrasso, M.; Natale, C.; Vitali, M.; Protano, C.; Avino, P. Pedestrians in Traffic Environments: Ultrafine Particle Respiratory Doses. Int. J. Environ. Res. Public Health 2017, 14, 288. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Zhou, S.; Xu, J.; Su, L. From PM2.5 exposure to PM2.5 risks of inhaled dose in daily activities: Empirical evidence during workdays from Guangzhou, China. Atmos. Environ. 2021, 249, 118224. [Google Scholar] [CrossRef]
- Giovanis, E. The relationship between teleworking, traffic and air pollution. Atmos. Pollut. Res. 2017, 9, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Bai, X. Integrating Global Environmental Concerns into Urban Management: The Scale and Readiness Arguments. J. Ind. Ecol. 2007, 11, 15–29. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OW | ST | DRI | COOK | Average | |
|---|---|---|---|---|---|
| Home | 9 | 14 | 12 | 18 | 13 ± 4 |
| Driving/commute | 33 (1.9) | 30 (1.6) | 42 (11.6) | 35 ± 6 | |
| Workplace | 14 (5.7) | ||||
| Cooking | 43 (2) | 41 (3.1) | 42 ± 1 | ||
| Beauty salon | 19 (1.7) | ||||
| School (classes) | 16 (4.3) | ||||
| School (Break) | 31 (0.8) | ||||
| Home (IST/ICS) | 244 (3.8) | 30 (2.6) * | 78(4.1) | 300 (4.5) | 207 ± 115 ** |
| Daily average | 12 | 18 | 27 | 24 | 20 ± 7 |
| Daily average (IST/ICS) | 49 | 20 * | 38 | 76 | 54 ± 20 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sidibe, A.; Sakamoto, Y.; Murano, K.; Koita, O.A.; Traore, I.; Dansoko, Y.; Kajii, Y. Personal Exposure to Fine Particles (PM2.5) in Northwest Africa: Case of the Urban City of Bamako in Mali. Int. J. Environ. Res. Public Health 2022, 19, 611. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010611
Sidibe A, Sakamoto Y, Murano K, Koita OA, Traore I, Dansoko Y, Kajii Y. Personal Exposure to Fine Particles (PM2.5) in Northwest Africa: Case of the Urban City of Bamako in Mali. International Journal of Environmental Research and Public Health. 2022; 19(1):611. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010611
Chicago/Turabian StyleSidibe, Alimata, Yosuke Sakamoto, Kentaro Murano, Ousmane A. Koita, Ibrahim Traore, Yacouba Dansoko, and Yoshizumi Kajii. 2022. "Personal Exposure to Fine Particles (PM2.5) in Northwest Africa: Case of the Urban City of Bamako in Mali" International Journal of Environmental Research and Public Health 19, no. 1: 611. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010611