
Female Sexual Dysfunction and Pelvic Floor Muscle Function Associated with Systemic Sclerosis: A Cross-Sectional Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Healthy Controls
2.2. Assessment Methods
- Demographic characteristics. Age at recruitment, education levels (primary, secondary, higher education), current sexual partnership, body mass index (BMI), alcohol intake, and smoking conditions.
- Clinical features. Disease duration (from the first SSc symptom except for Raynaud’s phenomenon), disease activity determined by the European Scleroderma Study Group (ESSG) SSc activity score [15], involvement of the skin evaluated by the modified Rodnan skin score (mRSS) [16], and current medical therapy. Capillaroscopy and pulmonary function tests were routinely performed using standard methods [17,18]. All assessments were performed according to well-established guidelines [19], and all clinical features were documented.
- Patient-reported outcomes (PROs). Fatigue was assessed by the Multidimensional Assessment of Fatigue Scale (MAF) [20] and the Fatigue Impact Scale (FIS) [21]. Depression was evaluated by the Beck’s Depression Inventory-II (BDI II) [22]. We used the Human Activity Profile (HAP) [23] to assess physical activity, and the Scleroderma Health Assessment Questionnaire (SHAQ) [24] and the Health Assessment Questionnaire (HAQ) [25] for functional status. The overall quality of life was analyzed using the 36-Item Short Form Survey (SF-36) [26]. Detailed descriptions have been stated elsewhere [27]. The Czech version of all questionnaires has previously been validated [28,29,30,31,32]. The importance of sexual life was subjectively assessed and recorded by a visual analog scale (VAS) ranging from 0 (not important at all) to 10 (extremely important).
- Laboratory evaluation. Serum concentrations of C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), antinuclear antibodies (ANA), and autoantibodies of the ENA complex were analyzed as described elsewhere [33].
- Gynecological features. Previous pelvic surgery, menstrual status, hormone replacement therapy, contraception use, reasons for lack of sexual activity, and disease-related symptoms affecting sexual activity were recorded.
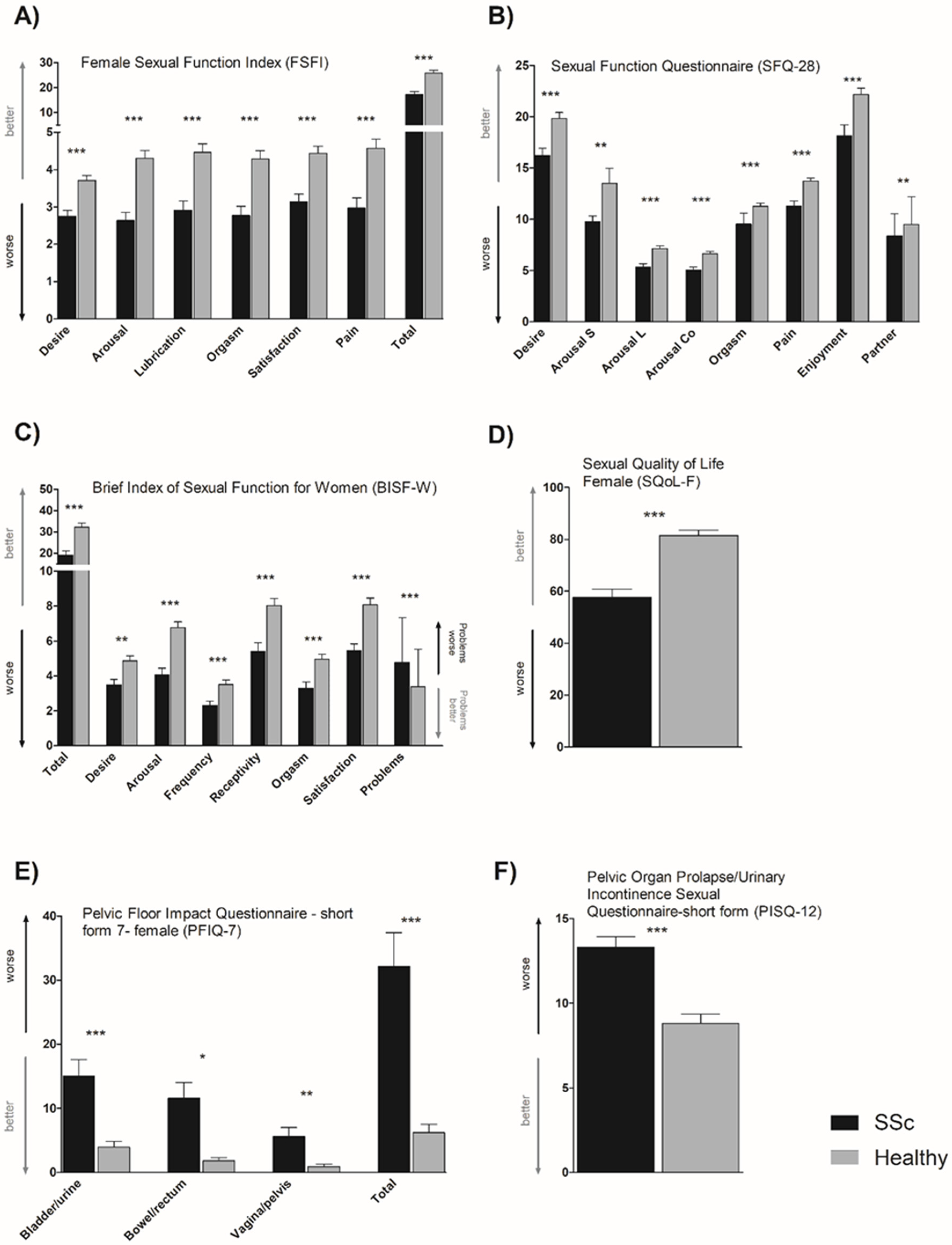
- Sexual function evaluation (PROs). Sexual function in women was assessed by the Female Sexual Function Index (FSFI) [34], the Brief Index of Sexual Functioning for Women (BISF-W) [35], and the Sexual Function Questionnaire (SFQ-28) [36]. The impact of female sexual dysfunction on the quality of life was assessed by the Sexual Quality of Life Questionnaire-Female (SQoL-F) [37]. The Czech version of all questionnaires has been validated [38]. Further details are provided elsewhere [27].
- Pelvic floor function evaluation (PROs). The sexual performance of women with pelvic floor problems was assessed using the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire Short Form (PISQ-12) [39]. We also used Pelvic Floor Impact Questionnaire-Short Form 7 (PFIQ-7) [40] to determine the impact of pelvic floor dysfunction on the patients’ quality of life. Both questionnaires were translated into Czech and have been validated [38]. Further details are provided elsewhere [27].
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Denton, C.P.; Khanna, D. Systemic sclerosis. Lancet 2017, 390, 1685–1699. [Google Scholar] [CrossRef]
- Bruni, C.; Raja, J.; Denton, C.; Matucci-Cerinic, M. The clinical relevance of sexual dysfunction in systemic sclerosis. Autoimmun. Rev. 2015, 14, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Levis, B.; Hudson, M.; Knafo, R.; Baron, M.; Nielson, W.R.; Hill, M.; Thombs, B.D.; Canadian Scleroderma Research Group (CSRG). Rates and correlates of sexual activity and impairment among women with systemic sclerosis. Arthritis Care Res. 2012, 64, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Saad, S.C.; Pietrzykowski, J.; Lewis, S.S.; Stepien, A.M.; Latham, V.A.; Messick, S.; Ensz, S.L.; Wetherell, C.; Behrendt, A.E. Vaginal lubrication in women with scleroderma and Sjogren’s syndrome. Sex. Disabil. 1999, 17, 103–113. [Google Scholar] [CrossRef]
- Tzioufas, A.G.; Liantinioti, G.; Vlachoyiannopoulos, P.G. Sjogren’s Syndrome (Ss) in Progressive Systemic Sclerosis (SSc). In Practical Management of Systemic Sclerosis in Clinical Practice; Springer: Berlin/Heidelberg, Germany, 2021; pp. 281–297. [Google Scholar]
- Impens, A.; Rothman, J.; Schiopu, E.; Cole, J.; Dang, J.; Gendrano, N.; Rosen, R.C.; Seibold, J.R. Sexual activity and functioning in female scleroderma patients. Clin. Exp. Rheumatol. 2009, 27, S38. [Google Scholar]
- Bhadauria, S.; Moser, D.K.; Clements, P.J.; Singh, R.R.; Lachenbruch, P.A.; Pitkin, R.M.; Weiner, S.R. Genital tract abnormalities and female sexual function impairment in systemic sclerosis. Am. J. Obstet. Gynecol. 1995, 172, 580–587. [Google Scholar] [CrossRef]
- Knafo, R.; Thombs, B.D.; Jewett, L.; Hudson, M.; Wigley, F.; Haythornthwaite, J.A. (Not) talking about sex: A systematic comparison of sexual impairment in women with systemic sclerosis and other chronic disease samples. Rheumatology 2009, 48, 1300–1303. [Google Scholar] [CrossRef] [Green Version]
- Schouffoer, A.; Van Der Marel, J.; Ter Kuile, M.; Weijenborg, P.; Voskuyl, A.; Vliet Vlieland, C.; van Laar, J.M.; Vliet Vlieland, T.P.M. Impaired sexual function in women with systemic sclerosis: A cross-sectional study. Arthritis Rheum. 2009, 61, 1601–1608. [Google Scholar] [CrossRef] [PubMed]
- Knafo, R.; Haythornthwaite, J.A.; Heinberg, L.; Wigley, F.M.; Thombs, B.D. The association of body image dissatisfaction and pain with reduced sexual function in women with systemic sclerosis. Rheumatology 2011, 50, 1125–1130. [Google Scholar] [CrossRef] [Green Version]
- Gigante, A.; Navarini, L.; Margiotta, D.; Barbano, B.; Afeltra, A.; Rosato, E. Female sexual dysfunction in systemic sclerosis: The role of endothelial growth factor and endostatin. J. Scleroderma Relat. Disord. 2019, 4, 71–76. [Google Scholar] [CrossRef]
- Nazarinia, M.; Esmaeilzadeh, E.; Khodamoradi, Z. Sexual Dysfunction in Female Scleroderma Patients and Its Correlation with Vascular Involvement. Rheumatol. Res. J. 2019, 4, 93–99. [Google Scholar] [CrossRef]
- Rosato, E.; Gigante, A.; Barbano, B.; La Marra, F.; Molinaro, I.; Quarta, S.; Digiulio, M.A.; Carmelina, R.; Cianci, R.; Pisarri, S.; et al. Clitoral blood flow in systemic sclerosis women: Correlation with disease clinical variables and female sexual dysfunction. Rheumatology 2013, 52, 2238–2242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valentini, G.; Bencivelli, W.; Bombardieri, S.; D’Angelo, S.; Della Rossa, A.; Silman, A.J.; Black, C.M.; Czirjak, L.; Nielsen, H.; Vlachoyiannopoulos, P.G. European Scleroderma Study Group to define disease activity criteria for systemic sclerosis. III. Assessment of the construct validity of the preliminary activity criteria. Ann. Rheum. Dis. 2003, 62, 901–903. [Google Scholar] [CrossRef] [Green Version]
- Clements, P.; Lachenbruch, P.; Seibold, J.; Zee, B.; Steen, V.; Brennan, P.; Silman, A.J.; Allegar, N.; Varga, J.; Massa, M. Skin thickness score in systemic sclerosis: An assessment of interobserver variability in 3 independent studies. J. Rheumatol. 1993, 20, 1892–1896. [Google Scholar] [PubMed]
- Cutolo, M.; Pizzorni, C.; Sulli, A. Capillaroscopy. Best Pract. Res. Clin. Rheumatol. 2005, 19, 437–452. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Bombardieri, S.; Medsger, T., Jr.; Silman, A.; Valentini, G. The assessment of the patient with systemic sclerosis. Introduction. Clin. Exp. Rheumatol. 2003, 21, S2–S4. [Google Scholar]
- Piper, B.F.; Dibble, S.L.; Dodd, M.J.; Weiss, M.C.; Slaughter, R.E.; Paul, S.M. (Eds.) The revised Piper Fatigue Scale: Psychometric evaluation in women with breast cancer. Oncol. Nurs. Forum. 1998, 25, 677–684. [Google Scholar]
- Fisk, J.D.; Ritvo, P.G.; Ross, L.; Haase, D.A.; Marrie, T.J.; Schlech, W.F. Measuring the functional impact of fatigue: Initial validation of the fatigue impact scale. Clin. Infect. Dis. 1994, 18, S79–S83. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the beck depression inventory-II. Psychol. Corp. 1996, 1, 82. [Google Scholar]
- Fix, A.J.; Daughton, D. Human Activity Profile: Professional Manual; Psychological Assessment Resources, Inc.: Odessa, FL, USA, 1988; 25p. [Google Scholar]
- Steen, V.D.; Medsger, T.A., Jr. The value of the Health Assessment Questionnaire and special patient-generated scales to demonstrate change in systemic sclerosis patients over time. Arthritis Rheum. 1997, 40, 1984–1991. [Google Scholar] [CrossRef]
- Fries, J.F.; Spitz, P.; Kraines, R.G.; Holman, H.R. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980, 23, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Gandek, B. Overview of the SF-36 health survey and the international quality of life assessment (IQOLA) project. J. Clin. Epidemiol. 1998, 51, 903–912. [Google Scholar] [CrossRef]
- Heřmánková, B.; Špiritović, M.; Oreská, S.; Štorkánová, H.; Komarc, M.; Klein, M.; Mann, H.; Pavelka, K.; Šenolt, L.; Vencovský, J.; et al. Sexual Function in Patients with Idiopathic Inflammatory Myopathies: A Cross-sectional Study. Rheumatology 2021, 60, 5060–5072. [Google Scholar] [CrossRef] [PubMed]
- Heřmánková, B.; Oreská, S.; Šmucrová, H.; Mikulášová, M.; Špiritović, M.; Štorkánová, H.; Bečvář, R.; Vencovský, J.; Mann, H.; Tomčík, M. Validation of Czech versions of questionnaires assessing functional impairment in patients with systemic sclerosis: Scleroderma Health Assessment Questionnaire (SHAQ), Cochin Hand Functional Scale (CHFS), Mouth Handicap in Systemic Sclerosis (MHISS), UCLA Scleroderma Clinical Trial Consortium Gastrointestinal Tract 2.0 (UCLA SCTC GIT 2.0 ). Ceska Revmatol. 2020, 28, 216–230. [Google Scholar]
- Heřmánková, B.; Štorkánová, H.; Mikulášová, M.; Oreská, S.; Špiritović, M.; Štorkánová, H.; Tomčík, M. Validation of Czech versions of questionnaires assessing fatigue and physical activity in patients with rheumatic diseases: Fatigue Impact Scale (FIS), Multidimensional Assessment of Fatigue Scale (MAF), Human Activity Profile (HAP). Ceska Revmatol. 2020, 28, 132–151. [Google Scholar]
- Ptáček, R.; Raboch, J.; Vňuková, M.; Hlinka, J.; Anders, M. Beckova škála deprese BDI-II-standardizace a využití v praxi. Ceská a Slovenská Psychiatrie 2016, 112, 270–274. [Google Scholar]
- SOBOTÍKZ Zkušenosti s použitím předběžné české verze amerického dotazníku o zdraví (SF-36). Zdravotnictví v České Republice 1998, 1, 50–54.
- Šléglová, O.; Dušek, L.; Olejárová, M.; Tegzová, D.; Vencovský, J.; Pavelka, K. Posuzování funkční schopnosti u pacientů s revmatoidní artritidou; validace české verze Stanfordského dotazníku Health Assessment Questionnaire (HAQ). Čes Revmatol. 2010, 18, 73–83. [Google Scholar]
- Štorkánová, H.; Oreská, S.; Špiritović, M.; Heřmánková, B.; Bubová, K.; Komarc, M.; Pavelka, K.; Vencovský, J.; Distler, J.H.W.; Šenolt, L.; et al. Plasma Hsp90 levels in patients with systemic sclerosis and relation to lung and skin involvement: A cross-sectional and longitudinal study. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef]
- Rosen, C.B.J.; Heiman, S.; Leiblum, C.; Meston, R.; Shabsigh, D.; Ferguson, R.; D’Agostino, R. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital. Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.F.; Rosen, R.C.; Leiblum, S.R. Self-report assessment of female sexual function: Psychometric evaluation of the Brief Index of Sexual Functioning for Women. Arch. Sex Behav. 1994, 23, 627–643. [Google Scholar] [CrossRef] [PubMed]
- Quirk, F.H.; Heiman, J.R.; Rosen, R.C.; Laan, E.; Smith, M.D.; Boolell, M. Development of a sexual function questionnaire for clinical trials of female sexual dysfunction. J. Womens Health Gend. Based Med. 2002, 11, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Symonds, T.; Boolell, M.; Quirk, F. Development of a questionnaire on sexual quality of life in women. J. Sex Marital. Ther. 2005, 31, 385–397. [Google Scholar] [CrossRef]
- Heřmánková, B.; Štorkánová, H.; Mikulášová, M.; Oreská, S.; Špiritović, M.; Štorkánová, H.; Tomčík, M. Validation of Czech versions of questionnaires assessing female sexual function and pelvic floor function. Ceska Revmatol. 2021, 29, 30–40. [Google Scholar]
- Rogers, R.G.; Kammerer-Doak, D.; Villarreal, A.; Coates, K.; Qualls, C. A new instrument to measure sexual function in women with urinary incontinence or pelvic organ prolapse. Am. J. Obstet. Gynecol. 2001, 184, 552–558. [Google Scholar] [CrossRef] [Green Version]
- Barber, M.; Walters, M.; Bump, R. Short forms of two condition-specific quality-of-life questionnaires for women with pelvic floor disorders (PFDI-20 and PFIQ-7). Am. J. Obstet. Gynecol. 2005, 193, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Sampaio-Barros, P.D.; Samara, A.M.; Marques Neto, J.F. Gynaecologic history in systemic sclerosis. Clin. Rheumatol. 2000, 19, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Ostojić, P.; Damjanov, N. Different clinical features in patients with limited and diffuse cutaneous systemic sclerosis. Clin. Rheumatol. 2006, 25, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Giraldi, A.; Rellini, A.; Pfaus, J.G.; Bitzer, J.; Laan, E.; Jannini, E.A.; Fugl-Meyer, A.R. Questionnaires for assessment of female sexual dysfunction: A review and proposal for a standardized screener. J. Sex Med. 2011, 8, 2681–2706. [Google Scholar] [CrossRef] [PubMed]
- Shah, D. Healthy worker effect phenomenon. Indian J. Occup. Environ. Med. 2009, 13, 77. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | SSc (n = 90) | Healthy Controls (n = 90) | p |
|---|---|---|---|
| Sociodemographic variables | |||
| Age, years | 49.5 (38.8–58.8) | 49.5 (38.8–58.8) | 0.9999 |
| Having a partner, n (%) | 70 (78) | 82 (91) | 0.0223 |
| Education level (primary/secondary/tertiary), n (%) | 1 (1)/60 (67)/29 (32) | 0 (0)/58 (64)/32 (36) | 0.5349 |
| Sexual health features | |||
| Sexual activity, n (%) | 62 (69) | 80 (89) | 0.0019 |
| Menopause, n (%) | 50 (56) | 49 (54) | 0.9997 |
| Pelvic surgery, n (%) | 16 (18) | 7 (8) | 0.0675 |
| Normal menstrual cycle, n (%) | 22 (55) | - | |
| Contraceptives, n (%) | 5 (13) | - | |
| HRT, n (%) | 6 (12) | - | |
| VAS: sexual life importance | 6.5 (3.8–8.0) | 7.0 (5.0–8.3) | 0.0649 |
| Clinical features | |||
| Disease duration, years | 4.0 (2.0–8.0) | - | |
| SSc subtype: lcSSc/dcSSc, n (%) | 61 (68)/29 (32) | - | |
| ESSG activity index | 2.0 (1.0–3.1) | - | |
| mRSS | 5.0 (0.0–13.0) | - | |
| SSc-associated symptoms: n (%) | - | ||
| ILD/PAH/OD/P/RI | 51 (57)/13 (15)/56 (63)/4 (5)/33 (39) | - | |
| RP/DU/CA/A/MW | 83 (92)/41 (46)/8 (9)/46 (52)/13 (15) | - | |
| Patient-reported outcomes | |||
| (score range worst–best) | |||
| FIS: fatigue (160–0) | 57.5 (33.5–86.3) | 26.0 (7.0–46.8) | 0.0002 |
| MAF: fatigue (50–1) | 27.8 (19.4–35.7) | 14.4 (9.1–21.1) | 0.0002 |
| BDI-II: depression (63–0) | 14.0 (7.0–20.0) | 4.5 (1.0–8.0) | 0.0002 |
| HAP AAS: physical activity (0–94) | 54.0 (35.5–72.5) | 82.0 (76.0–91.5) | 0.0002 |
| HAQ: functional status (3–0) | 0.75 (0.2–1.4) | 0.0 (0.0–0.0) | 0.0002 |
| SHAQ: SSc-related functional status (3–0) | 1.0 (0.5–1.4) | - | |
| Global SHAQ: SSc impairment (3–0) | 0.9 (0.4–1.4) | - | |
| SF-36 PCS: quality of life (16.6–57.9) | 31.1 (24.9–43.0) | 53.9 (46.0–56.8) | 0.0002 |
| SF-36 MCS: quality of life (5.5–63.6) | 42.6 (31.0–50.5) | 52.4 (47.2–57.0) | 0.0002 |
| Laboratory features | |||
| Autoantibodies, seronegative, n (%): | 3 (3) | - | |
| ANA/Scl70/ACA/RNA3P n (%) | 86 (96)/45(50)/20(22)/2 (2) | - | |
| CRP, mg/L | 3.2 (1.6–6.5) | - | |
| ESR, mm/h | 12.0 (8.0–25.0) | - | |
| Current treatment | |||
| Prednisone equivalent dose, mg/day | 0.0 (0.0–2.5) | - | |
| GC/MTX/CPA/AZA/MMF, n (%) | 26 (29)/20 (22)/19 (21)/9 (10)/8 (9) | - | |
| RTX/TCZ/CCB/antiHT/bosentan, n (%) | 3 (3)/1 (1)/4 (4)/15 (17)/6 (7) | - | |
| sildenafil/epoprostenol/alprostadil, n (%) | 4 (4)/1 (1)/12 (13) | - | |
| antidepressants and mood stabilizers, n (%) | 18 (20) | - |
| FSFI Total | FSFI Desire | FSFI Arousal | FSFI Lubrication | FSFI Orgasm | FSFI Satisfaction | FSFI Pain | BISF-W Total | SQoL-F | PISQ-12 | PFIQ-7 Total | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ESSG | r | −0.237 | −0.081 | −0.309 | −0.254 | −0.178 | −0.268 | −0.243 | −0.261 | −0.369 | 0.308 | 0.028 |
| p | 0.025 | 0.452 | 0.003 | 0.016 | 0.096 | 0.011 | 0.022 | 0.015 | 0.001 | 0.005 | 0.790 | |
| n | 89 | 89 | 89 | 89 | 89 | 89 | 89 | 87 | 83 | 83 | 90 | |
| ESR | r | −0.147 | −0.140 | −0.239 | −0.222 | −0.085 | −0.087 | −0.003 | −0.273 | −0.061 | 0.097 | −0.171 |
| p | 0.177 | 0.198 | 0.027 | 0.040 | 0.439 | 0.426 | 0.976 | 0.012 | 0.592 | 0.392 | 0.113 | |
| n | 86 | 86 | 86 | 86 | 86 | 86 | 86 | 84 | 80 | 80 | 87 | |
| Dyspnea | r | −0.227 * | −0.249 * | −0.246 * | −0.222 * | −0.250 * | −0.121 * | −0.134 * | −0.288 * | −0.106 * | 0.168 * | 0.168 * |
| p | 0.034 | 0.019 | 0.021 | 0.037 | 0.019 | 0.263 | 0.312 | 0.007 | 0.344 | 0.131 | 0.115 | |
| n | 88 | 88 | 88 | 88 | 88 | 88 | 88 | 86 | 82 | 82 | 89 | |
| ILD | r | −0.252 * | −0.329 * | −0.285 * | −0.264 * | −0.249 * | −0.153 * | −0.103 * | −0.347 * | −0.228 * | 0.190 * | 0.234 * |
| p | 0.019 | 0.002 | 0.008 | 0.014 | 0.020 | 0.157 | 0.342 | 0.001 | 0.041 | 0.089 | 0.028 | |
| n | 87 | 87 | 87 | 87 | 87 | 87 | 87 | 85 | 81 | 81 | 88 | |
| DLCO | r | 0.349 | 0.217 | 0.444 | 0.399 | 0.343 | 0.295 | 0.251 | 0.362 | 0.237 | −0.208 | −0.280 |
| p | 0.001 | 0.052 | 0.001 | 0.001 | 0.002 | 0.008 | 0.024 | 0.001 | 0.039 | 0.074 | 0.011 | |
| n | 81 | 81 | 81 | 81 | 81 | 81 | 81 | 80 | 76 | 75 | 82 | |
| Dysphagia/ pyrosis | r | −0.215 | 0.158 | −0.250 | −0.211 | −0.202 | −0.105 | −0.200 | −0.157 | −0.104 | 0.135 | 0.177 |
| p | 0.044 | 0.140 | 0.019 | 0.049 | 0.059 | 0.330 | 0.062 | 0.149 | 0.351 | 0.228 | 0.097 | |
| n | 88 | 88 | 88 | 88 | 88 | 88 | 88 | 86 | 82 | 82 | 89 | |
| Obstipation/ diarrhea | r | −0.184 | −0.273 | −0.180 | −0.210 | −0.200 | −0.099 | −0.067 | −0.220 | −0.093 | 0.325 | 0.163 |
| p | 0.087 | 0.011 | 0.095 | 0.051 | 0.063 | 0.361 | 0.537 | 0.043 | 0.410 | 0.003 | 0.130 | |
| n | 87 | 87 | 87 | 87 | 87 | 87 | 87 | 85 | 81 | 81 | 88 | |
| Antidepressants | r | −0.343 * | −0.269 * | −0.339 * | −0.267 * | −0.378 * | −0.345 * | −0.220 * | −0.326 * | −0.383 * | 0.336 * | 0.076 * |
| p | 0.002 | 0.017 | 0.002 | 0.017 | 0.001 | 0.002 | 0.050 | 0.004 | 0.001 | 0.003 | 0.503 | |
| n | 79 | 79 | 79 | 79 | 79 | 79 | 79 | 77 | 75 | 75 | 80 | |
| SSc limitations | r | −0.464 * | −0.472 * | −0.337 * | −0.380 * | −0.270 * | −0.396 * | −0.435 * | −0.517 * | −0.487 * | 0.437 * | −0.072 * |
| p | 0.001 | 0.001 | 0.011 | 0.004 | 0.045 | 0.003 | 0.001 | 0.001 | 0.001 | 0.001 | 0.947 | |
| n | 53 | 53 | 53 | 53 | 53 | 53 | 53 | 53 | 53 | 55 | 56 | |
| Education | r | 0.241 * | 0.228 * | 0.284 * | 0.223 * | 0.164 * | 0.260 * | 0.159 * | 0.270 * | 0.295 * | −0.202 * | −0.146 * |
| p | 0.023 | 0.033 | 0.007 | 0.037 | 0.127 | 0.014 | 0.139 | 0.012 | 0.007 | 0.069 | 0.173 | |
| n | 88 | 88 | 88 | 88 | 88 | 88 | 88 | 86 | 82 | 82 | 82 | |
| Alcohol | r | 0.381 | 0.316 | 0.399 | 0.420 | 0.307 | 0.313 | 0.221 | 0.454 | 0.259 | −0.117 | −0.185 |
| p | 0.001 | 0.005 | 0.001 | 0.001 | 0.006 | 0.005 | 0.050 | 0.001 | 0.025 | 0.317 | 0.100 | |
| n | 79 | 79 | 79 | 79 | 79 | 79 | 79 | 77 | 75 | 75 | 80 | |
| SHAQ global | r | −0.436 | −0.392 | −0.406 | −0.353 | −0.366 | −0.366 | −0.282 | −0.303 | −0.471 | 0.339 | 0.236 |
| p | 0.001 | 0.001 | 0.001 | 0.002 | 0.001 | 0.001 | 0.013 | 0.008 | 0.001 | 0.004 | 0.038 | |
| n | 77 | 77 | 77 | 77 | 77 | 77 | 77 | 75 | 72 | 71 | 78 | |
| HAQ | r | −0.393 | −0.354 | −0.364 | −0.307 | −0.328 | −0.344 | −0.298 | −0.280 | −0.483 | 0.326 | 0.144 |
| p | 0.001 | 0.001 | 0.001 | 0.004 | 0.002 | 0.001 | 0.005 | 0.009 | 0.001 | 0.003 | 0.179 | |
| n | 88 | 88 | 88 | 88 | 88 | 88 | 88 | 86 | 82 | 82 | 89 | |
| BDI-II | r | −0.506 | −0.527 | −0.455 | −0.442 | −0.416 | −0.484 | −0.328 | −0.475 | −0.532 | 0.385 | 0.451 |
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.002 | 0.001 | 0.001 | 0.001 | 0.001 | |
| n | 88 | 88 | 88 | 88 | 88 | 88 | 88 | 86 | 82 | 82 | 89 | |
| FIS | r | −0.496 | −0.484 | −0.465 | −0.398 | −0.416 | −0.461 | −0.278 | −0.477 | −0.433 | 0.296 | 0.297 |
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.008 | 0.001 | 0.001 | 0.007 | 0.005 | |
| n | 89 | 89 | 89 | 89 | 89 | 89 | 89 | 87 | 83 | 83 | 80 | |
| HAP-AAS | r | 0.535 | 0.478 | 0.499 | 0.427 | 0.433 | 0.440 | 0.448 | 0.533 | 0.389 | −0.325 | −0.217 |
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.003 | 0.041 | |
| n | 88 | 88 | 88 | 88 | 88 | 88 | 88 | 86 | 82 | 82 | 89 | |
| SF-36 PCS | r | 0.382 | 0.412 | 0.355 | 0.308 | 0.289 | 0.301 | 0.244 | 0.332 | 0.388 | −0.336 | −0.178 |
| p | 0.001 | 0.001 | 0.001 | 0.004 | 0.007 | 0.005 | 0.023 | 0.002 | 0.001 | 0.002 | 0.098 | |
| n | 87 | 87 | 87 | 87 | 87 | 87 | 87 | 85 | 81 | 81 | 88 | |
| SF-36 MCS | r | 0.394 | 0.370 | 0.370 | 0.332 | 0.344 | 0.429 | 0.247 | 0.321 | 0.352 | −0.266 | −0.372 |
| p | 0.001 | 0.001 | 0.001 | 0.002 | 0.001 | 0.001 | 0.021 | 0.003 | 0.001 | 0.017 | 0.001 | |
| n | 87 | 87 | 87 | 87 | 87 | 87 | 87 | 85 | 81 | 81 | 88 | |
| β (95% CI) | Stand. β | p | Adjusted R2 | p * | |
|---|---|---|---|---|---|
| FSFI | |||||
| Overall model | 0.219 | 0.0001 | |||
| ESSG activity index | −1.281 (−2.966; 0.403) | −0.172 | 0.134 | ||
| DLCO | 0.076 (−0.044; 0.196) | 0.144 | 0.210 | ||
| SHAQ-Global | −8.062 (−12.557; 3.568) | −0.390 | 0.001 | ||
| BISF-W | |||||
| Overall model | 0.292 | 0.0001 | |||
| ESSG activity index | −2.129 (−4.632; 0.375) | −0.170 | 0.094 | ||
| ESR | −0.108 (−0.282; −0.066) | −0.123 | 0.221 | ||
| ILD | −7.195 (−14.319; −0.070) | −0.196 | 0.048 | ||
| FIS total | 0.218 (−0.318; −0.118) | −0.412 | 0.0001 | ||
| SQoL-F | |||||
| Overall model | 0.341 | 0.0001 | |||
| ESSG activity index | −5223 (−9.211; −1.234) | −0.277 | 0.011 | ||
| DLCO | −0.045 (−0.328; 0.237) | −0.034 | 0.749 | ||
| SHAQ-Global | −25.974 (−36.470; 15.477) | −0.514 | 0.0001 | ||
| PISQ-12 | |||||
| Overall model | 0.207 | 0.002 | |||
| ESSG activity index | 0.868 (−0.006; 1.741) | 0.223 | 0.052 | ||
| Obstipation/diarrhea | 3.756 (0.716; 6.795) | 0.277 | 0.016 | ||
| SHAQ-Global | 2.232 (0.035; 4.429) | 0.230 | 0.047 | ||
| PFIQ-7 | |||||
| Overall model | 0.162 | 0.008 | |||
| SHAQ | 29.973 (8.543; 51.403) | 0.337 | 0.007 | ||
| DLCO | −0.380 (−0.949; 0.188) | −0.159 | 0.186 | ||
| HAP AAS | −0.063 (−0.651; 0.526) | −0.027 | 0.832 | ||
| Parameters (Score Range Worst–Best) | SA SSc (n = 62) | SA HC (n = 80) | p-Value |
|---|---|---|---|
| FSFI total (range 2–36) FSFI desire (range 1.2–6) FSFI arousal (range 0–6) FSFI lubrication (range 0–6) FSFI orgasm (range 0–6) FSFI satisfaction (range 0.8–6) FSFI pain (range 0–6) BISF-W total (range −16–75) BISF-W thoughts/desire (range 0–12) BISF-W arousal (range 0–12) BISF-W frequency of sexual activity (range 0–12) BISF-W receptivity/initiation (range 0–15) BISF-W pleasure/orgasm (range 0–12) BISF-W relationship satisfaction (range 0–12) BISF-W problems affecting sexual function (range 16–0) SFQ28 desire (range 5–31) SFQ28 arousal sensation (range 4–20) SFQ28 arousal lubrication (range 2–10) SFQ28 arousal cognitive (range 2–10) SFQ28 orgasm (range 1–15) SFQ28 pain (range 2–15) SFQ28 enjoyment (range 6–30) SFQ28 partner (range 2–10) SQoL-F (range 0–100) PISQ-12 (range 48–0) PFIQ-7 total (range 300–0), mean ± SD PFIQ-7 bladder/urine (range 100–0) PFIQ-7 bowel/rectum (range 100–0) PFIQ-7 vagina/pelvis (range 100–0) | 24.0 (16.7–30.2) 3.3 (1.7–4.2) 3.6 (2.3–5.1) 4.4 (2.7–5.7) 4.2 (2.4–5.2) 4.4 (2.0–5.6) 4.8 (2.8–6.0) 30.4 (13.0–38.4) 4.3 (2.3–6.4) 6.3 (4.0–7.8) 3.3 (1.3–5.0) 8.0 (5.0–10.0) 4.8 (2.0–7.0) 7.0 (5.0–10.0) 5.1 (3.5–7.0) 17.0 (12.0–20.0) 10.0 (8.0–13.0) 6.0 (4.0–7.0) 5.0 (4.0–6.0) 10.0 (6.0–12.0) 12.0 (10.0–15.0) 19.0 (14.0–24.0) 9.0 (7.5–10.0) 65.6 (40.3–92.5) 12.0 (9.0–16.5) 26.3 ± 46.5 12.5 ± 23.5 8.3 ± 19.1 5.5 ± 13.5 | 30.8 (26.8–33.1) 3.6 (3.6–4.8) 5.1 (4.5–5.7) 5.9 (4.8–6.0) 5.2 (4.1–6.0) 5.2 (4.0–6.0) 6.0 (5.2–6.0) 39.4 (30.3–46.5) 5.7 (3.9–7.0) 7.5 (6.3–9.8) 4.0 (2.4–5.4) 10.0 (7.0–11.0) 5.9 (4.4–7.5) 10.0 (7.0–11.0) 2.9 (1.8–5.4) 21.0 (17.0–23.0) 12.0 (9.0–15.0) 8.0 (6.0–9.0) 7.0 (5.0–8.0) 12.0 (10.0–13.0) 15.0 (13.0–15.0) 23.0 (20.0–25.0) 10.0 (9.0–10.0) 91.1 (73.9–96.9) 7.0 (5.0–11.0) 6.1 ± 11.6 3.9 ± 8.3 1.8 ± 4.8 0.9 ± 3.6 | 0.0002 0.0005 0.0002 0.0002 0.0010 0.0003 0.0001 0.0005 0.0187 0.0003 0.0437 0.0191 0.0349 0.0007 0.0002 0.0006 0.0034 0.0002 0.0001 0.0001 0.0002 0.0006 0.0014 0.0002 0.0002 0.0016 0.0326 0.2324 0.0035 |
| Parameters (Score Range Worst–Best) | SSc in Reproductive Age (n = 40) | HC in Reproductive Age (n = 41) | p-Value |
|---|---|---|---|
| FSFI total (range 2–36) FSFI desire (range 1.2–6) FSFI arousal (range 0–6) FSFI lubrication (range 0–6) FSFI orgasm (range 0–6) FSFI satisfaction (range 0.8–6) FSFI pain (range 0–6) BISF-W total (range −16–75) BISF-W thoughts/desire (range 0–12) BISF-W arousal (range 0–12) BISF-W frequency of sexual activity (range 0–12) BISF-W receptivity/initiation (range 0–15) BISF-W pleasure/orgasm (range 0–12) BISF-W relationship satisfaction (range 0–12) BISF-W problems affecting sexual function (range 16–0) SFQ28 desire (range 5–31) SFQ28 arousal sensation (range 4–20) SFQ28 arousal lubrication (range 2–10) SFQ28 arousal cognitive (range 2–10) SFQ28 orgasm (range 1–15) SFQ28 pain (range 2–15) SFQ28 enjoyment (range 6–30) SFQ28 partner (range 2–10) SQoL-F (range 0–100) PISQ-12 (range 48–0) PFIQ-7 total (range 300–0), mean ± SD PFIQ-7 bladder/urine (range 100–0) PFIQ-7 bowel/rectum (range 100–0) PFIQ-7 vagina/pelvis (range 100–0) | 24.5 (13.3–31.5) 3.6 (2.0–4.2) 3.8 (1.5–5.0) 5.1 (2.4–6.0) 3.6 (1.4–5.2) 4.0 (1.7–5.6) 5.2 (2.0–6.0) 28.8 (9.2–39.9) 5.1 (2.7–7.1) 6.3 (2.8–8.1) 3.0 (0.9–5.3) 7.5 (4.0–10.3) 4.6 (1.0–7.3) 7.0 (4.0–10.0) 4.7 (3.5–7.0) 19.0 (12.3–21.0) 11.0 (8.3–14.0) 7.0 (4.0–8.0) 6.0 (4.0–7.0) 10.0 (6.0–12.0) 13.0 (10.3–15.0) 20.0 (14.0–25.0) 9.0 (7.3–10.0) 64.4 (33.3–93.6) 12.0 (8.3–16.0) 22.2 ± 42.7 8.6 ± 16.5 7.3 ± 18.0 6.3 ± 14.5 | 32.2 (29.0–34.6) 4.8 (3.6–5.4) 5.7 (4.8–5.7) 6.0 (5.6–6.0) 5.6 (4.6–6.0) 5.2 (4.2–6.0) 6.0 (6.0–6.0) 44.3 (35.0–48.0) 6.6 (5.2–7.6) 8.8 (7.0–10.0) 4.7 (3.1–6.0) 10.0 (8.0–11.0) 6.7 (5.0–7.8) 10.0 (8.3–11.0) 2.4 (1.5–4.8) 22.0 (19.5–24.0) 14.0 (11.0–17.0) 8.0 (7.0–9.0) 8.0 (6.5–8.5) 12.0 (10.0–13.0) 15.0 (15.0–15.0) 25.0 (22.0–26.5) 10.0 (10.0–10.0) 92.8 (78.6–96.7) 7.0 (4.0–10.0) 3.7 ± 8.1 2.6 ± 6.8 1.2 ± 3.0 0.0 ± 0.0 | 0.0002 0.0006 0.0002 0.0003 0.0008 0.0068 0.0005 0.0022 0.0187 0.0003 0.0288 0.0175 0.0206 0.0005 0.0003 0.0017 0.0082 0.0021 0.0001 0.0001 0.0002 0.0061 0.0004 0.0001 0.0002 0.0057 0.0276 0.5382 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heřmánková, B.; Špiritović, M.; Šmucrová, H.; Oreská, S.; Štorkánová, H.; Komarc, M.; Pavelka, K.; Šenolt, L.; Vencovský, J.; Bečvář, R.; et al. Female Sexual Dysfunction and Pelvic Floor Muscle Function Associated with Systemic Sclerosis: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 612. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010612
Heřmánková B, Špiritović M, Šmucrová H, Oreská S, Štorkánová H, Komarc M, Pavelka K, Šenolt L, Vencovský J, Bečvář R, et al. Female Sexual Dysfunction and Pelvic Floor Muscle Function Associated with Systemic Sclerosis: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(1):612. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010612
Chicago/Turabian StyleHeřmánková, Barbora, Maja Špiritović, Hana Šmucrová, Sabína Oreská, Hana Štorkánová, Martin Komarc, Karel Pavelka, Ladislav Šenolt, Jiří Vencovský, Radim Bečvář, and et al. 2022. "Female Sexual Dysfunction and Pelvic Floor Muscle Function Associated with Systemic Sclerosis: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 1: 612. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010612